

The Prevalence of Pain in Chronic Diseases: An Umbrella Review of Systematic Reviews

Abstract
:
1. Introduction
2. Materials and Methods
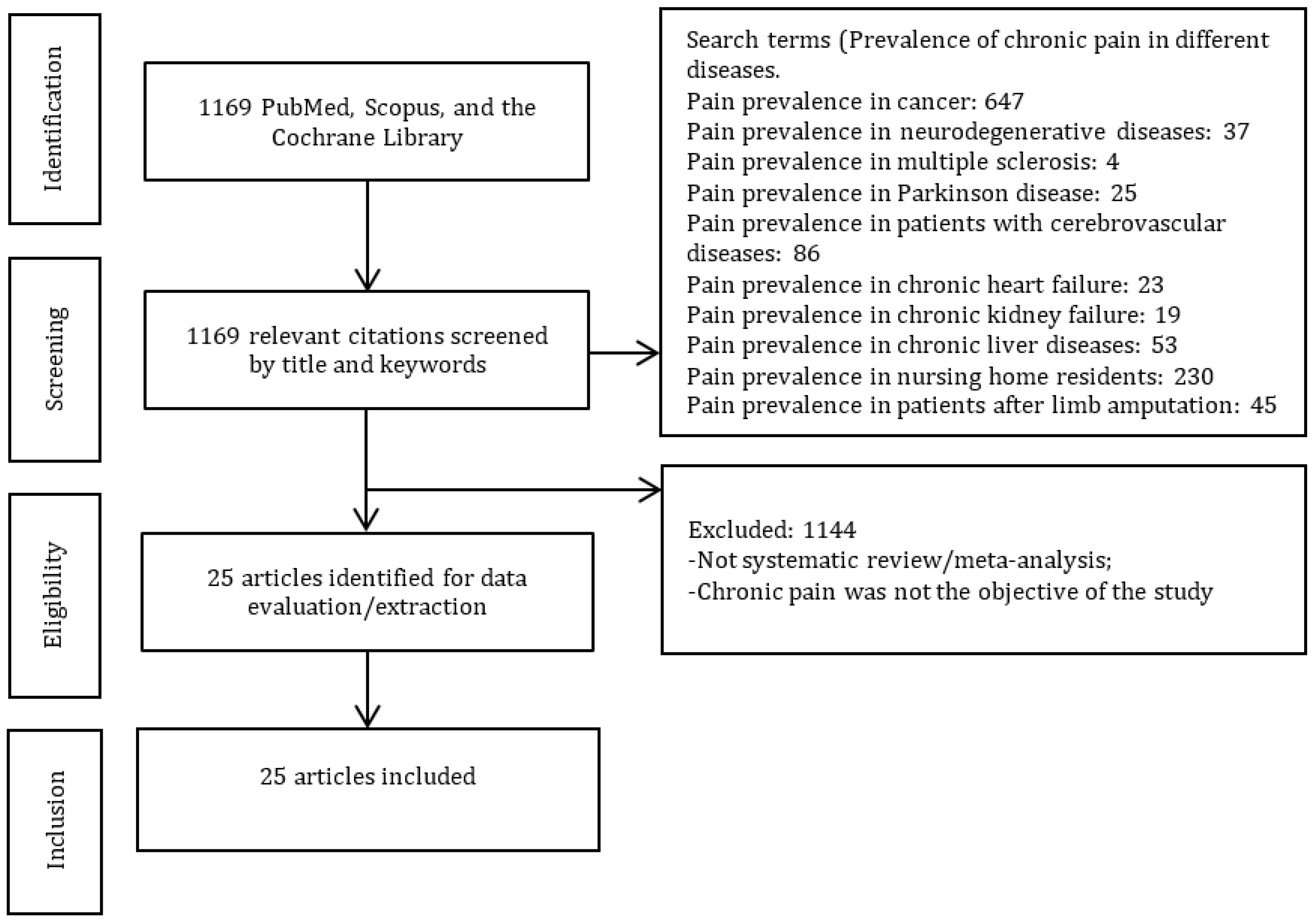
Search Strategy and Selection Criteria
- Systematic reviews and meta-analyses focused on the prevalence of pain;
- Studies published in peer-reviewed journals;
- When more than five systematic reviews were available, we included the five most recent ones.
3. Results
3.1. Patient Characteristics
3.1.1. Diseases/Conditions
3.1.2. Countries (Where the Included Studies Were Conducted/Data Collected)
3.2. Quality Assessment
3.3. Prevalence of Chronic Pain in Different Diseases/Conditions
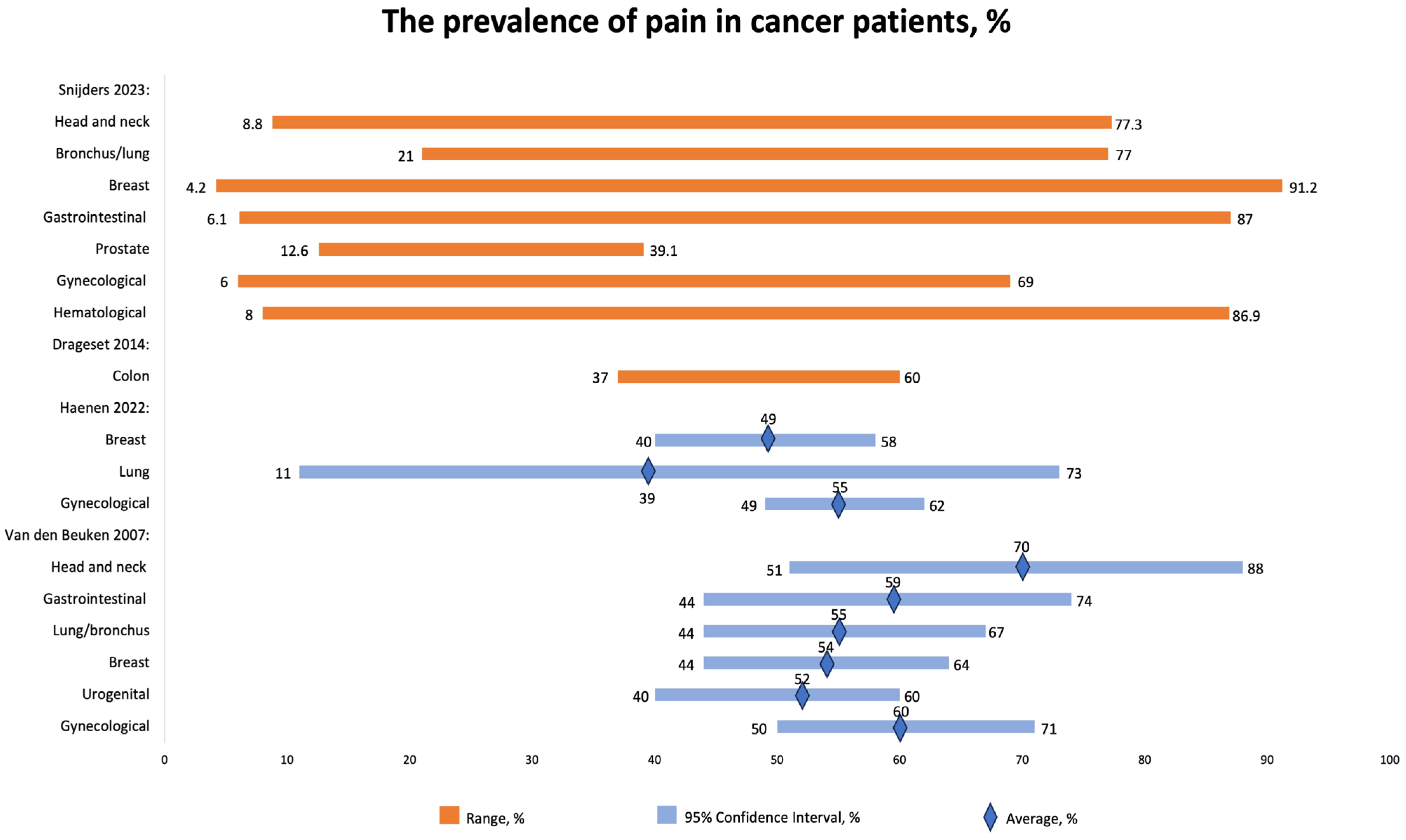
3.3.1. Prevalence of Chronic Pain in Cancer Patients
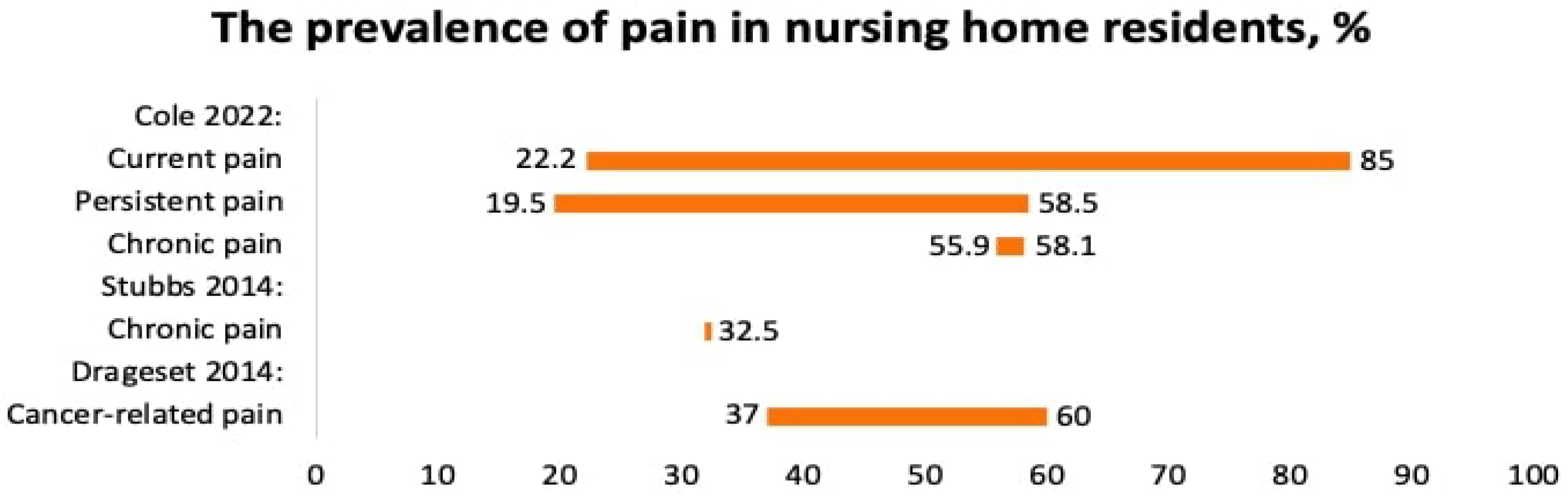
