

Efficacy Evaluation of Tissue Plasminogen Activator with Anti-Vascular Endothelial Growth Factor Drugs for Submacular Hemorrhage Treatment: A Meta-Analysis
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Literature Inclusion and Exclusion Criteria
2.3. Literature Quality Evaluation
2.4. Outcome Indicator
2.5. Data Extraction
2.6. Statistical Methods
3. Results
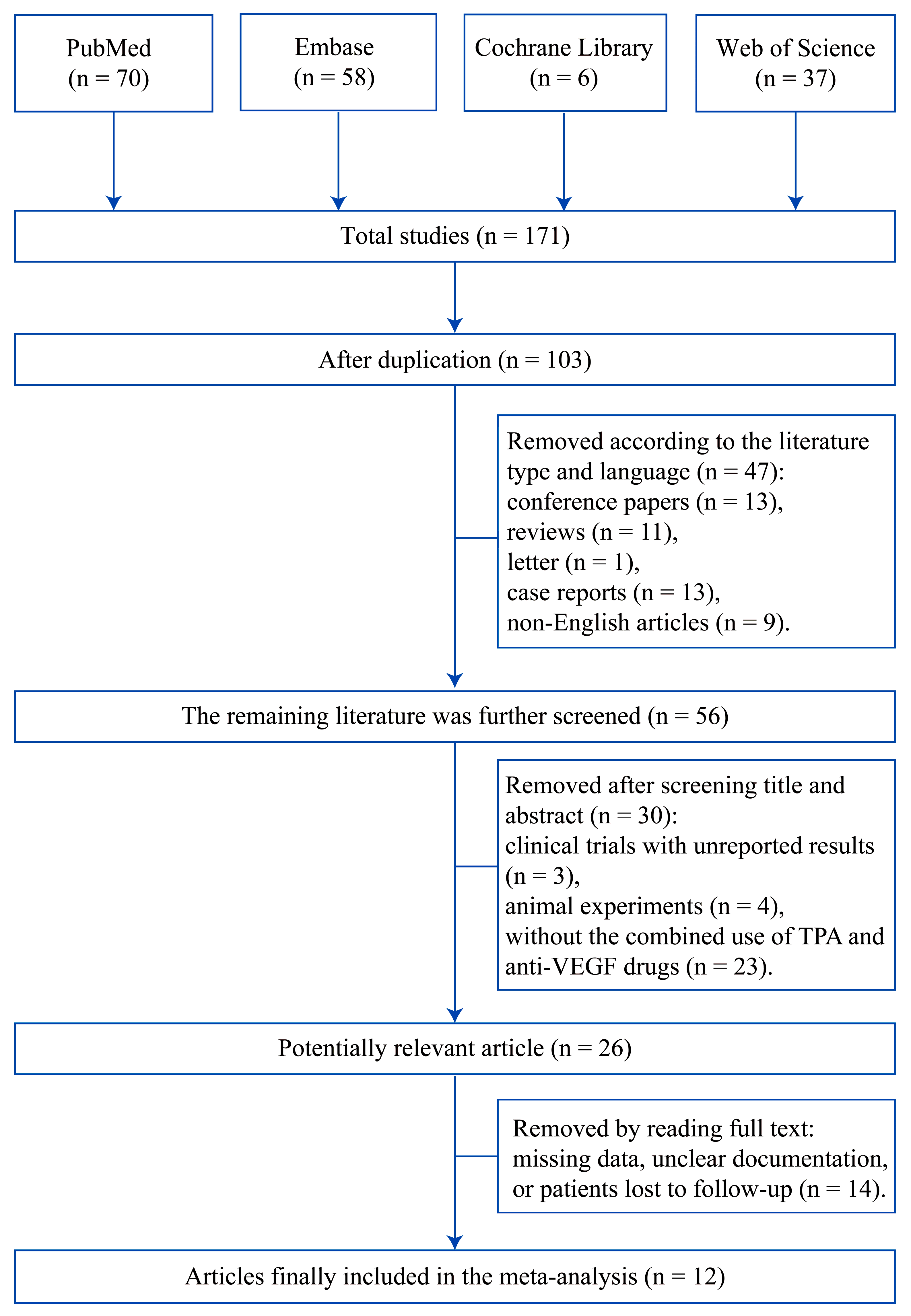
3.1. Search Results
3.2. Description of the Included Studies
3.3. Analysis Results
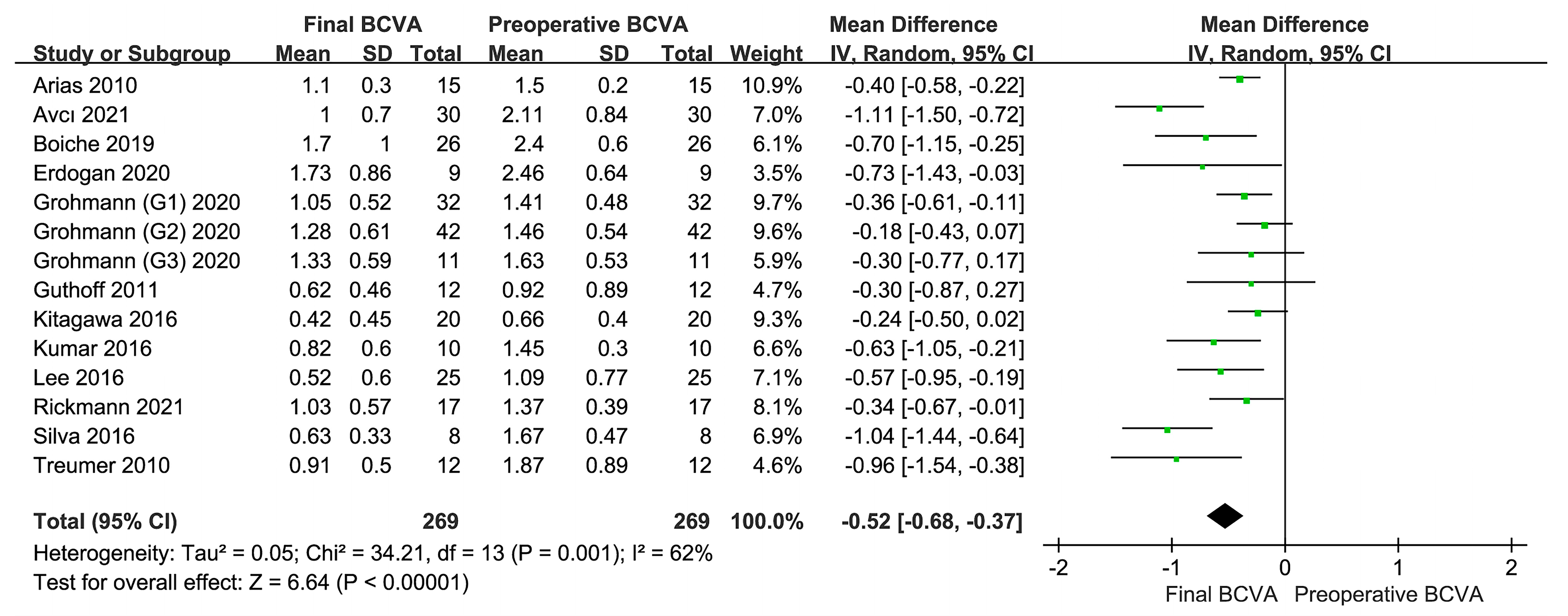
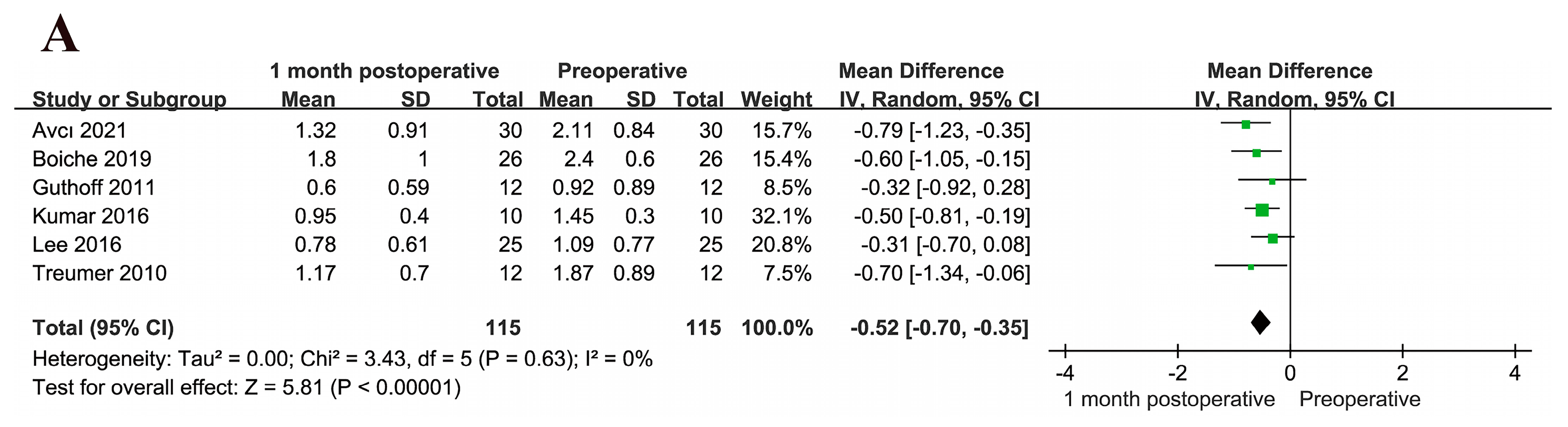
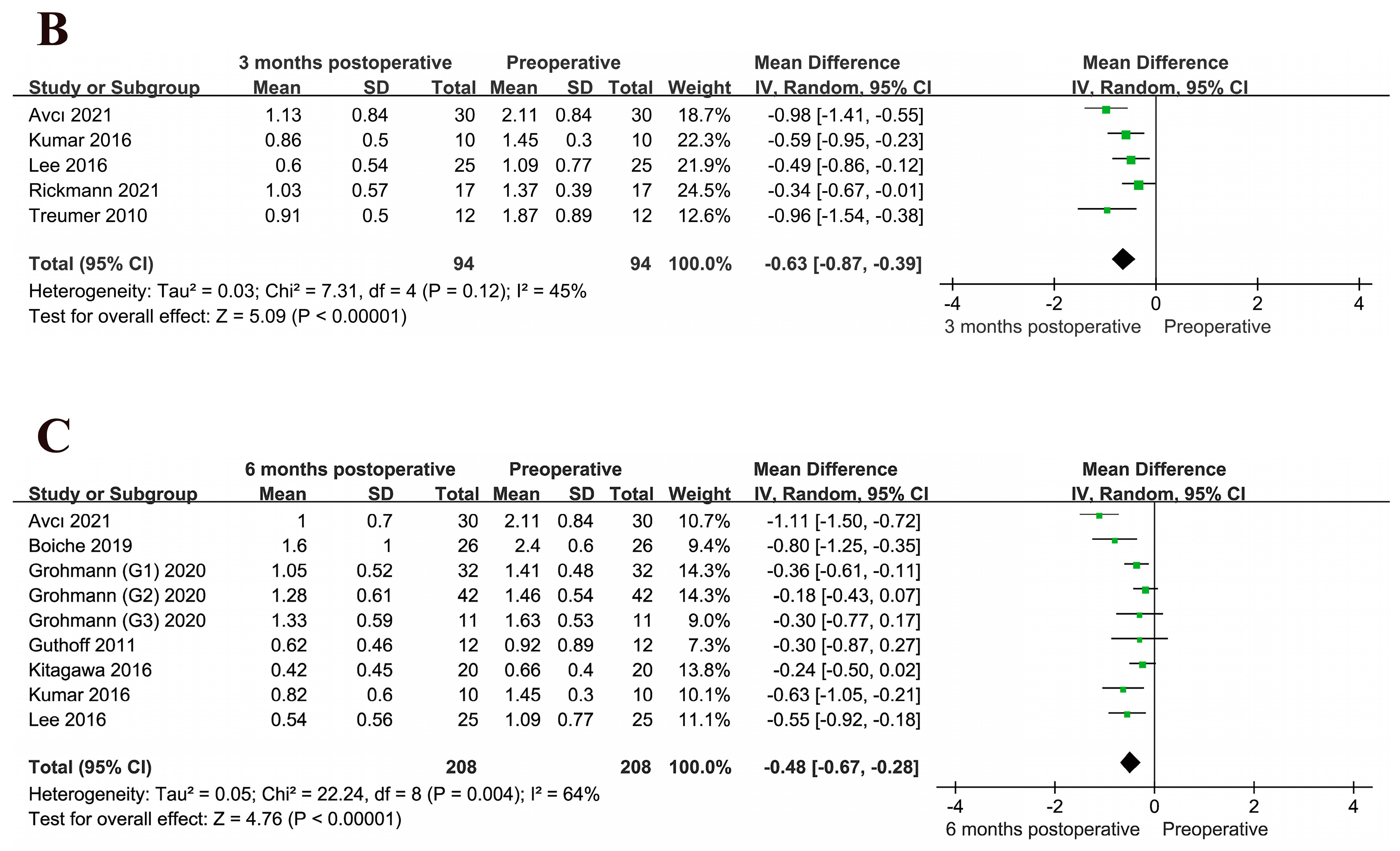
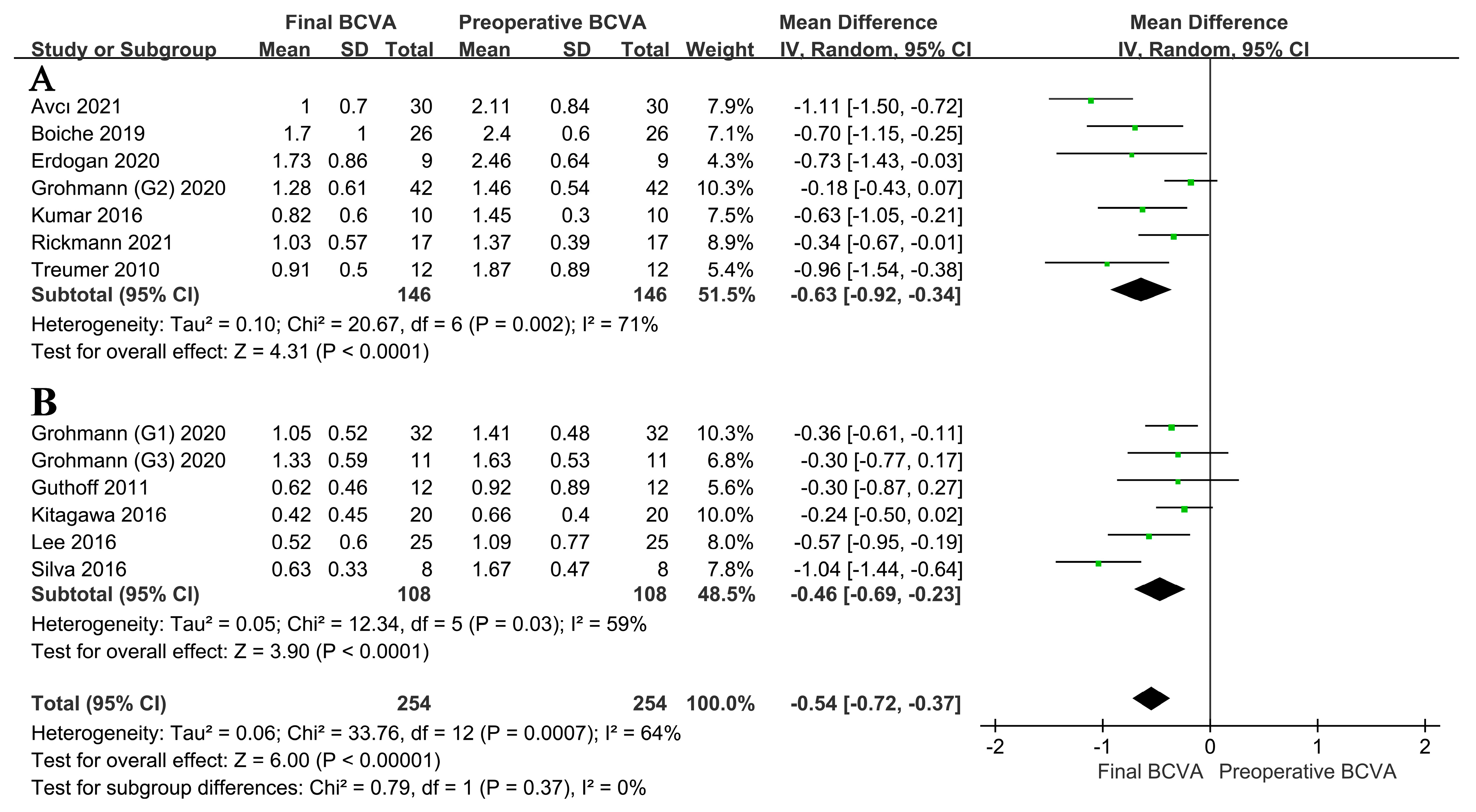
3.3.1. Analysis of BCVA
3.3.2. Effect of the Location of TPA Use on BCVA
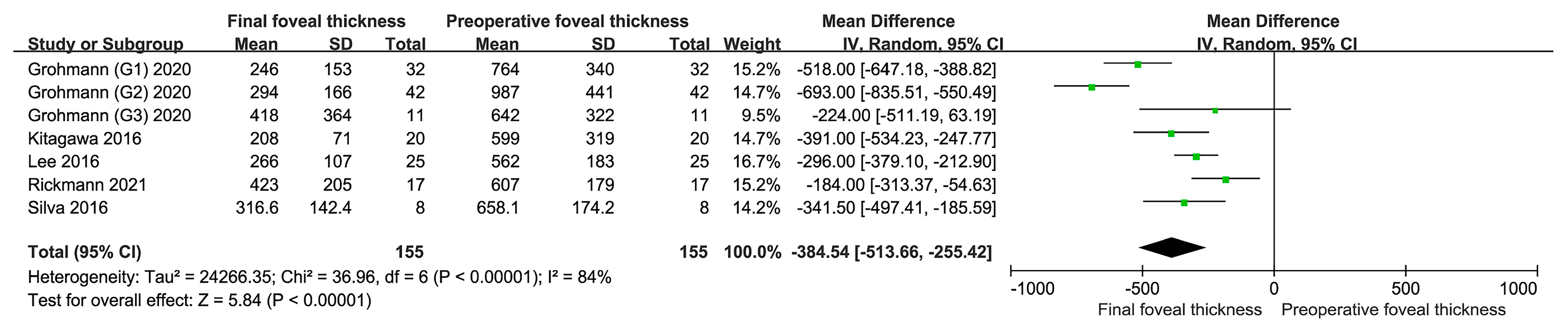
3.3.3. Analysis of Foveal Thickness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kunavisarut, P.; Thithuan, T.; Patikulsila, D.; Choovuthayakorn, J.; Watanachai, N.; Chaikitmongkol, V.; Pathanapitoon, K.; Rothova, A. Submacular Hemorrhage: Visual Outcomes and Prognostic Factors. Asia-Pac. J. Ophthalmol. 2018, 7, 109–113. [Google Scholar] [CrossRef]
- Hochman, M.A.; Seery, C.M.; Zarbin, M.A. Pathophysiology and management of subretinal hemorrhage. Surv. Ophthalmol. 1997, 42, 195–213. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, C.G.; Lee, D.W.; Yoo, S.J.; Lew, Y.J.; Cho, H.J.; Kim, J.Y.; Lee, S.H.; Kim, J.W. Intravitreal aflibercept for submacular hemorrhage secondary to neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 107–116. [Google Scholar] [CrossRef] [PubMed]
- McGowan, G.F.; Steel, D.; Yorston, D. AMD with submacular hemorrhage: New insights from a population-based study. Investig. Ophthalmol. Vis. Sci. 2014, 55, 662. [Google Scholar]
- Scimone, C.; Donato, L.; Marino, S.; Alafaci, C.; D’Angelo, R.; Sidoti, A. Vis-à-vis: A focus on genetic features of cerebral cavernous malformations and brain arteriovenous malformations pathogenesis. Neurol. Sci. 2019, 40, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Scimone, C.; Donato, L.; Alibrandi, S.; Esposito, T.; Alafaci, C.; D’Angelo, R.; Sidoti, A. Transcriptome analysis provides new molecular signatures in sporadic Cerebral Cavernous Malformation endothelial cells. Biochim. Biophys. Acta BBA—Mol. Basis Dis. 2020, 1866, 165956. [Google Scholar] [CrossRef] [PubMed]
