
Rehabilitation Exercises Supported by Monitor-Augmented Reality for Patients with High-Grade Glioma Undergoing Radiotherapy: Results of a Randomized Clinical Trial

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Sample Size
2.4. Radiotherapy Procedure
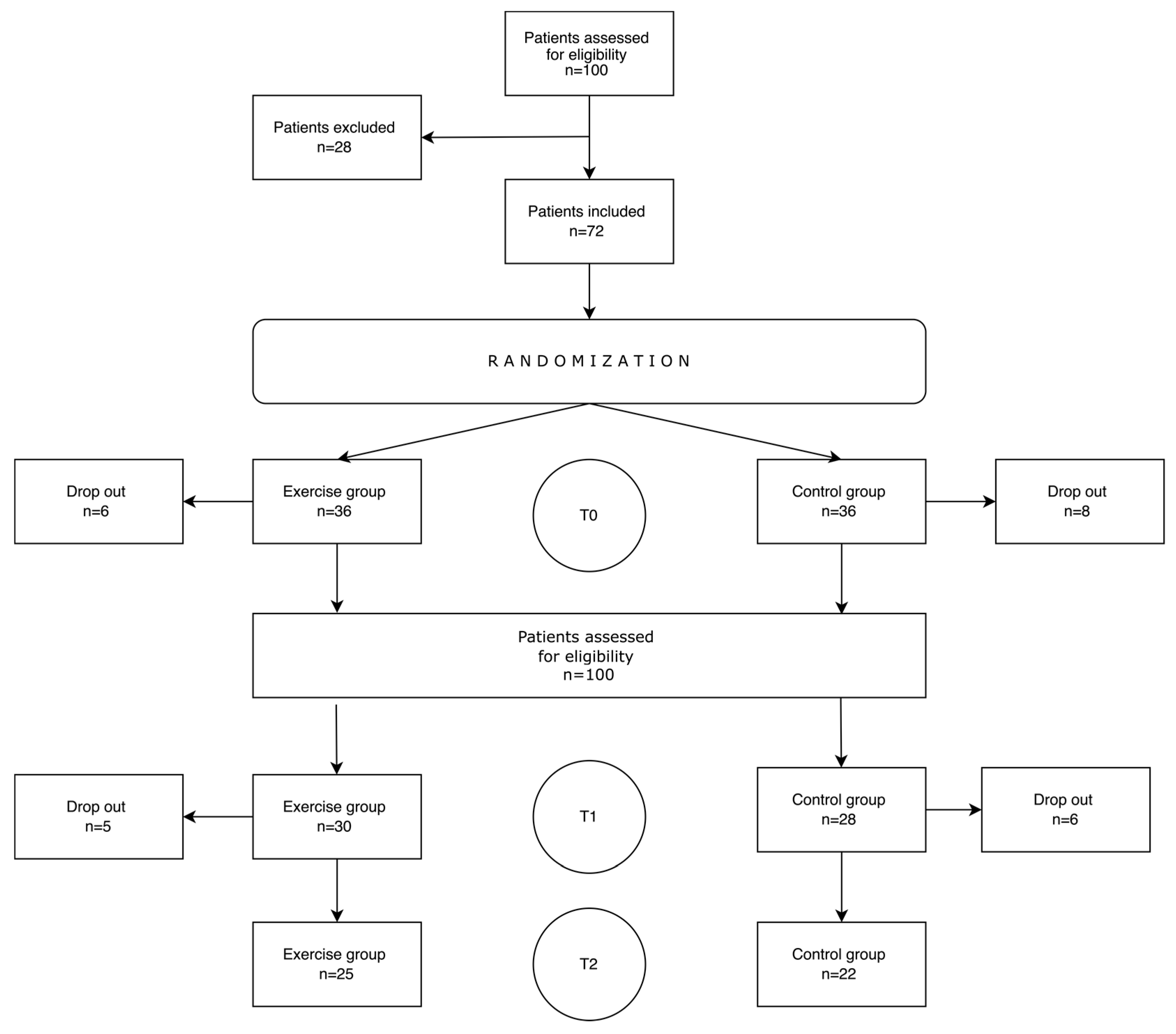
2.5. Randomization
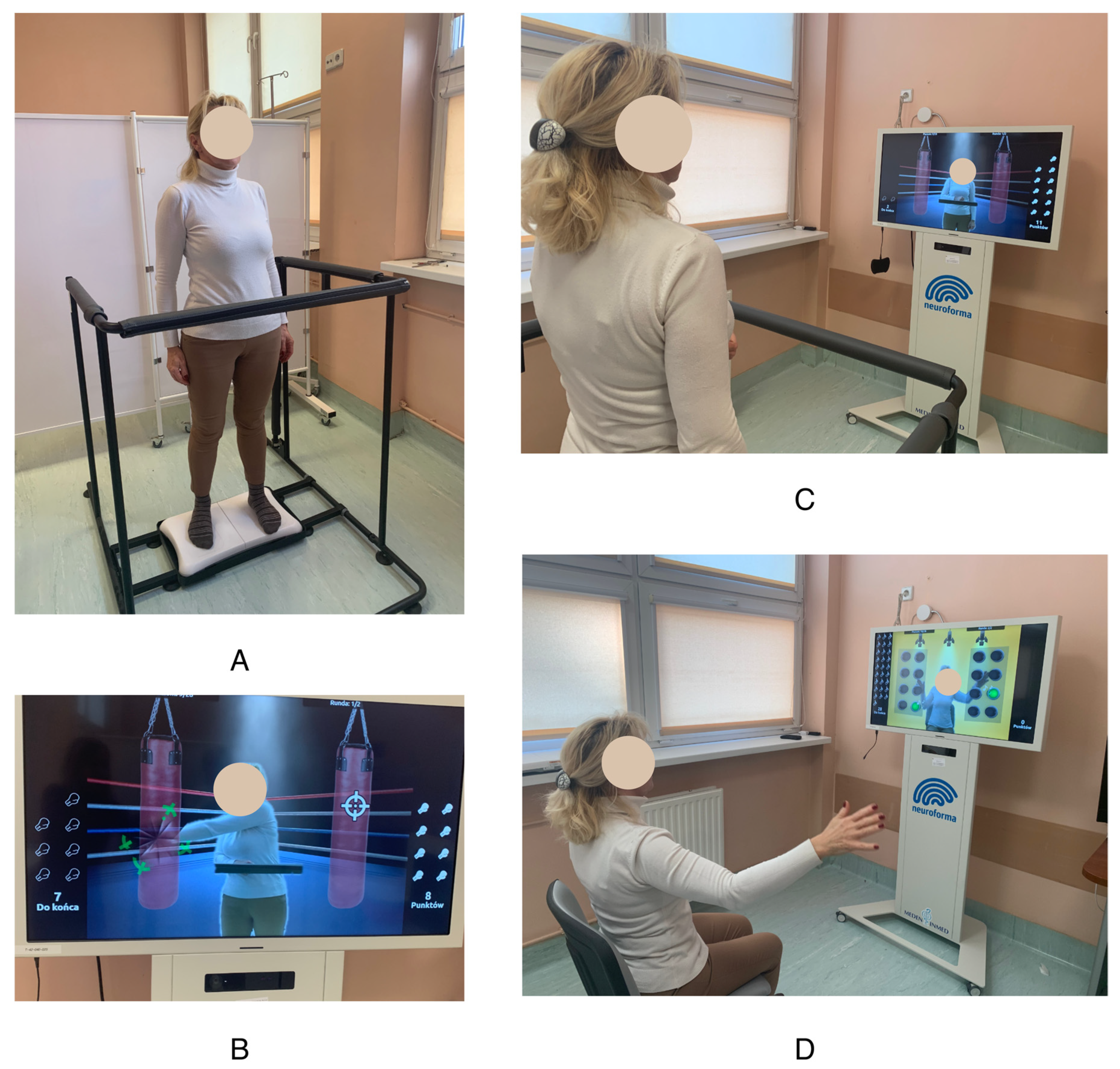
2.6. Exercise Program
2.7. Control Group
2.8. Study Scheme
2.9. Measurements
2.9.1. Hand Grip Strength (HGS) Test
2.9.2. 6-Minute Walk Test (6MWT)
2.9.3. Timed Up and Go (TUG) Test
2.9.4. The Functional Independence Measure (FIM)
2.9.5. Quality of Life
2.9.6. Fatigue
2.9.7. Depression and Anxiety
2.9.8. Addenbrooke’s Cognitive Examination III (ACE III)
2.9.9. Laboratory Tests
2.10. Statistical Analysis
3. Results
3.1. Physical Fitness, Mental Health, and Quality of Life Results
3.2. Laboratory Test Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Parameters (Mean ± SD) | Baseline | After RT | After 3 Months | p-Value |
|---|---|---|---|---|
| S-100 µg/L | 0.04 ± 0.02 | 0.04 ± 0.02 | 0.04 ± 0.02 | 0.223 |
| Sodium mmol/L | 139.88 ± 2.06 | 142.63 ± 4.37 | 139.17 ± 2.48 | 0.459 |
| Potassium mmol/L | 4.25 ± 0.36 | 4.35 ± 0.57 | 4.00 ± 0.15 | 0.789 |
| Glucose mg/dL | 94.69 ± 7.85 | 95.45 ± 15.58 | 99.50 ± 14.34 | 0.534 |
| Creatinine mg/dL | 0.87 ± 0.17 | 0.92 ± 0.18 | 0.97± 0.22 | 0.496 |
| AST U/L | 18.44 ± 5.34 | 18.90 ± 9.61 | 20.83 ± 4.36 | 0.311 |
| ALT U/L | 26.69 ± 12.20 | 34.80 ± 32.50 | 33.67± 18.77 | 0.401 |
| Bilirubin mg/dL | 0.50 ± 0.37 | 0.66 ± 0.41 | 0.76 ± 0.50 | 0.105 |
| WBC G/L | 7.95 ± 2.46 | 8.25 ± 3.54 | 8.55 ± 3.76 | 0.937 |
| LYM G/L | 2.01 ± 0.67 | 1.79 ± 0.90 | 1.73 ± 0.84 | 0.148 |
| NEU G/L | 5.14 ± 1.89 | 5.69 ± 2.93 | 5.97 ± 3.35 | 0.913 |
| MON G/L | 0.60 ± 0.26 | 0.62 ± 0.27 | 0.65 ± 0.26 | 0.803 |
| EOS G/L | 0.12 ± 0.10 | 0.14 ± 0.17 | 0.18 ± 0.25 | 0.661 |
| IG G/L | 0.08 ± 0.12 | 0.07 ± 0.07 | 0.12 ± 0.20 | 0.704 |
| BASO G/L | 0.04 ± 0.03 | 0.01 ± 0.02 | 0.02 ± 0.02 | 0.423 |
| RBC T/L | 4.71 ± 0.38 | 4.67 ± 0.56 | 4.68 ± 0.53 | 0.523 |
| HBG mmol/L | 8.59 ± 0.74 | 8.85 ± 1.07 | 8.69 ± 0.71 | 0.289 |
| HCT L/L | 0.42 ± 0.03 | 0.43 ± 0.05 | 0.42 ± 0.03 | 0.307 |
| MCV fL | 88.82 ± 4.89 | 91.34 ± 4.15 | 90.98 ± 7.24 | 0.029 b |
| MCH fmol | 1.83 ± 0.13 | 1.90 ± 0.10 | 1.88 ± 0.19 | 0.023 b |
| MCHC mmol/L | 20.54 ± 0.55 | 20.79 ± 0.43 | 20.57 ± 0.53 | 0.305 |
| PLT G/L | 267.94 ± 81.01 | 187.60 ± 51.45 | 229.17 ± 55.62 | 0.148 |
| BDNF pg/mL | 233.89 ± 222.25 | 242.94 ± 188.68 | 330.67 ± 297.57 | 0.847 |
| Parameters (Mean ± SD) | Baseline | After RT | After 3 Months | p-Value |
|---|---|---|---|---|
| S-100 µg/L | 0.13 ± 0.17 | 0.06 ± 0.05 | 0.07 ± 0.04 | 0.105 |
| Sodium mmol/L | 139.50 ± 2.99 | 139.17 ± 3.06 | 140.25 ± 2.19 | 0.09 |
| Potassium mmol/L | 4.12 ± 0.22 | 4.05 ± 0.33 | 4.07 ± 0.22 | 0.441 |
| Glucose mg/dL | 110.63 ± 27.50 | 98.86 ± 26.28 | 108.88 ± 26.71 | 0.779 |
| Creatinine mg/dL | 0.79 ± 0.10 | 0.87 ± 0.15 | 0.77 ± 0.05 | 0.075 |
| AST U/L | 18.93 ± 5.93 | 23.33 ± 16.00 | 20.00 ± 9.01 | 0.738 |
| ALT U/L | 31.53 ± 23.51 | 43.44 ± 17.52 | 39.75 ± 29.60 | 0.513 |
| Bilirubin mg/dL | 0.39 ± 0.12 | 0.44 ± 0.12 | 0.30 ± 0.09 | 0.094 |
| WBC G/L | 8.76 ± 3.88 | 6.90 ± 2.01 | 6.83 ± 2.60 | 0.399 |
| LYM G/L | 1.71 ± 0.76 | 1.34 ± 0.54 | 1.23 ± 0.65 | 0.186 |
| NEU G/L | 6.34 ± 3.32 | 5.14 ± 1.72 | 5.22 ± 2.36 | 0.686 |
| MON G/L | 0.56 ± 0.23 | 0.53 ± 0.21 | 0.38 ± 0.14 | 0.206 |
| EOS G/L | 0.07 ± 0.07 | 0.07 ± 0.11 | 0.04 ± 0.06 | 0.513 |
| IG G/L | 0.14 ± 0.24 | 0.06 ± 0.10 | 0.11 ± 0.18 | 0.216 |
| BASO G/L | 0.03 ± 0.04 | 0.01 ± 0.01 | 0.02 ± 0.03 | 0.129 |
| RBC T/L | 4.34 ± 0.40 | 4.30 ± 0.36 | 4.08 ± 0.43 | 0.149 |
| HBG mmol/L | 8.31 ± 0.77 | 8.34 ± 0.71 | 8.08 ± 0.80 | 0.658 |
| HCT L/L | 0.40 ± 0.03 | 0.40 ± 0.04 | 0.39 ± 0.03 | 0.760 |
| MCV fL | 92.31 ± 3.05 | 93.26 ± 2.31 | 96.37 ± 5.64 | 0.014 b |
| MCH fmol | 1.91 ± 0.07 | 1.94 ± 0.06 | 1.99 ± 0.10 | 0.0285 a,c |
| MCHC mmol/L | 20.75 ± 0.47 | 20.84 ± 0.45 | 20.65 ± 0.45 | 0.559 |
| PLT G/L | 253.75 ± 77.37 | 211.86 ± 71.76 | 187.10 ± 52.20 | 0.202 |
| BDNF pg/mL | 386.02 ± 369.26 | 227.69 ± 149.58 | 143.24 ± 99.94 | 0.234 |
| Parameters | T0 and T1 | T1 and T2 | T0 and T2 | |||
|---|---|---|---|---|---|---|
| EG | CG | EG | CG | EG | CG | |
