
Exercise Capacity and Clinical Outcomes in Chronic Heart Failure Patients with Mild Tricuspid Regurgitation
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
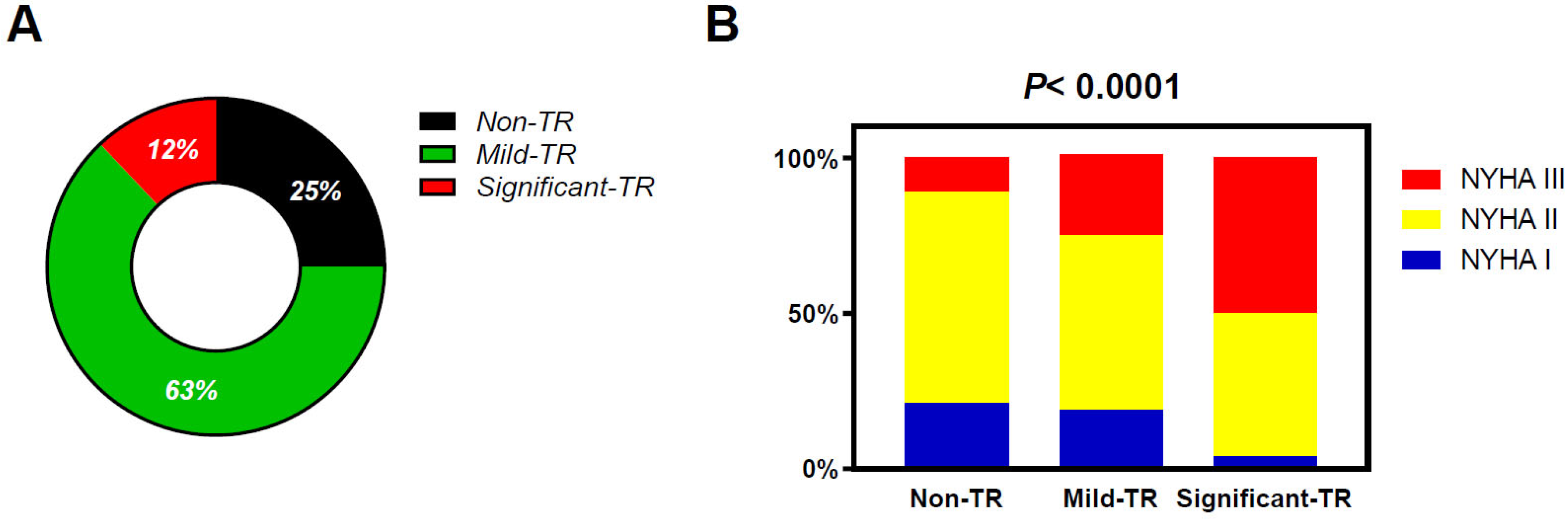
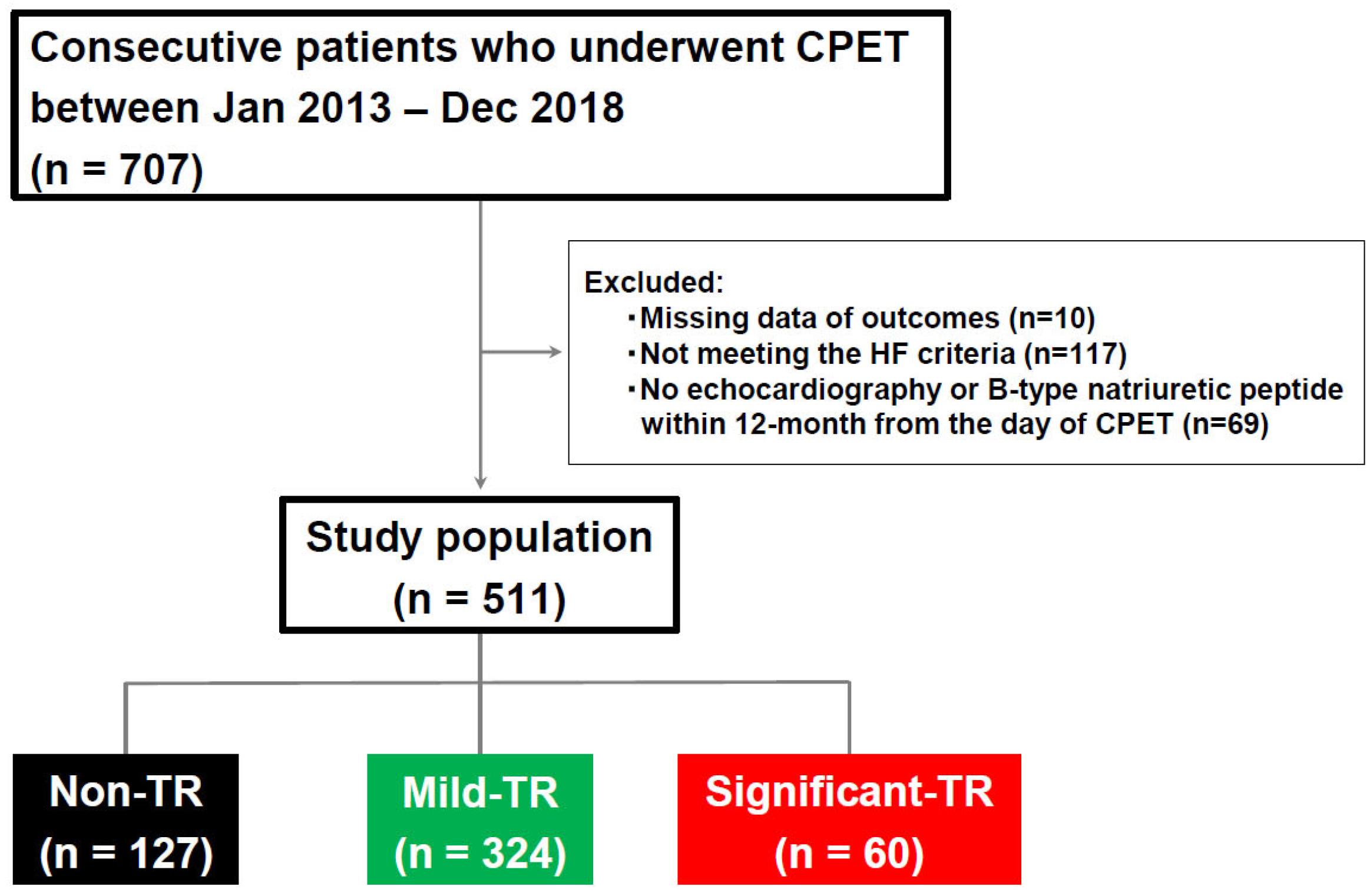
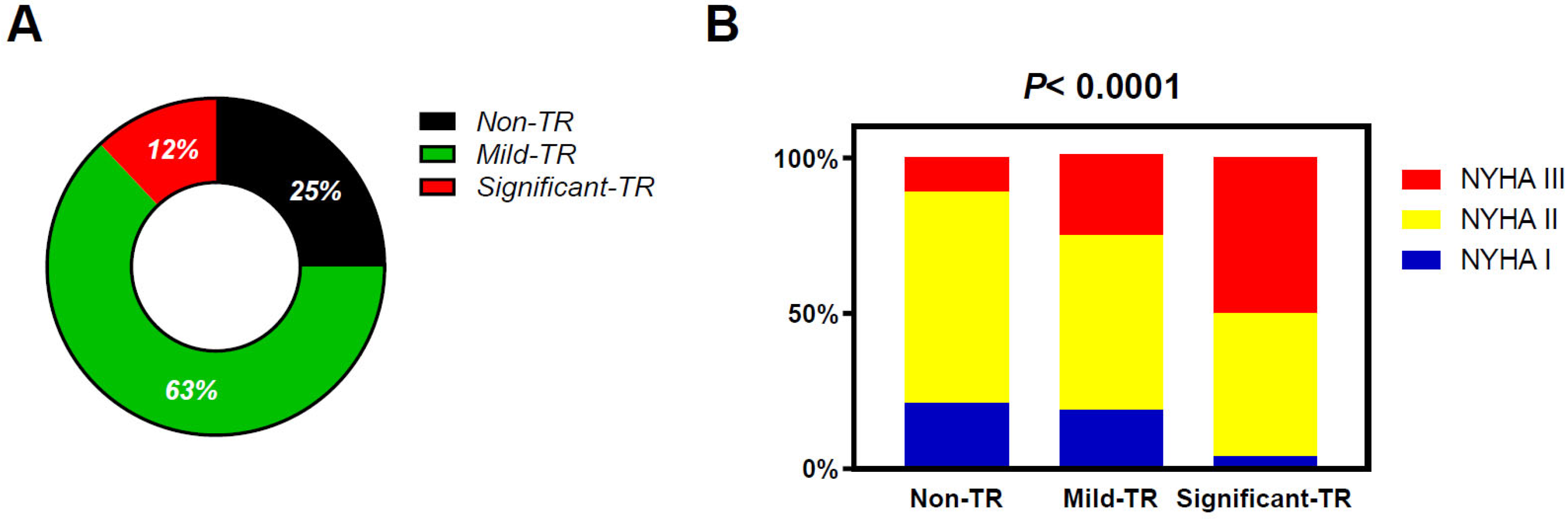
2.2. Study Population
2.3. Cardiopulmonary Exercise Testing
2.4. Cardiac Structure, Function, and Hemodynamics
2.5. Outcome Assessment
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Invasive Hemodynamics
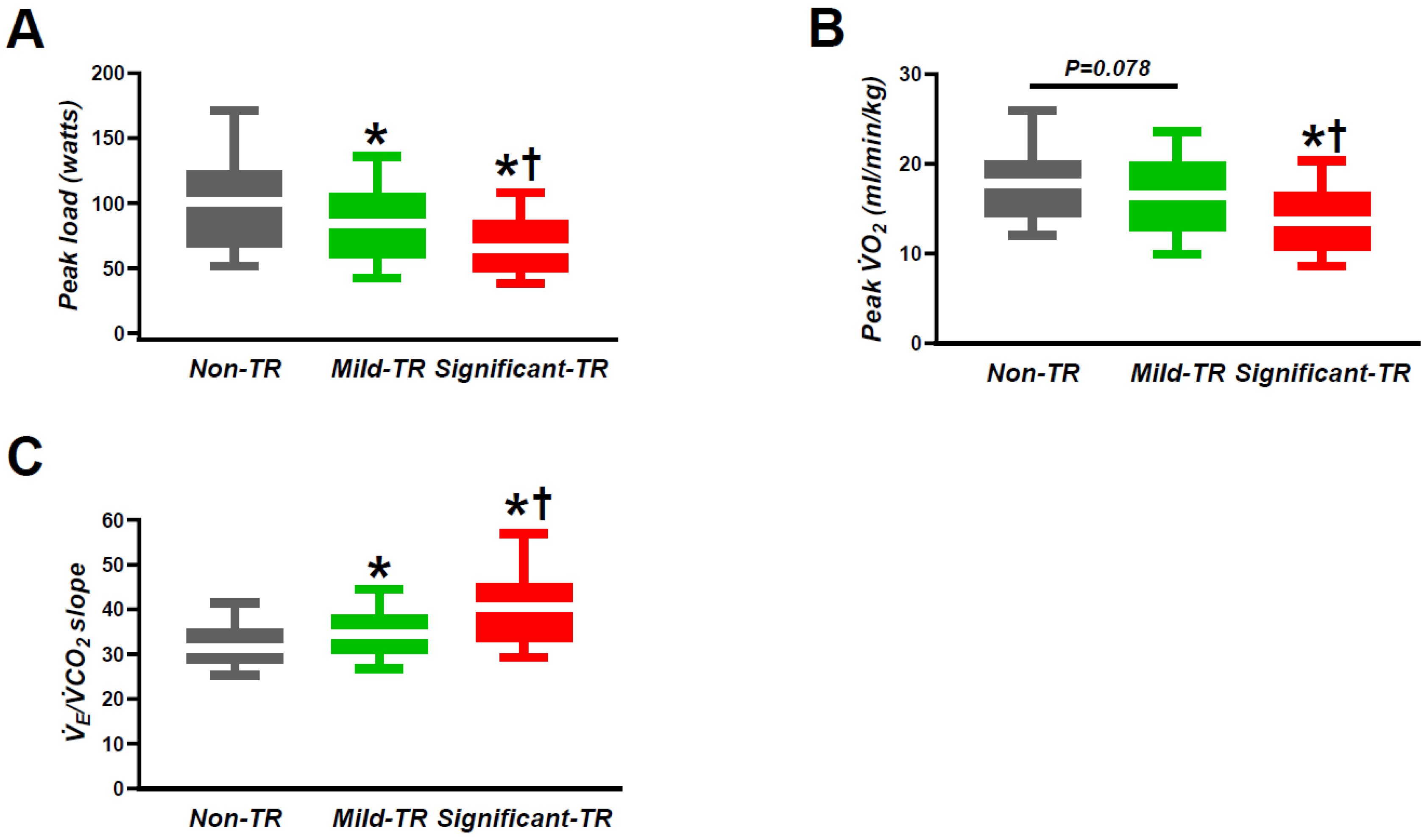
3.3. Cardiopulmonary Exercise Testing
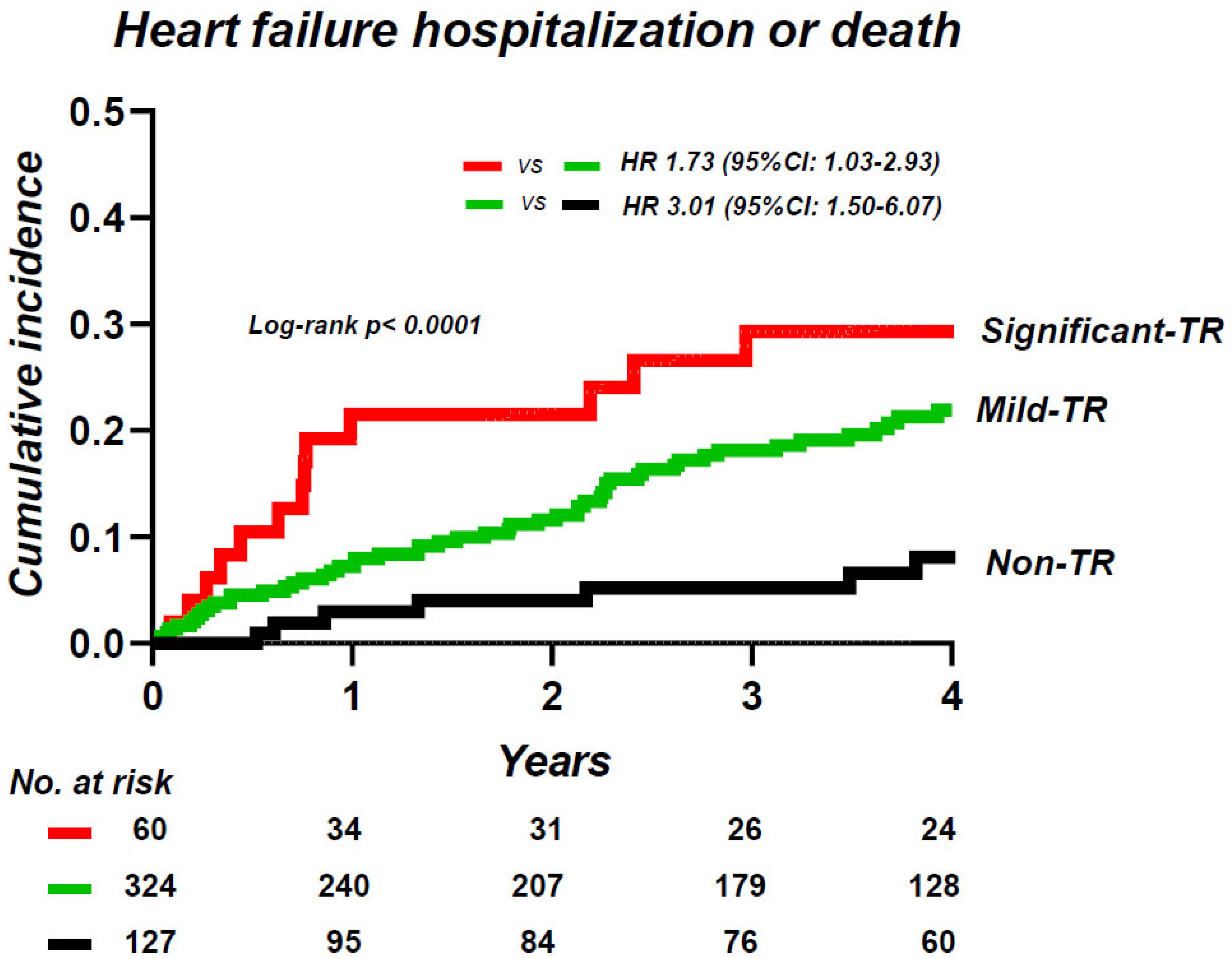
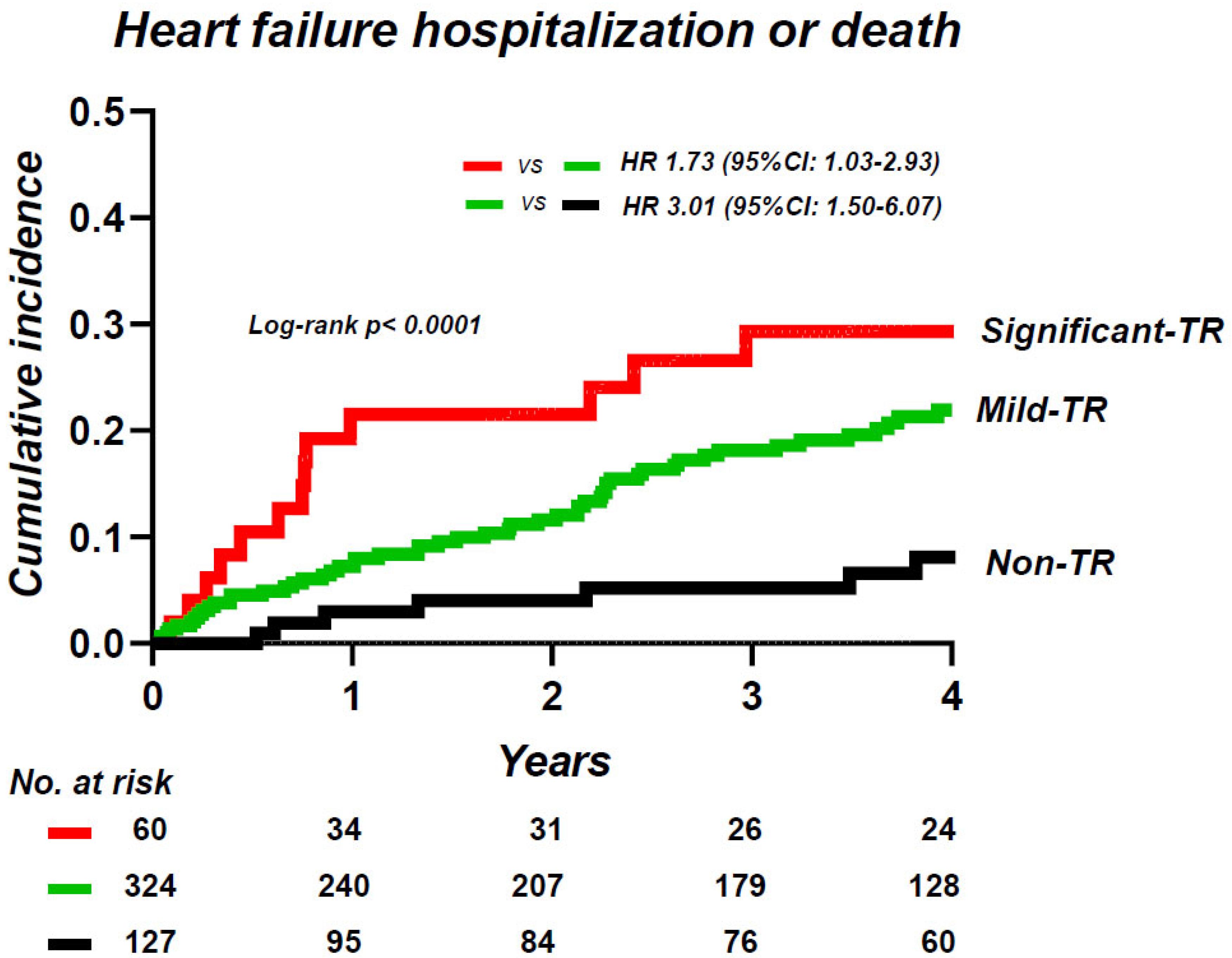
3.4. Tricuspid Regurgitation Severity and Clinical Outcomes
4. Discussion
4.1. Tricuspid Regurgitation in Chronic Heart Failure
4.2. Tricuspid Regurgitation and Functional Capacity
4.3. Tricuspid Regurgitation and Clinical Outcomes in Chronic Heart Failure
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akintoye, E.; Wang, T.K.M.; Nakhla, M.; Ali, A.H.; Fava, A.M.; Akyuz, K.; Popovic, Z.B.; Pettersson, G.B.; Gillinov, A.M.; Xu, B.; et al. Quantitative Echocardiographic Assessment and Optimal Criteria for Early Intervention in Asymptomatic Tricuspid Regurgitation. JACC. Cardiovasc. Imaging 2023, 16, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Bartko, P.E.; Arfsten, H.; Frey, M.K.; Heitzinger, G.; Pavo, N.; Cho, A.; Neuhold, S.; Tan, T.C.; Strunk, G.; Hengstenberg, C.; et al. Natural History of Functional