- Bennett, S.R.; Folk, J.C.; Blodi, C.F.; Klugman, M. Factors prognostic of visual outcome in patients with subretinal hemorrhage. Am. J. Ophthalmol 1990, 109, 33–37. [Google Scholar] [CrossRef]
- Stanescu-Segall, D.; Balta, F.; Jackson, T.L. Submacular hemorrhage in neovascular age-related macular degeneration: A synthesis of the literature. Surv. Ophthalmol. 2016, 61, 18–32. [Google Scholar] [CrossRef] [PubMed]
- Rijken, D.C. 2 Plasminogen activators and plasminogen activator inhibitors: Biochemical aspects. Baillière’s Clin. Haematol. 1995, 8, 291–312. [Google Scholar] [CrossRef]
- Chang, W.; Garg, S.J.; Maturi, R.; Hsu, J.; Sivalingam, A.; Gupta, S.A.; Regillo, C.D.; Ho, A.C. Management of thick submacular hemorrhage with subretinal tissue plasminogen activator and pneumatic displacement for age-related macular degeneration. Am. J. Ophthalmol. 2014, 157, 1250–1257. [Google Scholar] [CrossRef]
- Chen, C.Y.; Hooper, C.; Chiu, D.; Chamberlain, M.; Karia, N.; Heriot, W.J. Management of submacular hemorrhage with intravitreal injection of tissue plasminogen activator and expansile gas. Retina 2007, 27, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.S.; Johnson, M.W.; Schneiderman, T.E.; Regillo, C.D.; Tornambe, P.E.; Poliner, L.S.; Blodi, B.A.; Elner, S.G. Management of submacular hemorrhage with intravitreous tissue plasminogen activator injection and pneumatic displacement. Ophthalmology 1999, 106, 1900–1907. [Google Scholar] [CrossRef] [PubMed]
- Hattenbach, L.O.; Klais, C.; Koch, F.H.; Gümbel, H.O. Intravitreous injection of tissue plasminogen activator and gas in the treatment of submacular hemorrhage under various conditions. Ophthalmology 2001, 108, 1485–1492. [Google Scholar] [CrossRef]
- Kamei, M.; Misono, K.; Lewis, H. A study of the ability of tissue plasminogen activator to diffuse into the subretinal space after intravitreal injection in rabbits. Am. J. Ophthalmol. 1999, 128, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.I.; Drews-Botsch, C.; Sternberg, P.; Capone, A.; Aaberg, T.M. Submacular Hemorrhage Removal. Ophthalmology 1995, 102, 1393–1399. [Google Scholar] [CrossRef]
