The Significance of Histopathological Findings on Clinical Outcomes in Endoscopic Papillectomy with Endocut

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
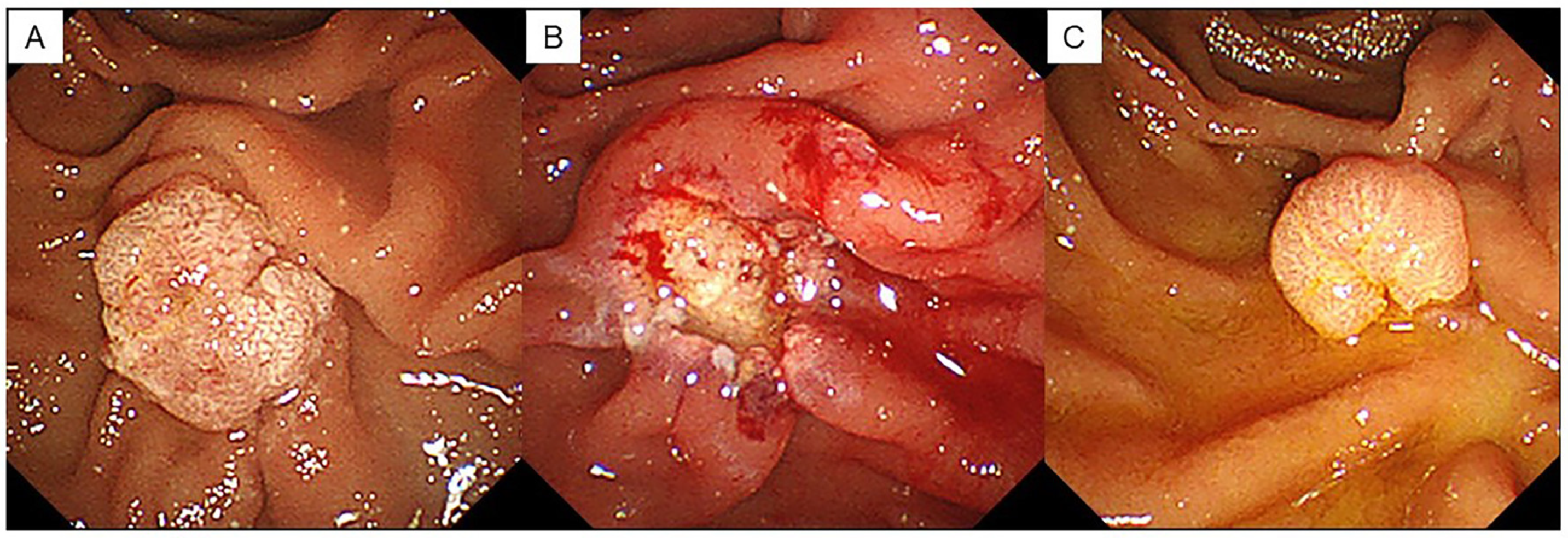
2.2. EP Procedure
2.3. Histopathological Evaluation
2.4. Follow-Up Method after Endoscopic Papillectomy
2.5. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
3.2. Clinical Factors Associated with Pathological Findings of Resection Margin
3.3. Residual Recurrence Rates Associated with Pathological Resection Margin
3.4. Timing of Endoscopic Diagnosis of Residual Tumor and Post-Treatment after EP
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alali, A.; Espino, A.; Moris, M.; Martel, M.; Schwartz, I.; Cirocco, M.; Streutker, C.; Mosko, J.; Kortan, P.; Barkun, A.; et al. Two cases of endoscopic resection for duodenal ampullar tumor. Prog. Dig. Endosc. 1983, 23, 236–239. [Google Scholar]
- Itoi, T.; Ryozawa, S.; Katanuma, A.; Kawashima, H.; Iwasaki, E.; Hashimoto, S.; Yamamoto, K.; Ueki, T.; Igarashi, Y.; Inui, K.; et al. Clinical practice guidelines for endoscopic papillectomy. Dig. Endosc. 2022, 34, 394–411. [Google Scholar] [CrossRef]
- Ceppa, E.P.; Burbridge, R.A.; Rialon, K.L.; Omotosho, P.A.; Emick, D.; Jowell, P.S.; Branch, M.S.; Pappas, T.N. Endoscopic versus surgical ampullectomy: An algorithm to treat disease of the ampulla of vater. Ann. Surg. 2013, 257, 315–322. [Google Scholar] [CrossRef] [PubMed]
- ASGE Standards of Practice Committee; Chathadi, K.V.; Khashab, M.A.; Acosta, R.D.; Chandrasekhara, V.; Eloubeidi, M.A.; Faulx, A.L.; Fonkalsrud, L.; Lightdale, J.R.; Salztman, J.R.; et al. The role of endoscopy in ampullary and duodenal adenomas. Gastrointest. Endosc. 2015, 82, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Nagino, M.; Hirano, S.; Yoshitomi, H.; Aoki, T.; Uesaka, K.; Unno, M.; Ebata, T.; Konishi, M.; Sano, K.; Shimada, K.; et al. Clinical practice guidelines for the management of biliary tract cancers 2019: The 3rd English edition. J. Hepatobiliary Pancreat. Sci. 2021, 28, 26–54. [Google Scholar] [CrossRef] [PubMed]
- Desilets, D.J.; Dy, R.M.; Ku, P.M.; Hanson, B.L.; Elton, E.; Mattia, A.; Howell, D.A. Endoscopic management of tumors of the major duodenal papilla: Refined techniques to improve outcome and avoid complications. Gastrointest. Endosc. 2001, 54, 202–208. [Google Scholar] [CrossRef]
- Zádorová, Z.; Dvofák, M.; Hajer, J. Endoscopic therapy of benign tumors of the papilla of Vater. Endoscopy 2001, 33, 345–347. [Google Scholar] [CrossRef]
- Kohler, A.; Maier, M.; Benz, C.; Martin, W.R.; Farin, G.; Riemann, J.F. A new HF current generator with automatically controlled system (Endocut mode) for endoscopic sphincterotomy—preliminary experience. Endoscopy 1998, 30, 351–355. [Google Scholar] [CrossRef]
- Norton, I.D.; Petersen, B.T.; Bosco, J.; Nelson, D.B.; Meier, P.B.; Baron, T.H.; Lange, S.M.; Gostout, C.J.; Loeb, D.S.; Levy, M.J.; et al. A randomized trial of endoscopic biliary sphincterotomy using pure-cut versus combined cut and coagulation waveforms. Clin. Gastroenterol. Hepatol. 2005, 3, 1029–1033. [Google Scholar] [CrossRef]
