
Pre- and Postoperative Evaluation of Immediate and Early Implant Placement in Esthetic Areas with Pre-Extraction Facial Dehiscence: A Retrospective Clinical Study


Abstract
:1. Introduction
- Immediate implant placement into extraction sockets is defined as “Type 1” implant placement;
- When the objective is the soft tissue coverage of the extraction socket, then a healing period of 4–8 weeks is observed before implant placement, which is defined as “Type 2” implant placement;
- When the socket is allowed to heal to have a partial bone fill of the socket, typically 12–16 weeks, this is defined as “Type 3” implant placement;
- When the extraction is fully healed after 16 weeks or more, the implant placement procedure is defined as “Type 4”.
2. Materials and Methods
2.1. Study Design and Population
- Implant placement must be performed on the day of extraction or between 4 and 16 weeks after extraction, at the same time as bone grafting;
- The presence of dehiscence in the facial alveolar bone before tooth extraction;
- An implant body with a tapered joint and platform shifting is inserted;
- A fixed superstructure is set.
- Patients were excluded from the study if they met the following criteria:
- Smoking [21];
- Patients treated for diabetes, including controlled patients [22];
- Patients with an acute infection at the planned extraction of the tooth and periodontal tissue.
2.2. Classification of Target Patients According to Different Surgical Techniques
- For the immediate implant placement group, primary surgery was performed on the same day as tooth extraction (Group I, mean age: 61.5 ± 14.0 years, 9 males, 11 females);