- Brown, D.M.; Kaiser, P.K.; Michels, M.; Soubrane, G.; Heier, J.S.; Kim, R.Y.; Sy, J.P.; Schneider, S. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1432–1444. [Google Scholar] [CrossRef] [PubMed]
- Shienbaum, G.; Garcia Filho, C.A.; Flynn, H.W., Jr.; Nunes, R.P.; Smiddy, W.E.; Rosenfeld, P.J. Management of submacular hemorrhage secondary to neovascular age-related macular degeneration with anti-vascular endothelial growth factor monotherapy. Am. J. Ophthalmol. 2013, 155, 1009–1013. [Google Scholar] [CrossRef] [PubMed]
- Iacono, P.; Parodi, M.B.; Introini, U.; La Spina, C.; Varano, M.; Bandello, F. Intravitreal ranibizumab for choroidal neovascularization with large submacular hemorrhage in age-related macular degeneration. Retina 2014, 34, 281–287. [Google Scholar] [CrossRef]
- Bardak, H.; Bardak, Y.; Erçalık, Y.; Erdem, B.; Arslan, G.; Timlioglu, S. Sequential tissue plasminogen activator, pneumatic displacement, and anti-VEGF treatment for submacular hemorrhage. Eur J. Ophthalmol. 2018, 28, 306–310. [Google Scholar] [CrossRef]
- Avcı, R.; Yıldız, A.M.; Çınar, E.; Yılmaz, S.; Küçükerdönmez, C.; Akalp, F.D.; Avcı, E. Subretinal coapplication of tissue plasminogen activator and bevacizumab with concurrent pneumatic displacement for submacular hemorrhages secondary to neovascular age-related macular degeneration. Turk. J. Ophthalmol. 2021, 51, 38–44. [Google Scholar] [CrossRef]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Arias, L.; Monés, J. Transconjunctival sutureless vitrectomy with tissue plasminogen activator, gas and intravitreal bevacizumab in the management of predominantly hemorrhagic age-related macular degeneration. Clin. Ophthalmol. 2010, 4, 67–72. [Google Scholar] [CrossRef]
- Treumer, F.; Klatt, C.; Roider, J.; Hillenkamp, J. Subretinal coapplication of recombinant tissue plasminogen activator and bevacizumab for neovascular age-related macular degeneration with submacular haemorrhage. Br. J. Ophthalmol. 2010, 94, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Guthoff, R.; Guthoff, T.; Meigen, T.; Goebel, W. Intravitreous injection of bevacizumab, tissue plasminogen activator, and gas in the treatment of submacular hemorrhage in age-related macular degeneration. Retin. 2011, 31, 36–40. [Google Scholar] [CrossRef] [PubMed]
