
Reactive Hypoglycemia: A Trigger for Nutrient-Induced Endocrine and Metabolic Responses in Polycystic Ovary Syndrome

Abstract
:
1. Introduction
- Does replacement of dietary fat with CHOs vs. protein influence the amount of weight loss and body composition?
- What are the acute metabolic and endocrine effects of CHO and protein intake on PCOS?
- Do the amino acid compositions of dietary proteins affect weight loss and/or insulin resistance?
1.1. Comparing Low-Fat/High-CHO vs. Low-Fat/High-Protein Diets during Weight Loss in Women with PCOS
Acute Effects of Simple CHOs vs. Protein
1.2. Postprandial Hypoglycemia after Simple Sugar vs. Protein Intake
1.3. Effects of Dietary CHOs vs. Protein on Anthropometric Outcomes during Weight Loss Intervention
1.4. Effects of Amino Acid Composition of Dietary Protein on Weight Loss and Metabolic Parameters in Women with PCOS
2. Discussion and a Unifying Hypothesis
- One third of the women with PCOS developed physiologically significant reactive hypoglycemia after simple sugar intake and secretion of cortisol and adrenal androgens.
- Adrenal steroid secretion coincided with hypoglycemic symptoms.
- Whey protein intake stimulated insulin secretion but did not cause hypoglycemia.
- Whey protein supplementation suppressed the hunger signal ghrelin for a longer period as compared to simple CHO supplement.
- A weight loss diet containing a WP supplement was associated with greater weight loss and fat mass loss and a decrease in leptin when compared to the diet containing a simple CHO supplement.
- When the WP supplement was compared to the gelatin supplement, there was no difference in the amount of weight loss or the improvement in insulin sensitivity, despite the lower essential AA- and BCAA content of gelatin.