3.3.2. Prevalence of Pain in Nursing Home Residents
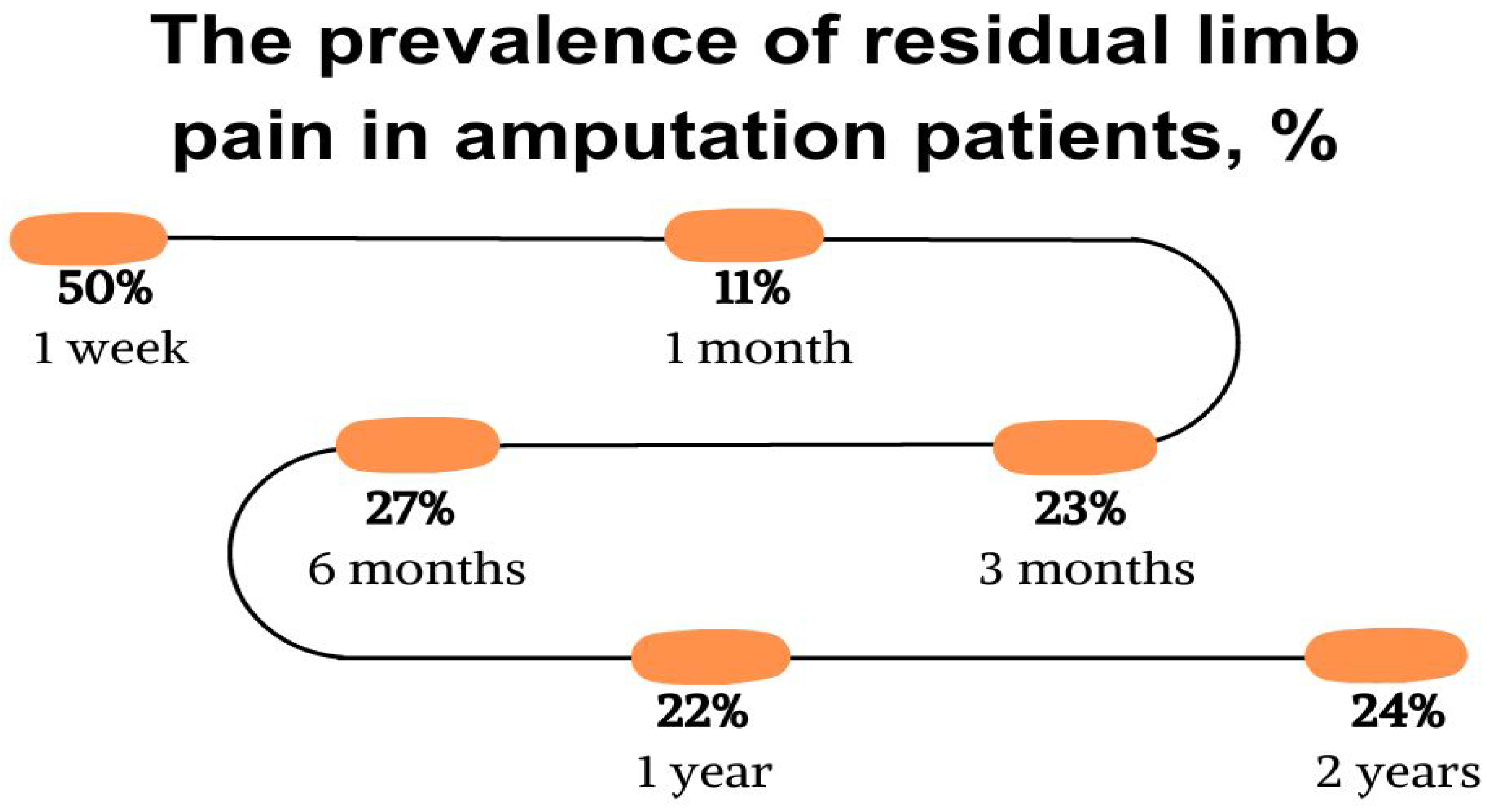
3.3.3. Residual Limb Pain after Amputation
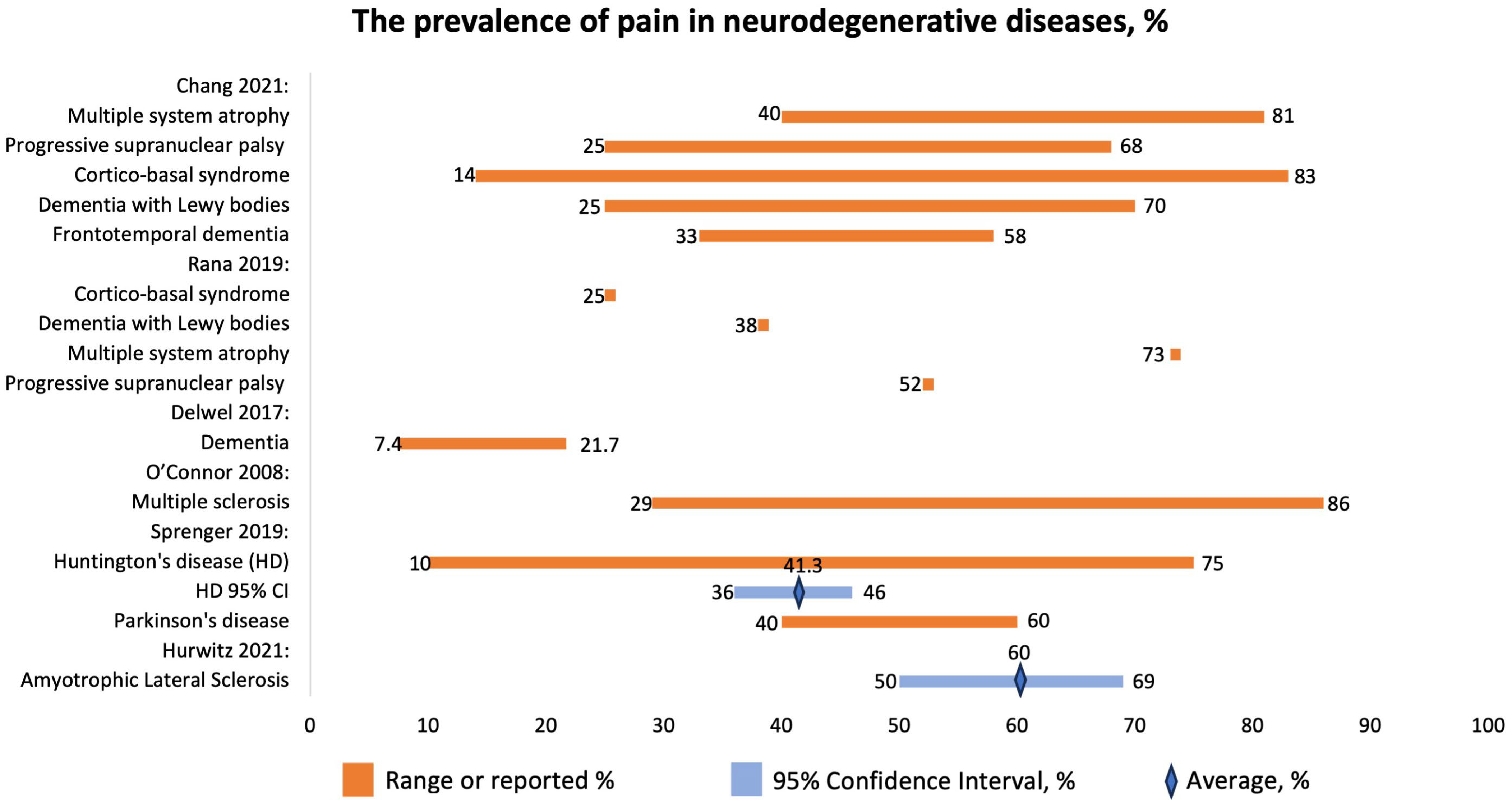
3.3.4. Prevalence of Pain in Patients with Neurodegenerative Diseases
- MSA: neck, back, limbs; MSK, neuropathic, dystonic;
- PSP: limbs, neck, back, MSK;
- CBS: limbs, dystonic;
- DLB: multiple places, neuropathic, MSK;
- FTD: head, neck, shoulder, abdomen, MSK.
Characteristics of Pain
3.3.5. Prevalence of Pain in Chronic Heart Failure Patients
3.3.6. Prevalence of Pain in COPD
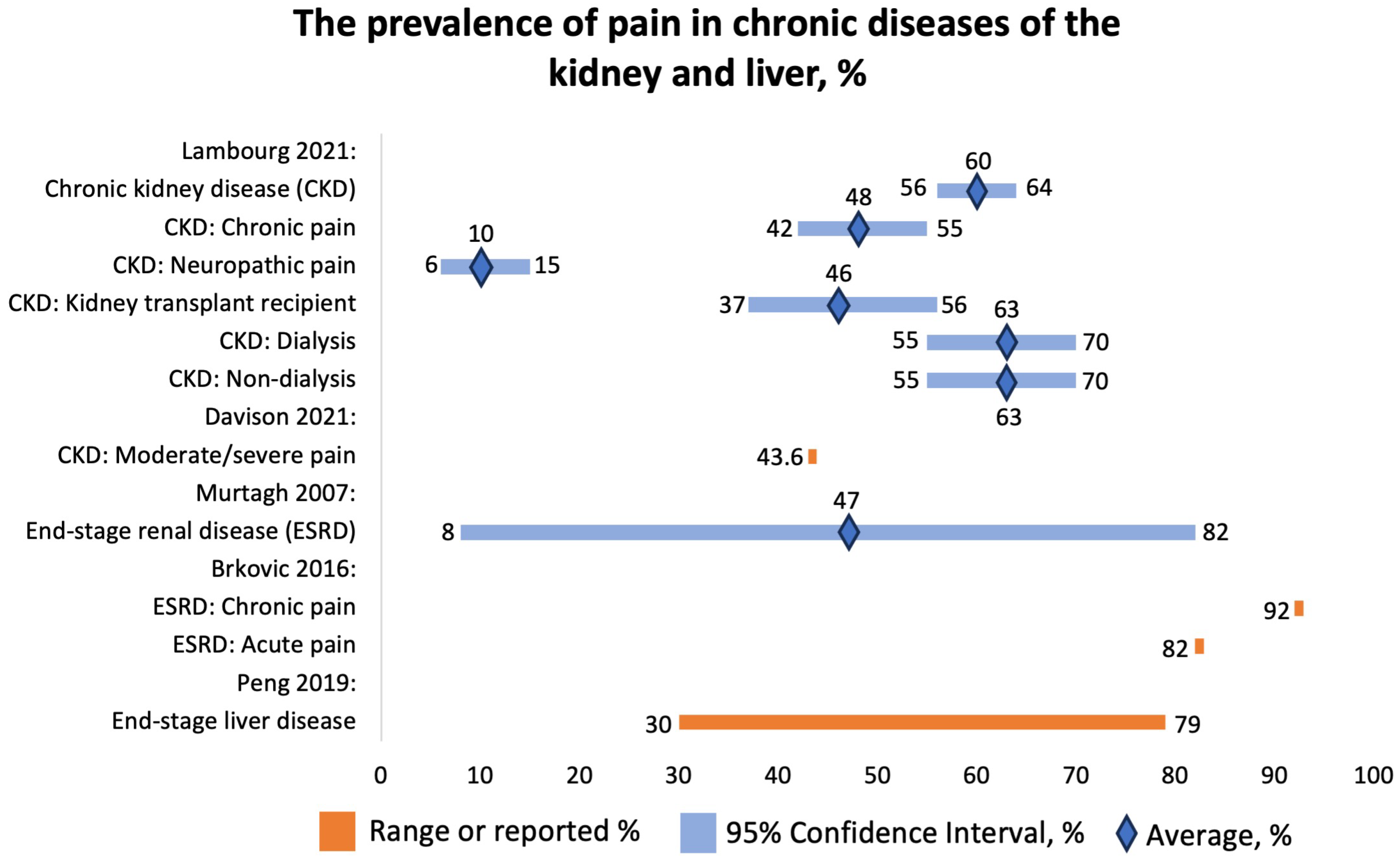
3.3.7. Prevalence of Pain in Chronic Kidney Diseases
3.3.8. Prevalence of Pain in Patients with Liver Diseases
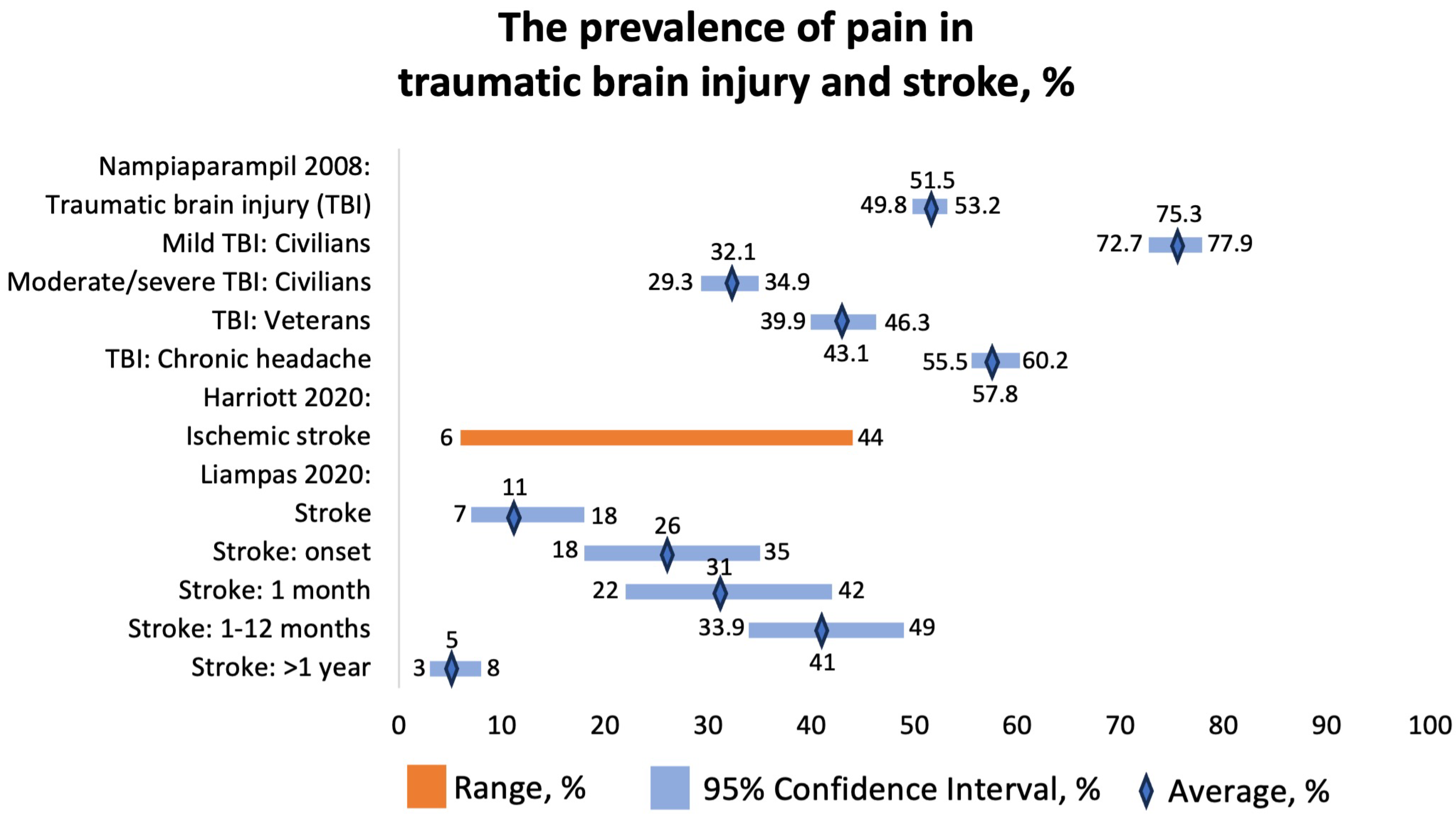
