

Different Prognostic Role of Soluble PD-L1 in the Course of Severe and Non-Severe COVID-19

 , , , , ,
, , , , ,  ,
,  ,
,  ,
,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
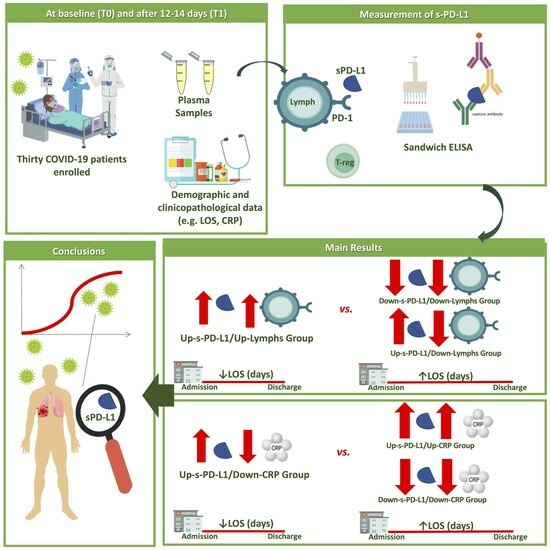
2.1. Study Population
2.2. Collection of Blood Samples and Determination of the Amount of Soluble PD-L1
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
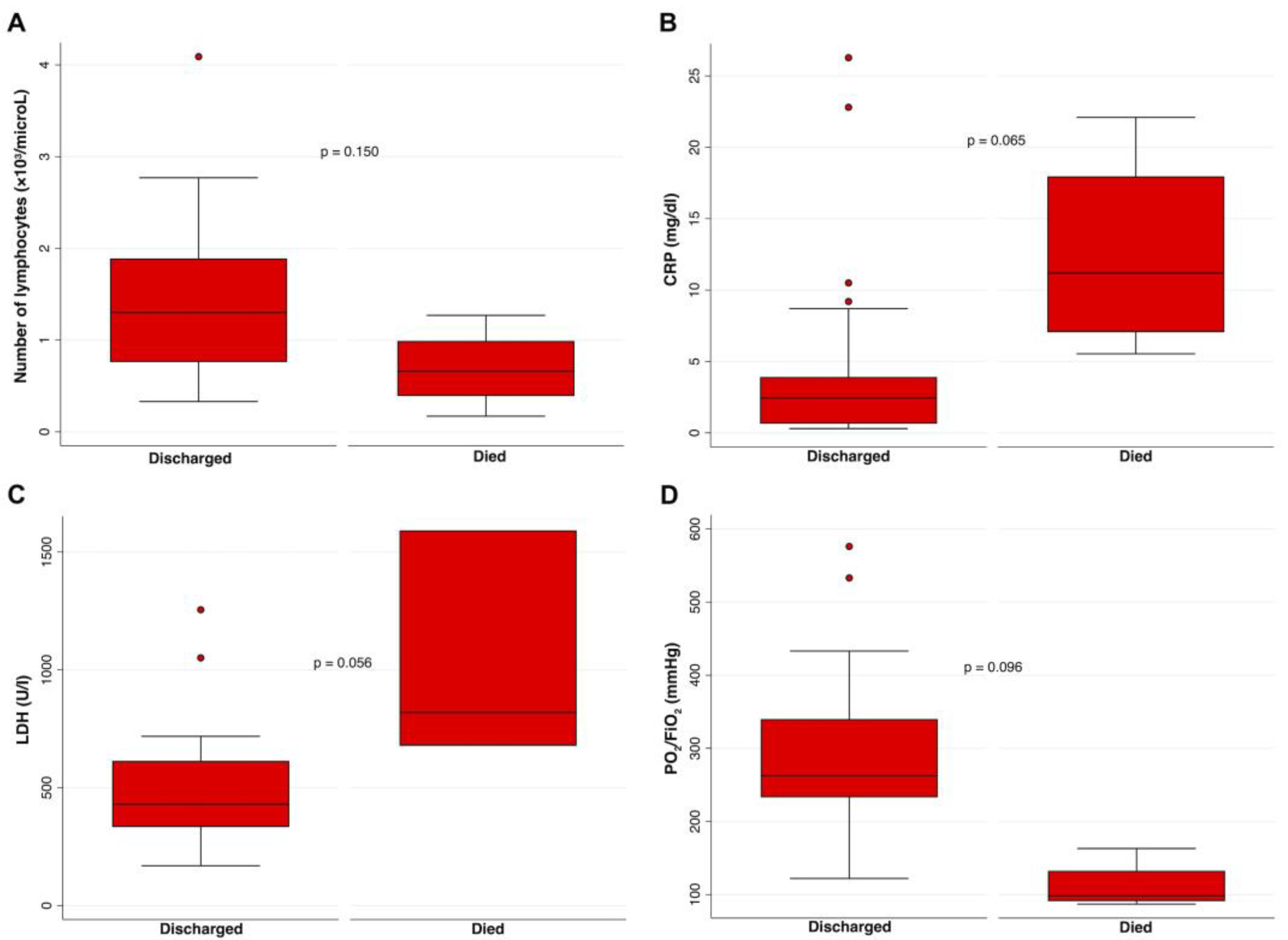
3.2. Correlation between Baseline Biohumoral Characteristics of COVID-19 Patients with Their Clinical Outcomes
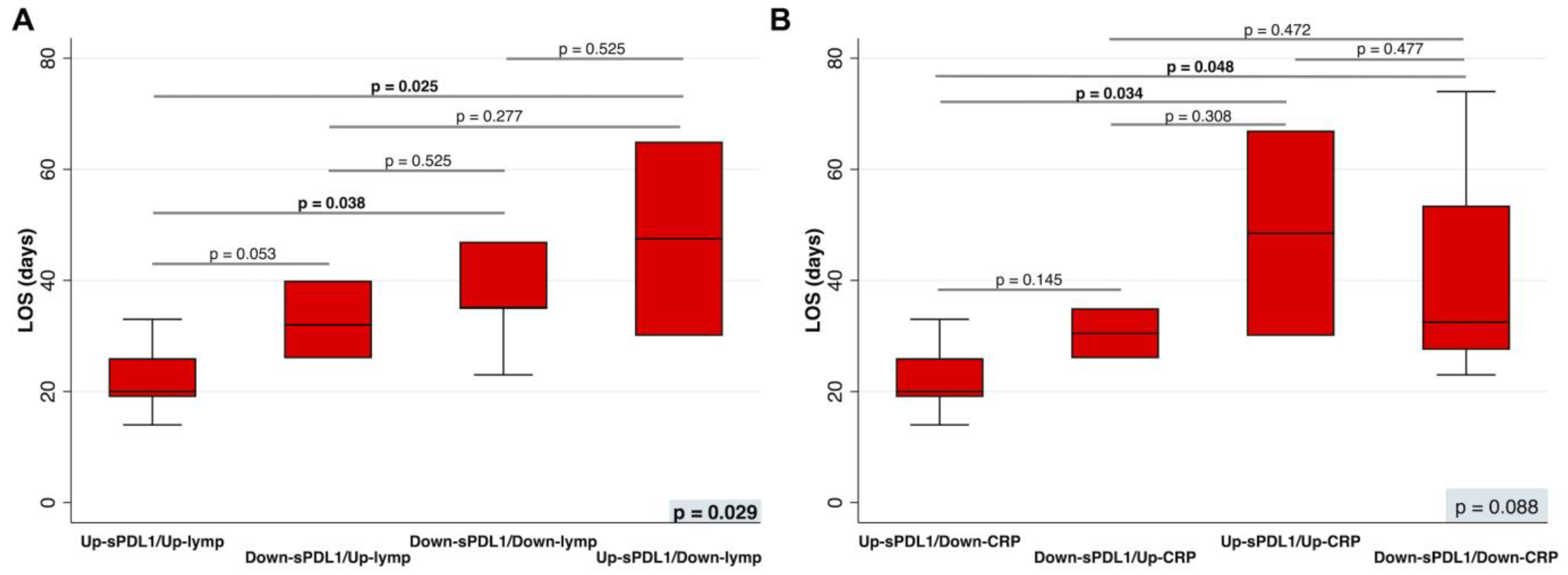
3.3. Correlation between Differences in Biohumoral Characteristics during Hospitalization of COVID-19 Patients with Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abbasi, J. What to Know About EG.5, the Latest SARS-CoV-2 “Variant of Interest”. JAMA 2023, 330, 900–901. [Google Scholar] [CrossRef]
- Pagliano, P.; Scarpati, G.; Sellitto, C.; Conti, V.; Spera, A.M.; Ascione, T.; Piazza, O.; Filippelli, A. Experimental Pharmacotherapy for COVID-19: The Latest Advances. J. Exp. Pharmacol. 2021, 13, 1–13. [Google Scholar] [CrossRef]
- Conti, V.; Sellitto, C.; Torsiello, M.; Manzo, V.; De Bellis, E.; Stefanelli, B.; Bertini, N.; Costantino, M.; Maci, C.; Raschi, E.; et al. Identification of Drug Interaction Adverse Events in Patients With COVID-19: A Systematic Review. JAMA Netw. Open 2022, 5, e227970. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Lei, R.; Mohan, C. Immunological Biomarkers of COVID-19. Crit. Rev. Immunol. 2020, 40, 497–512. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, W.; Liu, J.; Chen, Z.; Lv, Q.; Zhang, Z. Immunotherapy Summary for Cytokine Storm in COVID-19. Front. Pharmacol. 2021, 12, 731847. [Google Scholar] [CrossRef]
- Xu, R.; Liu, C.; Xu, X.; Hu, Y.; Zhu, B.; Yang, C. Role of cytokine storm in coronavirus infections: Culprit or accomplice? Front. Biosci. 2022, 27, 102. [Google Scholar] [CrossRef]
- Franceschi, C.; Bonafè, M.; Valensin, S. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann. N. Y. Acad. Sci. 2000, 908, 244–254. [Google Scholar] [CrossRef]
- Hakim, A.; Hasan, M.M.; Hasan, M.; Lokman, S.M.; Azim, K.F.; Raihan, T.; Chowdhury, P.A.; Azad, A.K. Major Insights in Dynamics of Host Response to SARS-CoV-2: Impacts and Challenges. Front. Microbiol. 2021, 12, 637554. [Google Scholar] [CrossRef]