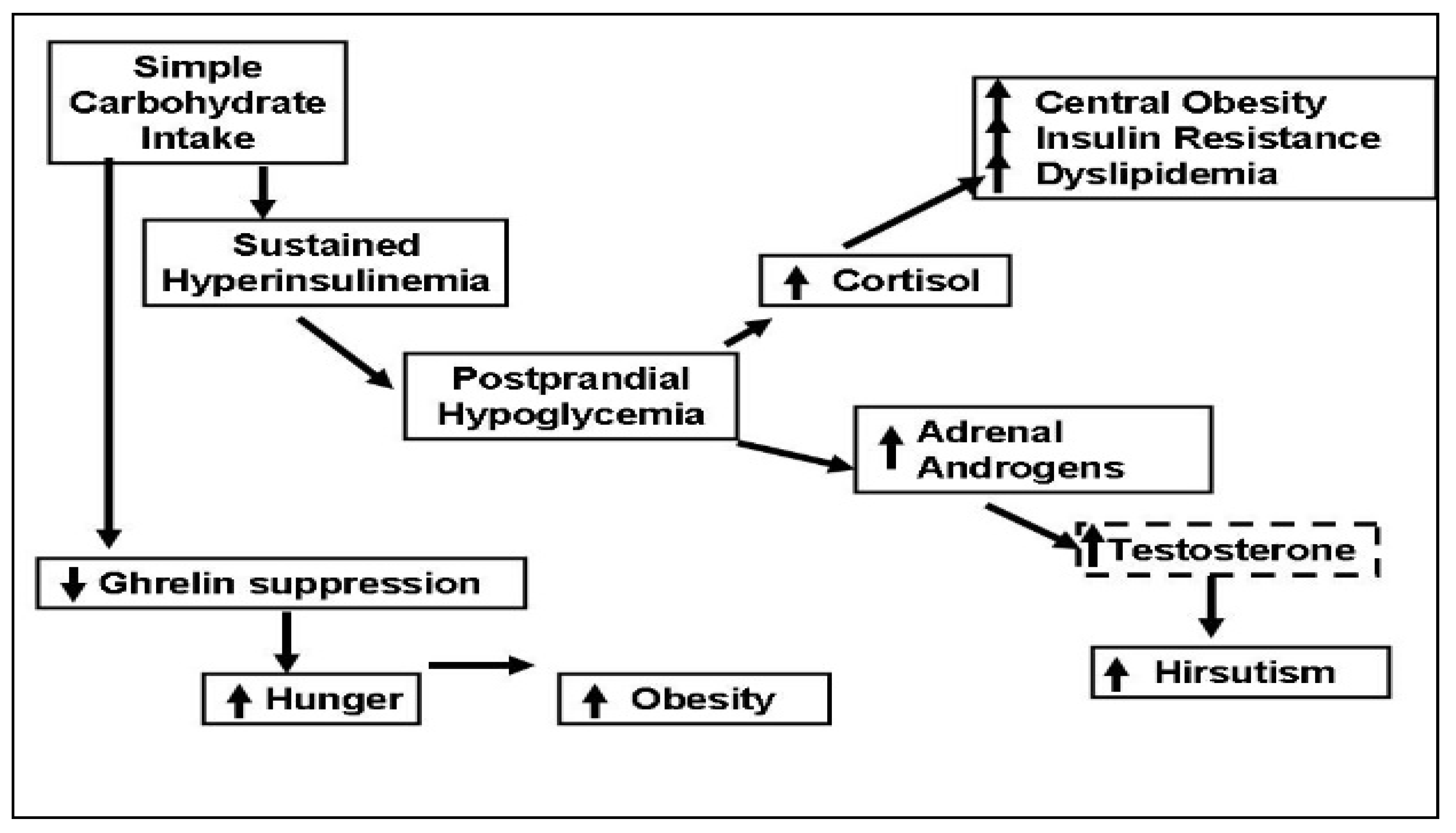
- Polycystic ovary syndrome is an insulin-resistant state, compensated for by the body via hyperinsulinemia. Simple CHO intake results in large amounts of insulin secretion. Insulin levels in the circulation remain elevated after emptying of the stomach, and this causes reactive hypoglycemia. Protein intake also stimulates insulin secretion but does not cause hypoglycemia, possibly because protein intake stimulates glucagon, which facilitates glycogenolysis in the liver [34]. In addition, amino acids, especially alanine, serve as glucose precursors for gluconeogenesis [35].
- Reactive hypoglycemia triggers an adrenergic response, as evidenced by the symptoms of tremors and sweating and stimulates steroid hormone secretion from the adrenals. Cortisol causes central fat deposition, insulin resistance and dyslipidemia. This concept is supported by our observation that the women with hypoglycemic symptoms were more obese and insulin-resistant. Adrenal androgens are converted to testosterone in the peripheral tissues and increase hirsutism. We found that the women with hypoglycemic symptoms had a 1.7-times higher testosterone level/DHEAS molar ratio as compared to those without hypoglycemic symptoms.
- Even though protein and CHOs are equally effective in suppressing the hunger signal ghrelin, the effect of CHOs does not last as long. Moran et al. reported no difference between the suppressive effects of oral protein vs. CHO challenges during a 3 h test [36]. We saw that the suppressive effects of CHO vs. protein intakes differed after the 3rd hour. After protein intake, ghrelin remained suppressed for 5 h; after simple CHO intake, ghrelin started to rise by the 3rd hour and returned to baseline by the 5th hour.