Tricuspid Regurgitation: Implications of Quantitative Doppler Assessment. JACC. Cardiovasc. Imaging 2019, 12, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, M.; Vanermen, H.; Maisano, F.; Guidotti, A.; La Canna, G.; Alfieri, O. The growing clinical importance of secondary tricuspid regurgitation. J. Am. Coll. Cardiol. 2012, 59, 703–710. [Google Scholar] [CrossRef]
- Obokata, M.; Reddy, Y.N.V.; Melenovsky, V.; Pislaru, S.; Borlaug, B.A. Deterioration in right ventricular structure and function over time in patients with heart failure and preserved ejection fraction. Eur. Heart J. 2019, 40, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Harada, T.; Obokata, M.; Omote, K.; Iwano, H.; Ikoma, T.; Okada, K.; Yoshida, K.; Kato, T.; Kurosawa, K.; Nagai, T.; et al. Functional Tricuspid Regurgitation and Right Atrial Remodeling in Heart Failure With Preserved Ejection Fraction. Am. J. Cardiol. 2022, 162, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.J.; Nishimura, R.A.; Borlaug, B.A. The hemodynamic basis of exercise intolerance in tricuspid regurgitation. Circ. Heart Fail. 2014, 7, 911–917. [Google Scholar] [CrossRef]
- Amano, M.; Izumi, C.; Taniguchi, T.; Morimoto, T.; Miyake, M.; Nishimura, S.; Kitai, T.; Kato, T.; Kadota, K.; Ando, K.; et al. Impact of concomitant tricuspid regurgitation on long-term outcomes in severe aortic stenosis. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 353–360. [Google Scholar] [CrossRef]