- Villa, F.; Malovini, A.; Carrizzo, A. Serum BPIFB4 levels classify health status in long-living individuals. Immun. Ageing 2015, 12, 27. [Google Scholar] [CrossRef]
- Ciaglia, E.; Lopardo, V.; Montella, F.; Sellitto, C.; Manzo, V.; De Bellis, E.; Iannaccone, T.; Franci, G.; Zannella, C.; Pagliano, P.; et al. BPIFB4 Circulating Levels and Its Prognostic Relevance in COVID-19. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 1775–1783. [Google Scholar] [CrossRef]
- Chowdhury, M.A.; Hossain, N.; Kashem, M.A.; Shahid, M.A.; Alam, A. Immune Response in COVID-19: A Review. J. Infect. Public Health 2020, 13, 1619–1629. [Google Scholar] [CrossRef]
- Tan, J.; Li, Y. Immune Checkpoint Alterations and Their Blockade in COVID-19 Patients. Blood Sci. 2022, 4, 192–198. [Google Scholar] [CrossRef]
- De Biasi, S.; Meschiari, M.; Gibellini, L.; Bellinazzi, C.; Borella, R.; Fidanza, L.; Gozzi, L.; Iannone, A.; Lo Tartaro, D.; Mattioli, M.; et al. Marked T Cell Activation, Senescence, Exhaustion and Skewing towards TH17 in Patients with COVID-19 Pneumonia. Nat. Commun. 2020, 11, 3434. [Google Scholar] [CrossRef]
- Abbott, M.; Ustoyev, Y. Cancer and the Immune System: The History and Background of Immunotherapy. Semin. Oncol. Nurs. 2019, 35, 150923. [Google Scholar] [CrossRef]
- Bailly, C.; Thuru, X.; Quesnel, B. Soluble Programmed Death Ligand-1 (SPD-L1): A Pool of Circulating Proteins Implicated in Health and Diseases. Cancers 2021, 13, 3034. [Google Scholar] [CrossRef]
- Tang, Y.; Liu, J.; Zhang, D.; Xu, Z.; Ji, J.; Wen, C. Cytokine Storm in COVID-19: The Current Evidence and Treatment Strategies. Front. Immunol. 2020, 11, 1708. [Google Scholar] [CrossRef]
- Abu Hejleh, T.; Furqan, M.; Ballas, Z.; Clamon, G. The Clinical Significance of Soluble PD-1 and PD-L1 in Lung Cancer. Crit. Rev. Oncol. Hematol. 2019, 143, 148–152. [Google Scholar] [CrossRef]
- Oh, S.Y.; Kim, S.; Keam, B.; Kim, T.M.; Kim, D.-W.; Heo, D.S. Soluble PD-L1 Is a Predictive and Prognostic Biomarker in Advanced Cancer Patients Who Receive Immune Checkpoint Blockade Treatment. Sci. Rep. 2021, 11, 19712. [Google Scholar] [CrossRef]
- Sabbatino, F.; Conti, V.; Franci, G.; Sellitto, C.; Manzo, V.; Pagliano, P.; De Bellis, E.; Masullo, A.; Salzano, F.A.; Caputo, A.; et al. PD-L1 Dysregulation in COVID-19 Patients. Front. Immunol. 2021, 12, 695242. [Google Scholar] [CrossRef]