- Group IC patients underwent primary surgery on the same day as tooth extraction and connective tissue grafting was also performed (mean age: 58.4 ± 15.2 years, 6 males, 10 females);
- The early implant placement group (Group E, mean age: 61.8 ± 20.0 years, 6 males, 10 females) underwent primary surgery after waiting 4 to 16 weeks for healing after tooth extraction. In Group E, no connective tissue grafting was performed.
2.3. Implant Materials
2.4. Surgical Procedure
2.5. Bone Graft Materials
2.6. Prosthetic Procedure
2.7. CBCT Protocol
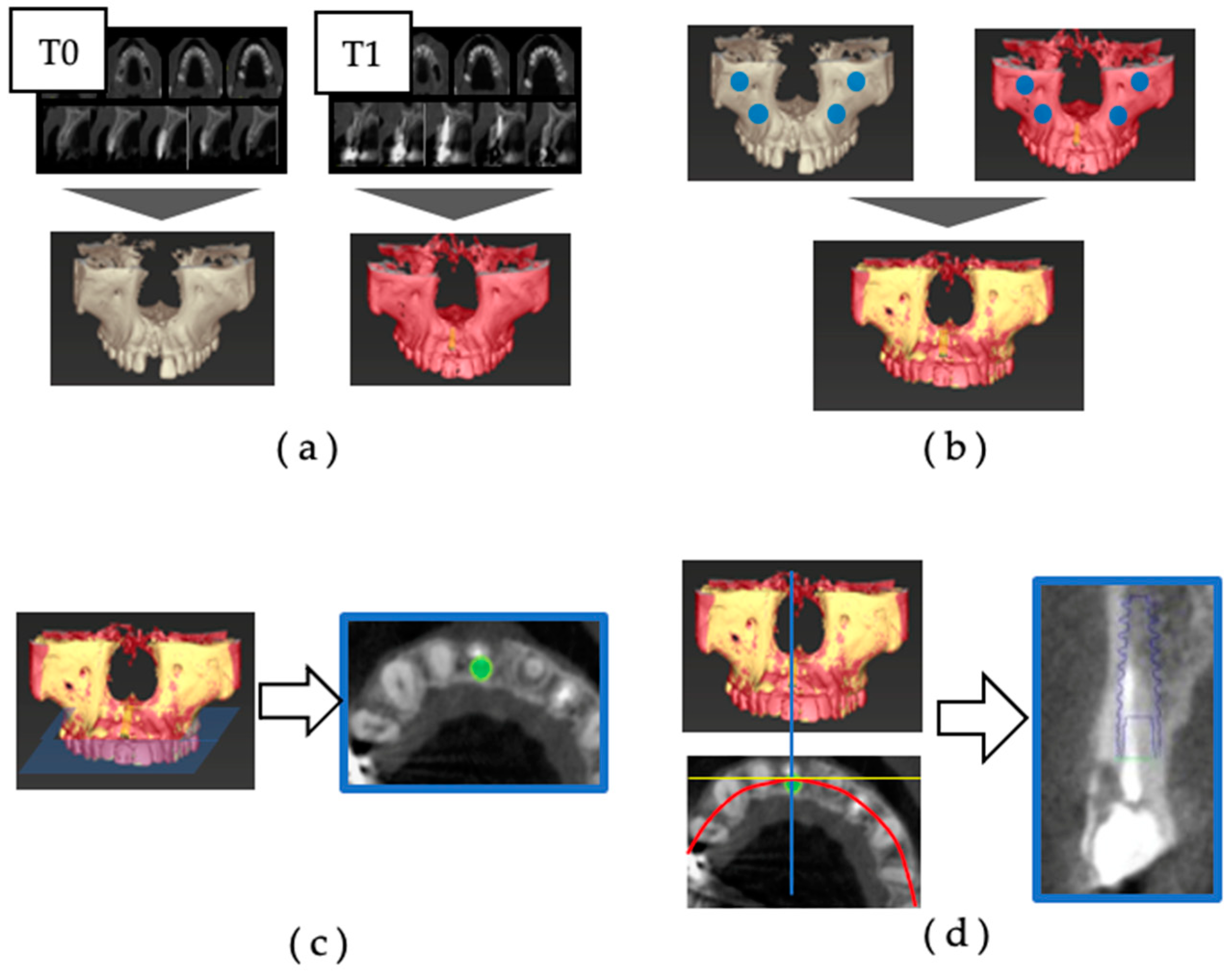
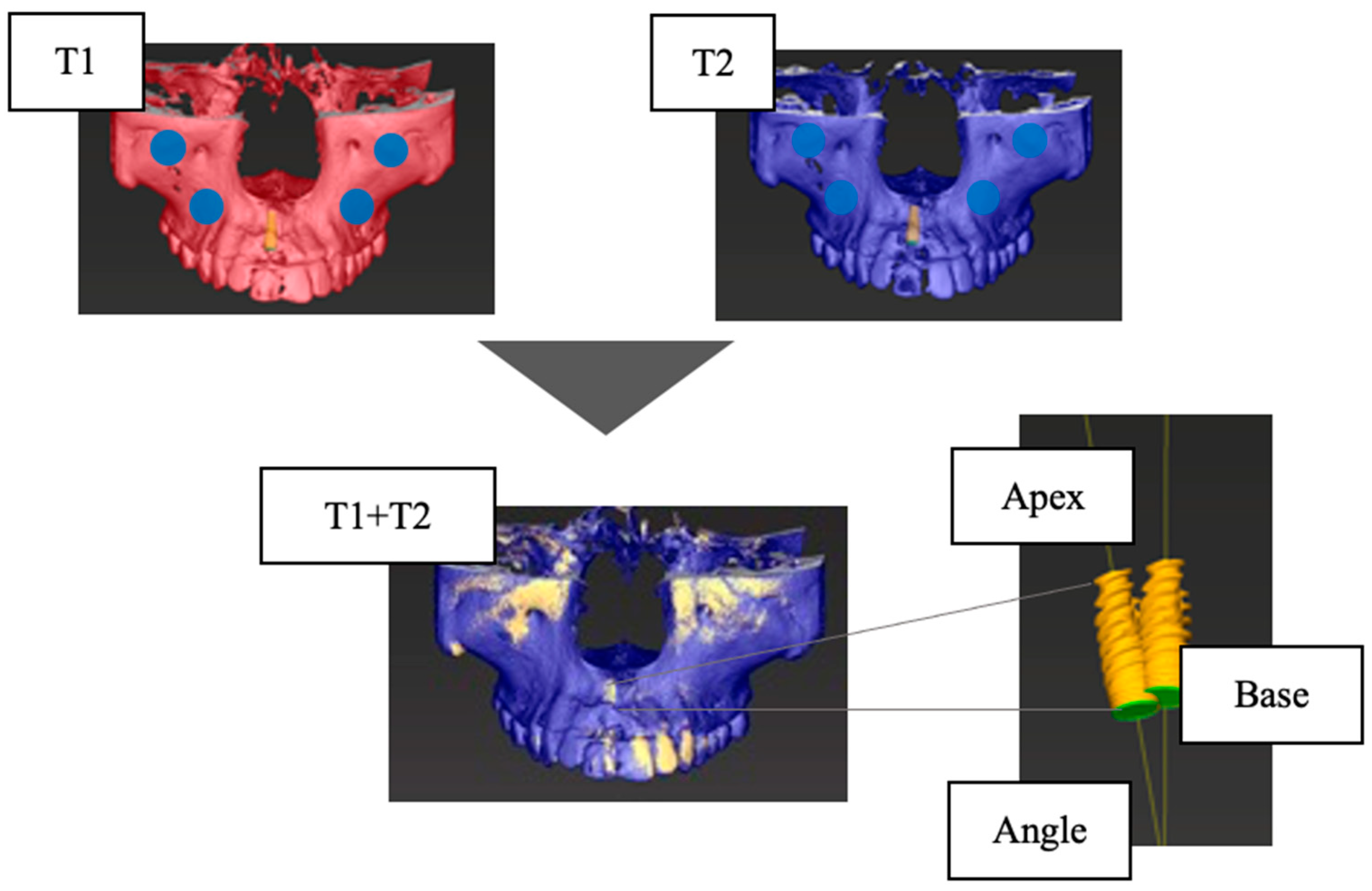
2.8. Accuracy of Superposition of CBCT before and after Operation
- (a)
- The 3D jawbone models of T0 and T1 were created based on CBCT data.
- (b)
- The reference points for superimposition were set at the infraorbital foramen and zygomatic process on the left and right sides, and the 3D jaw models of T0 and T1 were superimposed.
- (c)
- Using superimposition of the three-dimensional jawbone model, an implant model (IM) was placed in the same position as the actually placed implant body on the preoperative CBCT data. The dental arch was set to pass through the center of the implant body and the center of the remaining teeth on the horizontal section, and the cross-section including the platform of the IM was defined as the axial section.
- (d)
- In the axial section, the cross-section was defined as the section that was orthogonal to the tangent line of the dental arch and passed through the center of the IM.