- Chen, L.; Larsen, C.M.; Le, R.J.; Connolly, H.M.; Pislaru, S.V.; Murphy, J.G.; McGoon, M.D.; Frantz, R.P.; Kane, G.C. The prognostic significance of tricuspid valve regurgitation in pulmonary arterial hypertension. Clin. Respir. J. 2018, 12, 1572–1580. [Google Scholar] [CrossRef]
- Maeder, M.T.; Holst, D.P.; Kaye, D.M. Tricuspid regurgitation contributes to renal dysfunction in patients with heart failure. J. Card. Fail. 2008, 14, 824–830. [Google Scholar] [CrossRef]
- Nath, J.; Foster, E.; Heidenreich, P.A. Impact of tricuspid regurgitation on long-term survival. J. Am. Coll. Cardiol. 2004, 43, 405–409. [Google Scholar] [CrossRef]
- Nishi, H.; Takahashi, T.; Matsumiya, G.; Takano, H.; Ichikawa, H.; Miyagawa, S.; Sawa, Y. Preoperative assessment of congestive liver dysfunction using technetium-99 m galactosyl human serum albumin liver scintigraphy in patients with severe valvular heart disease. Surg. Today 2007, 37, 564–569. [Google Scholar] [CrossRef]
- Offen, S.; Playford, D.; Strange, G.; Stewart, S.; Celermajer, D.S. Adverse Prognostic Impact of Even Mild or Moderate Tricuspid Regurgitation: Insights from the National Echocardiography Database of Australia. J. Am. Soc. Echocardiogr. 2022, 35, 810–817. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef] [PubMed]
- Shimono, Y.; Ishizaka, S.; Omote, K.; Nakamura, K.; Yasui, Y.; Mizuguchi, Y.; Takenaka, S.; Aoyagi, H.; Tamaki, Y.; Sato, T.; et al. Impact of Cardiac Power Output on Exercise Capacity and Clinical Outcome in Patients With Chronic Heart Failure. Am. J. Cardiol. 