- Jeanniard-Malet, O.; Caillol, F.; Pesenti, C.; Bories, E.; Monges, G.; Giovannini, M. Short-term results of 42 endoscopic ampullectomies: A single-center experience. Scand. J. Gastroenterol. 2011, 46, 1014–1019. [Google Scholar] [CrossRef]
- Patel, R.; Davitte, J.; Varadarajulu, S.; Wilcox, C.M. Endoscopic resection of ampullary adenomas: Complications and outcomes. Dig. Dis. Sci. 2011, 56, 3235–3240. [Google Scholar] [CrossRef] [PubMed]
- Laleman, W.; Verreth, A.; Topal, B.; Aerts, R.; Komuta, M.; Roskams, T.; Van der Merwe, S.; Cassiman, D.; Nevens, F.; Verslype, C.; et al. Endoscopic resection of ampullary lesions: A single-center 8-year retrospective cohort study of 91 patients with long-term follow-up. Surg. Endosc. 2013, 27, 3865–3876. [Google Scholar] [CrossRef] [PubMed]
- Will, U.; Müller, A.K.; Fueldner, F.; Wanzar, I.; Meyer, F. Endoscopic papillectomy: Data of a prospective observational study. World J. Gastroenterol. 2013, 19, 4316–4324. [Google Scholar] [CrossRef] [PubMed]
- Napoleon, B.; Gincul, R.; Ponchon, T.; Berthiller, J.; Escourrou, J.; Canard, J.M.; Boyer, J.; Barthet, M.; Ponsot, P.; Laugier, R.; et al. Endoscopic papillectomy for early ampullary tumors: Long-term results from a large multicenter prospective study. Endoscopy 2014, 46, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Shim, C.N.; Chung, M.J.; Bang, S.; Park, S.W.; Song, S.Y.; Chung, J.B.; Park, J.Y. Clinicopathologic characteristics associated with complications and long-term outcomes of endoscopic papillectomy for adenoma. Yonsei Med. J. 2014, 55, 644–650. [Google Scholar] [CrossRef]
- Kang, S.H.; Kim, K.H.; Kim, T.N.; Jung, M.K.; Cho, C.M.; Cho, K.B.; Han, J.M.; Kim, H.G.; Kim, H.S. Therapeutic outcomes of endoscopic papillectomy for ampullary neoplasms: Retrospective analysis of a multicenter study. BMC Gastroenterol. 2017, 17, 69. [Google Scholar] [CrossRef]
- Attila, T.; Parlak, E.; Alper, E.; Dişibeyaz, S.; Çiçek, B.; Ödemiş, B. Endoscopic papillectomy of benign ampullary lesions: Outcomes from a multicenter study. Turk. J. Gastroenterol. 2018, 29, 325–334. [Google Scholar] [CrossRef]
- Stolte, M.; Pscherer, C. Adenoma-carcinoma sequence in the papilla of Vater. Scand. J. Gastroenterol. 1996, 31, 376–382. [Google Scholar] [CrossRef]
- Catalano, M.F.; Linder, J.D.; Chak, A.; Sivak, M.V., Jr.; Raijman, I.; Geenen, J.E.; Howell, D.A. Endoscopic management of adenoma of the major duodenal papilla. Gastrointest. Endosc. 2004, 59, 225–232. [Google Scholar] [CrossRef]
- Harano, M.; Ryozawa, S.; Iwano, H.; Taba, K.; Sen-Yo, M.; Sakaida, I. Clinical impact of endoscopic papillectomy for benign-malignant borderline lesions of the major duodenal papilla. J. Hepatobiliary Pancreat. Sci. 2011, 18, 190–194. [Google Scholar] [CrossRef]
