
Heart Rate and Heart Rate Variability in Healthy Preterm-Born Young Adults and Association with Vitamin D: A Wearable Device Assessment

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
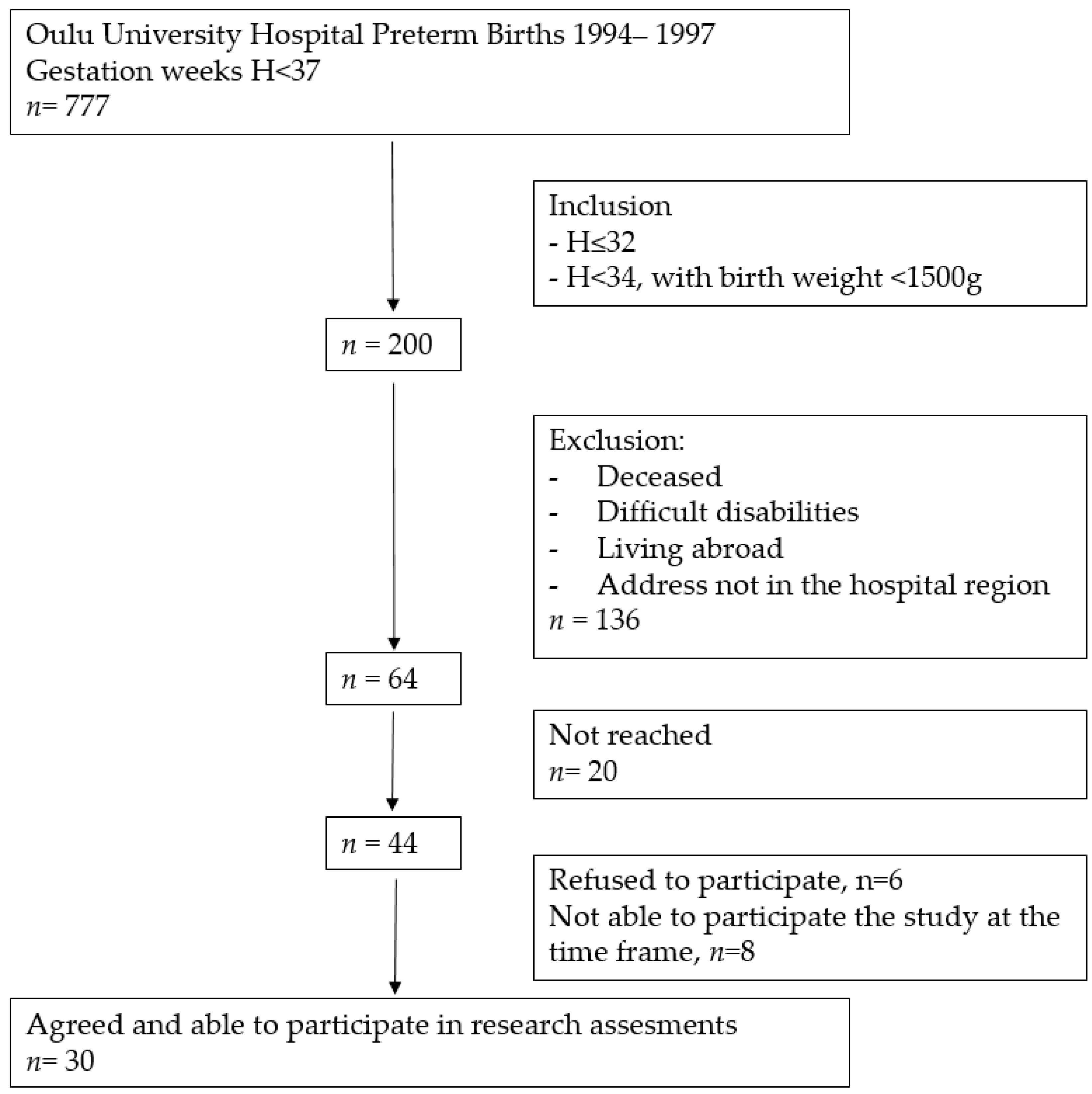
3.1. Study Participants
3.2. Autonomic Heart Function Parameters
3.3. Gender Differences
3.4. Association of Physical Activity with Cardiac Parameters
3.5. Association of Neonatal Factors with Cardiac Parameters
3.6. Association of Vitamin D with Cardiac Parametres
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [PubMed]
- Chehade, H.; Simeoni, U.; Guignard, J.-P.; Boubred, F. Preterm Birth: Long Term Cardiovascular and Renal Consequences. Curr. Pediatr. Rev. 2018, 14, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Bavineni, M.; Wassenaar, T.M.; Agnihotri, K.; Ussery, D.W.; Lüscher, T.F.; Mehta, J.L. Mechanisms linking preterm birth to onset of cardiovascular disease later in adulthood. Eur. Heart J. 2019, 40, 1107–1112. [Google Scholar] [CrossRef] [PubMed]
- Markopoulou, P.; Papanikolaou, E.; Analytis, A.; Zoumakis, E.; Siahanidou, T. Preterm Birth as a Risk Factor for Metabolic Syndrome and Cardiovascular Disease in Adult Life: A Systematic Review and Meta-Analysis. J. Pediatr. 2019, 210, 69–80.e5. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, A.J.; Levy, P.T.; Bates, M.L.; McNamara, P.J.; Nuyt, A.M.; Goss, K.N. Impact of the Vulnerable Preterm Heart and Circulation on Adult Cardiovascular Disease Risk. Hypertension 2020, 76, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Groves, A.; Sundquist, J.; Sundquist, K. Association of Preterm Birth with Long-term Risk of Heart Failure into Adulthood. JAMA Pediatr. 2021, 175, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Bates, M.L.; Levy, P.T.; Nuyt, A.M.; Goss, K.N.; Lewandowski, A.J.; McNamara, P.J. Adult Cardiovascular Health Risk and Cardiovascular Phenotypes of Prematurity. J. Pediatr. 2020, 227, 17–30. [Google Scholar] [CrossRef]
- Lammertink, F.; Vinkers, C.H.; Tataranno, M.L.; Benders, M.J.N.L. Premature Birth and Developmental Programming: Mechanisms of Resilience and Vulnerability. Front. Psychiatry 2021, 11, 531571. [Google Scholar] [CrossRef]
- Mulkey, S.B.; Dú Plessis, A. The Critical Role of the Central Autonomic Nervous System in Fetal-Neonatal Transition. Semin. Pediatr. Neurol. 2018, 28, 29–37. [Google Scholar] [CrossRef]
- Herzig, D.; Eser, P.; Omlin, X.; Riener, R.; Wilhelm, M.; Achermann, P. Reproducibility of heart rate variability is parameter and sleep stage dependent. Front. Physiol. 2018, 8, 1100. [Google Scholar] [CrossRef]
- Berntson, G.G.; Bigger, J.T.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H.; et al. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology 1997, 34, 623–648. [Google Scholar] [CrossRef] [PubMed]