2023, 206, 4–11. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Gorter, T.M.; Obokata, M.; Reddy, Y.N.V.; Melenovsky, V.; Borlaug, B.A. Exercise unmasks distinct pathophysiologic features in heart failure with preserved ejection fraction and pulmonary vascular disease. Eur. Heart J. 2018, 39, 2825–2835. [Google Scholar] [CrossRef]
- Borlaug, B.A.; Reddy, Y.N.V. The Role of the Pericardium in Heart Failure: Implications for Pathophysiology and Treatment. JACC Heart Fail. 2019, 7, 574–585. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; Obokata, M.; Verbrugge, F.H.; Lin, G.; Borlaug, B.A. Atrial Dysfunction in Patients With Heart Failure With Preserved Ejection Fraction and Atrial Fibrillation. J. Am. Coll. Cardiol. 2020, 76, 1051–1064. [Google Scholar] [CrossRef]
- Borlaug, B.A.; Carter, R.E.; Melenovsky, V.; DeSimone, C.V.; Gaba, P.; Killu, A.; Naksuk, N.; Lerman, L.; Asirvatham, S.J. Percutaneous Pericardial Resection: A Novel Potential Treatment for Heart Failure With Preserved Ejection Fraction. Circ. Heart Fail. 2017, 10, e003612. [Google Scholar] [CrossRef]
- Borlaug, B.A.; Schaff, H.V.; Pochettino, A.; Pedrotty, D.M.; Asirvatham, S.J.; Abel, M.D.; Carter, R.E.; Mauermann, W.J. Pericardiotomy Enhances Left Ventricular Diastolic Reserve with Volume Loading in Humans. Circulation 2018, 138, 2295–2297. [Google Scholar] [CrossRef] [PubMed]