- Bellizzi, A.M.; Kahaleh, M.; Stelow, E.B. The assessment of specimens procured by endoscopic ampullectomy. Am. J. Clin. Pathol. 2009, 132, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Sakai, A.; Tsujimae, M.; Masuda, A.; Iemoto, T.; Ashina, S.; Yamakawa, K.; Tanaka, T.; Tanaka, S.; Yamada, Y.; Nakano, R.; et al. Clinical outcomes of ampullary neoplasms in resected margin positive or uncertain cases after endoscopi papillectomy. World J. Gastroenterol. 2019, 23, 1387–1397. [Google Scholar] [CrossRef] [PubMed]
- Norton, I.D.; Gostout, C.J.; Baron, T.H.; Geller, A.; Petersen, B.T.; Wiersema, M.J. Safety and outcome of endoscopic snare excision of the major duodenal papilla. Gastrointest. Endosc. 2002, 56, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.M.; Kim, M.H.; Kim, M.J.; Jang, S.J.; Lee, T.Y.; Kwon, S.; Oh, H.C.; Lee, S.S.; Seo, D.W.; Lee, S.K. Focal early stage cancer in ampullary adenoma: Surgery or endoscopic papillectomy? Gastrointest. Endosc. 2007, 66, 701–707. [Google Scholar] [CrossRef]
- Iwasaki, E.; Minami, K.; Itoi, T.; Yamamoto, K.; Tsuji, S.; Sofuni, A.; Tsuchiya, T.; Tanaka, R.; Tonozuka, R.; Machida, Y.; et al. Impact of electrical pulse cut mode during endoscopic papillectomy: Pilot randomized clinical trial. Dig. Endosc. 2020, 32, 127–135. [Google Scholar] [CrossRef]
- Minami, K.; Iwasaki, E.; Fukuhara, S.; Horibe, M.; Seino, T.; Kawasaki, S.; Katayama, T.; Takimoto, Y.; Tamagawa, H.; Machida, Y.; et al. Electric Endocut and Autocut Resection for Endoscopic Papillectomy: A Systematic Review. Intern. Med. 2019, 58, 2767–2772. [Google Scholar] [CrossRef]
- Elta, G.H.; Barnett, J.L.; Wille, R.T.; Brown, K.A.; Chey, W.D.; Scheiman, J.M. Pure-cut electrocautery current for sphincterotomy causes less postprocedural pancreatitis than a blended current. Gastrointest. Endosc. 1998, 47, 149–153. [Google Scholar] [CrossRef]
- Stefanidis, G.; Karamanolis, G.; Viazis, N.; Sgouros, S.; Papadopoulou, E.; Ntatsakis, K.; Mantides, A.; Nastos, H. Comparative study of post-endoscopic sphincterotomy complications associated with various types of electrosurgical currents in patients with choledocholithiasis. Gastrointest. Endosc. 2003, 57, 192–197. [Google Scholar] [CrossRef]
- Ridtitid, W.; Tan, D.; Schmidt, S.E.; Fogel, E.L.; McHenry, L.; Watkins, J.L.; Lehman, G.A.; Sherman, S.; Coté, G.A. Endoscopic papillectomy: Risk factors for incomplete resection and recurrence during long-term follow-up. Gastrointest. Endosc. 2014, 79, 289–296. [Google Scholar] [CrossRef]
- Yasuda, I.; Kobayashi, S.; Takahashi, K.; Nanjo, S.; Mihara, H.; Kajiura, S.; Ando, T.; Tajiri, K.; Fujinami, H. Management of Remnant or Recurrent Lesions after Endoscopic Papillectomy. Clin. Endosc. 2020, 53, 659–662. [Google Scholar] [CrossRef]