- de Silva, S.R.; Bindra, M.S. Early treatment of acute submacular haemorrhage secondary to wet AMD using intravitreal tissue plasminogen activator, C3F8, and an anti-VEGF agent. Eye 2016, 30, 952–957. [Google Scholar] [CrossRef]
- Kitagawa, Y.; Shimada, H.; Mori, R.; Tanaka, K.; Yuzawa, M. Intravitreal Tissue Plasminogen Activator, Ranibizumab, and Gas Injection for Submacular Hemorrhage in Polypoidal Choroidal Vasculopathy. Ophthalmology 2016, 123, 1278–1286. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Roy, S.; Bansal, M.; Tinwala, S.; Aron, N.; Temkar, S.; Pujari, A. Modified Approach in Management of Submacular Hemorrhage Secondary to Wet Age-Related Macular Degeneration. Asia Pac. J. Ophthalmol. 2016, 5, 143–146. [Google Scholar] [CrossRef]
- Lee, J.P.; Park, J.S.; Kwon, O.W.; You, Y.S.; Kim, S.H. Management of Acute Submacular Hemorrhage with Intravitreal Injection of Tenecteplase, Anti-vascular Endothelial Growth Factor and Gas. Korean J. Ophthalmol. 2016, 30, 192–197. [Google Scholar] [CrossRef]
- Boiche, M.; Angioi-Duprez, K.; Conart, J.B.; Berrod, J.P. Treatment of hematomas in age related macular degeneration by vitrectomy and subretinal injection r-tPA: Preliminary results. J. Fr. D’ophtalmologie 2019, 42, E391–E397. [Google Scholar] [CrossRef]
- Erdogan, G.; Kirmaci, A.; Perente, I.; Artunay, O. Gravitational displacement of submacular haemorrhage in patients with age-related macular disease. Eye 2020, 34, 1136–1141. [Google Scholar] [CrossRef]
- Grohmann, C.; Dimopoulos, S.; Bartz-Schmidt, K.U.; Schindler, P.; Katz, T.; Spitzer, M.S.; Skevas, C. Surgical management of submacular hemorrhage due to n-AMD: A comparison of three surgical methods. Int. J. Retin. Vitr. 2020, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- Rickmann, A.; Paez, L.R.; Della Volpe Waizel, M.; Bisorca-Gassendorf, L.; Schulz, A.; Vandebroek, A.C.; Szurman, P.; Januschowski, K. Functional and structural outcome after vitrectomy combined with subretinal rtPA Injection with or without additional intravitreal Bevacizumab injection for submacular hemorrhages. PLoS ONE 2021, 16, e0250587. [Google Scholar] [CrossRef] [PubMed]
- Ferris, F.L.; Kassoff, A.; Bresnick, G.H.; Bailey, I. New Visual Acuity Charts for Clinical Research. Am. J. Ophthalmol. 1982, 94, 91–96. [Google Scholar] [CrossRef]