- Obokata, M.; Reddy, Y.N.V.; Pislaru, S.V.; Melenovsky, V.; Borlaug, B.A. Evidence Supporting the Existence of a Distinct Obese Phenotype of Heart Failure with Preserved Ejection Fraction. Circulation 2017, 136, 6–19. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-TR (n = 127) | Mild TR (n = 324) | Significant TR (n = 60) | p-Value | |
|---|---|---|---|---|
| Age (years) | 53 ± 18 | 61 ± 15 * | 60 ± 16 * | <0.0001 |
| Women, n (%) | 34 (27%) | 101 (31%) | 23 (38%) | 0.28 |
| Body mass index (kg/m2) | 24.2 ± 4.9 | 22.8 ± 3.5 * | 22.2 ± 4.0 * | 0.014 |
| Underlying heart disease | ||||
| DCM | 29 (23%) | 64 (20%) | 12 (20%) | 0.77 |
| HCM | 9 (7%) | 36 (11%) | 2 (3%) | 0.07 |
| HHD | 13 (10%) | 24 (7%) | 2 (3%) | 0.21 |
| IHD | 34 (27%) | 72 (22%) | 6 (10%) *† | 0.02 |
| Left side of valvular heart disease | 21 (17%) | 43 (13%) | 8 (13%) | 0.67 |
| Others | 21 (17%) | 85 (26%) | 30 (50%) *† | <0.0001 |
| Comorbidities, n (%) | ||||
| Coronary disease | 24 (20%) | 64 (20%) | 6 (10%) | 0.20 |
| Diabetes mellitus | 29 (23%) | 75 (23%) | 13 (22%) | 0.084 |
| Hypertension | 62 (49%) | 137 (42%) | 19 (32%) | 0.97 |
| Atrial fibrillation | 15 (12%) | 88 (27%) | 26 (43%) | <0.0001 |
| Medications, n (%) | ||||
| Renin-angiotensin system blocker | 98 (77%) | 252 (78%) | 52 (41%) | 0.098 |
| Beta-Blocker | 93 (73%) | 254 (78%) | 37 (62%) | 0.019 |
| Loop | 52 (41%) | 150 (46%) | 45 (75%) | <0.0001 |
| Laboratories | ||||
| Hemoglobin (g/dL) | 13.7 ± 1.7 | 13.5 ± 4.9 | 12.9 ± 2.0 * | 0.014 |
| Estimated GFR (mL/min/1.73m2) | 71 ± 27 | 64 ± 24 * | 62 ± 24 * | 0.004 |