| S-100 µg/L | 0.00 ± 0.02 | −0.07 ± 0.17 | −0.01 ± 0.02 | −0.01 ± 0.07 | −0.01 ± 0.02 | −0.11 ± 0.19 |
| Sodium mmol/L | 2.63 ± 4.60 | 0.17 ± 2.48 | −3.50 ± 7.90 | 1.80 ± 1.10 | 0.00 ± 3.10 | 1.75 ± 2.25 |
| Potassium mmol/L | 0.18 ± 0.67 | −0.04 ± 0.33 | 0.16 ± 0.15 | 0.10 ± 0.29 | −0.01 ± 0.35 | −0.06 ± 0.28 |
| Glucose mg/dL | 2.82 ± 11.49 | −6.14 ± 22.16 | 5.80 ± 22.16 | −14.75 ± 35.69 | 3.17 ± 16.99 | −0.50 ± 39.83 |
| Creatinine mg/dL | 0.07 ± 0.13 | 0.11 ± 0.12 | −0.01 ± 0.12 | −0.09 ± 0.14 | −0.01 ± 0.12 | −0.09 ± 0.14 |
| AST U/L | −0.60 ± 11.17 | 3.44 ± 10.86 | 3.33 ± 5.20 | 0.50 ± 5.47 | −0.83 ± 5.78 | 0.88 ± 7.51 |
| ALT U/L | 6.90 ± 35.31 | 9.78 ± 12.53 | 6.67 ± 20.11 | 5.50 ± 23.67 | 2.50 ± 13.53 | 4.25 ± 33.88 |
| Bilirubin mg/dL | 0.24 ± 0.26 | 0.08 ± 0.17 | −0.04 ± 0.07 | −0.15 ± 0.10 | 0.30 ± 0.41 * | −0.07 ± 0.10 * |
| WBC G/L | 0.37 ± 3.12 | −1.57 ± 4.37 | −0.37 ± 3.39 | 0.66 ± 1.97 | −0.02 ± 3.65 | −0.88 ± 4.11 |
| LYM G/L | −0.11 ± 0.90 | −0.33 ± 0.57 | −0.36 ± 0.96 | −0.05 ± 0.42 | −0.33 ± 0.68 | −0.29 ± 0.53 |
| NEU G/L | 0.51 ± 2.77 | −0.95 ± 3.51 | −0.01 ± 3.48 | 0.60 ± 2.16 | 0.29 ± 3.13 | −0.29 ± 3.88 |
| MON G/L | 0.02 ± 0.21 | −0.02 ± 0.29 | −0.02 ± 0.32 | −0.09 ± 0.19 | 0.03 ± 0.35 | −0.13 ± 0.15 |
| EOS G/L | 0.02 ± 0.20 | 0.01 ± 0.13 | 0.02 ± 0.18 | −0.01 ± 0.08 | 0.06 ± 0.24 | 0.00 ± 0.09 |
| IG G/L | −0.02 ± 0.10 | −0.09 ± 0.20 | 0.05 ± 0.20 | 0.06 ± 0.22 | 0.02 ± 0.21 | −0.07 ± 0.33 |
| BASO G/L | −0.02 ± 0.04 | −0.02 ± 0.04 | −0.02 ± 0.03 | −0.01 ± 0.03 | −0.02 ± 0.03 | −0.01 ± 0.03 |
| RBC T/L | 0.02 ± 0.42 | −0.09 ± 0.45 | −0.14 ± 0.36 | −0.23 ± 0.35 | 0.00 ± 0.39 | −0.32 ± 0.64 |
| HBG mmol/L | 0.27 ± 0.70 | −0.07 ± 0.73 | −0.23 ± 0.66 | −0.21 ± 0.81 | 0.26 ± 0.62 | −0.24 ± 1.06 |
| HCT L/L | 0.01 ± 0.04 | 0.00 ± 0.04 | −0.01 ± 0.03 | −0.01 ± 0.03 | 0.01 ± 0.03 | −0.01 ± 0.04 |
| MCV fL | 1.75 ± 2.27 | 1.04 ± 1.74 | 0.70 ± 2.69 | 3.85 ± 5.70 | 0.70 ± 2.69 | 3.85 ± 5.70 |
| MCH fmol | 0.05 ± 0.07 | 0.02 ± 0.05 | 0.01 ± 0.06 | 0.06 ± 0.09 | 0.01 ± 0.06 | 0.06 ± 0.09 |
| MCHC mmol/L | 0.22 ± 0.51 | 0.02 ± 0.32 | −0.06 ± 0.34 | −0.18 ± 0.77 | 0.13 ± 0.43 | −0.11 ± 0.61 |
| PLT G/L | −77.73 ± 100.23 | −37.93 ± 101.16 | 22.00 ± 52.23 | −28.30 ± 70.23 | −49.08 ± 72.23 | −54.50 ± 86.43 |
| BDNF pg/mL | 9.05 ± 237.11 | −189.70 ± 409.98 | 87.73 ± 202.68 | −106.78 ± 194.25 | 96.78 ± 407.53 | −285.83 ± 455.51 |
References
- Kumari, S.; Gupta, R.; Ambasta, R.K.; Kumar, P. Multiple therapeutic approaches of glioblastoma multiforme: From terminal to therapy. Biochim. Biophys. Acta Rev. Cancer 2023, 1878, 188913. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.C.; Ashley, D.M.; López, G.Y.; Malinzak, M.; Friedman, H.S.; Khasraw, M. Management of glioblastoma: State of the art and future directions. CA Cancer J. Clin. 2020, 70, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Kushner, D.S.; Amidei, C. Rehabilitation of motor dysfunction in primary brain tumor patients. Neurooncol. Pract. 2015, 2, 185–191. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dilalla, V.; Chaput, G.; Williams, T.; Sultanem, K. Radiotherapy side effects: Integrating a survivorship clinical lens to better serve patients. Curr. Oncol. 2020, 27, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Asher, A.; Fu, J.B.; Bailey, C.; Hughes, J.K. Fatigue among patients with brain tumors. CNS Oncol. 2016, 5, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Schiff, D.; Alyahya, M. Neurological and Medical Complications in Brain Tumor Patients. Curr. Neurol. Neurosci. Rep. 2020, 20, 33. [Google Scholar] [CrossRef] [PubMed]
- Coomans, M.B.; Dirven, L.; Aaronson, N.; Baumert, B.G.; van den Bent, M.; Bottomley, A.; Brandes, A.A.; Chinot, O.; Coens, C.; Gorlia, T.; et al. Factors associated with health-related quality of life (HRQoL) deterioration in glioma patients during the progression-free survival period. Neuro Oncol. 2022, 24, 2159–2169. [Google Scholar] [CrossRef]
- Ståhl, P.; Henoch, I.; Smits, A.; Rydenhag, B.; Ozanne, A. Quality of life in patients with glioblastoma and their relatives. Acta Neurol. Scand. 2022, 146, 82–91. [Google Scholar] [CrossRef]