3.3.9. Prevalence of Pain in Patients with Traumatic Brain Injury (TBI)
3.3.10. Prevalence of Pain in Cerebrovascular Diseases
4. Discussion
4.1. Brief Summary
4.2. Limitations
4.2.1. Nursing Home Residents
4.2.2. Postamputation Pain
4.2.3. Neurodegenerative Diseases
4.2.4. COPD
4.2.5. CKD
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schappert, S.M.; Burt, C.W. Ambulatory Care Visits to Physician Offices, Hospital Outpatient Departments, and Emergency Departments: United States, 2001–2002. Vital Health Stat. Ser. 13 Data Natl. Health Surv. 2006, 159, 1–66. [Google Scholar]
- Gureje, O.; Von Korff, M.; Simon, G.E.; Gater, R. Persistent Pain and Well-Being: A World Health Organization Study in Primary Care. JAMA 1998, 280, 147. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.H.; Elliott, A.M.; Chambers, W.A.; Smith, W.C.; Hannaford, P.C.; Penny, K. The Impact of Chronic Pain in the Community. Fam. Pract. 2001, 18, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research; The National Academies Collection: Reports Funded by National Institutes of Health; National Academies Press (US): Washington, DC, USA, 2011; ISBN 978-0-309-21484-1. [Google Scholar]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic Pain as a Symptom or a Disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef]
- Interagency Pain Research Coordinating Committee. National Pain Strategy: A Comprehensive Population Health-Level Strategy for Pain; US Department of Health and Human Services: Washington, DC, USA; National Institutes of Health: Washington, DC, USA, 2016.