| BNP (pg/mL) | 69.2 (37.7, 184) | 126 (59.2, 246) * | 146 (80, 402) *† | <0.0001 |
| Echocardiography | ||||
| LV diastolic dimension (mm) | 57 ± 10 | 57 ± 11 | 53 ± 13 *† | 0.033 |
| LV systolic dimension (mm) | 44 ± 13 | 45 ± 15 | 41 ± 16 | 0.089 |
| LV mass index (g/m2) | 127 ± 49 | 124 ± 39 | 108 ± 42 *† | 0.001 |
| LA volume index (mL/m2) | 40 ± 14 | 52 ± 23 * | 68 ± 29 *† | <0.0001 |
| LVEF (%) | 44 ± 15 | 42 ± 16 | 43 ± 19 | 0.59 |
| E/e’ | 10 (7, 12) | 10 (8, 13) | 10 (8, 15) | 0.31 |
| TAPSE (mm) | 17 ± 5 | 16 ± 5 | 16 ± 5 | 0.18 |
| RV basal diameter (mm) | 39 ± 6 | 43 ± 6 * | 49 ± 7 *† | <0.0001 |
| RV mid-diameter (mm) | 28 ± 4 | 32 ± 6 * | 37 ± 7 *† | <0.0001 |
| TR velocity (m/s) | 2.3 ± 0.6 | 2.5 ± 0.4 * | 3.2 ± 0.8 *† | <0.0001 |
| Secondary TR | - | 242 (75%) | 39 (65%) | 0.12 |
| Moderate or greater mitral regurgitation | 15 (12%) | 78 (24%) | 23 (38%) | 0.0002 |
| Moderate or greater aortic regurgitation | 13 (10%) | 24 (7%) | 1 (2%) *† | 0.04 |
| Heart failure classification according to LVEF | 0.36 | |||
| HFrEF | 62 (49%) | 169 (52%) | 28 (47%) | |
| HFmrEF | 22 (17%) | 54 (17%) | 6 (10%) | |
| HFpEF | 43 (34%) | 101 (31%) | 26 (43%) | |
| Invasive hemodynamics, n = 304 | ||||
| Heart rate (bpm) | 66 ± 13 | 67 ± 13 | 69 ± 15 | 0.69 |
| Systolic BP (mm Hg) | 123 ± 24 | 113 ± 23 * | 108 ± 22 * | 0.005 |
| RAP (mm Hg) | 7 ± 4 | 6 ± 3 | 10 ± 6 *† | 0.040 |
| PA systolic pressure (mm Hg) | 30 ± 12 | 30 ± 11 | 42 ± 20 *† | 0.0005 |