Funding
Data Availability Statement
Conflicts of Interest
References
- Carmina, E.; Legro, R.S.; Stamets, K.; Lowell, J.; Lobo, R.A. Difference in body weight between American and Italian women with polycystic ovary syndrome: Influence of the diet. Hum. Reprod. 2003, 18, 2289–2293. [Google Scholar] [CrossRef] [PubMed]
- Glueck, C.J.; Papanna, R.; Wang, P.; Goldenberg, N.; Sieve-Smith, L. Incidence and treatment of metabolic syndrome in newly referred women with confirmed polycystic ovarian syndrome. Metabolism 2003, 52, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Haase, C.L.; Varbo, A.; Laursen, P.N.; Schnecke, V.; Balen, A.H. Association between body mass index, weight loss and the chance of pregnancy in women with polycystic ovary syndrome and overweight or obesity: A retrospective cohort study in the UK. Hum. Reprod. 2023, 38, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Marzouk, T.M.; Sayed Ahmed, W.A. Effect of Dietary Weight Loss on Menstrual Regularity in Obese Young Adult Women with Polycystic Ovary Syndrome. J. Pediatr. Adolesc. Gynecol. 2015, 28, 457–461. [Google Scholar] [CrossRef]
- Ravn, P.; Haugen, A.G.; Glintborg, D. Overweight in polycystic ovary syndrome. An update on evidence based advice on diet, exercise and metformin use for weight loss. Minerva Endocrinol. 2013, 38, 59–76. [Google Scholar]
- Thomson, R.L.; Buckley, J.D.; Moran, L.J.; Noakes, M.; Clifton, P.M.; Norman, R.J.; Brinkworth, G.D. The effect of weight loss on anti-Mullerian hormone levels in overweight and obese women with polycystic ovary syndrome and reproductive impairment. Hum. Reprod. 2009, 24, 1976–1981. [Google Scholar] [CrossRef]
- Mueller-Cunningham, W.M.; Quintana, R.; Kasim-Karakas, S.E. An ad libitum, very low-fat diet results in weight loss and changes in nutrient intakes in postmenopausal women. J. Am. Diet Assoc. 2003, 103, 1600–1606. [Google Scholar] [CrossRef]
- Kasim-Karakas, S.E.; Tsodikov, A.; Singh, U.; Jialal, I. Responses of inflammatory markers to a low-fat, high-carbohydrate diet: Effects of energy intake. Am. J. Clin. Nutr. 2006, 83, 774–779. [Google Scholar] [CrossRef]
- Gurusinghe, D.; Gill, S.; Almario, R.U.; Lee, J.; Horn, W.F.; Keim, N.L.; Kim, K.; Karakas, S.E. In polycystic ovary syndrome, adrenal steroids are regulated differently in the morning versus in response to nutrient intake. Fertil. Steril. 2010, 93, 1192–1199. [Google Scholar] [CrossRef]
- Kasim-Karakas, S.E.; Cunningham, W.M.; Tsodikov, A. Relation of nutrients and hormones in polycystic ovary syndrome. Am. J. Clin. Nutr. 2007, 85, 688–694. [Google Scholar] [CrossRef]
- Field, J.B. Hypoglycemia. Definition, clinical presentations, classification, and laboratory tests. Endocrinol. Metab. Clin. N. Am. 1989, 18, 27–43. [Google Scholar] [CrossRef]
- Brun, J.F.; Fedou, C.; Mercier, J. Postprandial reactive hypoglycemia. Diabetes Metab. 2000, 26, 337–351. [Google Scholar] [PubMed]
- Kasim-Karakas, S.E.; Almario, R.U.; Cunningham, W. Effects of protein versus simple sugar intake on weight loss in polycystic ovary syndrome (according to the National Institutes of Health criteria). Fertil. Steril. 2009, 92, 262–270. [Google Scholar] [CrossRef]