- Haraldsdottir, K.; Watson, A.M.; Goss, K.N.; Beshish, A.G.; Pegelow, D.F.; Palta, M.; Tetri, L.H.; Barton, G.P.; Brix, M.D.; Centanni, R.M.; et al. Impaired autonomic function in adolescents born preterm. Physiol. Rep. 2018, 6, e13620. [Google Scholar] [CrossRef] [PubMed]
- Haraldsdottir, K.; Watson, A.M.; Beshish, A.G.; Pegelow, D.F.; Palta, M.; Tetri, L.H.; Brix, M.D.; Centanni, R.M.; Goss, K.N.; Eldridge, M.W. Heart rate recovery after maximal exercise is impaired in healthy young adults born preterm. Eur. J. Appl. Physiol. 2019, 119, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Ogliari, G.; Mahinrad, S.; Stott, D.J.; Jukema, J.W.; Mooijaart, S.P.; Macfarlane, P.W.; Clark, E.N.; Kearney, P.M.; Westendorp, R.G.J.; De Craen, A.J.M.; et al. Resting heart rate, heart rate variability and functional decline in old age. CMAJ 2015, 187, E442–E449. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wu, H.; Zhang, X.; Wei, X.; Hou, F.; Ma, Y. Sleep heart rate variability assists the automatic prediction of long-term cardiovascular outcomes. Sleep Med. 2020, 67, 217–224. [Google Scholar] [CrossRef]
- Stone, J.D.; Ulman, H.K.; Tran, K.; Thompson, A.G.; Halter, M.D.; Ramadan, J.H.; Stephenson, M.; Finomore, V.S.; Galster, S.M.; Rezai, A.R.; et al. Assessing the Accuracy of Popular Commercial Technologies That Measure Resting Heart Rate and Heart Rate Variability. Front. Sports Act. Living 2021, 3, 585870. [Google Scholar] [CrossRef]
- Kinnunen, H.; Rantanen, A.; Kentt, T.; Koskim ki, H. Feasible assessment of recovery and cardiovascular health: Accuracy of nocturnal HR and HRV assessed via ring PPG in comparison to medical grade ECG. Physiol. Meas. 2020, 41, 04NT01. [Google Scholar] [CrossRef]
- Karemaker, R.; Karemaker, J.M.; Kavelaars, A.; Tersteeg-Kamperman, M.; Baerts, W.; Veen, S.; Samsom, J.F.; van Bel, F.; Heijnen, C.J. Effects of neonatal dexamethasone treatment on the cardiovascular stress response of children at school age. Pediatrics 2008, 122, 978–987. [Google Scholar] [CrossRef]
- Nixon, P.A.; Washburn, L.K.; Michael O’Shea, T.; Shaltout, H.A.; Russell, G.B.; Snively, B.M.; Rose, J.C. Antenatal steroid exposure and heart rate variability in adolescents born with very low birth weight. Pediatr. Res. 2017, 81, 57–62. [Google Scholar] [CrossRef]
- Gholami, F.; Moradi, G.; Zareei, B.; Rasouli, M.A.; Nikkhoo, B.; Roshani, D.; Ghaderi, E. The association between circulating 25-hydroxyvitamin D and cardiovascular diseases: A meta-analysis of prospective cohort studies. BMC Cardiovasc. Disord. 2019, 19, 248. [Google Scholar] [CrossRef]