- Taphoorn, M.J.B.; Henriksson, R.; Bottomley, A.; Cloughesy, T.; Wick, W.; Mason, W.P.; Saran, F.; Nishikawa, R.; Hilton, M.; Theodore-Oklota, C.; et al. Health-Related Quality of Life in a Randomized Phase III Study of Bevacizumab, Temozolomide, and Radiotherapy in Newly Diagnosed Glioblastoma. J. Clin. Oncol. 2015, 33, 2166–2175. [Google Scholar] [CrossRef]
- Spina, S.; Facciorusso, S.; Cinone, N.; Pellegrino, R.; Fiore, P.; Santamato, A. Rehabilitation interventions for glioma patients: A mini-review. Front. Surg. 2023, 10, 1137516. [Google Scholar] [CrossRef]
- Sandler, C.X.; Matsuyama, M.; Jones, T.L.; Bashford, J.; Langbecker, D.; Hayes, S.C. Physical activity and exercise in adults diagnosed with primary brain cancer: A systematic review. J. Neurooncol. 2021, 153, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.; Pedersen, C.B.; Jarden, J.O.; Beier, D.; Minet, L.R.; Søgaard, K. Effectiveness of Physical Therapy- and Occupational Therapy-Based Rehabilitation in People Who Have Glioma and Are Undergoing Active Anticancer Treatment: Single-Blind, Randomized Controlled Trial. Phys. Ther. 2020, 100, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Steindorf, K.; Depenbusch, J.; Haussmann, A.; Tsiouris, A.; Schmidt, L.; Hermann, S.; Sieverding, M.; Wiskemann, J.; Ungar, N. Change patterns and determinants of physical activity differ between breast, prostate, and colorectal cancer patients. Support. Care Cancer 2020, 28, 3207–3218. [Google Scholar] [CrossRef] [PubMed]
- Pieczyńska, A.; Pilarska, A.; Hojan, K. Predictors of functional outcomes in adults with brain tumor undergoing rehabilitation treatment: A systematic review. Eur. J. Phys. Rehabil. Med. 2022, 58, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Hojan, K.; Gerreth, K. Can Multidisciplinary Inpatient and Outpatient Rehabilitation Provide Sufficient Prevention of Disability in Patients with a Brain Tumor?-A Case-Series Report of Two Programs and A Prospective, Observational Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 6488. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.; Chun, M.H.; Lee, S.J.; Kim, B.R. Effect of virtual reality-based rehabilitation on upper-extremity function in patients with brain tumor: Controlled trial. Am. J. Phys. Med. Rehabil. 2015, 94, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Chun, M.H.; Son, Y.R. Effect of virtual reality on cognitive dysfunction in patients with brain tumor. Ann. Rehabil. Med. 2014, 38, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Gil, M.J.V.; Gonzalez-Medina, G.; Lucena-Anton, D.; Perez-Cabezas, V.; Ruiz-Molinero, M.D.C.; Martín-Valero, R. Augmented Reality in Physical Therapy: Systematic Review and Meta-analysis. JMIR Serious Games 2021, 9, e30985. [Google Scholar] [CrossRef]
- Denche-Zamorano, A.; Rodriguez-Redondo, Y.; Barrios-Fernandez, S.; Mendoza-Muñoz, M.; Castillo-Paredes, A.; Rojo-Ramos, J.; Garcia-Gordillo, M.A.; Adsuar, J.C. Rehabilitation Is the Main Topic in Virtual and Augmented Reality and Physical Activity Research: A Bibliometric Analysis. Sensors 2023, 23, 2987. [Google Scholar] [CrossRef]
- Yang, Z.-Q.; Du, D.; Wei, X.-Y.; Tong, R.K.-Y. Augmented reality for stroke rehabilitation during COVID-19. J. Neuroeng. Rehabil. 2022, 19, 136. [Google Scholar] [CrossRef]
- Cerdán de Las Heras, J.; Tulppo, M.; Kiviniemi, A.M.; Hilberg, O.; Løkke, A.; Ekholm, S.; Catalán-Matamoros, D.; Bendstrup, E. Augmented reality glasses as a new tele-rehabilitation tool for home use: Patients’ perception and expectations. Disabil. Rehabil. Assist. Technol. 2022, 17, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Weyer-Jamora, C.; Brie, M.S.; Luks, T.L.; Smith, E.M.; Hervey-Jumper, S.L.; Taylor, J.W. Postacute Cognitive Rehabilitation for Adult Brain Tumor Patients. Neurosurgery 2021, 89, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Pilarska, A.; Pieczyńska, A.; Hojan, K. Neuropsychological monitoring of cognitive function and ICF-based mental components in patients with malignant brain tumours. Front. Psychol. 2023, 14, 1033185. [Google Scholar] [CrossRef] [PubMed]
- Colucci-D’Amato, L.; Speranza, L.; Volpicelli, F. Neurotrophic Factor BDNF, Physiological Functions and Therapeutic Potential in Depression, Neurodegeneration and Brain Cancer. Int. J. Mol. Sci. 2020, 21, 7777. [Google Scholar] [CrossRef] [PubMed]
- Miranda, M.; Morici, J.F.; Zanoni, M.B.; Bekinschtein, P. Brain-Derived Neurotrophic Factor: A Key Molecule for Memory in the Healthy and the Pathological Brain. Front. Cell. Neurosci. 2019, 13, 363. [Google Scholar] [CrossRef] [PubMed]