- Drummond, J.B.; Soares, B.S.; Pedrosa, W.; Ribeiro-Oliveira, A., Jr. Revisiting peak serum cortisol response to insulin-induced hypoglycemia in children. J. Endocrinol. Investig. 2021, 44, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Streeten, D.H.; Anderson, G.H., Jr.; Dalakos, T.G.; Seeley, D.; Mallov, J.S.; Eusebio, R.; Sunderlin, F.S.; Badawy, S.Z.A.; King, R.B. Normal and abnormal function of the hypothalamic-pituitary-adrenocortical system in man. Endocr. Rev. 1984, 5, 371–394. [Google Scholar] [CrossRef]
- Gorissen, S.H.M.; Crombag, J.J.R.; Senden, J.M.G.; Waterval, W.A.H.; Bierau, J.; Verdijk, L.B.; van Loon, L.J.C. Protein content and amino acid composition of commercially available plant-based protein isolates. Amino Acids 2018, 50, 1685–1695. [Google Scholar] [CrossRef]
- Newgard, C.B. Interplay between lipids and branched-chain amino acids in development of insulin resistance. Cell Metab. 2012, 15, 606–614. [Google Scholar] [CrossRef]
- Newgard, C.B.; An, J.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Lien, L.F.; Haqq, A.M.; Shah, S.H.; Arlotto, M.; Slentz, C.A.; et al. A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab. 2009, 9, 311–326. [Google Scholar] [CrossRef]
- Eastoe, J.E. The amino acid composition of mammalian collagen and gelatin. Biochem. J. 1955, 61, 589–600. [Google Scholar] [CrossRef]
- Piccolo, B.D.; Comerford, K.B.; Karakas, S.E.; Knotts, T.A.; Fiehn, O.; Adams, S.H. Whey protein supplementation does not alter plasma branched-chained amino acid profiles but results in unique metabolomics patterns in obese women enrolled in an 8-week weight loss trial. J. Nutr. 2015, 145, 691–700. [Google Scholar] [CrossRef]
- Altuntas, Y.; Bilir, M.; Ucak, S.; Gundogdu, S. Reactive hypoglycemia in lean young women with PCOS and correlations with insulin sensitivity and with beta cell function. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 119, 198–205. [Google Scholar] [CrossRef]
- Mumm, H.; Altinok, M.L.; Henriksen, J.E.; Ravn, P.; Glintborg, D.; Andersen, M. Prevalence and possible mechanisms of reactive hypoglycemia in polycystic ovary syndrome. Hum. Reprod. 2016, 31, 1105–1112. [Google Scholar] [CrossRef]
- Sam, S.; Vellanki, P.; Yalamanchi, S.K.; Bergman, R.N.; Dunaif, A. Exaggerated glucagon responses to hypoglycemia in women with polycystic ovary syndrome. Metabolism 2017, 71, 125–131. [Google Scholar] [CrossRef]
- Gennarelli, G.; Holte, J.; Stridsberg, M.; Niklasson, F.; Berne, C.; Backstrom, T. The counterregulatory response to hypoglycaemia in women with the polycystic ovary syndrome. Clin. Endocrinol. 1997, 46, 167–174. [Google Scholar] [CrossRef]
- Kishimoto, I. Subclinical Reactive Hypoglycemia with Low Glucose Effectiveness-Why We Cannot Stop Snacking despite Gaining Weight. Metabolites 2023, 13, 754. [Google Scholar] [CrossRef] [PubMed]
- Ooi, D.S.Q.; Ling, J.Q.R.; Ong, F.Y.; Tai, E.S.; Henry, C.J.; Leow, M.K.S.; Khoo, E.Y.H.; Tan, C.S.; Chong, M.F.F.; Khoo, C.M.; et al. Branched Chain Amino Acid Supplementation to a Hypocaloric Diet Does Not Affect Resting Metabolic Rate but Increases Postprandial Fat Oxidation Response in Overweight and Obese Adults after Weight Loss Intervention. Nutrients 2021, 13, 4245. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Moran, L.J.; Clifton, P.M.; Noakes, M.; Brinkworth, G.D. Effects of energy-restricted high-protein, low-fat compared with standard-protein, low-fat diets: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 96, 1281–1298. [Google Scholar] [CrossRef]