- Choi, S.J.; Lee, H.S.; Kim, J.; Choe, J.W.; Lee, J.M.; Hyun, J.J.; Yoon, J.H.; Kim, H.J.; Kim, J.S.; Choi, H.S. Clinical outcomes of endoscopic papillectomy for ampullary adenoma: A multicenter study. World J. Gastroenterol. 2022, 28, 1845–1859. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, H.; Ohno, E.; Ishikawa, T.; Iida, T.; Tanaka, H.; Furukawa, K.; Nakamura, M.; Honda, T.; Hashimoto, S.; Itoh, A.; et al. Endoscopic papillectomy for ampullary adenoma and early adenocarcinoma: Analysis of factors related to treatment outcomes and long-term prognosis. Dig. Endosc. 2021, 33, 858–869. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Cheon, J.H.; Kim, T.I.; Baik, S.H.; Kim, N.K.; Kim, H.; Kim, W.H. Effectiveness of radical surgery after incomplete endoscopic mucosal resection for early colorectal cancer: A clinical study investigating the risk factors for residual cancer. Dig. Dis. Sci. 2008, 53, 2941–2946. [Google Scholar] [CrossRef]
- Cecinato, P.; Parmeggiani, F.; Braglia, L.; Carlinfante, G.; Zecchini, R.; Decembrino, F.; Iori, V.; Sereni, G.; Tioli, C.; Cavina, M.; et al. Endoscopic papillectomy for ampullary adenomas: Different outcomes in sporadic tumors and familial adenomatous polyps. J. Gastrointest. Surg. 2021, 25, 457–466. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Values |
|---|---|
| Age (years) | 67 (55–76) |
| Sex (male/female) | 55/15 |
| Familial adenomatous polyposis, n (%) | 10 (13.9%) |
| Clinical presentation, n (%) | |
| Incidental findings | 55 (78.5%) |
| Symptomatic | 15 (21.4%) |
| Tumor size (mm) | 12 (8.8–16.3) |
| Resection, n (%) | |
| En block | 61 (87.1%) |
| Piecemeal | 9 (12.9%) |
| Early complications, n (%) | 15 (20.8%) |
| Pancreatitis/cholangitis/bleeding/stent migration | 4/8/2/1 |
| Late complications, n (%) | 8 (11.1%) |
| Pancreatitis/biliary stone/cholangitis | 4/3/1 |
| Final pathological diagnosis, n (%) | |
| Adenoma | 56 (80.0%) |
| High-grade dysplasia, adenocarcinoma | 13 (18.6%) |
| Adenomyomatosis | 1 (1.4%) |
| Resection margin, n (%) | |
| Negative | 27 (38.6%) |
| Positive | 15 (21.4%) |
| Uncertain | 28 (40.0%) |
| Follow-up period (months) | 47 (22–84) |
| Data are expressed as number (percentage) or median (interquartile ranges) | |
| Evaluable Margin (n = 42) | Unevaluable Margin (n = 28) | p Value | |
|---|---|---|---|
| Age (years) | 68 (60–77) | 63 (53–74) | 0.332 |
| Sex (male/female) | 34/8 | 21/7 | 0.567 |
| Familial adenomatous polyposis, n (%) | 4 (9.5%) | 6 (21.4%) | 0.183 |
| Resection, n (%) | 0.468 | ||
| En block | 38 (90.5%) | 23 (82.1%) | |
| Piecemeal | 4 (9.5%) | 5 (17.9%) | |
| Tumor size (mm) | 12 (9–15) | 10.5 (8–17.5) | 0.276 |
| Pathological diagnosis, n (%) | 0.854 | ||
| Adenoma | 34 (81.0%) | 22 (78.6%) | |
| High-grade dysplasia, adenocarcinoma | 7 (16.7%) | 6 (21.4%) | |
| Adenomyomatosis | 1 (2.4%) | 0 |
| Case | Age (Years) | Sex | FAP | Size (mm) | Pathological Final Diagnosis | Resection Margin | HM/VM | En Block/Piecemeal Resection | Pathological Residual Diagnosis | Post-Treatment | Time to Recurrence (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 53 | M | + | 5 | Adenoma | Negative | -/- | En block | Adenoma | PD | 3 |
| 2 | 76 | M | - | 15 | Adenoma | Positive | -/+ | En block | Adenoma | EP | 3 |