- Miklja, Z.; Gabel, N.; Altshuler, D.; Wang, L.; Hervey-Jumper, S.L.; Smith, S. Exercise improves health-related quality of life sleep and fatigue domains in adult high- and low-grade glioma patients. Support. Care Cancer 2022, 30, 1493–1500. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Mao, X.; Ye, L.; Cheng, H.; Dai, X. The Role of the S100 Protein Family in Glioma. J. Cancer 2022, 13, 3022–3030. [Google Scholar] [CrossRef]
- Mokhtarzade, M.; Motl, R.; Negaresh, R.; Zimmer, P.; Khodadoost, M.; Baker, J.S.; Patel, D.; Majdinasab, N.; Ranjbar, R. Exercise-induced changes in neurotrophic factors and markers of blood-brain barrier permeability are moderated by weight status in multiple sclerosis. Neuropeptides 2018, 70, 93–100. [Google Scholar] [CrossRef]
- Barha, C.K.; Hsiung, G.Y.R.; Liu-Ambrose, T. The Role of S100B in Aerobic Training Efficacy in Older Adults with Mild Vascular Cognitive Impairment: Secondary Analysis of a Randomized Controlled Trial. Neuroscience 2019, 410, 176–182. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Scaringi, C.; Agolli, L.; Minniti, G. Technical Advances in Radiation Therapy for Brain Tumors. Anticancer Res. 2018, 38, 6041–6045. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.A.; Andrews, K.S.; Brooks, D.; Fedewa, S.A.; Manassaram-Baptiste, D.; Saslow, D.; Brawley, O.W.; Wender, R.C. Cancer screening in the United States, 2017: A review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J. Clin. 2017, 67, 100–121. [Google Scholar] [CrossRef] [PubMed]
- Doyle, C.; Kushi, L.H.; Byers, T.; Courneya, K.S.; Demark-Wahnefried, W.; Grant, B.; McTiernan, A.; Rock, C.L.; Thompson, C.; Gansler, T.; et al. Nutrition and physical activity during and after cancer treatment: An American Cancer Society guide for informed choices. CA Cancer J. Clin. 2006, 56, 323–353. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, E.; Thalla, N.; Nepaul, S.; Wisotzky, E. Outcome Measures in Cancer Rehabilitation: Pain, Function, and Symptom Assessment. Front. Pain. Res. 2021, 2, 692237. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Esteban-Simón, A.; Díez-Fernández, D.M.; Artés-Rodríguez, E.; Casimiro-Artés, M.Á.; Rodríguez-Pérez, M.A.; Moreno-Martos, H.; Casimiro-Andújar, A.J.; Soriano-Maldonado, A. Absolute and Relative Handgrip Strength as Indicators of Self-Reported Physical Function and Quality of Life in Breast Cancer Survivors: The EFICAN Study. Cancers 2021, 13, 5292. [Google Scholar] [CrossRef] [PubMed]
- Hadzibegovic, S.; Porthun, J.; Lena, A.; Weinländer, P.; Lück, L.C.; Potthoff, S.K.; Rösnick, L.; Fröhlich, A.-K.; Ramer, L.V.; Sonntag, F.; et al. Hand grip strength in patients with advanced cancer: A prospective study. J. Cachexia Sarcopenia Muscle 2023, 14, 1682–1694. [Google Scholar] [CrossRef]
- MacDermid, J.C.; Solomon, G.S.; Valdes, K.A. Clinical Assessment Recommendations, 3rd ed.; American Society of Hand Therapists: Mount Laurel, NJ, USA, 2015; ISBN 9780692525159. [Google Scholar]
- Michael, C.M.; Lehrer, E.J.; Schmitz, K.H.; Zaorsky, N.G. Prehabilitation exercise therapy for cancer: A systematic review and meta-analysis. Cancer Med. 2021, 10, 4195–4205. [Google Scholar] [CrossRef]
- Agarwala, P.; Salzman, S.H. Six-Minute Walk Test: Clinical Role, Technique, Coding, and Reimbursement. Chest 2020, 157, 603–611. [Google Scholar] [CrossRef]
- Kear, B.M.; Guck, T.P.; McGaha, A.L. Timed Up and Go (TUG) Test: Normative Reference Values for Ages 20 to 59 Years and Relationships with Physical and Mental Health Risk Factors. J. Prim. Care Community Health 2017, 8, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Noll, K.R.; Bradshaw, M.E.; Weinberg, J.S.; Wefel, J.S. Neurocognitive functioning is associated with functional independence in newly diagnosed patients with temporal lobe glioma. Neurooncol. Pract. 2018, 5, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-H.; Byun, Y. Trajectories of Symptom Clusters, Performance Status, and Quality of Life During Concurrent Chemoradiotherapy in Patients with High-Grade Brain Cancers. Cancer Nurs. 2018, 41, E38–E47. [Google Scholar] [CrossRef] [PubMed]