- Stamets, K.; Taylor, D.S.; Kunselman, A.; Demers, L.M.; Pelkman, C.L.; Legro, R.S. A randomized trial of the effects of two types of short-term hypocaloric diets on weight loss in women with polycystic ovary syndrome. Fertil. Steril. 2004, 81, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Ko, H.; Misso, M.; Marsh, K.; Noakes, M.; Talbot, M.; Frearson, M.; Thondan, M.; Stepto, N.; Teede, H.J. Dietary composition in the treatment of polycystic ovary syndrome: A systematic review to inform evidence-based guidelines. J. Acad. Nutr. Dietetics 2013, 113, 520–545. [Google Scholar] [CrossRef]
- Douglas, C.C.; Gower, B.A.; Darnell, B.E.; Ovalle, F.; Oster, R.A.; Azziz, R. Role of diet in the treatment of polycystic ovary syndrome. Fertil. Steril. 2006, 85, 679–688. [Google Scholar] [CrossRef]
- Marsh, K.A.; Steinbeck, K.S.; Atkinson, F.S.; Petocz, P.; Brand-Miller, J.C. Effect of a low glycemic index compared with a conventional healthy diet on polycystic ovary syndrome. Am. J. Clin. Nutr. 2010, 92, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Galletly, C.; Moran, L.; Noakes, M.; Clifton, P.; Tomlinson, L.; Norman, R. Psychological benefits of a high-protein, low-carbohydrate diet in obese women with polycystic ovary syndrome—A pilot study. Appetite 2007, 49, 590–593. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, L.B.; Soe, M.; Halkier, K.H.; Stigsby, B.; Astrup, A. Effects of increased dietary protein-to-carbohydrate ratios in women with polycystic ovary syndrome. Am. J. Clin. Nutr. 2012, 95, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, R.; Takano, K.; Fujimoto, K.; Kobayashi, M.; Kitamura, T.; Shichiri, M.; Miyatsuka, T. Robust increase in glucagon secretion after oral protein intake, but not after glucose or lipid intake in Japanese people without diabetes. J. Diabetes Investig. 2023, 14, 1172–1174. [Google Scholar] [CrossRef]
- Ishikawa, E.; Aikawa, T.; Matsutaka, H. The roles of alanine as a major precursor among amino acids for hepatic gluconeogenesis and as a major end product of the degradation of amino acids in rat tissues. J. Biochem. 1972, 71, 1097–1099. [Google Scholar] [CrossRef]
- Moran, L.J.; Noakes, M.; Clifton, P.M.; Wittert, G.A.; Le Roux, C.W.; Ghatei, M.A.; Stephen, R.B.; Robert, J.N. Postprandial ghrelin, cholecystokinin, peptide, Y.Y.; and appetite before and after weight loss in overweight women with and without polycystic ovary syndrome. Am. J. Clin. Nutr. 2007, 86, 1603–1610. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | 2 mo. | Change | P1 | P2 | |
|---|---|---|---|---|---|
| Fasting glucose (mg/dL) | |||||
| Whey protein | 111 ± 5 | 110 ± 5 | −1.5 ± 3.3 | (log) | |
| Simple carbohydrates | 102 ± 6 | 97 ± 4 | −4.5 ± 2.9 | 0.561 | 0.513 |
| Fasting insulin (mIU/mL) | |||||
| Whey protein | 31.8 ± 4.2 | 28.6 ± 4.6 | −3.2 ± 2.1 | ||
| Simple carbohydrates | 23.9 ± 5.0 | 22.0 ± 5.4 | −1.9 ± 2.1 | 0.664 | 0.664 |
| Adiponectin (μg/L) (log) | |||||
| Whey protein | 8.6 ± 1.2 | 6.7 ± 0.6 | −1.9 ± 0.8 a | (log) | |
| Simple carbohydrates | 8.6 ± 1.5 | 8.0 ± 1.2 | −0.6 ± 0.8 | 0.159 | 0.126 |
| HOMA | |||||
| Whey protein | 9.0 ± 1.3 | 7.3 ± 1.6 | −1.7 ± 1.0 | ||
| Simple carbohydrates | 6.1 ± 1.8 | 5.5 ± 1.6 | −0.6 ± 0.6 | 0.306 | 0.298 |
| HgBA1 (%) | |||||
| Whey protein | 5.7 ± 0.1 | 5.5 ± 0.2 | −0.1 ± 0.1 | ||
| Simple carbohydrates | 5.4 ± 0.1 | 5.2 ± 0.1 | −0.1 ± 0.1 | 0.855 | 0.855 |
| Triglyceride (mg/dL) | |||||
| Whey protein | 149 ± 16 | 117 ± 19 | −32 ± 21 | ||