- Latic, N.; Erben, R.G. Vitamin D and cardiovascular disease, with emphasis on hypertension, atherosclerosis, and heart failure. Int. J. Mol. Sci. 2020, 21, 6483. [Google Scholar] [CrossRef] [PubMed]
- Marquina, C.; Mousa, A.; Scragg, R.; de Courten, B. Vitamin D and cardiometabolic disorders: A review of current evidence, genetic determinants and pathomechanisms. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2019, 20, 262–277. [Google Scholar] [CrossRef] [PubMed]
- Matter, M.; El-Sherbiny, E.; Elmougy, A.; Abass, M.; Aldossary, S.; Ali, W.A. Myocardial function in Saudi adolescents with vitamin D deficiency: Tissue Doppler imaging study. J. Saudi Heart Assoc. 2016, 28, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Sauder, K.A.; Stamatoiu, A.V.; Leshchinskaya, E.; Ringham, B.M.; Glueck, D.H.; Dabelea, D. Cord Blood Vitamin D Levels and Early Childhood Blood Pressure: The Healthy Start Study. J. Am. Heart Assoc. 2019, 8, e011485. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Liu, X.; Bartell, T.R.; Pearson, C.; Cheng, T.L.; Wang, X. Vitamin D Trajectories from Birth to Early Childhood and Elevated Systolic Blood Pressure During Childhood and Adolescence. Hypertension 2019, 74, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.R.; Jin, H.F.; Du, J.B. Vitamin D and Cardiovascular Risk in Children. Chin. Med. J. 2017, 130, 2857–2862. [Google Scholar] [CrossRef] [PubMed]
- Canpolat, U.; Özcan, F.; Özeke, Ö.; Turak, O.; Yayla, Ç.; Açıkgöz, S.K.; Cay, S.; Topaloğlu, S.; Aras, D.; Aydoğdu, S. Impaired Cardiac Autonomic Functions in Apparently Healthy Subjects with Vitamin D Deficiency. Ann. Noninvasive Electrocardiol. 2015, 20, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Mann, M.C.; Exner, D.V.; Hemmelgarn, B.R.; Sola, D.Y.; Turin, T.C.; Ellis, L.; Ahmed, S.B. Vitamin D levels are associated with cardiac autonomic activity in healthy humans. Nutrients 2013, 5, 2114–2127. [Google Scholar] [CrossRef]
- Tak, Y.J.; Lee, J.G.; Kim, Y.J.; Lee, S.Y.; Cho, B.M. 25-hydroxyvitamin D and its relationship with autonomic dysfunction using time- and frequency-domain parameters of heart rate variability in Korean populations: A cross-sectional study. Nutrients 2014, 6, 4373–4388. [Google Scholar] [CrossRef]
- Mathewson, K.J.; Van Lieshout, R.J.; Saigal, S.; Morrison, K.M.; Boyle, M.H.; Schmidt, L.A. Autonomic Functioning in Young Adults Born at Extremely Low Birth Weight. Glob. Pediatr. Health 2015, 2, 2333794X1558956. [Google Scholar] [CrossRef]
- Karvonen, R.; Sipola, M.; Kiviniemi, A.; Tikanmäki, M.; Järvelin, M.R.; Eriksson, J.G.; Tulppo, M.; Vääräsmäki, M.; Kajantie, E. Cardiac Autonomic Function in Adults Born Preterm. J. Pediatr. 2019, 208, 96–103.e4. [Google Scholar] [CrossRef] [PubMed]