| PA mean pressure (mm Hg) | 20 ± 10 | 20 ± 8 | 26 ± 12 *† | 0.002 |
| PCWP (mm Hg) | 11 ± 6 | 13 ± 7 | 14 ± 8 | 0.16 |
| PVR (WU) | 1.5 (1.2, 1.9) | 1.7 (1.2, 2.4) | 1.8 (1.3, 2.3) | 0.078 |
| PAC (mL/mm Hg) | 5.4 ± 2.1 | 4.5 ± 2.3 * | 3.0 ± 1.5 *† | <0.0001 |
| PA Ea (mm Hg/mL) | 0.4 ± 0.2 | 0.5 ± 0.2 * | 0.7 ± 0.4 *† | <0.0001 |
| CO (L/min) | 4.8 ± 1.3 | 4.1 ± 1.1 * | 4.0 ± 1.2 * | 0.0003 |
| Non-TR (n = 127) | Mild TR (n = 324) | Significant TR (n = 60) | p-Value | |
|---|---|---|---|---|
| Resting heart rate (bpm) | 72 ± 13 | 70 ± 14 | 72 ± 15 | 0.37 |
| Peak heart rate (bpm) | 127 ± 29 | 119 ± 29 | 115 ± 30 *† | 0.013 |
| Resting systolic BP (mmHg) | 118 ± 21 | 115 ± 21 | 108 ± 20 * | 0.014 |
| Peak systolic BP (mmHg) | 166 ± 34 | 158 ± 36 | 142 ± 38 *† | <0.0001 |
| Peak VO2 (mL/min/kg) | 18.2 ± 5.7 | 16.9 ± 5.8 | 14.1 ± 4.9 *† | <0.0001 |
| VE/VCO2 | 32.6 ± 6.6 | 35.0 ± 7.3 * | 40.1 ± 10.5 *† | <0.0001 |
| O2 pulse | 9.8 ± 4.8 | 8.9 ± 3.2 | 7.3 ± 2.4 *† | <0.0001 |
| Anaerobic threshold (ml/min/kg) | 10.7 ± 2.9 | 10.4 ± 2.6 | 9.3 ± 2.6 *† | 0.004 |
| Peak load (Watts) | 101 ± 43 | 88 ± 41 * | 69 ± 33 *† | <0.0001 |
| Peak RER | 1.24 ± 0.14 | 1.24 ± 0.13 | 1.27 ± 0.14 | 0.42 |
| Variables | Univariable Analysis | Multivariable Analysis * | ||
|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| TR Mild vs. Non | 3.01 (1.50–6.07) | 0.002 | 2.97 (1.35–6.55) | 0.007 |