- Casini, G.; Loiudice, P.; Menchini, M.; Sartini, F.; De Cillà, S.; Figus, M.; Nardi, M. Traumatic submacular hemorrhage: Available treatment options and synthesis of the literature. Int. J. Retin. Vitr. 2019, 5, 48. [Google Scholar] [CrossRef] [PubMed]
- van Zeeburg, E.J.; Cereda, M.G.; van Meurs, J.C. Recombinant tissue plasminogen activator, vitrectomy, and gas for recent submacular hemorrhage displacement due to retinal macroaneurysm. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 251, 733–740. [Google Scholar] [CrossRef]
- Collinge, J.E.; Simirskii, V.N.; Duncan, M.K. Expression of tissue plasminogen activator during eye development. Exp. Eye Res. 2005, 81, 90–96. [Google Scholar] [CrossRef]
- Tripathi, R.C.; Tripathi, B.J. Tissue plasminogen activator therapy for the eye. Br. J. Ophthalmol. 2005, 89, 1390–1391. [Google Scholar] [CrossRef] [PubMed]
- Noma, H.; Yasuda, K.; Shimura, M. Involvement of Cytokines in the Pathogenesis of Diabetic Macular Edema. Int. J. Mol. Sci. 2021, 22, 3427. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, S.M.; Arepalli, S.; Ehlers, J.P. Current and Future Anti-VEGF Agents for Neovascular Age-Related Macular Degeneration. J. Exp. Pharmacol. 2021, 13, 905–912. [Google Scholar] [CrossRef]
- Wilkins, C.S.; Mehta, N.; Wu, C.Y.; Barash, A.; Deobhakta, A.A.; Rosen, R.B. Outcomes of pars plana vitrectomy with subretinal tissue plasminogen activator injection and pneumatic displacement of fovea-involving submacular haemorrhage. BMJ Open Ophthalmol. 2020, 5, e000394. [Google Scholar] [CrossRef]
- Ohayon, A.; Schwartz, S.; Loewenstein, A.; Seknazi, D.; Souied, E.H.; Barak, A. A Modified Surgical Technique for Submacular Injection. Ophthalmic Surg. Lasers Imaging Retin. 2021, 52, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Tranos, P.; Tsiropoulos, G.N.; Koronis, S.; Vakalis, A.; Asteriadis, S.; Stavrakas, P. Comparison of subretinal versus intravitreal injection of recombinant tissue plasminogen activator with gas for submacular hemorrhage secondary to wet age-related macular degeneration: Treatment outcomes and brief literature review. Int. Ophthalmol. 2021, 41, 4037–4046. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.E.; Shulman, J.P.; Swan, R.J.; Teske, M.P.; Bernstein, P.S. Intravitreal Versus Subretinal Tissue Plasminogen Activator Injection for Submacular Hemorrhage. Ophthalmic Surg. Lasers Imaging Retin. 2017, 48, 26–32. [Google Scholar] [CrossRef]