- Altini, M.; Plews, D. What is behind changes in resting heart rate and heart rate variability? A large-scale analysis of longitudinal measurements acquired in free-living. Sensors 2021, 21, 7932. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Thayer, J.F. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosci. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef] [PubMed]
- Bonnemeier, H.; Richardt, G.; Potratz, J.; Wiegand, U.K.H.; Brandes, A.; Kluge, N.; Katus, H.A. Circadian profile of cardiac autonomic nervous modulation in healthy subjects: Differing effects of aging and gender on heart rate variability. J. Cardiovasc. Electrophysiol. 2003, 14, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Tegegne, B.S.; Man, T.; van Roon, A.M.; Riese, H.; Snieder, H. Determinants of heart rate variability in the general population: The Lifelines Cohort Study. Heart Rhythm 2018, 15, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Sammito, S.; Böckelmann, I. Reference values for time- and frequency-domain heart rate variability measures. Heart Rhythm 2016, 13, 1309–1316. [Google Scholar] [CrossRef] [PubMed]
- Kaseva, N.; Martikainen, S.; Tammelin, T.; Hovi, P.; Järvenpää, A.L.; Andersson, S.; Eriksson, J.G.; Räikkönen, K.; Pesonen, A.K.; Wehkalampi, K.; et al. Objectively measured physical activity in young adults born preterm at very low birth weight. J. Pediatr. 2015, 166, 474–476. [Google Scholar] [CrossRef] [PubMed]
- Hautala, A.J.; Karjalainen, J.; Kiviniemi, A.M.; Kinnunen, H.; Mäkikallio, T.H.; Huikuri, H.V.; Tulppo, M.P. Physical activity and heart rate variability measured simultaneously during waking hours. Am. J. Physiol. Heart Circ. Physiol. 2010, 298, H874–H880. [Google Scholar] [CrossRef]
- Huckstep, O.J.; Burchert, H.; Williamson, W.; Telles, F.; Tan, C.M.J.; Bertagnolli, M.; Arnold, L.; Mohamed, A.; Mccormick, K.; Hanssen, H.; et al. Impaired myocardial reserve underlies reduced exercise capacity and heart rate recovery in preterm-born young adults. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 572–580. [Google Scholar] [CrossRef]
- Raulio, S.; Erlund, I.; Männistö, S.; Sarlio-Lähteenkorva, S.; Sundvall, J.; Tapanainen, H.; Vartiainen, E.; Virtanen, S.M. Successful nutrition policy: Improvement of Vitamin D intake and status in Finnish adults over the last decade. Eur. J. Public Health 2017, 27, 268–273. [Google Scholar] [CrossRef]