- Cramer, J.D.; Johnson, J.T.; Nilsen, M.L. Pain in Head and Neck Cancer Survivors: Prevalence, Predictors, and Quality-of-Life Impact. Otolaryngol. Head Neck Surg. 2018, 159, 853–858. [Google Scholar] [CrossRef]
- Kroenke, K.; Theobald, D.; Wu, J.; Loza, J.K.; Carpenter, J.S.; Tu, W. The Association of Depression and Pain with Health-Related Quality of Life, Disability, and Health Care Use in Cancer Patients. J. Pain Symptom Manag. 2010, 40, 327–341. [Google Scholar] [CrossRef]
- Lin, C.-C.; Lai, Y.-L.; Ward, S.E. Effect of Cancer Pain on Performance Status, Mood States, and Level of Hope among Taiwanese Cancer Patients. J. Pain Symptom Manag. 2003, 25, 29–37. [Google Scholar] [CrossRef]
- Strang, P. Cancer Pain—A Provoker of Emotional, Social and Existential Distress. Acta Oncol. 1998, 37, 641–644. [Google Scholar] [CrossRef]
- Kwon, J.H. Overcoming Barriers in Cancer Pain Management. J. Clin. Oncol. 2014, 32, 1727–1733. [Google Scholar] [CrossRef]
- Mercadante, S.; Adile, C.; Tirelli, W.; Ferrera, P.; Penco, I.; Casuccio, A. Barriers and Adherence to Pain Management in Advanced Cancer Patients. Pain Pract. 2021, 21, 388–393. [Google Scholar] [CrossRef]
- Stoorvogel, H.; van Haastregt, J.; Theunissen, M.; Schoenmaekers, J.; Hoeben, A.; van den Beuken-van Everdingen, M. Unacceptable Pain in Oncology: The Patients’ Perspective on Reasons for Absence of Pain Interventions. Eur. J. Cancer Care 2022, 31, e13628. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Snijders, R.A.H.; Brom, L.; Theunissen, M.; van den Beuken-van Everdingen, M.H.J. Update on Prevalence of Pain in Patients with Cancer 2022: A Systematic Literature Review and Meta-Analysis. Cancers 2023, 15, 591. [Google Scholar] [CrossRef] [PubMed]
- Haenen, V.; Evenepoel, M.; De Baerdemaecker, T.; Meeus, M.; Devoogdt, N.; Morlion, B.; Dams, L.; Van Dijck, S.; Van der Gucht, E.; De Vrieze, T.; et al. Pain Prevalence and Characteristics in Survivors of Solid Cancers: A Systematic Review and Meta-Analysis. Support. Care Cancer 2022, 31, 85. [Google Scholar] [CrossRef] [PubMed]
- Cole, C.S.; Carpenter, J.S.; Chen, C.X.; Blackburn, J.; Hickman, S.E. Prevalence and Factors Associated with Pain in Nursing Home Residents: A Systematic Review of the Literature. J. Am. Med. Dir. Assoc. 2022, 23, 1916–1925.e1. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.G.; Chaker, S.C.; Curran, G.E.; Downer, M.A.; Assi, P.E.; Joseph, J.T.; Kassis, S.A.; Thayer, W.P. Postamputation Residual Limb Pain Severity and Prevalence: A Systematic Review and Meta-Analysis. Plast. Surg. 2022, 30, 254–268. [Google Scholar] [CrossRef]
- Hurwitz, N.; Radakovic, R.; Boyce, E.; Peryer, G. Prevalence of Pain in Amyotrophic Lateral Sclerosis: A Systematic Review and Meta-Analysis. Amyotroph. Lateral Scler. Front. Degener. 2021, 22, 449–458. [Google Scholar] [CrossRef]
- Innes, K.E.; Sambamoorthi, U. The Potential Contribution of Chronic Pain and Common Chronic Pain Conditions to Subsequent Cognitive Decline, New Onset Cognitive Impairment, and Incident Dementia: A Systematic Review and Conceptual Model for Future Research. J. Alzheimers Dis. 2020, 78, 1177–1195. [Google Scholar] [CrossRef]
- Chang, J.Y.; Rukavina, K.; Lawn, T.; Chaudhuri, K.R. Pain in Neurodegenerative Diseases with Atypical Parkinsonism: A Systematic Review on Prevalence, Clinical Presentation, and Findings from Experimental Studies. J. Integr. Neurosci. 2021, 20, 1067–1078. [Google Scholar] [CrossRef] [PubMed]
- Sprenger, G.P.; van der Zwaan, K.F.; Roos, R.A.C.; Achterberg, W.P. The Prevalence and the Burden of Pain in Patients with Huntington Disease: A Systematic Review and Meta-Analysis. Pain 2019, 160, 773–783. [Google Scholar] [CrossRef]
- Rana, A.Q.; Qureshi, A.R.; Siddiqui, O.; Sarfraz, Z.; Rana, R.; Shtilbans, A. Prevalence of Pain in Atypical Parkinsonism: A Systematic Review and Meta-Analysis. J. Neurol. 2019, 266, 2093–2102. [Google Scholar] [CrossRef] [PubMed]
- Delwel, S.; Binnekade, T.T.; Perez, R.S.G.M.; Hertogh, C.M.P.M.; Scherder, E.J.A.; Lobbezoo, F. Oral Health and Orofacial Pain in Older People with Dementia: A Systematic Review with Focus on Dental Hard Tissues. Clin. Oral Investig. 2017, 21, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Drageset, J.; Corbett, A.; Selbaek, G.; Husebo, B.S. Cancer-Related Pain and Symptoms among Nursing Home Residents: A Systematic Review. J. Pain Symptom Manag. 2014, 48, 699–710.e1. [Google Scholar] [CrossRef]
- Stubbs, B.; Binnekade, T.; Eggermont, L.; Sepehry, A.A.; Patchay, S.; Schofield, P. Pain and the Risk for Falls in Community-Dwelling Older Adults: Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2014, 95, 175–187.e9. [Google Scholar] [CrossRef] [PubMed]
- Alemzadeh-Ansari, M.J.; Ansari-Ramandi, M.M.; Naderi, N. Chronic Pain in Chronic Heart Failure: A Review Article. J. Tehran Univ. Heart Cent. 2017, 12, 49–56. [Google Scholar]
- Van Dam van Isselt, E.F.; Groenewegen-Sipkema, K.H.; Spruit-van Eijk, M.; Chavannes, N.H.; de Waal, M.W.M.; Janssen, D.J.A.; Achterberg, W.P. Pain in Patients with COPD: A Systematic Review and Meta-Analysis. BMJ Open 2014, 4, e005898. [Google Scholar] [CrossRef]
- Lee, A.L.; Harrison, S.L.; Goldstein, R.S.; Brooks, D. Pain and Its Clinical Associations in Individuals with COPD: A Systematic Review. Chest 2015, 147, 1246–1258. [Google Scholar] [CrossRef]
- Van den Beuken-van Everdingen, M.H.J.; de Rijke, J.M.; Kessels, A.G.; Schouten, H.C.; van Kleef, M.; Patijn, J. Prevalence of Pain in Patients with Cancer: A Systematic Review of the Past 40 Years. Ann. Oncol. 2007, 18, 1437–1449. [Google Scholar] [CrossRef]
- Davison, S.N.; Rathwell, S.; Ghosh, S.; George, C.; Pfister, T.; Dennett, L. The Prevalence and Severity of Chronic Pain in Patients With Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Can. J. Kidney Health Dis. 2021, 8, 205435812199399. [Google Scholar] [CrossRef]