- Chavez-Galan, L.; Ruiz, A.; Martinez-Espinosa, K.; Aguilar-Duran, H.; Torres, M.; Falfan-Valencia, R.; Pérez-Rubio, G.; Selman, M.; Buendia-Roldan, I. Circulating Levels of PD-L1, TIM-3 and MMP-7 Are Promising Biomarkers to Differentiate COVID-19 Patients That Require Invasive Mechanical Ventilation. Biomolecules 2022, 12, 445. [Google Scholar] [CrossRef]
- Pagliano, P.; Sellitto, C.; Conti, V.; Ascione, T.; Esposito, S. Characteristics of viral pneumonia in the COVID-19 era: An update. Infection 2021, 49, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Schönrich, G.; Raftery, M.J. The PD-1/PD-L1 Axis and Virus Infections: A Delicate Balance. Front. Cell. Infect. Microbiol. 2019, 9, 207. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Gu, Y.-K.; Li, S.-L.; Chen, H.; Chen, M.-S.; Cai, Q.-Q.; Deng, H.-X.; Zuo, M.-X.; Huang, J.-H. Pre-Treatment Serum Levels of Soluble Programmed Cell Death-Ligand 1 Predict Prognosis in Patients with Hepatitis B-Related Hepatocellular Carcinoma. J. Cancer Res. Clin. Oncol. 2019, 145, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Avendaño-Ortiz, J.; Rubio-Garrido, M.; Lozano-Rodríguez, R.; Del Romero, J.; Rodríguez, C.; Moreno, S.; Aguirre, L.A.; Holguín, Á.; López-Collazo, E. Soluble PD-L1: A Potential Immune Marker for HIV-1 Infection and Virological Failure. Medicine 2020, 99, e20065. [Google Scholar] [CrossRef] [PubMed]
- Yamagiwa, S.; Ishikawa, T.; Waguri, N.; Sugitani, S.; Kamimura, K.; Tsuchiya, A.; Takamura, M.; Kawai, H.; Terai, S. Increase of Soluble Programmed Cell Death Ligand 1 in Patients with Chronic Hepatitis C. Int. J. Med. Sci. 2017, 14, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Gay, C.L.; Bosch, R.J.; Ritz, J.; Hataye, J.M.; Aga, E.; Tressler, R.L.; Mason, S.W.; Hwang, C.K.; Grasela, D.M.; Ray, N.; et al. Clinical Trial of the Anti-PD-L1 Antibody BMS-936559 in HIV-1 Infected Participants on Suppressive Antiretroviral Therapy. J. Infect. Dis. 2017, 215, 1725–1733. [Google Scholar] [CrossRef] [PubMed]
- Gane, E.; Verdon, D.J.; Brooks, A.E.; Gaggar, A.; Nguyen, A.H.; Subramanian, G.M.; Schwabe, C.; Dunbar, P.R. Anti-PD-1 Blockade with Nivolumab with and without Therapeutic Vaccination for Virally Suppressed Chronic Hepatitis B: A Pilot Study. J. Hepatol. 2019, 71, 900–907. [Google Scholar] [CrossRef]