- Nalbant, A.; Vatan, M.B.; Varım, P.; Varım, C.; Kaya, T.; Tamer, A. Does vitamin D deficiency effect heart rate variability in low cardiovascular risk population? Open Access Maced. J. Med. Sci. 2017, 5, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Cao, R.; Azimi, I.; Sarhaddi, F.; Niela-Vilen, H.; Axelin, A.; Liljeberg, P.; Rahmani, A.M. Accuracy Assessment of Oura Ring Nocturnal Heart Rate and Heart Rate Variability in Comparison with Electrocardiography in Time and Frequency Domains: Comprehensive Analysis. J. Med. Internet Res. 2022, 24, e27487. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.J.; Sargent, C.; Roach, G.D. A Validation of Six Wearable Devices for Estimating Sleep, Heart Rate and Heart Rate Variability in Healthy Adults. Sensors 2022, 22, 6317. [Google Scholar] [CrossRef] [PubMed]
- Lowe, A.; Littlewood, C.; McLean, S.; Kilner, K. Physiotherapy and physical activity: A cross-sectional survey exploring physical activity promotion, knowledge of physical activity guidelines and the physical activity habits of UK physiotherapists. BMJ Open Sport Exerc. Med. 2017, 3, e000290. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Values | PT (n = 30) | FT (n = 16) |
|---|---|---|
| Mean birth gestation weeks (SD) | 30.3 (1.4) | 39.7 (0.8) |
| Sex, Female/male (% male) | 19/11 (37) | 11/5 (31) |
| Mean birth weight, g (SD) | ||
| All | 1361 (311) | 3520 (424) |
| Female | 1357 (356) | 3475 (472) |
| Male | 1368 (230) | 3620 (315) |
| ELBW, n (%) | 6 (20) | - |
| SGA, n (%) | 4 (13) | - |
| AND, n (%) | 12 (40) | - |
| PND, n (%) | 9 (30) | - |
| RDS, n (%) | 20 (67) | - |
| BPD, n (%) | 5 (17) | - |
| IVH gr II–III, n (%) | 1 (3) | - |
| Age in years, mean (SD) | ||
| All | 24.4 (0.9) | 24.0 (1.0) |
| Female | 24.5 (1.2) | 24.2 (0.9) |
| Male | 24.0 (1.1) | 23.7 (1.0) |
| Weight in kg, mean (SD) | ||
| All | 66.2 (10.4) | 67.0 (11.0) |
| Female | 63.8 (11.2) | 63.9 (10.5) |
| Male | 70.4 (7.7) | 73.9 (9.4) |
| Height in cm, mean (SD) | ||
| All | 167.9 (8.0) | 170.4 (7.9) |
| Female | 163.7 (5.8) | 167.0 (5.6) |
| Male | 175.3 (5.8) | 178.0 (7.1) |
| BMI, mean (SD) | ||
| All | 23.5 (3.4) | 23.0 (3.2) |
| Female | 23.8 (3.8) | 22.9 (3.8) |
| Male | 23.0 (2.4) | 23.2 (1.0) |
| High school, n (%) | 22 (73) | 15 (94) * |
| University/College, n (%) | 19 (63) | 15 (94) * |
| Parameter | PT; n = 30 F/M 19/11 | FT; n = 16 F/M 11/5 | p-Value |
|---|---|---|---|
| Lowest Heart Rate (bpm): mean (SD) | |||
| On weekdays | |||
| All | 51.1 (6.5) | 49.0 (6.1) | 0.29 |
| Female | 53.1 (6.1) | 51.2 (5.5) | 0.42 |
| Male | 47.7 (6.1) | 44.0 (4.2) | 0.24 |
| On weekends | |||
| All | 51.9 (7.4) | 48.4 (5.6) | 0.10 |
| Female | 53.3 (7.0) | 50.6 (4.9) | 0.26 |
| Male | 49.3 (7.6) | 43.5 (3.5) | 0.13 |
| Over two weeks | |||
| All | 51.4 (6.8) | 48.7 (5.8) | 0.18 |
| Female | 53.2 (6.4) | 50.9 (5.2) | 0.33 |
| Male | 48.4 (6.6) | 43.8 (3.8) | 0.17 |
| RMSSD (ms): mean (SD) | |||
| On weekdays | |||
| All | 73.6 (31.5) | 78.0 (33.9) | 0.66 |