- Lambourg, E.; Colvin, L.; Guthrie, G.; Murugan, K.; Lim, M.; Walker, H.; Boon, G.; Bell, S. The Prevalence of Pain among Patients with Chronic Kidney Disease Using Systematic Review and Meta-Analysis. Kidney Int. 2021, 100, 636–649. [Google Scholar] [CrossRef]
- Brkovic, T.; Burilovic, E.; Puljak, L. Prevalence and Severity of Pain in Adult End-Stage Renal Disease Patients on Chronic Intermittent Hemodialysis: A Systematic Review. Patient Prefer. Adherence 2016, 10, 1131–1150. [Google Scholar] [CrossRef]
- Murtagh, F.E.M.; Addington-Hall, J.; Higginson, I.J. The Prevalence of Symptoms in End-Stage Renal Disease: A Systematic Review. Adv. Chronic Kidney Dis. 2007, 14, 82–99. [Google Scholar] [CrossRef]
- Peng, J.-K.; Hepgul, N.; Higginson, I.J.; Gao, W. Symptom Prevalence and Quality of Life of Patients with End-Stage Liver Disease: A Systematic Review and Meta-Analysis. Palliat. Med. 2019, 33, 24–36. [Google Scholar] [CrossRef]
- Nampiaparampil, D.E. Prevalence of Chronic Pain after Traumatic Brain Injury: A Systematic Review. JAMA 2008, 300, 711–719. [Google Scholar] [CrossRef]
- Harriott, A.M.; Karakaya, F.; Ayata, C. Headache after Ischemic Stroke: A Systematic Review and Meta-Analysis. Neurology 2020, 94, e75–e86. [Google Scholar] [CrossRef]
- Liampas, A.; Velidakis, N.; Georgiou, T.; Vadalouca, A.; Varrassi, G.; Hadjigeorgiou, G.M.; Tsivgoulis, G.; Zis, P. Prevalence and Management Challenges in Central Post-Stroke Neuropathic Pain: A Systematic Review and Meta-Analysis. Adv. Ther. 2020, 37, 3278–3291. [Google Scholar] [CrossRef]
- O’Connor, A.B.; Schwid, S.R.; Herrmann, D.N.; Markman, J.D.; Dworkin, R.H. Pain Associated with Multiple Sclerosis: Systematic Review and Proposed Classification. Pain 2008, 137, 96–111. [Google Scholar] [CrossRef]
- Deng, G. Integrative Medicine Therapies for Pain Management in Cancer Patients. Cancer J. 2019, 25, 343–348. [Google Scholar] [CrossRef]
- Beckwée, D.; Bautmans, I.; Lefeber, N.; Lievens, P.; Scheerlinck, T.; Vaes, P. Effect of Transcutaneous Electric Nerve Stimulation on Pain after Total Knee Arthroplasty: A Blind Randomized Controlled Trial. J. Knee Surg. 2018, 31, 189–196. [Google Scholar] [CrossRef]
- Lalla, R.V.; Bowen, J.; Barasch, A.; Elting, L.; Epstein, J.; Keefe, D.M.; McGuire, D.B.; Migliorati, C.; Nicolatou-Galitis, O.; Peterson, D.E.; et al. MASCC/ISOO Clinical Practice Guidelines for the Management of Mucositis Secondary to Cancer Therapy. Cancer 2014, 120, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Wylde, V.; Dennis, J.; Beswick, A.D.; Bruce, J.; Eccleston, C.; Howells, N.; Peters, T.J.; Gooberman-Hill, R. Systematic Review of Management of Chronic Pain after Surgery. Br. J. Surg. 2017, 104, 1293–1306. [Google Scholar] [CrossRef] [PubMed]
- Filippatos, G.; Angermann, C.E.; Cleland, J.G.F.; Lam, C.S.P.; Dahlström, U.; Dickstein, K.; Ertl, G.; Hassanein, M.; Hart, K.W.; Lindsell, C.J.; et al. Global Differences in Characteristics, Precipitants, and Initial Management of Patients Presenting with Acute Heart Failure. JAMA Cardiol. 2020, 5, 401–410. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Citation | Location | Study Design | Diagnosis | Characteristics of Population | Number of Patients |
|---|---|---|---|---|---|
| Snijders 2023 [16] | Head and neck: Europe, Asia, North America Bronchus/lung: Europe, Asia, North America, Oceania Breast: all continents GI: Europe, Asia, North America, Oceania Prostate: Europe, Asia, North America, Oceania Gyn: Europe, Asia, North America, Oceania Hematological: Europe, Asia, North America, Oceania | SR + MA | Cancer: head and neck, bronchus/lung, breast, GI, prostate, Gyn, hematological | Cancer | Head and Neck: 4718 Bronchus/lung: 15,725 Breast: 52,376 GI: 19,911 Prostate: 4445 Gyn: 5924 Hematological: 4869 |
| Haenen 2022 [17] | Breast: Asia, Europe Gyn: Europe, Oceania Lung: Europe, North America Prostate: Europe Rectal: South America | SR + MA | Cancer: breast, lung, Gyn, prostate, rectal | Solid cancer | Breast: 11,996 Lung: 588 Gyn: 337 Prostate: 109 Rectal: 40 |
| Cole 2022 [18] | Finland, Netherlands, Italy, Norway, US, Hong Kong, Czech Republic, England, France, Germany, Israel, Japan, Brazil, Turkey, Austria, Sweden, Australia, China, Korea | SR | Arthritis, depression, dementia, osteoporosis, pressure ulcer, falls, anxiety, contracture | Nursing home residents | 106–1,387,405 |
| Evans 2022 [19] | Denmark, UK, Turkey, Scotland, US, Germany, Italy, Greece, India, Egypt, Finland | SR + MA | Amputation: cancer, trauma, vasculopathy | Residual limb pain | 1347 |
| Hurwitz 2021 [20] | Japan, US, Italy, Germany, Canada, France, Australia, Sweden, Finland, UK, | SR + MA | ALS | ALS | 1426 |
| Innes 2020 [21] | OA: Taiwan, US Fibromyalgia: Taiwan Headache: Taiwan, Norway, Canada | SR | Dementia | OA, fibromyalgia, headache, migraine, Alzheimer’s | 701,593 OA: 201,495 Fibromyalgia: 165,000 Headache: 319,023 |
| Chang 2021 [22] | NG | SR | Neurodegenerative diseases with atypical parkinsonism | MSA, PSP, CBS, DLB, FTD | NG |
| Sprenger 2019 [23] | UK, Germany, France, US, Italy, Cyprus, Norway | SR + MA | HD | HD | 2578 |
| Rana 2019 [24] | Sweden, UK, Austria, Italy, Spain, Israel, Germany, US, Canada, China | SR + MA | Atypical parkinsonism | MSA, PSP, CBS, LBD | CBS: 55 LBD: 95 MSA: 599 PSP: 242 |
| Delwel 2017 [25] | UK, Brazil, Australia, US, Denmark, Switzerland, Malaysia, Norway, Japan, Turkey, Greece, Thailand, Finland, Germany | SR | Dementia | Dementia | 257 (focused on pain) |
| Drageset 2014 [26] | US (no information on all the studies) | SR | Cancer: colon | Nursing Home Residents with Cancer | 277,249 |