| Simple carbohydrates | 92 ± 11 | 94 ± 12 | 2 ± 8 | 0.15 | 0.0974 |
| Cholesterol (mg/dL) | |||||
| Whey protein | 201 ± 8 | 168 ± 10 | −33 ± 8.4 b | ||
| Simple carbohydrates | 164 ± 6 | 162 ± 7 | −2.3 ± 6.8 | 0.0089 | 0.0053 |
| HDL cholesterol (mg/dL) | |||||
| Whey protein | 38 ± 2 | 34 ± 2 | −4.5 ± 1.3 b | ||
| Simple carbohydrates | 37 ± 1 | 36 ± 2 | −0.4 ± 1.3 | 0.0395 | 0.024 |
| Apo B (mg/dL) | |||||
| Whey protein | 117 ± 4 | 97 ± 7 | −20 ± 5 b | ||
| Simple carbohydrates | 90 ± 5 | 93 ± 6 | 3 ± 5 | 0.0045 | 0.0045 |
| hs-CRP (ng/mL) | |||||
| Whey protein | 4.7 ± 0.9 | 3.7 ± 0.8 | −1.0 ± 0.6 | ||
| Simple carbohydrates | 4.5 ± 1.2 | 3.6 ± 1.1 | −0.9 ± 0.6 | 0.887 | 0.881 |
| Total testosterone (ng/mL) | |||||
| Whey protein | 0.95 ± 0.19 | 0.79 ± 0.11 | −0.16 ± 0.16 | (log) | |
| Simple carbohydrates | 0.70 ± 0.07 | 0.73 ± 0.09 | 0.04 ± 0.04 | 0.817 | 0.791 |
| SHBG (nmol/L) | |||||
| Whey protein | 37.8 ± 8.5 | 32.7 ± 8.5 | −5.1 ± 4.0 | (log) | |
| Simple carbohydrates | 48.3 ± 10.6 | 41.0 ± 7.2 | −7.4 ± 6.6 | 0.774 | 0.755 |
| Free androgen index | |||||
| Whey protein | 15.8 ± 4.8 | 14.6 ± 3.0 | −1.2 ± 3.9 | (log) | |
| Simple carbohydrates | 7.5 ± 1.5 | 9.2 ± 1.8 | 1.7 ± 1.2 | 0.943 | 0.941 |
| DHEAS (ng/mL) | |||||
| Whey protein | 203.8 ± 34.1 | 256.8 ± 57.1 | 53.1 ± 43.8 | ||
| Simple carbohydrates | 261.8 ± 45.2 | 275.7 ± 50.6 | 14.0 ± 22.6 | 0.425 | 0.425 |
| WP vs. Simple-CHO | WP vs. Gelatin | |||
|---|---|---|---|---|
| Acute Challenge Studies (Reference [10]) | WP | Simple-CHO | ||
| Glucose: No change Increased Insulin: Increased Increased Ghrelin: Suppressed 5 h Suppressed 3 h | ----- | |||
| Adrenal-Steroid Response to Acute Challenge (Reference [9]) | Responders | Non-Responders | ----- | |
| Cortisol: Increased No change DHEA: Increased No change Hypoglycemia: Yes No | ||||
| Weight Loss studies Reference [13]) | WP | Simple-CHO | WP | Gelatin |
| Weight: Decreased Decreased less BMI: Decreased Decreased less Fat mass: Decreased No change Leptin: Decreased No change | Similar decreases in weight, BMI, and plasma glucose, insulin, and lipids in both groups | |||
| Plasma Metabolome Changes (Reference [18]) | ------------ | Before, but not after, weight loss, branch chain amino acids (Leu, Ile, Val) correlated with homeostasis model assessment of insulin resistance (HOMA) (p < 0.05 for all). Proline and cystine related pathways discriminated WP vs. gelatin supplementations. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karakas, S.E. Reactive Hypoglycemia: A Trigger for Nutrient-Induced Endocrine and Metabolic Responses in Polycystic Ovary Syndrome. J. Clin. Med. 2023, 12, 7252. https://doi.org/10.3390/jcm12237252
Karakas SE. Reactive Hypoglycemia: A Trigger for Nutrient-Induced Endocrine and Metabolic Responses in Polycystic Ovary Syndrome. Journal of Clinical Medicine. 2023; 12(23):7252. https://doi.org/10.3390/jcm12237252
Chicago/Turabian StyleKarakas, Sidika E. 2023. "Reactive Hypoglycemia: A Trigger for Nutrient-Induced Endocrine and Metabolic Responses in Polycystic Ovary Syndrome" Journal of Clinical Medicine 12, no. 23: 7252. https://doi.org/10.3390/jcm12237252
APA StyleKarakas, S. E. (2023). Reactive Hypoglycemia: A Trigger for Nutrient-Induced Endocrine and Metabolic Responses in Polycystic Ovary Syndrome. Journal of Clinical Medicine, 12(23), 7252. https://doi.org/10.3390/jcm12237252