| 3 | 73 | M | - | 15 | Adenoma | Positive | -/+ | Piecemeal | Adenoma | EP | 3 |
| 4 | 37 | F | + | 18 | Adenoma | Positive | -/+ | En block | Adenoma | Follow-up | 3 |
| 5 | 82 | F | - | 10 | Adenoma | Positive | +/- | En block | Adenoma | EP | 6 |
| 6 | 27 | M | + | 6 | Adenoma | Positive | +/- | En block | Adenoma | EP | 50 |
| 7 | 59 | F | - | 10 | Adenoma | Uncertain | X/X | Piecemeal | Adenoma | APC | 3 |
| 8 | 81 | F | - | 25 | Adenoma | Uncertain | X/X | Piecemeal | Adenoma | Follow-up | 6 |
| 9 | 66 | F | - | 10 | Adenocarcinoma T1a | Uncertain | X/X | En block | Adenoma | PD | 3 |
| 10 | 83 | M | - | 16 | Adenocarcinoma T1a | Uncertain | X/X | En block | Adenoma | EP | 3 |
| 11 | 88 | M | + | 12 | Adenocarcinoma T1a | Uncertain | X/X | En block | Adenoma | Follow-up | 3 |
| No Residual Recurrence (n = 59) | Residual Recurrence (n = 11) | p Value | |
|---|---|---|---|
| Age (years) | 66 (58–74) | 73 (37–82) | 0.744 |
| Sex (male/female) | 50/9 | 5/6 | 0.009 |
| Familial adenomatous polyposis, n (%) | 6 (10.2%) | 4 (36.4%) | 0.044 |
| Resection, n (%) | 0.143 | ||
| En block | 53 (89.8%) | 8 (72.7%) | |
| Piecemeal | 6 (10.2%) | 3 (27.3%) | |
| Tumor size (mm) | 12 (8–15) | 10 (7–17.5) | 0.931 |
| Pathological diagnosis, n (%) | 0.513 | ||
| Adenoma | 48 (81.4%) | 8 (72.7%) | |
| High-grade dysplasia, adenocarcinoma | 10 (16.9%) | 3 (27.2%) | |
| Adenomyomatosis | 1 (1.7%) | 0 | |
| Resection margin, n (%) | 0.041 | ||
| Negative | 26 (44.1%) | 1 (9.1%) | |
| Positive/Uncertain | 33 (55.9%) | 10 (90.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyamoto, S.; Serikawa, M.; Ishii, Y.; Tatsukawa, Y.; Nakamura, S.; Ikemoto, J.; Tamura, Y.; Nakamura, K.; Furukawa, M.; Yamashita, Y.; et al. The Significance of Histopathological Findings on Clinical Outcomes in Endoscopic Papillectomy with Endocut. J. Clin. Med. 2023, 12, 6853. https://doi.org/10.3390/jcm12216853
Miyamoto S, Serikawa M, Ishii Y, Tatsukawa Y, Nakamura S, Ikemoto J, Tamura Y, Nakamura K, Furukawa M, Yamashita Y, et al. The Significance of Histopathological Findings on Clinical Outcomes in Endoscopic Papillectomy with Endocut. Journal of Clinical Medicine. 2023; 12(21):6853. https://doi.org/10.3390/jcm12216853
Chicago/Turabian StyleMiyamoto, Sayaka, Masahiro Serikawa, Yasutaka Ishii, Yumiko Tatsukawa, Shinya Nakamura, Juri Ikemoto, Yosuke Tamura, Kazuki Nakamura, Masaru Furukawa, Yumiko Yamashita, and et al. 2023. "The Significance of Histopathological Findings on Clinical Outcomes in Endoscopic Papillectomy with Endocut" Journal of Clinical Medicine 12, no. 21: 6853. https://doi.org/10.3390/jcm12216853
APA StyleMiyamoto, S., Serikawa, M., Ishii, Y., Tatsukawa, Y., Nakamura, S., Ikemoto, J., Tamura, Y., Nakamura, K., Furukawa, M., Yamashita, Y., Iijima, N., Arihiro, K., & Oka, S. (2023). The Significance of Histopathological Findings on Clinical Outcomes in Endoscopic Papillectomy with Endocut. Journal of Clinical Medicine, 12(21), 6853. https://doi.org/10.3390/jcm12216853