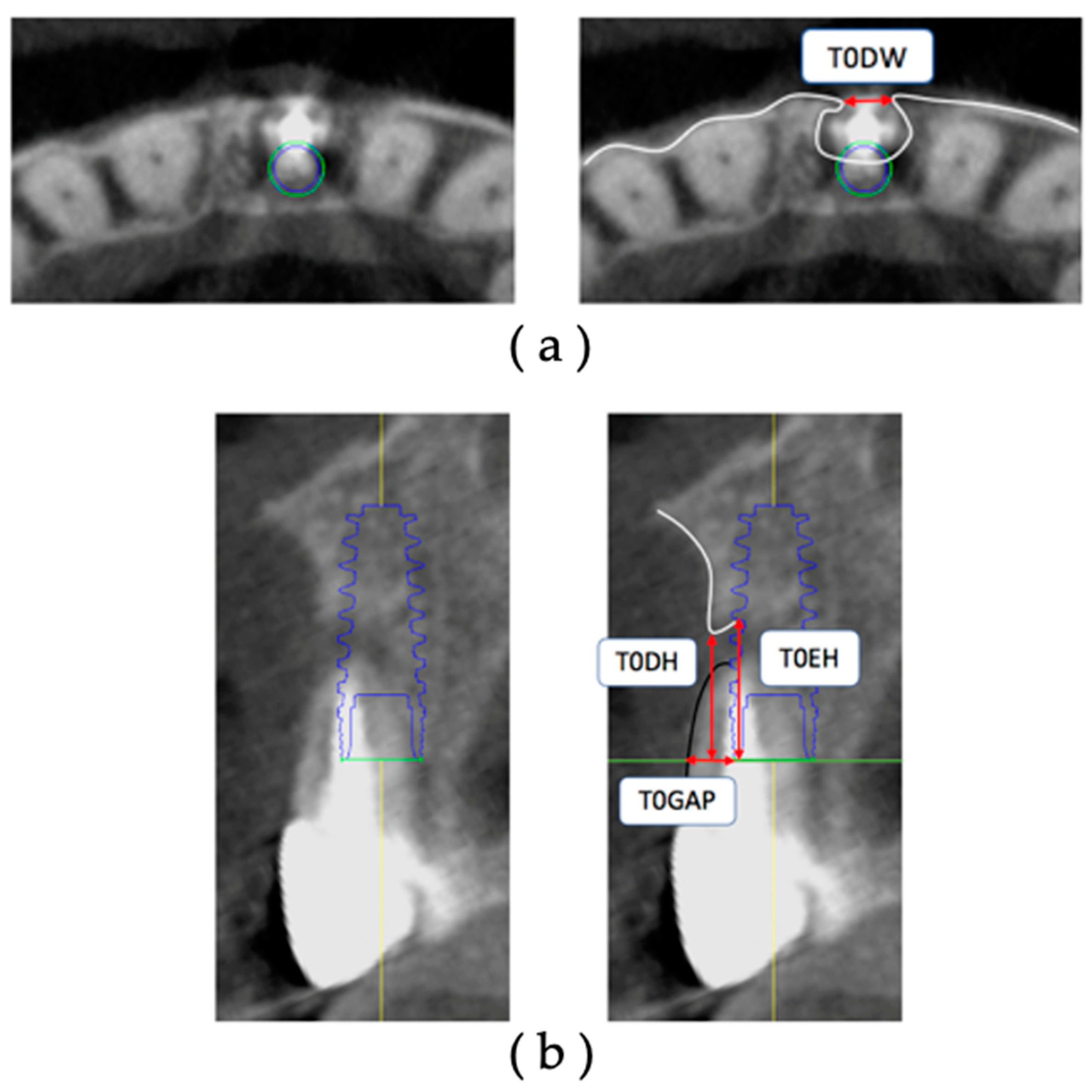
2.9. Measurement of Facial Alveolar Bone Morphology before Operation
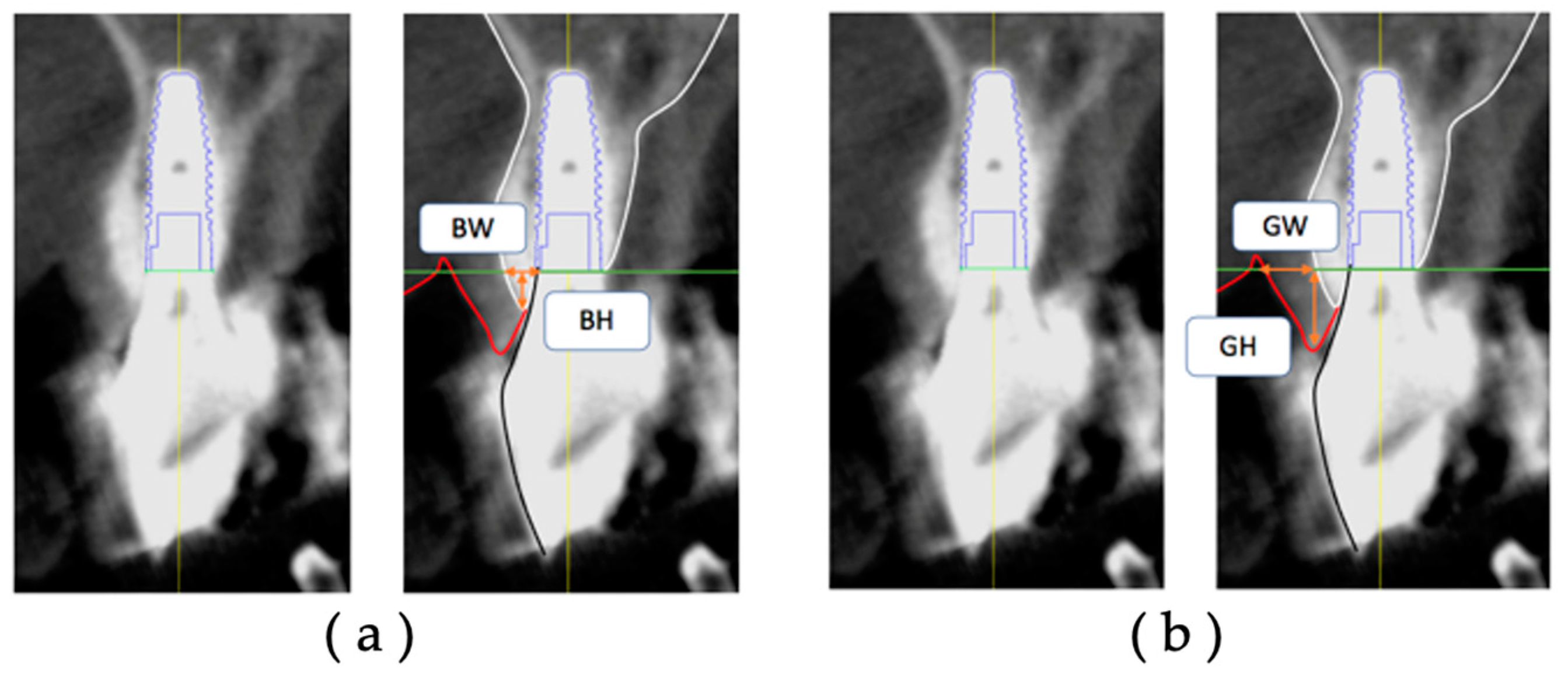
2.10. Measurement of Facial Alveolar Bone Morphology after Restoration
2.11. Statistical Analysis
3. Results
3.1. Patients
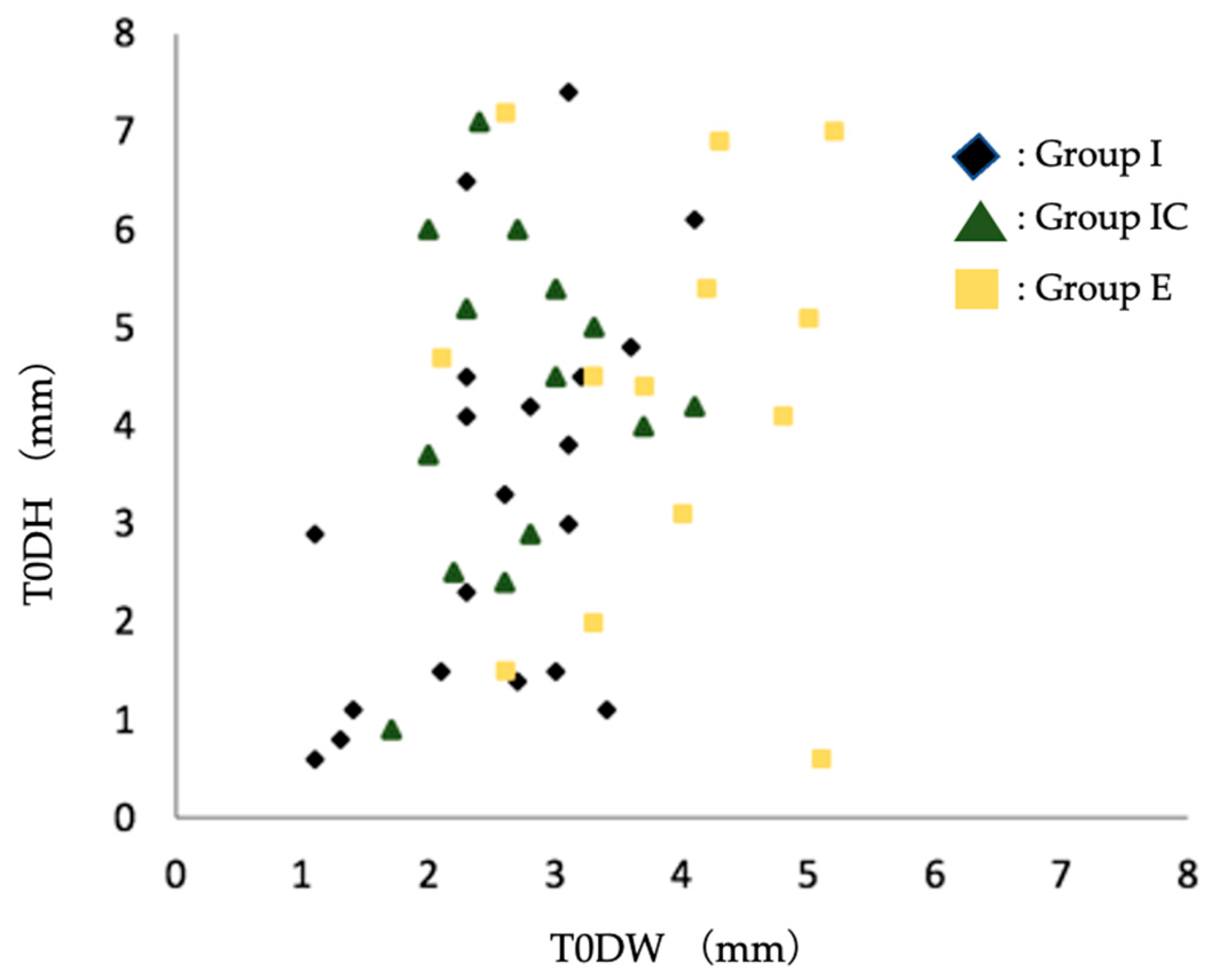