- Addeo, R.; Caraglia, M.; Faiola, V.; Capasso, E.; Vincenzi, B.; Montella, L.; Guarrasi, R.; Caserta, L.; Del Prete, S. Concomitant treatment of brain metastasis with whole brain radiotherapy WBRT and temozolomide TMZ is active and improves quality of life. BMC Cancer 2007, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Thavarajah, N.; Bedard, G.; Zhang, L.; Cella, D.; Beaumont, J.L.; Tsao, M.; Barnes, E.; Danjoux, C.; Sahgal, A.; Soliman, H.; et al. Psychometric validation of the functional assessment of cancer therapy—Brain (FACT-Br) for assessing quality of life in patients with brain metastases. Support. Care Cancer 2014, 22, 1017–1028. [Google Scholar] [CrossRef] [PubMed]
- Weitzner, M.A.; Meyers, C.A.; Gelke, C.K.; Byrne, K.S.; Levin, V.A.; Cella, D.F. The functional assessment of cancer therapy (FACT) scale. Development of a brain subscale and revalidation of the general version (FACT-G) in patients with primary brain tumors. Cancer 1995, 75, 1151–1161. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Garg, R.; Minhas, V.; Bhatnagar, S.; Mishra, S.; Kumar, V.; Bharati, S.J.; Gupta, N.; Khan, M.A. To assess the Prevalence and Predictors of Cancer-related Fatigue and its Impact on Quality of Life in Advanced Cancer Patients Receiving Palliative Care in a Tertiary Care Hospital: A Cross-sectional Descriptive Study. Indian J. Palliat. Care 2020, 26, 523–527. [Google Scholar] [CrossRef]
- Annunziata, M.A.; Muzzatti, B.; Bidoli, E.; Flaiban, C.; Bomben, F.; Piccinin, M.; Gipponi, K.M.; Mariutti, G.; Busato, S.; Mella, S. Hospital Anxiety and Depression Scale (HADS) accuracy in cancer patients. Support. Care Cancer 2020, 28, 3921–3926. [Google Scholar] [CrossRef]
- Matías-Guiu, J.A.; Fernández-Bobadilla, R.; Cortés-Martínez, A. Addenbrooke’s Cognitive Examination III: Un test neuropsicológico útil para el cribado y la obtención de perfiles cognitivos. Neurologia (Engl. Ed.) 2018, 33, 140. [Google Scholar] [CrossRef]
- Valiyaveettil, D.G.A.; Malik, M.; Eaga, P.; Ahmed, S.F.; Joseph, D. “A prospective study of assessment of neurocognitive function in illiterate patients with gliomas treated with chemoradiation”: Assessment of neurocognitive function in gliomas. Cancer Treat. Res. Commun. 2021, 26, 100288. [Google Scholar] [CrossRef]
- Christensen, J.F.; Simonsen, C.; Hojman, P. Exercise Training in Cancer Control and Treatment. Compr. Physiol. 2018, 9, 165–205. [Google Scholar] [CrossRef]
- Cormie, P.; Nowak, A.K.; Chambers, S.K.; Galvão, D.A.; Newton, R.U. The potential role of exercise in neuro-oncology. Front. Oncol. 2015, 5, 85. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.W.; Guill, B.; Keir, S.T.; Carter, K.; Friedman, H.S.; Bigner, D.D.; Reardon, D.A. Exercise interest and preferences among patients diagnosed with primary brain cancer. Support. Care Cancer 2007, 15, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.D.; Rizzo, A.; Loetscher, T. Factors Associated with Virtual Reality Sickness in Head-Mounted Displays: A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef] [PubMed]
- van Coevorden-van Loon, E.M.P.; Horemans, H.H.L.D.; Heijenbrok-Kal, M.H.; van den Berg-Emons, R.J.G.; Rozenberg, R.; Vincent, A.J.P.E.; Ribbers, G.M.; van den Bent, M.J. Physical fitness and its association with fatigue in patients with low-grade glioma. Disabil. Rehabil. 2022, 45, 3323–3329. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.K.; Newton, R.U.; Cruickshank, T.; Cormie, P.; Halkett, G.K.B.; Tsoi, D.; Galvão, D.A. A feasibility, safety, and efficacy evaluation of supervised aerobic and resistance exercise for patients with glioblastoma undertaking adjuvant chemoradiotherapy. Neurooncol. Pract. 2023, 10, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Eisenhut, L.; Sadeghi-Bahmani, D.; Gerber, M.; Saemann, A.; Staub, L.; Brand, S.; Cordier, D. Effects of two types of exercise training on psychological well-being, sleep and physical fitness in patients with high-grade glioma (WHO III and IV). J. Psychiatr. Res. 2022, 151, 354–364. [Google Scholar] [CrossRef]
- Habets, E.J.J.; Hendriks, E.J.; Taphoorn, M.J.B.; Douw, L.; Zwinderman, A.H.; Vandertop, W.P.; Barkhof, F.; de Witt Hamer, P.C.; Klein, M. Association between tumor location and neurocognitive functioning using tumor localization maps. J. Neurooncol. 2019, 144, 573–582. [Google Scholar] [CrossRef]