| Female | 73.9 (36.2) | 70.0 (33.6) | 0.77 |
| Male | 73.0 (22.6) | 95.6 (30.2) | 0.12 |
| On weekends | |||
| All | 72.8 (31.1) | 81.3 (32.1) | 0.39 |
| Female | 74.2 (35.1) | 74.8 (33.1) | 0.97 |
| Male | 70.3 (23.9) | 95.6 (27.6) | 0.08 |
| Over 2 weeks | |||
| All | 73.2 (30.6) | 79.4 (33.0) | 0.53 |
| Female | 74.0 (35.0) | 72.0 (33.2) | 0.88 |
| Male | 71.8 (22.6) | 95.6 (29.0) | 0.10 |
| Metabolic Equivalent Value: mean (SD) | |||
| All | 1.44 (0.2) | 1.50 (0.2) | 0.28 |
| Female | 1.44 (0.2) | 1.50 (0.2) | 0.40 |
| Male | 1.45 (0.1) | 1.50 (0.2) | 0.51 |
| Laboratory Values | All PT; n = 30 F/M 19/11 | FT; n = 16 F/M 11/5 | p-Value |
|---|---|---|---|
| S-25OHD: nmol/L, mean (SD) | |||
| All | 73.4 (28.4) | 56.9 (17.5) | 0.02 |
| Female | 69.6 (24.1) | 61.1 (16.7) | 0.27 |
| Male | 80.0 (34.9) | 47.8 (17.3) | 0.07 |
| Calcium: mmol/L, mean (SD) | |||
| All | 2.37 (0.08) | 2.33 (0.08) | 0.14 |
| Female | 2.35 (0.08) | 2.34 (0.09) | 0.82 |
| Male | 2.41 (0.06) | 2.31 (0.05) | 0.01 |
| Phosphorous: mmol/L, mean (SD) | |||
| All | 1.14 (0.28) | 1.23 (0.14) | 0.23 |
| Female | 1.12 (0.33) | 1.22 (0.13) | 0.36 |
| Male | 1.17 (0.14) | 1.24 (0.17) | 0.35 |
| Alkaline phosphatase: U/L, mean (SD) | |||
| All | 64.6 (13.1) | 68.1 (25.1) | 0.61 |
| Female | 59.2 (11.7) | 65.5 (22.2) | 0.32 |
| Male | 74.0 (9.8) | 74.0 (32.8) | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Björkman, K.; Valkama, M.; Bruun, E.; Pätsi, P.; Kulmala, P.; Tulppo, M.P.; Leskinen, M.; Ojaniemi, M. Heart Rate and Heart Rate Variability in Healthy Preterm-Born Young Adults and Association with Vitamin D: A Wearable Device Assessment. J. Clin. Med. 2023, 12, 7504. https://doi.org/10.3390/jcm12247504
Björkman K, Valkama M, Bruun E, Pätsi P, Kulmala P, Tulppo MP, Leskinen M, Ojaniemi M. Heart Rate and Heart Rate Variability in Healthy Preterm-Born Young Adults and Association with Vitamin D: A Wearable Device Assessment. Journal of Clinical Medicine. 2023; 12(24):7504. https://doi.org/10.3390/jcm12247504
Chicago/Turabian StyleBjörkman, Krista, Marita Valkama, Ella Bruun, Pauli Pätsi, Petri Kulmala, Mikko P. Tulppo, Markku Leskinen, and Marja Ojaniemi. 2023. "Heart Rate and Heart Rate Variability in Healthy Preterm-Born Young Adults and Association with Vitamin D: A Wearable Device Assessment" Journal of Clinical Medicine 12, no. 24: 7504. https://doi.org/10.3390/jcm12247504
APA StyleBjörkman, K., Valkama, M., Bruun, E., Pätsi, P., Kulmala, P., Tulppo, M. P., Leskinen, M., & Ojaniemi, M. (2023). Heart Rate and Heart Rate Variability in Healthy Preterm-Born Young Adults and Association with Vitamin D: A Wearable Device Assessment. Journal of Clinical Medicine, 12(24), 7504. https://doi.org/10.3390/jcm12247504