- Conti, V.; Corbi, G.; Sabbatino, F.; De Pascale, D.; Sellitto, C.; Stefanelli, B.; Bertini, N.; De Simone, M.; Liguori, L.; Di Paola, I.; et al. Long COVID: Clinical Framing, Biomarkers, and Therapeutic Approaches. J. Pers. Med. 2023, 13, 334. [Google Scholar] [CrossRef]
- Moritz, R.K.C.; Gutzmer, R.; Zimmer, L.; Meier, F.; Ahmed, M.S.; Sell, S.; Schlaak, M.; Kapp, F.; Sachse, M.M.; Haferkamp, S.; et al. SARS-CoV-2 Infections in Melanoma Patients Treated with PD-1 Inhibitors: A Survey of the German ADOREG Melanoma Registry. Eur. J. Cancer 2021, 144, 382–385. [Google Scholar] [CrossRef]
- Loretelli, C.; Abdelsalam, A.; D’Addio, F.; Ben Nasr, M.; Assi, E.; Usuelli, V.; Maestroni, A.; Seelam, A.J.; Ippolito, E.; Di Maggio, S.; et al. PD-1 Blockade Counteracts Post-COVID-19 Immune Abnormalities and Stimulates the Anti-SARS-CoV-2 Immune Response. JCI Insight 2021, 6, e146701. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Rizvi, H.; Egger, J.V.; Preeshagul, I.R.; Wolchok, J.D.; Hellmann, M.D. Impact of PD-1 Blockade on Severity of COVID-19 in Patients with Lung Cancers. Cancer Discov. 2020, 10, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Lovly, C.M.; Boyd, K.L.; Gonzalez-Ericsson, P.I.; Lowe, C.L.; Brown, H.M.; Hoffman, R.D.; Sterling, B.C.; Kapp, M.E.; Johnson, D.B.; Kopparapu, P.R.; et al. Rapidly Fatal Pneumonitis from Immunotherapy and Concurrent SARS-CoV-2 Infection in a Patient with Newly Diagnosed Lung Cancer. medRxiv 2020. preprint. [Google Scholar] [CrossRef]
- Dipasquale, A.; Persico, P.; Lorenzi, E.; Rahal, D.; Santoro, A.; Simonelli, M. COVID-19 Lung Injury as a Primer for Immune Checkpoint Inhibitors (ICIs)-Related Pneumonia in a Patient Affected by Squamous Head and Neck Carcinoma Treated with PD-L1 Blockade: A Case Report. J. Immunother. Cancer 2021, 9, e001870. [Google Scholar] [CrossRef]
- Qian, W.; Ye, Y.; Zuo, L.; Song, T.; Xu, Q.; Wang, Y.; Qian, J.; Tian, Y. Immune Checkpoint Inhibitors Use and Effects on Prognosis of COVID-19 Infection: A Systematic Review and Meta-Analysis. Immunotherapy 2021, 13, 1271–1282. [Google Scholar] [CrossRef] [PubMed]