- Donato, L.; Scimone, C.; Alibrandi, S.; Scalinci, S.Z.; Rinaldi, C.; D’Angelo, R.; Sidoti, A. Epitranscriptome Analysis of Oxidative Stressed Retinal Epithelial Cells Depicted a Possible RNA Editing Landscape of Retinal Degeneration. Antioxidants 2022, 11, 1967. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Publication Time (Year) | Patient No. | Eye No. | Country | Etiology | Age (Years) | Duration (Days) | Hemorrhage Area (DD) | NOS | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Total | Mean | SD | Mean | SD | Mean | SD | ||||||
| Arias [22] | 2010 | 5 | 10 | 15 | 15 | Spain | AMD | 79.6 | 8.6 | ≤5 | 9.8 | 2.9 | ☆☆☆☆☆ | |
| Avcı [20] | 2021 | 14 | 16 | 30 | 30 | Turkey | AMD | 73.33 | 8.23 | 13.7 | 8.05 | 22.7 | 15.9 | ☆☆☆☆☆ |
| Boiche [29] | 2019 | 9 | 17 | 26 | 26 | French | AMD | 78 | 8 | 7 | 4.8 | 4.2 | 1.7 | ☆☆☆☆☆ |
| Erdogan [30] | 2020 | 4 | 5 | 9 | 9 | Turkey | AMD | 72.2 | 10.2 | 15.3 | 12.8 | - | - | ☆☆☆☆☆ |
| Grohmann (G1) [31] | 2020 | - | - | 32 | 32 | Germany | AMD | 85.36 | - | 9.1 | 4.6 | 4.4 | 1.8 | ☆☆☆☆☆☆☆ |
| Grohmann (G2) [31] | 2020 | - | - | 42 | 42 | Germany | AMD | 85.36 | - | 9.1 | 4.6 | 4.14 | 1.3 | ☆☆☆☆☆☆☆ |
| Grohmann (G3) [31] | 2020 | - | - | 11 | 11 | Germany | AMD | 85.36 | - | 9.1 | 4.6 | 4.68 | 2.8 | ☆☆☆☆☆☆☆ |
| Guthoff [24] | 2011 | 5 | 7 | 12 | 12 | Germany | AMD | 80.67 | 11.25 | 6.23 | 4.58 | 2.28 | ☆☆☆☆☆☆☆ | |
| Kitagawa [26] | 2016 | 16 | 4 | 20 | 20 | Japan | AMD & PCV | 70 | 11 | 9.9 | 9.8 | 4.07 | 3.19 | ☆☆☆☆☆ |
| Kumar [27] | 2016 | 6 | 4 | 10 | 10 | India | AMD | 66.9 | 7.3 | 5 | 3.1 | - | - | ☆☆☆☆☆ |
| Lee [28] | 2016 | 14 | 11 | 25 | 25 | Korea | AMD | 67.6 | 8.9 | 7.2 | 8.2 | 7.5 | 5.0 | ☆☆☆☆☆ |
| Rickmann [32] | 2021 | 6 | 11 | 17 | 17 | Germany | AMD | 81.7 | 5.2 | 3.3 | 1.6 | - | - | ☆☆☆☆☆☆☆ |
| Silva [25] | 2016 | 4 | 4 | 8 | 8 | UK | AMD | 81 | 4.3 | 3 | 1 | 6.0 | 5.2 | ☆☆☆☆☆ |
| Treumer [23] | 2010 | 3 | 9 | 12 | 12 | Germany | AMD | 81.5 | 5.4 | 4.8 | 3.8 | 4.3 | 3.2 | ☆☆☆☆☆ |
| Author | Publication Time (Year) | Operations | Complication Rate | Displacement Rate | Postoperative Position | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PPV | SRI TPA | IVI TPA | SRI Anti-VEGF | IVI Anti-VEGF | Gas Tamponade | Total | Subtotal | Position | Time (Days) | |||