3.2. Group Evaluation of Dehiscence Morphology of Facial Alveolar Bone before Tooth Extraction
3.3. Group Evaluation of the Change in Postoperative Implant Facial Tissue Morphology over Time
4. Discussion
4.1. Group Evaluation of Dehiscence Morphology of Labial Alveolar Bone before Tooth Extraction
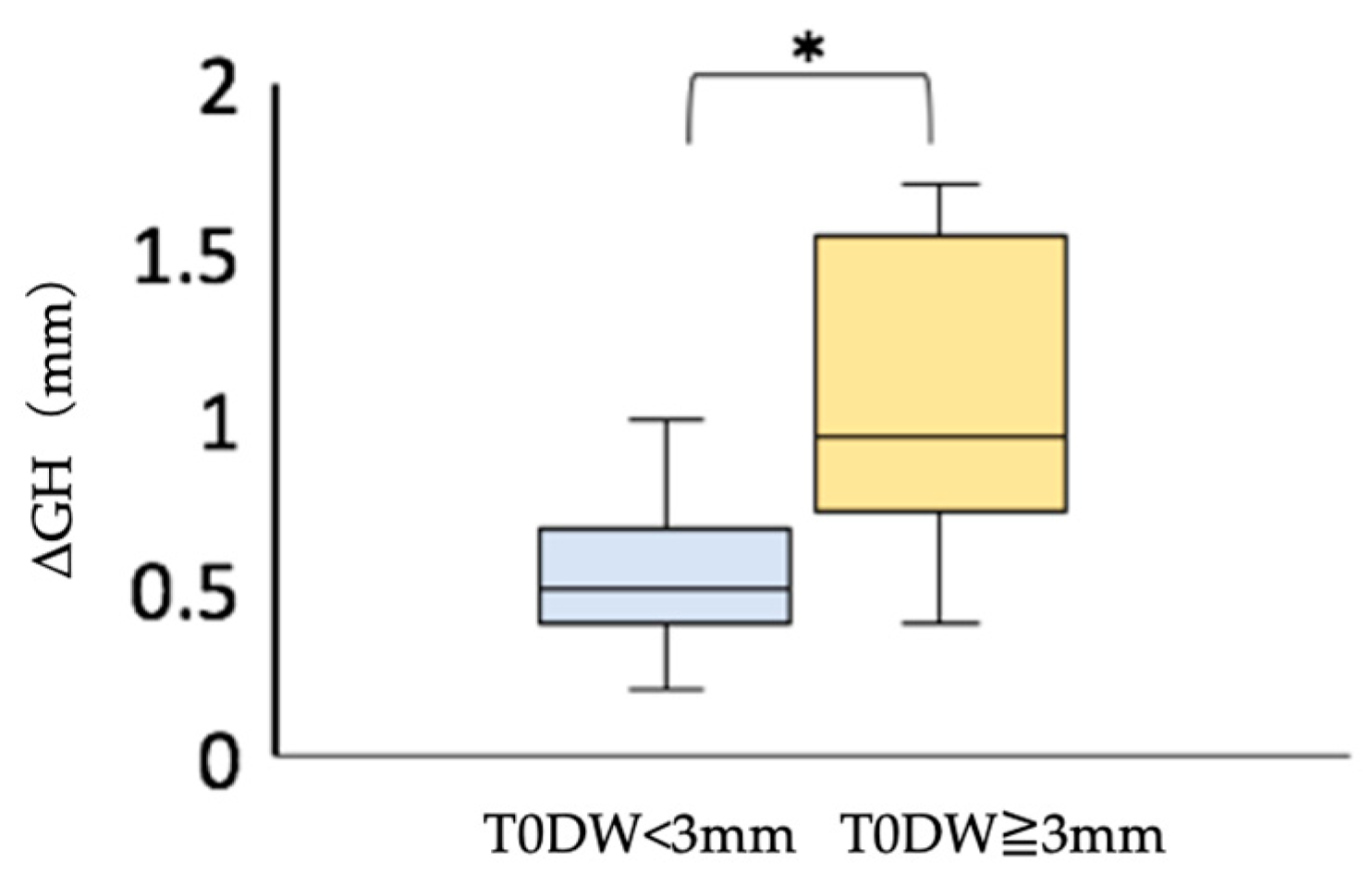
4.2. Group Evaluation of the Change in Postoperative Implant Labial Tissue Morphology over Time
5. Conclusions
- It was found that immediate implant placement might have good esthetic results if the dehiscence was less than 3 mm wide. If the dehiscence was wider than 3–4 mm, there was a tendency to avoid immediate implant placement.