| Stubbs 2014 [27] | US, UK, Australia, Italy, Japan, China, Nigeria, Netherlands, Taiwan, Turkey | SR + MA | Chronic pain | Seniors | 32,705 for narrative, 17,926 for MA |
| Alemzadeh-Ansari 2017 [28] | NG | SR | CHF | CHF | 20,875 |
| van Isselt 2014 [29] | US, UK, Canada, Norway, Netherlands | SR + MA | COPD | COPD | 12,479 |
| Lee 2015 [30] | Norway, Canada, US | SR | COPD | COPD | 8677 |
| Van den Beuken-van Everdingen 2007 [31] | All continents | SR | Cancer: head and neck, GI, lung/bronchus, breast, urogenital, Gyn | Cancer | Head and neck: 95 GI: 564 Lung/bronchus: 1546 Breast: 420 Urogenital: 336 Gyn: 372 |
| Davison 2021 [32] | US, Saudi Arabia, Norway, Republic of Guinea, Italy, Morocco, Australia, Spain, Republic of Korea, Hong Kong, Canada, Brazil, Turkey, Israel, Uruguay, Switzerland, Lebanon, Taiwan, Poland, UK, India, Netherlands, Iran, Sri Lanka, Malaysia, Germany, China | SR + MA | CKD | CKD | 16,558 |
| Lambourg 2021 [33] | US, UK—most common | SR + MA | CKD | CKD | 40,678 |
| Brkovic 2016 [34] | Scotland, Italy, Kuwait, Brazil, US, Canada, Morocco, Spain, UK, Serbia, Turkey, Switzerland, Israel, Pakistan, Japan, Iran, France | SR | ESRD | ESRD patients on hemodialysis | 6917 |
| Murtagh 2007 [35] | NG | SR | ESRD | ESRD | 462 for pain only |
| Peng 2019 [36] | North America, Europe, Asia, Africa | SR + MA | End-stage liver disease | End-stage liver disease | 5434 |
| Nampiaparampil 2008 [37] | NG | SR | TBI | TBI | Headache: 1670 Chronic pain among civilians: 3289 Chronic pain among veterans: 917 |
| Harriott 2020 [38] | Europe, Asia, North America | SR + MA | Ischemic stroke | Ischemic stroke | 33,231 |
| Liampas 2020 [39] | NG | SR + MA | Stroke | Stroke | 20,668 |
| O’Connor 2008 [40] | Belgium, Denmark, Canada, Italy, Norway, Sweden | SR | MS | MS | 3360 |
| Author, Year, Citation | Reported Prevalence | Prevalence of Other Symptoms | Characteristics of Pain: (a) Organ, (b) Type | Reported Mechanism of Pain | Conclusions |
|---|---|---|---|---|---|
| Snijders 2023 [16] | Head and neck: 8.8–77.3% Bronchus/lung: 21–77% Breast: 4.2–91.2% GI: 6.1–87% Prostate: 12.6–39.1% Gyn: 6–69% Hematological: 8–86.9% | NG | (a) Head and neck, bronchus/lung, breast, GI, prostate, Gyn | NG | The prevalence of pain is high, especially with advanced stage |
| Haenen 2022 [17] | Breast: 49% (95% CI 40–58%) Lung: 39% (95% CI 11–73%) Gyn: 55% (95% CI 49–62%) | NG | (a) Breast, lung, Gyn, prostate, rectal (b) Neuropathic | Not reported in studies | At least half of cancer patients experience pain at least three months after therapy |
| Cole 2022 [18] | Current pain: 22.2–85% Persistent pain: 19.5–58.5% Chronic pain: 55.9–58.1% | NG | - | Depression can lower the pain threshold, or chronic pain can cause mood disorders | Many factors can affect pain, especially depression |
| Evans 2022 [19] | 1 w: 50% 1 mo: 11% 3 mo: 23% 6 mo: 27% 1 y: 22% 2 y: 24% | NG | (a) Upper and lower limbs (b) Neuropathic pain | Nerve injuries | Upper limb amputations due to cancer and trauma are the most painful |
| Hurwitz 2021 [20] | 60% (95% CI = 50–69%) | NG | (a) Head, neck, trunk, back—24.8% Upper limbs—41.5% Lower limbs—33.7% (b) Neuropathic | Multifactorial pain, causes include inadequate posture | Pain in ALS is high |
| Innes 2020 [21] | Not the focus | Prevalence of dementia OA: 7.5% Fibromyalgia: 3.8% Headache: 1.5% | (a) Head | Lifestyle, a vicious cycle between pain and cognitive decline | Dementia might lead to the development of chronic pain |
| Chang 2021 [22] | MSA: 40–81% PSP: 25–68% CBS: 14–83% DLB: 25–70% FTD: 33–58% | NG | (a) MSA: neck, back, limbs PSP: limbs, neck, back CBS: limbs DLB: multiple places FTD: head, neck, shoulder, abdomen (b) MSA: MSK, neuropathic, dystonic PSP: MSK CBS: dystonic DLB: neuropathic, MSK FTD: MSK | NG | Neurodegenerative diseases can lead to chronic pain. However, prevalence might be underestimated due to the cognitive decline of patients |
| Sprenger 2019 [23] | 41.3% (95% CI: 36–46%) Range: 10–75% | SF-36 score is 84 (95% CI: 81–86%) | NG | Many confounding factors | Pain might be one of the HD symptoms. Pain burden in the HD population is lower than that in the general population |
| Rana 2019 [24] | CBS: 25% LBD: 38% MSA: 73% PSP: 52% | NG | (a) LBD: multilocalized (b) MSA: MSK, neuropathic, central, radicular, arthritis PSP: neuropathic, MSK, central, arthritis CBS: dystonic, central, MSK LBD: MSK | Damage of pain receptors, improper posture | Patients with atypical parkinsonism experience pain, especially in the limbs |
| Delwel 2017 [25] | 7.4–21.7% | NG | (a) Orofacial | NG | Patients with dementia have poorer oral health. No conclusions on orofacial pain can be drawn |
| Drageset 2014 [26] | 37–60% (not all the studies reported pain) | NG | NG | NG | High prevalence of pain in cancer patients |
| Stubbs 2014 [27] | 32.5% (not the focus) | Prevalence of falls: 50.5% | (a) Lower limb pain | Not the focus | Seniors with pain are likely to fall, especially with foot pain |
| Alemzadeh-Ansari 2017 [28] | 23–85% | NG | (a) Chest (b) Neuropathic | Ischemia, inflammation, ascites, constipation | Pain is common in CHF and is poorly controlled |
| van Isselt 2014 [29] | 32–60% | FEV1% 21–48% | (a) Shoulders and neck, lumbar region, chest | NG | Patients with moderate COPD have increased pain |
| Lee 2015 [30] | 66% (95% CI 44–85%) | NG | (a) Shoulder, neck, upper limb, chest, diffuse, lower limb, head, buttocks, back | Altered respiration mechanics | COPD patients with pain have worse symptoms and QoL |
| Van den Beuken-van Everdingen 2007 [31] | Head and neck: 70 (51–88%) GI: 59 (44–74%) Lung/bronchus: 55 (44–67%) Breast: 54 (44–64%) Urogenital: 52 (40–60%) Gyn: 60 (50–71%) | NG | (a) Head and neck, GI, lung/bronchus, breast, urogenital, Gyn | NG | Cancer pain is common |