| TR Significant vs. Mild | 1.73 (1.03–2.93) | 0.040 | 2.04 (1.13–3.67) | 0.018 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, K.; Ishizaka, S.; Omote, K.; Yasui, Y.; Mizuguchi, Y.; Takenaka, S.; Shimono, Y.; Motoi, K.; Aoyagi, H.; Tamaki, Y.; et al. Exercise Capacity and Clinical Outcomes in Chronic Heart Failure Patients with Mild Tricuspid Regurgitation. J. Clin. Med. 2023, 12, 7459. https://doi.org/10.3390/jcm12237459
Nakamura K, Ishizaka S, Omote K, Yasui Y, Mizuguchi Y, Takenaka S, Shimono Y, Motoi K, Aoyagi H, Tamaki Y, et al. Exercise Capacity and Clinical Outcomes in Chronic Heart Failure Patients with Mild Tricuspid Regurgitation. Journal of Clinical Medicine. 2023; 12(23):7459. https://doi.org/10.3390/jcm12237459
Chicago/Turabian StyleNakamura, Kosuke, Suguru Ishizaka, Kazunori Omote, Yutaro Yasui, Yoshifumi Mizuguchi, Sakae Takenaka, Yui Shimono, Ko Motoi, Hiroyuki Aoyagi, Yoji Tamaki, and et al. 2023. "Exercise Capacity and Clinical Outcomes in Chronic Heart Failure Patients with Mild Tricuspid Regurgitation" Journal of Clinical Medicine 12, no. 23: 7459. https://doi.org/10.3390/jcm12237459
APA StyleNakamura, K., Ishizaka, S., Omote, K., Yasui, Y., Mizuguchi, Y., Takenaka, S., Shimono, Y., Motoi, K., Aoyagi, H., Tamaki, Y., Kazui, S., Takahashi, Y., Saiin, K., Naito, S., Tada, A., Kobayashi, Y., Sato, T., Kamiya, K., Nagai, T., & Anzai, T. (2023). Exercise Capacity and Clinical Outcomes in Chronic Heart Failure Patients with Mild Tricuspid Regurgitation. Journal of Clinical Medicine, 12(23), 7459. https://doi.org/10.3390/jcm12237459