- In cases with dehiscence, thicker labial soft tissues could be obtained by combining immediate implant placement and connective tissue grafting or by waiting for the soft tissues to heal after tooth extraction in early implant placement. This result suggests that the amount of soft tissue regression can be reduced.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buser, D.; Chappuis, V.; Belser, U.C.; Chen, S. Implant placement post extraction in esthetic single tooth sites: When immediate, when early, when late? Periodontology 2000 2017, 73, 84–102. [Google Scholar] [CrossRef]
- Hämmerle, C.H.F.; Chen, S.T.; Wilson, T.G. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int. J. Oral Maxillofac. Implant. 2004, 19, 26–28. [Google Scholar]
- Chen, S.T.; Buser, D. Clinical and esthetic outcomes of implants placed in postextraction sites. Int. J. Oral Maxillofac. Implant. 2009, 24, 186–217. [Google Scholar]
- Arora, H.; Ivanovski, S. Correlation between preoperative buccal bone thickness and soft tissue changes around immediately placed and restored implants in the maxillary anterior region: A 2-year prospective study. Clin. Oral Implant. Res. 2017, 28, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Pun, L.; Lau, K.Y.; Li, K.Y.; Wong, M.C.M. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin. Oral Implant. Res. 2012, 23, 39–66. [Google Scholar] [CrossRef] [PubMed]
- Roe, P.J.; Kan, J.Y.K.; Rungcharassaeng, K.; Caruso, J.M.; Zimmerman, G.; Mesquida, J. Horizontal and vertical dimensional changes of peri-implant facial bone following immediate placement and provisionalization of maxillary anterior single implants: A 1-year cone beam computed tomography study. Int. J. Oral Maxillofac. Implant. 2012, 27, 393–400. [Google Scholar]
- Tonetti, M.S. Immediate versus delayed implant placement after anterior single tooth extraction: The timing randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 215–224. [Google Scholar] [CrossRef]
- Cosyn, J.; Eghbali, A.; Hermans, A.; Vervaeke, S.; Bruyn, H.; Cleymaet, R. A 5-year prospective study on single immediate implants in the aesthetic zone. J. Clin. Periodontol. 2016, 43, 702–709. [Google Scholar] [CrossRef]
- Morton, D.; Chen, S.; Martin, W.; Levine, R.; Buser, D. Consensus Statements and Recommended Clinical Procedures Regarding Optimizing Esthetic Outcomes in Implant Dentistry. Int. J. Oral Maxillofac. Implant. 2014, 29, 186–215. [Google Scholar] [CrossRef]
- Zuiderveld, E.G.; Meijer, H.J.A.; Hartog, L.; Vissink, A.; Raghoebar, G.M. Effect of connective tissue grafting on peri-implant tissue in single immediate implant sites: A RCT. J. Clin. Periodontol. 2018, 45, 253–264. [Google Scholar] [CrossRef]
- Zuffetti, F.; Capelli, M.; Galli, F.; Fabbro, M.; Testori, A. Post-extraction implant placement into infected versus non-infected sites: A multicenter retrospective clinical study. Clin. Implant Dent. Relat. Res. 2017, 19, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Gong, T.; Lin, W.; Yuan, Q.; Man, Y. Immediate implant placement into posterior sockets with or without buccal bone dehiscence defects: A retrospective cohort study. J. Dent. 2017, 65, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Schärer, P.; Marinello, C.P. Factors influencing the success of GBR. Smoking, timing of implant placement, implant location, bone quality and provisional restoration. J. Clin. Periodontol. 1999, 26, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Ouyang, X.Y. Radiographic and Clinical Outcomes of Ridge Augmentation in Molar Extraction Sockets with Severe Bone Wall Defect. Chin. J. Dent. Res. 2015, 18, 221–228. [Google Scholar]
- Raghoebar, G.M.; Slater, J.J.H.; Den Hartog, L.; Meijer, H.J.A.; Vissink, A. Comparison of procedures for immediate reconstruction of large osseous defects resulting from removal of a single tooth to prepare for insertion of an endosseous implant after healing. Int. J. Oral Maxillofac. Surg. 2009, 38, 736–743. [Google Scholar] [CrossRef]
- Nemcovsky, C.E.; Artzi, Z. Comparative Study of Buccal Dehiscence Defects in Immediate, Delayed, and Late Maxillary Implant Placement with Collagen Membranes: Clinical Healing Between Placement and Second-Stage Surgery. J. Periodontol. 2022, 73, 754–761. [Google Scholar] [CrossRef]
- Benic, G.I.; Mokti, M.; Chen, C.J.; Weber, H.P.; Hämmerle, C.H.F.; Gallucci, G.O. Dimensions of buccal bone and mucosa at immediately placed implants after 7 years: A clinical and cone beam computed tomography study. Clin. Oral Implant. Res. 2012, 23, 560–566. [Google Scholar] [CrossRef]