| Davison 2021 [32] | Moderate or severe pain: 43.6% Chronic pain in hemodialysis patients: 60.5% | NG | (a) Bone, joint, muscle, widespread, lower extremities, neck and shoulders, back, upper extremities (b) MSK, neuropathic, atheropathic | NG | Chronic pain is common in CKD |
| Lambourg 2021 [33] | Overall: 60 (95% CI 56–64%) Chronic pain: 48 (95% CI 42–55%) Neuropathic pain: 10 (95% CI 6–15%) Transplant recipients: 46 (95% CI 37–56%) Dialysis: 63% (95% CI 55–70%) Non-dialysis: 63 (95% CI 55–70%) | NG | (a) Abdominal, headache, joint, bone (b) Neuropathic, MSK | Postsurgical, drug toxicity, mineral turnover | CKD patients experience severe pain |
| Brkovic 2016 [34] | Acute: 82% Chronic: 92% | NG | (a) Most—headache, MSK, diffuse (b) Ischemic, neuropathic | Probably comorbidities, procedural pain | High prevalence of pain in CKD patients |
| Murtagh 2007 [35] | 47% (8–82%) | Fatigue 71% (12–97%), pruritus 55% (10–77%), constipation 53% (8–57%), anorexia 49% (25–61%), sleep disturbance 44% (20–83%), anxiety 38% (12–52%), dyspnea 35% (11–55%), nausea 33% (15–48%), restless legs 30% (8–52%), depression 27% (5–58%) | (a) Muscle cramps, headache | NG | (Not related to pain) |
| Peng 2019 [36] | 30–79% | Breathlessness 20–88%, muscle cramps 56–68%, insomnia 26–77%, daytime sleepiness 29.5–71%, depression 4.5–64%, anxiety 14–45%, erectile dysfunction 53–93% | NG | NG | Symptoms of end-stage liver disease are similar to the symptoms of other advanced diseases |
| Nampiaparampil 2008 [37] | Headache: 57.8 (95% CI 55.5–60.2%) Chronic pain among civilians: 51.5 (95% CI 49.8–53.2%) Chronic pain among veterans: 43.1 (95% CI 39.9–46.3%) | NG | (a) Headache | Brain injury | Chronic pain is common in TBI |
| Harriott 2020 [38] | 6–44% | NG | (a) Headache | Changes in innervation, increases in compartmental pressures, meningeal inflammation | Headache is common after an ischemic stroke |
| Liampas 2020 [39] | Overall: 11 (95% CI 7–18%) Stroke onset: 26% (95% CI 18–35%); 1mo: 31% (95% CI 22–42%); 1 mo-1y: 41% (95% CI 33.9–49.0%); 1y+: 5% (95% CI 3–8%) | NG | (b) Neuropathic | NG | Neuropathic pain is common up to one year poststroke |
| O’Connor 2008 [40] | 29–86% | NG | (a) Extremity, back pain, headache, trigeminal neuralgia (b) Neuropathic, MSK, mixed | Psychosocial factors | Extremity pain is the most common in MS |
| Author, Citation | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Snijders 2023 [16] | + | - | - | PY | + | - | - | PY | PY | - | + | - | - | - | - | + |
| Haenen 2022 [17] | + | PY | - | PY | + | - | - | PY | PY | - | + | - | - | + | - | + |
| Cole 2022 [18] | + | - | - | PY | + | - | - | PY | PY | - | N/A | N/A | - | N/A | - | + |
| Evans 2022 [19] | + | + | - | PY | + | + | - | PY | PY | - | + | - | - | - | - | + |
| Hurwitz 2021 [20] | + | - | - | PY | - | - | - | PY | PY | - | + | - | - | + | - | + |
| Innes 2020 [21] | + | - | + | PY | - | - | - | + | PY | - | + | - | - | - | - | + |
| Chang 2021 [22] | + | - | - | PY | - | - | - | - | - | - | N/A | N/A | - | N/A | - | + |
| Sprenger 2019 [23] | + | + | - | PY | + | - | - | PY | PY | - | + | - | - | - | - | - |
| Rana 2019 [24] | + | - | - | PY | + | - | - | PY | - | - | + | - | - | + | + | + |
| Delwel 2017 [25] | + | - | - | PY | + | - | + | PY | PY | - | N/A | N/A | - | N/A | - | + |
| Drageset 2014 [26] | + | - | - | PY | + | - | - | PY | PY | - | N/A | N/A | - | N/A | - | + |
| Stubbs 2014 [27] | + | - | - | PY | + | - | - | + | PY | - | + | - | - | + | + | + |
| Alemzadeh-Ansari 2017 [28] | + | - | - | PY | - | - | - | PY | - | - | N/A | N/A | - | N/A | - | - |
| van Isselt 2014 [29] | + | - | - | PY | + | + | - | PY | PY | - | + | - | - | - | - | + |
| Lee 2015 [30] | + | + | - | PY | + | - | - | PY | PY | - | N/A | N/A | - | N/A | - | + |
| Van den Beuken [31] | + | - | + | PY | - | - | - | PY | PY | - | + | - | - | + | - | - |
| Davison 2021 [32] | + | + | - | - | + | + | + | PY | PY | - | + | - | - | + | + | + |
| Lambourg 2021 [33] | + | + | - | PY | + | - | - | PY | PY | - | + | - | - | + | + | + |
| Brkovic 2016 [34] | + | + | - | PY | + | - | - | PY | PY | - | N/A | N/A | - | N/A | - | + |
| Murtagh 2007 [35] | + | - | + | + | - | - | - | PY | - | - | N/A | N/A | - | N/A | - | + |
| Peng 2019 [36] | + | - | - | PY | + | - | - | - | PY | - | + | - | - | - | - | + |
| Nampiaparampil 2008 [37] | + | - | + | + | - | - | - | PY | - | - | + | - | - | - | - | + |
| Harriott 2020 [38] | + | - | - | PY | + | - | - | PY | - | - | + | - | - | + | + | + |
| Liampas 2020 [39] | + | + | + | PY | + | + | - | - | PY | - | + | - | + | - | + | + |
| O’Connor 2008 [40] | + | - | - | + | - | - | - | + | - | - | N/A | N/A | - | N/A | - | + |
| ||||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viderman, D.; Tapinova, K.; Aubakirova, M.; Abdildin, Y.G. The Prevalence of Pain in Chronic Diseases: An Umbrella Review of Systematic Reviews. J. Clin. Med. 2023, 12, 7302. https://doi.org/10.3390/jcm12237302
Viderman D, Tapinova K, Aubakirova M, Abdildin YG. The Prevalence of Pain in Chronic Diseases: An Umbrella Review of Systematic Reviews. Journal of Clinical Medicine. 2023; 12(23):7302. https://doi.org/10.3390/jcm12237302
Chicago/Turabian StyleViderman, Dmitriy, Karina Tapinova, Mina Aubakirova, and Yerkin G. Abdildin. 2023. "The Prevalence of Pain in Chronic Diseases: An Umbrella Review of Systematic Reviews" Journal of Clinical Medicine 12, no. 23: 7302. https://doi.org/10.3390/jcm12237302
APA StyleViderman, D., Tapinova, K., Aubakirova, M., & Abdildin, Y. G. (2023). The Prevalence of Pain in Chronic Diseases: An Umbrella Review of Systematic Reviews. Journal of Clinical Medicine, 12(23), 7302. https://doi.org/10.3390/jcm12237302