- Gehring, K.; Stuiver, M.M.; Visser, E.; Kloek, C.; van den Bent, M.; Hanse, M.; Tijssen, C.; Rutten, G.-J.; Taphoorn, M.J.B.; Aaronson, N.K.; et al. A pilot randomized controlled trial of exercise to improve cognitive performance in patients with stable glioma: A proof of concept. Neuro Oncol. 2020, 22, 103–115. [Google Scholar] [CrossRef]
- Salerno, E.A.; Culakova, E.; Kleckner, A.S.; Heckler, C.E.; Lin, P.-J.; Matthews, C.E.; Conlin, A.; Weiselberg, L.; Mitchell, J.; Mustian, K.M.; et al. Physical Activity Patterns and Relationships With Cognitive Function in Patients With Breast Cancer Before, During, and After Chemotherapy in a Prospective, Nationwide Study. J. Clin. Oncol. 2021, 39, 3283–3292. [Google Scholar] [CrossRef]
- Wilson, R.; Kang, D.-W.; Tahbaz, M.; Norris, M.; Uno, H.; Ligibel, J.; Guenette, J.; Christopher, C.; Dieli-Conwright, C. Improving Cognitive Function Through High-Intensity Interval Training in Breast Cancer Patients Undergoing Chemotherapy: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2023, 12, e39740. [Google Scholar] [CrossRef] [PubMed]
- Szuhany, K.L.; Bugatti, M.; Otto, M.W. A meta-analytic review of the effects of exercise on brain-derived neurotrophic factor. J. Psychiatr. Res. 2015, 60, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Nolen, S.C.; Lee, B.; Shantharam, S.; Yu, H.J.; Su, L.; Billimek, J.; Bota, D.A. The effects of sequential treatments on hippocampal volumes in malignant glioma patients. J. Neurooncol. 2016, 129, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Schuermann, M.; Dzierma, Y.; Nuesken, F.; Oertel, J.; Rübe, C.; Melchior, P. Automatic Radiotherapy Planning for Glioblastoma Radiotherapy With Sparing of the Hippocampus and nTMS-Defined Motor Cortex. Front. Neurol. 2021, 12, 787140. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Stubbs, B.; Vancampfort, D.; Schuch, F.; Lagopoulos, J.; Rosenbaum, S.; Ward, P.B. Effect of aerobic exercise on hippocampal volume in humans: A systematic review and meta-analysis. Neuroimage 2018, 166, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Niemann, C.; Godde, B.; Voelcker-Rehage, C. Not only cardiovascular, but also coordinative exercise increases hippocampal volume in older adults. Front. Aging Neurosci. 2014, 6, 170. [Google Scholar] [CrossRef] [PubMed]
- Nauer, R.K.; Dunne, M.F.; Stern, C.E.; Storer, T.W.; Schon, K. Improving fitness increases dentate gyrus/CA3 volume in the hippocampal head and enhances memory in young adults. Hippocampus 2020, 30, 488–504. [Google Scholar] [CrossRef]
- Clifford, B.K.; Kaakoush, N.O.; Tedla, N.; Goldstein, D.; Simar, D. The effect of exercise intensity on the inflammatory profile of cancer survivors: A randomised crossover study. Eur. J. Clin. Investig. 2023, 53, e13984. [Google Scholar] [CrossRef]
- Cartmel, B.; Hughes, M.; Ercolano, E.A.; Gottlieb, L.; Li, F.; Zhou, Y.; Harrigan, M.; Ligibel, J.A.; Von Gruenigen, V.E.; Gogoi, R.; et al. Randomized trial of exercise on depressive symptomatology and brain derived neurotrophic factor (BDNF) in ovarian cancer survivors: The Women’s Activity and Lifestyle Study in Connecticut (WALC). Gynecol. Oncol. 2021, 161, 587–594. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Zhou, H.-H.; Luo, Q.; Cui, S. The effect of physical exercise on circulating brain-derived neurotrophic factor in healthy subjects: A meta-analysis of randomized controlled trials. Brain Behav. 2022, 12, e2544. [Google Scholar] [CrossRef]
- Ruiz-González, D.; Hernández-Martínez, A.; Valenzuela, P.L.; Morales, J.S.; Soriano-Maldonado, A. Effects of physical exercise on plasma brain-derived neurotrophic factor in neurodegenerative disorders: A systematic review and meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 2021, 128, 394–405. [Google Scholar] [CrossRef]