| Arias [22] | 2010 | + | + | + | + | + | 20% | 100% | ||||
| Avcı [20] | 2021 | + | + | + | + | 53.3% | 46.7% | Reading position | 5 | |||
| Boiche [29] | 2019 | + | + | + | + | 15.4% | 81% | Head down | 3 | |||
| Erdogan [30] | 2020 | + | + | + | Lying down | 1–3 | ||||||
| Grohmann (G1) [31] | 2020 | + | + | + | 2.4% | 100% | Prone position | At least 7 | ||||
| Grohmann (G2) [31] | 2020 | + | + | + | + | |||||||
| Grohmann (G3) [31] | 2020 | + | + | + | + | |||||||
| Guthoff [24] | 2011 | + | + | + | Prone position | 2 | ||||||
| Kitagawa [26] | 2016 | + | + | 20.0% | 85% | 15% | Prone position | 2 | ||||
| Kumar [27] | 2016 | + | + | + | + | 20.0% | 100% | |||||
| Lee [28] | 2016 | + | + | + | 8.0% | Prone position | At least 7 | |||||
| Rickmann [32] | 2021 | + | + | + | + | 17.6% | 47% | Face down | ||||
| Silva [25] | 2016 | + | + | + | 37.5% | 100% | Face down | 5 | ||||
| Treumer [23] | 2010 | + | + | + | + | 33.3% | 75% | 25% | Prone position | 1 | ||
| Author | Publication Time (Year) | Preoperative BCVA | Postoperative BCVA | Final BCVA | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Month | 2 Months | 3 Months | 6 Months | 12 Months | |||||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Arias [22] | 2010 | 1.5 | 0.2 | 1.1 | 0.3 | ||||||||||
| Avcı [20] | 2021 | 2.11 | 0.84 | 1.32 | 0.91 | 0.94 | 0.66 | 1.13 | 0.84 | 1.0 | 0.7 | 1.0 | 0.7 | ||
| Boiche [29] | 2019 | 2.4 | 0.6 | 1.8 | 1.0 | 1.6 | 1.0 | 1.7 | 1.0 | ||||||
| Erdogan [30] | 2020 | 2.46 | 0.64 | 1.73 | 0.86 | ||||||||||
| Grohmann (G1) [31] | 2020 | 1.41 | 0.48 | 1.05 | 0.52 | 1.05 | 0.52 | ||||||||
| Grohmann (G2) [31] | 2020 | 1.46 | 0.54 | 1.28 | 0.61 | 1.28 | 0.61 | ||||||||
| Grohmann (G3) [31] | 2020 | 1.63 | 0.53 | 1.33 | 0.59 | 1.33 | 0.59 | ||||||||
| Guthoff [24] | 2011 | 0.92 | 0.89 | 0.6 | 0.59 | 0.62 | 0.46 | 0.62 | 0.46 | ||||||
| Kitagawa [26] | 2016 | 0.66 | 0.4 | 0.42 | 0.45 | 0.42 | 0.45 | ||||||||
| Kumar [27] | 2016 | 1.45 | 0.3 | 0.95 | 0.4 | 0.86 | 0.5 | 0.82 | 0.6 | 0.82 | 0.6 | ||||
| Lee [28] | 2016 | 1.09 | 0.77 | 0.78 | 0.61 | 0.6 | 0.54 | 0.54 | 0.56 | 0.52 | 0.6 | 0.52 | 0.6 | ||