- Ansari, M.J.I.; Salama, A.D.; Chitnis, T.; Smith, R.N.; Yagita, H.; Akiba, H.; Yamazaki, T.; Azuma, M.; Iwai, H.; Khoury, S.J.; et al. The Programmed Death-1 (PD-1) Pathway Regulates Autoimmune Diabetes in Nonobese Diabetic (NOD) Mice. J. Exp. Med. 2003, 198, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yoshida, T.; Nakaki, F.; Hiai, H.; Okazaki, T.; Honjo, T. Establishment of NOD-Pdcd1-/- Mice as an Efficient Animal Model of Type I Diabetes. Proc. Natl. Acad. Sci. USA 2005, 102, 11823–11828. [Google Scholar] [CrossRef]
- Francisco, L.M.; Salinas, V.H.; Brown, K.E.; Vanguri, V.K.; Freeman, G.J.; Kuchroo, V.K.; Sharpe, A.H. PD-L1 Regulates the Development, Maintenance, and Function of Induced Regulatory T Cells. J. Exp. Med. 2009, 206, 3015–3029. [Google Scholar] [CrossRef]
- Park, H.J.; Park, J.S.; Jeong, Y.H.; Son, J.; Ban, Y.H.; Lee, B.-H.; Chen, L.; Chang, J.; Chung, D.H.; Choi, I.; et al. PD-1 Upregulated on Regulatory T Cells during Chronic Virus Infection Enhances the Suppression of CD8+ T Cell Immune Response via the Interaction with PD-L1 Expressed on CD8+ T Cells. J. Immunol. 2015, 194, 5801–5811. [Google Scholar] [CrossRef]
- Xu, J.; Wang, J.; Wang, X.; Tan, R.; Qi, X.; Liu, Z.; Qu, H.; Pan, T.; Zhan, Q.; Zuo, Y.; et al. Soluble PD-L1 Improved Direct ARDS by Reducing Monocyte-Derived Macrophages. Cell Death Dis. 2020, 11, 934. [Google Scholar] [CrossRef]
- Monaghan, S.F.; Chung, C.-S.; Chen, Y.; Lomas-Neira, J.; Fairbrother, W.G.; Heffernan, D.S.; Cioffi, W.G.; Ayala, A. Soluble Programmed Cell Death Receptor-1 (SPD-1): A Potential Biomarker with Anti-Inflammatory Properties in Human and Experimental Acute Respiratory Distress Syndrome (ARDS). J. Transl. Med. 2016, 14, 312. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of the Study Population | T0 | T1 |
|---|---|---|
| Age, years (range) | 66.3 (42–84) | |
| Sex, n (%): | ||
| Male | 20 (66.7) | |
| Female | 10 (33.3) | |
| Mean number of PBMCs: | ||
| White blood cells count, ×103/µL (range) | 7.9 (2.47–19.04) | 8.0 (2.77–15.42) |
| Lymphocytes, ×103/µL (range) | 1.3 (0.17–4.09) | 1.5 (0.4–2.72) |
| Platelets, ×103/mL (range) | 226.9 (74–568) | 235.3 (26–414) |
| LDH, U/I (range) | 557.9 (169–1592) | 604.3 (204–2957) |
| ESR, mm (range) | 35.7 (16–75) | 33.4 (2–50) |
| CRP, mg/dL (range) | 5.67 (0.3–26.27) | 2.5 (0.15–14.77) |