- Assaf, J.H.; Assaf, D.C.; Antoniazzi, R.P.; Osório, L.B.; França, F.M.G. Correction of Buccal Dehiscence During Immediate Implant Placement Using the Flapless Technique: A Tomographic Evaluation. J. Periodontol. 2017, 88, 173–180. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Reyes, M.; Shahim, K.; Nolte, L.P.; Buser, D. Ridge alterations post-extraction in the esthetic zone: A 3D analysis with CBCT. J. Dent. Res. 2013, 92, 12. [Google Scholar] [CrossRef]
- Wang, D. Accuracy of peri-implant bone thickness and validity of assessing bone augmentation material using cone beam computed tomography. Clin. Oral Investig. 2013, 17, 1601–1609. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Huynh-Ba, G. History of treated periodontitis and smoking as risks for implant therapy. Int. J. Oral Maxillofac. Implant. 2009, 24, 39–68. [Google Scholar]
- Nevins, M.L.; Karimbux, N.Y.; Peter Webe, H.; Giannobile, W.V.; Fiorellini, J.P. Wound healing around endosseous implants in experimental diabetes. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 1999, 87, 293. [Google Scholar] [CrossRef]
- Kaminaka, A.; Nakano, T.; Ono, S.; Kato, T.; Yatani, H. Cone-Beam Computed Tomography Evaluation of Horizontal and Vertical Dimensional Changes in Buccal Peri-Implant Alveolar Bone and Soft Tissue: A 1-Year Prospective Clinical Study. Clin. Implant Dent. Relat. Res. 2015, 17, e576–e585. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, K.; Nakano, T.; Shimomoto, T.; Fujita, Y.; Ishigaki, S. The efficacy of immediate implant placement in the anterior maxilla with dehiscence in the facial alveolar bone: A case series. Clin. Implant Dent. Relat. Res. 2021, 24, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.K.; Rungcharassaeng, K.; Sclar, A.; Lozada, J.L. Effects of the Facial Osseous Defect Morphology on Gingival Dynamics After Immediate Tooth Replacement and Guided Bone Regeneration: 1-Year Results. J. Oral Maxillofac. Surg. 2007, 65, 13–19. [Google Scholar] [CrossRef]
- Shiratori, L.N.; Chilvarquer, I. Measurement of buccal bone volume of dental implants by means of cone-beam computed tomography. Clin. Oral Implant. Res. 2012, 23, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.M.; Duncan, W.J.; Coates, D.E. Attributes of Bio-Oss® and Moa-Bone® graft materials in a pilot study using the sheep maxillary sinus model. J. Periodontal Res. 2018, 53, 80–90. [Google Scholar] [CrossRef]
- Sartori, S.; Silvestri, M.; Forni, F.; Cornaglia, A.I.; Tesei, P.; Cattaneo, V. Ten-year follow-up in a maxillary sinus augmentation using anorganic bovine bone (Bio-Oss). A case report with histomorphometric evaluation. Clin. Oral Implant. Res. 2003, 14, 369–372. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Lindhe, J. Healing around implants placed in bone defects treated with Bio-Oss®: An experimental study in the dog. Clin. Oral Implant. Res. 1997, 8, 117–124. [Google Scholar] [CrossRef]
- Miyamoto, Y.; Obama, T. Dental cone beam computed tomography analyses of postoperative labial bone thickness in maxillary anterior implants: Comparing immediate and delayed implant placement. Int. J. Periodontics Restor. Dent. 2011, 31, 215–225. [Google Scholar]
- Chu, S. Flapless Postextraction Socket Implant Placement, Part 2: The Effects of Bone Grafting and Provisional Restoration on Peri-implant Soft Tissue Height and Thickness—A Retrospective Study. Int. J. Periodontics Restor. Dent. 2015, 35, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Darby, I.B.; Adams, G.G.; Reynolds, E.C. A prospective clinical study of bone augmentation techniques at immediate implants. Clin. Oral Implant. Res. 2005, 16, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Chappuis, V.; Bornstein, M.M.; Buser, D.; Belser, U. Influence of implant neck design on facial bone crest dimensions in the esthetic zone analyzed by cone beam CT: A comparative study with a 5-to-9-year follow-up. Clin. Oral Implant. Res. 2016, 27, 1055–1064. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Field of View (FOV) | 833 cm3: Diameter 102 mm × Height 102 mm |
|---|---|
| Voxel value | 0.2 mm |
| Tube Voltage | 80 kV |
| Tube current | 7 mA |
| Shooting time | 17,000 msec |
| Average | SD | |
|---|---|---|
| Base (mm) | 0.05 | 0.02 |
| Apex (mm) | 0.07 | 0.03 |
| Angle (°) | 0.21 | 0.07 |
| Measurement Item | Intraexaminer Reliability ICC (1, 1) | Interexaminer Reliability ICC (2, 1) |
|---|---|---|
| T0DW | 0.91 | 0.90 |
| T0DH | 0.89 | 0.87 |
| T0GAP | 0.87 | 0.89 |
| T0EH | 0.93 | 0.94 |