| Rickmann [32] | 2021 | 1.37 | 0.39 | 1.03 | 0.57 | 1.03 | 0.57 | ||||||||
| Silva [25] | 2016 | 1.67 | 0.47 | 0.63 | 0.33 | ||||||||||
| Treumer [23] | 2010 | 1.87 | 0.89 | 1.17 | 0.7 | 0.91 | 0.5 | 0.91 | 0.5 | ||||||
| Author | Publication Time (Year) | Preoperative Foveal Thickness (μm) | Postoperative Foveal Thickness (μm) | Final Foveal Thickness (μm) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Month | 3 Months | 6 Months | |||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Grohmann (G1) [31] | 2020 | 764 | 340 | 246 | 153 | 246 | 153 | ||||
| Grohmann (G2) [31] | 2020 | 987 | 441 | 294 | 166 | 294 | 166 | ||||
| Grohmann (G3) [31] | 2020 | 642 | 322 | 418 | 364 | 418 | 364 | ||||
| Kitagawa [26] | 2016 | 599 | 319 | 208 | 71 | 208 | 71 | ||||
| Lee [28] | 2016 | 562 | 183 | 244 | 85 | 215 | 58 | 250 | 119 | 266 | 107 |
| Rickmann [32] | 2021 | 607 | 179 | 423 | 205 | 423 | 205 | ||||
| Silva [25] | 2016 | 658.1 | 174.2 | 316.6 | 142.4 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, X.; Cao, W.; Wang, Z.; Zhang, N.; Xu, K.; Yu, L.; Xing, Y.; Yang, N. Efficacy Evaluation of Tissue Plasminogen Activator with Anti-Vascular Endothelial Growth Factor Drugs for Submacular Hemorrhage Treatment: A Meta-Analysis. J. Clin. Med. 2023, 12, 1035. https://doi.org/10.3390/jcm12031035
He X, Cao W, Wang Z, Zhang N, Xu K, Yu L, Xing Y, Yang N. Efficacy Evaluation of Tissue Plasminogen Activator with Anti-Vascular Endothelial Growth Factor Drugs for Submacular Hemorrhage Treatment: A Meta-Analysis. Journal of Clinical Medicine. 2023; 12(3):1035. https://doi.org/10.3390/jcm12031035
Chicago/Turabian StyleHe, Xuejun, Wenye Cao, Zhiyi Wang, Ningzhi Zhang, Kexin Xu, Lu Yu, Yiqiao Xing, and Ning Yang. 2023. "Efficacy Evaluation of Tissue Plasminogen Activator with Anti-Vascular Endothelial Growth Factor Drugs for Submacular Hemorrhage Treatment: A Meta-Analysis" Journal of Clinical Medicine 12, no. 3: 1035. https://doi.org/10.3390/jcm12031035
APA StyleHe, X., Cao, W., Wang, Z., Zhang, N., Xu, K., Yu, L., Xing, Y., & Yang, N. (2023). Efficacy Evaluation of Tissue Plasminogen Activator with Anti-Vascular Endothelial Growth Factor Drugs for Submacular Hemorrhage Treatment: A Meta-Analysis. Journal of Clinical Medicine, 12(3), 1035. https://doi.org/10.3390/jcm12031035