| Fibrinogen, mg% (range) | 535.7 (210–908) | 518.6 (296–1016) |
| PaO2/FiO2 ratio | 258.9 | 272.5 |
| Severe | 10 (33.0) | |
| Non-severe | 20 (67.0) | |
| Chronic diseases, n (%): | ||
| Hypertension | 14 (46.7) | |
| Cardiovascular diseases | 14 (45.0) | |
| Diabetes | 8 (26.7) | |
| Previous neoplasms | 5 (16.7) | |
| Obesity | 4 (13.3) | |
| Chronic kidney disease | 4 (13.0) | |
| Dyslipidemia | 3 (10.0) | |
| Neurologic diseases | 2 (6.7) | |
| Liver and biliary tract diseases | 2 (6.7) | |
| Chronic pulmonary disease | 1 (3.0) | |
| Medium LOS, days (range) | 34.6 (12–74) | |
| Mean time to SARS-CoV-2 negativization, days (range) | 34.8 (13–73) | |
| Therapy, n (%): | ||
| Low molecular weight heparin | 12 (40.0) | |
| Corticosteroids | 11 (36.6) | |
| Azithromycin | 4 (13.3) | |
| Tocilizumab | 2 (6.6) | |
| Casivirimab/Indevimab | 1 (3.3) | |
| Number of deaths (%) | 4 (13.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sabbatino, F.; Pagliano, P.; Sellitto, C.; Stefanelli, B.; Corbi, G.; Manzo, V.; De Bellis, E.; Liguori, L.; Salzano, F.A.; Pepe, S.; et al. Different Prognostic Role of Soluble PD-L1 in the Course of Severe and Non-Severe COVID-19. J. Clin. Med. 2023, 12, 6812. https://doi.org/10.3390/jcm12216812
Sabbatino F, Pagliano P, Sellitto C, Stefanelli B, Corbi G, Manzo V, De Bellis E, Liguori L, Salzano FA, Pepe S, et al. Different Prognostic Role of Soluble PD-L1 in the Course of Severe and Non-Severe COVID-19. Journal of Clinical Medicine. 2023; 12(21):6812. https://doi.org/10.3390/jcm12216812
Chicago/Turabian StyleSabbatino, Francesco, Pasquale Pagliano, Carmine Sellitto, Berenice Stefanelli, Graziamaria Corbi, Valentina Manzo, Emanuela De Bellis, Luigi Liguori, Francesco Antonio Salzano, Stefano Pepe, and et al. 2023. "Different Prognostic Role of Soluble PD-L1 in the Course of Severe and Non-Severe COVID-19" Journal of Clinical Medicine 12, no. 21: 6812. https://doi.org/10.3390/jcm12216812
APA StyleSabbatino, F., Pagliano, P., Sellitto, C., Stefanelli, B., Corbi, G., Manzo, V., De Bellis, E., Liguori, L., Salzano, F. A., Pepe, S., Filippelli, A., & Conti, V. (2023). Different Prognostic Role of Soluble PD-L1 in the Course of Severe and Non-Severe COVID-19. Journal of Clinical Medicine, 12(21), 6812. https://doi.org/10.3390/jcm12216812