| Measurement Item | Intraexaminer Reliability ICC (1, 1) | Interexaminer Reliability ICC (2, 1) |
|---|---|---|
| BW | 0.92 | 0.93 |
| BH | 0.87 | 0.89 |
| GW | 0.89 | 0.87 |
| GH | 0.84 | 0.89 |
| Group I | Group IC | Group E | p Value | ||
|---|---|---|---|---|---|
| Male/female ratio * | 9/11 | 6/10 | 6/10 | 0.97 | |
| Age (year) † | 61.5 ± 13.9 | 58.4 ± 15.1 | 61.2 ± 19.3 | 0.62 | |
| Measurement area (location) * | Middle incisors | 7 | 8 | 5 | 0.11 |
| Lateral incisors | 9 | 4 | 4 | ||
| Canine | 2 | 2 | 3 | ||
| First premolar | 2 | 2 | 4 | ||
| Group I | Group IC | Group E | p Value | |||
|---|---|---|---|---|---|---|
| Length of implant body (mm) † | 12.3 ± 1.1 | 12.4 ± 1.1 | 11.8 ± 1.0 | 0.35 | ||
| Diameter of the implant body (mm) † | 3.7 ± 0.4 | 4.0 ± 0.4 | 3.9 ± 0.4 | 0.11 | ||
| Manufacturer of implant body, Implant design * | Nobel Biocare | Nobel Active | 13 | 10 | 7 | 0.83 |
| Nobel Parallel Conical Connection | 0 | 1 | 2 | |||
| Nobel Replace Conical Connection | 2 | 2 | 2 | |||
| Straumann | BLT | 5 | 3 | 5 | ||
| Superstructure fixation style * | Screw retain | 16 | 12 | 13 | 0.98 | |
| Cement retain | 4 | 4 | 3 | |||
| Number of surviving implants | 20/20 | 16/16 | 16/16 | |||
| Group I (n = 20) | Group IC (n = 16) | Group E (n = 16) | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| Measurement Item | Mean (SD) | Median [Max, Min] | Mean (SD) | Median [Max, Min] | Mean (SD) | Median [Max, Min] | |
| T0DW (mm) | 2.5 (0.8) | 2.7 [4.1, 1.1] | 2.7 (0.7) | 2.7 [4.1, 1.7] | 3.9 (1.0) | 4.0 [5.2, 2.1] | 0.003 |
| T0DH (mm) | 3.3 (2.0) | 3.2 [7.4, 0.6] | 4.3 (1.7) | 4.4 [7.1, 0.9] | 4.3 (2.1) | 4.5 [7.2, 0.6] | 0.193 |
| T0GAP (mm) | 2.1 (0.7) | 2.1 [4.7, 0.9] | 2.4 (1.1) | 2.2 [4.4, 0.6] | 2.4 (0.8) | 2.5 [4.2, 1.0] | 0.531 |
| T0EH (mm) | 4.9 (1.5) | 5.2 [7.4, 2.0] | 5.1 (1.8) | 5.6 [7.2, 0.8] | 5.4 (2.3) | 4.9 [9.6, 2.3] | 0.881 |
| Group I (n = 20) | Group IC (n = 16) | Group E (n = 16) | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| Measurement Item | Mean (SD) | Median [Max, Min] | Mean (SD) | Median [Max, Min] | Mean (SD) | Median [Max, Min] | |
| T1BW (mm) | 2.1 (0.8) | 1.9 [ 3.5, 0.4] | 2.0 (1.0) | 1.8 [4.0, 0.4] | 2.3 (1.0) | 2.5 [3.5, 0.6] | 0.552 |
| T2BW (mm) | 1.6 (0.8) | 1.7 [3.4, 0.3] | 1.8 (1.0) | 1.7 [3.6, 0.4] | 2.0 (1.0) | 2.0 [3.4, 0.4] | 0.459 |
| ΔBW(mm) | 0.5 (0.5) | 0.3 [2.0, 0] | 0.3 (0.2) | 0.3 [0.6, 0] | 0.3 (0.2) | 0.3 [0.8, 0] | 0.668 |
| T1BH (mm) | 1.7 (0.6) | 1.7 [2.8, 0.6] | 1.6 (1.0) | 1.7 [3.1, 0] | 1.6 (0.8) | 1.5 [2.7, 0] | 0.923 |
| T2BH (mm) | 1.0 (0.5) | 1.0 [2.1, 0.3] | 1.3 (1.0) | 1.4 [2.9, 0] | 1.3 (0.8) | 1.1 [2.6, 0] | 0.447 |
| ΔBH (mm) | 0.7 (0.4) | 0.7 [1.4, 0.2] | 0.3 (0.2) | 0.2 [0.7, 0] | 0.2 (0.2) | 0.2 [0.7, 0] | 0.000 |
| T1GW (mm) | 2.1 (0.4) | 2.1 [3.0, 1.5] | 2.8 (0.7) | 2.8 [3.8, 1.9] | 2.7 (0.7) | 2.7 [3.8, 1.8] | 0.001 |
| T2GW (mm) | 1.8 (0.4) | 1.8 [2.7, 1.2] | 2.6 (0.7) | 2.5 [3.7, 1.5] | 2.4 (0.6) | 2.3 [3.4, 1.5] | 0.001 |
| ΔGW (mm) | 0.3 (0.2) | 0.3 [0.8, 0] | 0.2 (0.2) | 0.2 [0.7, 0] | 0.3 (0.2) | 0.2 [0.8, 0] | 0.582 |
| T1GH (mm) | 4.5 (0.9) | 4.4 [5.7, 1.8] | 5.0 (1.0) | 5.2 [6.2, 2.5] | 4.6 (1.0) | 4.9 [6.0, 2.9] | 0.334 |
| T2GH (mm) | 3.8 (1.0) | 3.9 [5.2, 1.1] | 4.6 (1.0) | 4.6 [5.8, 2.1] | 4.4 (1.1) | 4.1 [6.0, 2.4] | 0.054 |
| ΔGH (mm) | 0.7 (0.4) | 0.6 [1.7, 0.2] | 0.3 (0.3) | 0.3 [1.0, 0] | 0.3 (0.2) | 0.2 [0.8, 0] | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujii, M.; Nakano, T.; Ishigaki, S. Pre- and Postoperative Evaluation of Immediate and Early Implant Placement in Esthetic Areas with Pre-Extraction Facial Dehiscence: A Retrospective Clinical Study. J. Clin. Med. 2023, 12, 6616. https://doi.org/10.3390/jcm12206616
Fujii M, Nakano T, Ishigaki S. Pre- and Postoperative Evaluation of Immediate and Early Implant Placement in Esthetic Areas with Pre-Extraction Facial Dehiscence: A Retrospective Clinical Study. Journal of Clinical Medicine. 2023; 12(20):6616. https://doi.org/10.3390/jcm12206616
Chicago/Turabian StyleFujii, Misa, Tamaki Nakano, and Shoichi Ishigaki. 2023. "Pre- and Postoperative Evaluation of Immediate and Early Implant Placement in Esthetic Areas with Pre-Extraction Facial Dehiscence: A Retrospective Clinical Study" Journal of Clinical Medicine 12, no. 20: 6616. https://doi.org/10.3390/jcm12206616
APA StyleFujii, M., Nakano, T., & Ishigaki, S. (2023). Pre- and Postoperative Evaluation of Immediate and Early Implant Placement in Esthetic Areas with Pre-Extraction Facial Dehiscence: A Retrospective Clinical Study. Journal of Clinical Medicine, 12(20), 6616. https://doi.org/10.3390/jcm12206616