

Clinical Evidence Regarding the Dynamic of Baker Cyst Dimensions after Intermittent Vacuum Therapy as Rehabilitation Treatment in Patients with Knee Osteoarthritis
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Model
2.2. Study Population
2.3. Procedures
2.4. Randomization, Group Allocation and Blinding
2.5. Sample Size
2.6. Study Objectives
2.7. Data Analysis
3. Results
3.1. Study Population
3.2. Clinical–Functional Status
4. Discussion
4.1. Study Strengths
4.2. Study Limitations
4.3. Facts and Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abate, M.; Di Carlo, L.; Di Iorio, A.; Salini, V. Baker’s Cyst with Knee Osteoarthritis: Clinical and Therapeutic Implications. Med. Princ. Pract. 2021, 30, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Henricsdotter, C.; Ellegaard, K.; Klokker, L.; Bartholdy, C.; Bandak, E.; Bartels, E.M.; Bliddal, H.; Henriksen, M. Changes in ultrasound assessed markers of inflammation following intra-articular steroid injection combined with exercise in knee osteoarthritis: Exploratory outcome from a randomized trial. Osteoarthr. Cartil. 2016, 24, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Taş, N.; Uzkeser, H.; Erdal, A. Is USG-guided aspiration more effective than physiotherapy in the treatment of Baker’s cyst? Anatol. Curr. Med. J. 2022, 4, 24–28. [Google Scholar] [CrossRef]
- Di Sante, L.; Paoloni, M.; Ioppolo, F.; Dimaggio, M.; Di Renzo, S.; Santilli, V. Ultrasound-guided aspiration and corticosteroid injection of Baker’s cysts in knee osteoarthritis: A prospective observational study. Am. J. Phys. Med. Rehabil. 2010, 89, 970–975. [Google Scholar] [CrossRef]
- Zhou, X.N.; Li, B.; Wang, J.S.; Bai, L.H. Surgical treatment of popliteal cyst: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2016, 15, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Wiecha, S.; Jarocka, M.; Wiśniowski, P.; Cieśliński, M.; Price, S.; Makaruk, B.; Kotowska, J.; Drabarek, D.; Cieśliński, I.; Sacewicz, T. The efficacy of intermittent pneumatic compression and negative pressure therapy on muscle function, soreness and serum indices of muscle damage: A randomized controlled trial. BMC Sports Sci. Med. Rehabil. 2021, 13, 144. [Google Scholar] [CrossRef] [PubMed]
- Parganlija, D.; Nieberg, V.; Sauer, M.; Rittweger, J.; Bloch, W.; Zange, J. Lower body negative pressure enhances oxygen availability in the knee extensor muscles during intense resistive exercise in supine position. Eur. J. Appl. Physiol. 2019, 119, 1289–1303. [Google Scholar] [CrossRef]
- Dong, H.H.; Gao, B.H.; Zhu, H.; Yang, S.T. The effects of lower limb intermittent negative pressure therapy on the skin microcirculation perfusion of quadriceps in male rowers. Zhongguo Ying Yong Sheng Li Xue Za Zhi 2019, 35, 126–129. [Google Scholar]
- Yogendrakumar, V.; Lun, R.; Hutton, B.; Fergusson, D.A.; Dowlatshahi, D. Comparing pharmacological venous thromboembolism prophylaxis to intermittent pneumatic compression in acute intracerebral haemorrhage: Protocol for a systematic review and network meta-analysis. BMJ Open 2018, 8, e024405. [Google Scholar] [CrossRef]
- Sarman, H.; Muezzinoglu, U.S.; Memisoglu, K.; Baran, T. Vacuum-assisted closure for skin necrosis after revision total knee arthroplasty. Int. Wound J. 2016, 13, 843–847. [Google Scholar] [CrossRef]