- Spencer, J.; Staffileno, B.A. Exercise Intervention: A Pilot Study to Assess the Feasibility and Impact on Cancer-Related Fatigue and Quality of Life Among Patients with High-Grade Glioma. Clin. J. Oncol. Nurs. 2021, 25, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E. Cancer-related fatigue—Mechanisms, risk factors, and treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Peng, P.; Xu, Z.; Ding, X. The effects of exercise on the quality of life of patients with breast cancer: A systematic review and meta-analysis based on the QLQ-C30 quality of life scale. Gland Surg. 2023, 12, 633–650. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.-Y.; Roh, H.-T. Effects of Exercise Training on Neurotrophic Factors and Blood-Brain Barrier Permeability in Young-Old and Old-Old Women. Int. J. Environ. Res. Public Health 2022, 19, 16896. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.T.; DelCimmuto, N.R.; Flack, K.D.; Stec, D.E.; Hinds, T.D. Reactive Oxygen Species (ROS) and Antioxidants as Immunomodulators in Exercise: Implications for Heme Oxygenase and Bilirubin. Antioxidants 2022, 11, 179. [Google Scholar] [CrossRef] [PubMed]
- Hinds, T.D.; Creeden, J.F.; Gordon, D.M.; Stec, D.F.; Donald, M.C.; Stec, D.E. Bilirubin Nanoparticles Reduce Diet-Induced Hepatic Steatosis, Improve Fat Utilization, and Increase Plasma β-Hydroxybutyrate. Front. Pharmacol. 2020, 11, 594574. [Google Scholar] [CrossRef]



| Variable (Mean ± SD or Median (Range) or n (%)) | Exercise Group, n = 25 | Control Group, n = 22 | p-Value |
|---|---|---|---|
| Age, years | 45.59 ± 11.15 | 60 ± 13.55 | 0.002 |
| Sex | 0.1 | ||
| Female | 3 (17.65) | 7 (43.75) | |
| Male | 14 (82.35) | 9 (56.25) | |
| Time from tumor resection, weeks | 4.38 | 4.29 | 0.7 |
| Education | 0.03 | ||
| Primary | 0 | 0 | |
| Vocational | 2 (11.76) | 5 (31.25) | |
| Secondary | 7 (41.18) | 10 (62.50) | |
| High | 8 (47.06) | 1 (6.25) | |
| FIM | 124.5 (121–126) | 122 (86–126) | 0.083 |
| ACE III | 91 (72–100) | 88 (60–94) | 0.052 |
| Parameters (Mean ± SD or Median [Range]) | Baseline | After RT | After 3 Months | p-Value |
|---|---|---|---|---|
| HGS, kg | 32.76 ± 8.24 | 35.35 ± 9.59 | 35.73 ± 9.21 | 0.092 |
| TUG, s | 7.25 ± 2.03 | 7.22 ± 1.90 | 7.55 ± 2.48 | 0.695 |
| 6MWT, m | 483.59 ± 116.48 | 500.74 ± 114.90 | 473.45 ± 85.20 | 0.385 |
| FIM self-care | 42 (42–42) | 42 (42–42) | 42 (12–42) | 0.135 |
| FIM sphincter control | 14 (14–14) | 14 (14–14) | 14 (10–14) | 0.368 |
| FIM transverse | 21 (21–21) | 21 (21–21) | 21 (9–21) | 0.135 |
| FIM locomotion | 14 (13–14) | 14 (12–14) | 14 (6–14) | 0.038 |
| FIM communication | 14 (12–14) | 14 (12–14) | 14 (13–14) | 0.607 |
| FIM social cognition | 20 (16–21) | 20 (15–21) | 20 (16–21) | 0.482 |
| FIM total score | 124.5 (121–126) | 125 (119–126) | 124 (69–126) | 0.575 |
| FACT-G PWB | 22 (18–28) | 23 (19–28) | 21.5 (5–25) | 0.509 |
| FACT-G SWB | 23 (13–27) | 23 (16–28) | 21 (13–28) | 0.273 |
| FACT-G EWB | 18 (7–24) | 18.5 (7–24) | 16 (6–20) | 0.84 |
| FACT-G FWB | 21 (10–28) | 20.5 (10–28) | 16 (0–24) | 0.067 |
| FACT-G total | 80 (66–107) | 82.5 (57–108) | 76.0 (47–95) | 0.093 |
| FACT-BR | 73 (54–91) | 70 (52–92) | 67 (52–82) | 0.074 |
| FACIT-F | 42 (28–52) | 40 (28–52) | 33 (22–49) | 0.068 |
| ACE III attention | 18 (8–18) | 18 (15–18) | 18 (13–18) | 0.951 |
| ACE III memory | 23 (12–26) | 24 (10–26) | 23.5 (11–25) | 0.421 |
| ACE III fluency | 11 (1–14) | 10.5 (6–14) | 11.5 (2–20) | 0.664 |
| ACE III language | 26 (18–26) | 26 (22–26) | 26 (21–26) | 0.074 |
| ACE III VS | 16 (15–16) | 16 (13–16) | 15.5 (8–15) | 0.485 |
| ACE III total | 91 (72–100) | 91 (78–100) | 93.5 (59–100) | 0.749 |
| HADS anxiety | 3 (0–14) | 0 (0–18) | 0 (0–5) | 0.125 |
| HADS depression | 2 (0–9) | 0 (0–7) | 0 (0–6) | 0.146 |
| Parameters (Mean ± SD or Median (Range) | Baseline | After RT | After 3 Months | p-Value |
|---|---|---|---|---|
| HGS, kg | 26.63 ± 12.08 | 26.55 ± 10.65 | 17.89 ± 4.23 | 0.017 b |
| TUG, s | 10.03 ± 3.03 | 9.63 ± 2.36 | 10.75 ± 1.33 | 0.197 |
| 6MWT, m | 382.21 ± 68.52 | 379.91 ± 85.65 | 361 ± 72.07 | 0.375 |
| FIM self-care | 42 (30–42) | 42 (42–42) | 42 (18–42) | 0.156 |
| FIM sphincter control | 14 (8–14) | 14 (14–14) | 14 (12–14) | 0.368 |
| FIM transverse | 21 (20–21) | 21 (21–21) | 21 (9–21) | 0.368 |
| FIM locomotion | 14 (10–14) | 14 (14–14) | 14 (6–14) | 0.368 |
| FIM communication | 14 (7–14) | 14 (12–14) | 14 (11–14) | 0.368 |
| FIM social cognition | 18.5(11–21) | 21 (16–21) | 18.5 (10–21) | 0.670 |
| FIM total score | 12 (86–126) | 126 (121–126) | 121.5 (68–126) | 0.368 |
| FACT-G PWB | 22 (10–28) | 22 (10–28) | 15 (4–22) | 0.089 |
| FACT-G SWB | 24.5 (20–28) | 23 (4–28) | 20.5 (2–28) | 0.326 |
| FACT-G EWB | 16 (0–24) | 15 (11–24) | 13.5 (3–18) | 0.698 |
| FACT-G FWB | 16.5(2–28) | 17 (6–27) | 18 (7–22) | 0.738 |
| FACT-G total | 79.5 (41–100) | 88 (43–101) | 71 (18–83) | 0.648 |
| FACT-BR | 64 (32–87) | 58.5 (43–84) | 52 (33–80) | 0.085 |
| FACIT-F | 36.5 (11–52) | 40 (20–50) | 36.5 (3–49) | 0.379 |
| ACE III attention | 18 (12–18) | 18 (13–18) | 17.5 (11–18) | 0.047 |
| ACE III memory | 20 (12–26) | 21 (9–26) | 19.5 (10–26) | 0.972 |
| ACE III fluency | 9.5 (1–13) | 9.5 (1–14) | 8.5 (1–12) | 0.167 |
| ACE III language | 25 (17–26) | 25.5 (17–26) | 25 (20–26) | 0.834 |
| ACE III VS | 15 (8–17) | 15.5 (6–17) | 15.5 (8–16) | 0.350 |
| ACE III total | 88 (60–94) | 89 (55–96) | 80.5 (55–94) | 0.558 |
| HADS anxiety | 4 (0–12) | 4 (0–7) | 7 (0–11) | 0.639 |
| HADS depression | 3 (0–20) | 4 (0–15) | 3(0–9) | 0.507 |
| Parameters | Difference between T0 and T1 | Difference between T1 and T2 | Difference between T0 and T2 | |||
|---|---|---|---|---|---|---|
| EG | CG | EG | CG | EG | CG | |
| HGS, kg | 2.59 ± 5.14 * | −1.82 ± 2.75 * | −0.45 ± 6.46 | −6.33 ± 7.33 | 2.91 ± 4.87 * | −8.00 ± 9.54 * |
| TUG, s | −0.03 ± 073 | 0.29 ± 1.61 | −0.02 ± 0.95 | 1.68 ± 1.6 | −0.02 ± 1.08 * | 1.75 ± 2.31 * |
| 6MWT, m | 16.88 ± 33.16 | −8.73 ± 54.17 | −3.55 ± 54.69 | −30.71 ± 41.89 | 16.45 ± 68.13 | −21.86 ± 65.88 |
| FIM total score | −1.44 ± 2.06 | 0.36 ± 2.3 | −6.77 ± 16.16 | −7.50 ± 20.42 | −8.23 ± 16.31 | −7.44 ± 19.22 |
| FACT-G PWB | 0.44 ± 1.67 | −0.73 ± 3.26 | −3.09 ± 5.2 | −4.43 ± 5.44 | −2.83 ± 5.1 | −2.5 ± 5.11 |
| FACT-G SWB | −1.21 ± 3.28 | −2.73 ± 7.09 | −0.82 ± 2.93 | −0.14 ± 2.34 | −1.25 ± 3.89 | −3.75 ± 7.11 |
| FACT-G EWB | −0.19 ± 2.9 | 0.18 ± 3.74 | −1.36 ± 5.03 | −1.00 ± 3.11 | −1.50 ± 4.32 | −2.00 ± 4.96 |
| FACT-G FWB | 0.56 ± 5.4 | 0.00 ± 6.07 | −3.55 ± 5.91 | −0.57 ± 7.04 | −3.75 ± 6.17 | −1.25 ± 6.73 |
| FACT-G total | −0.50 ± 8.47 | −3.27 ± 9.25 | −5.18± 14.65 | −6.14 ± 9.15 | −7.27 ± 8.34 | −14.38 ± 22.18 |
| FACT-BR | −2.29 ± 5.57 | −2.25 ± 10.45 | −4.0 ± 11.1 | −6.00 ± 7.00 | −7.00 ± 11.23 | −7.00± 9.93 |
| FACIT-F | −2.53 ± 10.9 | 1.09 ± 6.19 | −2.58 ± 9.77 | −4.00 ± 15.81 | −6.66 ± 8.18 | −2.30 ± 13.02 |
| ACE III attention | 0.31 ± 2.52 | −0.29 ± 0.73 | −0.15 ± 069 | −0.90 ± 1.85 | −0.43 ± 1.65 | −1.00 ± 2.16 |
| ACE III memory | 0.81 ± 3.29 | 0.14 ± 3.16 | −2.23 ± 4.3 | −0.10 ± 2.08 | −1.00 ± 5.45 | 0.20 ± 3.74 |
| ACE III fluency | 0.19 ± 2.59 | −0.07 ± 1.64 | 0.69 ± 4.94 | −1.40 ± 2.22 | 0.71 ± 5.62 | −1.00 ± 1.7 |
| ACE III language | 0.06 ± 1.18 | −0.86 ± 2.03 | −0.54 ± 1.45 | 0.10 ± 3.14 | −0.57 ± 1.34 | −0.10 ± 3.31 |
| ACE III VS | −0.31 ± 1.01 | −0.21 ± 1.31 | −0.46 ± 1.76 | −0.80 ± 1.93 | −1.00 ± 0.29 | −0.70 ± 2.0 |
| ACE III total | 1.19 ± 5.21 | −1.50 ± 7.53 | −2.85 ± 9.58 | −3.20 ± 6.55 | −2.29 ± 12.03 | −2.50 ± 7.49 |
| HADS anxiety | −2.13 ± 4.49 | −0.27 ± 3.35 | −1.38 ± 5.35 | 2.13 ± 3.64 | −2.62 ± 4.41 | 0.22 ± 6.1 |
| HADS depression | −1.69 ± 3.42 * | 2.09 ± 5.86 * | −0.46 ± 1.9 | −2.13 ± 4.52 | −1.69 ± 3.25 | −2.22 ± 7.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pieczyńska, A.; Zasadzka, E.; Pilarska, A.; Procyk, D.; Adamska, K.; Hojan, K. Rehabilitation Exercises Supported by Monitor-Augmented Reality for Patients with High-Grade Glioma Undergoing Radiotherapy: Results of a Randomized Clinical Trial. J. Clin. Med. 2023, 12, 6838. https://doi.org/10.3390/jcm12216838
Pieczyńska A, Zasadzka E, Pilarska A, Procyk D, Adamska K, Hojan K. Rehabilitation Exercises Supported by Monitor-Augmented Reality for Patients with High-Grade Glioma Undergoing Radiotherapy: Results of a Randomized Clinical Trial. Journal of Clinical Medicine. 2023; 12(21):6838. https://doi.org/10.3390/jcm12216838
Chicago/Turabian StylePieczyńska, Anna, Ewa Zasadzka, Agnieszka Pilarska, Danuta Procyk, Krystyna Adamska, and Katarzyna Hojan. 2023. "Rehabilitation Exercises Supported by Monitor-Augmented Reality for Patients with High-Grade Glioma Undergoing Radiotherapy: Results of a Randomized Clinical Trial" Journal of Clinical Medicine 12, no. 21: 6838. https://doi.org/10.3390/jcm12216838
APA StylePieczyńska, A., Zasadzka, E., Pilarska, A., Procyk, D., Adamska, K., & Hojan, K. (2023). Rehabilitation Exercises Supported by Monitor-Augmented Reality for Patients with High-Grade Glioma Undergoing Radiotherapy: Results of a Randomized Clinical Trial. Journal of Clinical Medicine, 12(21), 6838. https://doi.org/10.3390/jcm12216838