- Hageman, D.; Fokkenrood, H.J.P.; van Deursen, B.A.C.; Gommans, L.N.M.; Cancrinus, E.; Scheltinga, M.R.M.; Teijink, J.A.W. Randomized controlled trial of vacuum therapy for intermittent claudication. J. Vasc. Surg. 2020, 71, 1692–1701.e1. [Google Scholar] [CrossRef]
- Derouet, H.; Caspari, D.; Rohde, V.; Rommel, G.; Ziegler, M. Treatment of erectile dysfunction with external vacuum devices. Andrologia 1999, 31 (Suppl. S1), 89–94. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Wu, D.; Li, J. Clinical Efficacy of Mudpack Therapy in Treating Knee Osteoarthritis: A Meta-Analysis of Randomized Controlled Studies. Am. J. Phys. Med. Rehabil. 2016, 95, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Sukenik, S. Balneotherapy for rheumatic diseases at the Dead Sea area. Isr. J. Med. Sci. 1996, 32 (Suppl. S1), S16–S19. [Google Scholar] [PubMed]
- Iliescu, M.G.; Ionescu, E.V.; Tica, I.; Prazaru, M.D.; Popa, F.L.; Popescu, M.N.; Berteanu, M.; Irsay, L.; Ciortea, V.M.; Voinea, F.; et al. The role of natural biotherapeutic factors in pain and functional management of knee osteoarthritis. Farmacia 2022, 70, 65–69. [Google Scholar] [CrossRef]
- Ionescu, E.V.; Suta, M.; Surdu, O.; Oprea, C.; Stoicescu, R.M.; Taralunga, G.; Lilios, G. Clinical and Biological Effects Induced by Sapropelic Mud from the Lake Techirghiol in Patients with Osteoarthritis. J. Environ. Prot. Ecol. 2014, 15, 332–339. [Google Scholar]
- Vojtassak, J., Jr.; Vojtassak, J., Sr. Ultrasound monitoring of the treatment of clinically significant knee osteoarthritis. Bratisl. Lek. Listy 2014, 115, 86–90. [Google Scholar] [PubMed]
- Bećić, T.; Prlić, N.; Babić-Naglić, D. The effect of muscle strengthening exercises on the Baker cyst and functional capacity in patients with knee osteoarthritis. Rheumatol. Int. 2019, 39, 123–131. [Google Scholar]
- Tuncer, T.; Kanatlı, U.; Şahin, H.; Duygun, F. Prevalence and clinical characteristics of Baker’s cyst in rheumatoid arthritis. Clin. Rheumatol. 2015, 34, 741–746. [Google Scholar]
- Han, D.Y.; Ryu, K.N.; Park, J.S.; Jin, W.; Park, S.Y.; Yun, S.J. The prevalence of Baker cyst in relation to the arrangement pattern between the medial head of gastrocnemius tendon and the semimembranosus tendon. Eur. Radiol. 2020, 30, 1544–1553. [Google Scholar] [CrossRef]
- Tanaka, N.; Sakahashi, H.; Ishima, T.; Imai, T.; Nakamura, T. Popliteal cyst in adults: Prevalence, associated intra-articular lesions, and results of excision. Rheumatology 2001, 40, 696–700. [Google Scholar]
- Kanthawang, T.; Bodden, J.; Joseph, G.B.; Lane, N.E.; Nevitt, M.; McCulloch, C.E.; Link, T.M. Obese and overweight individuals have greater knee synovial inflammation and associated structural and cartilage compositional degeneration: Data from the osteoarthritis initiative. Skelet. Radiol. 2021, 50, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Laberge, M.A.; Baum, T.; Virayavanich, W.; Nardo, L.; Nevitt, M.C.; Lynch, J.; McCulloch, C.E.; Link, T.M. Obesity increases the prevalence and severity of focal knee abnormalities diagnosed using 3T MRI in middle-aged subjects—Data from the Osteoarthritis Initiative. Skelet. Radiol. 2012, 41, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Malas, F.Ü.; Kara, M.; Kaymak, B.; Akıncı, A.; Özçakar, L. Ultrasonographic evaluation in symptomatic knee osteoarthritis: Clinical and radiological correlation. Int. J. Rheum. Dis. 2014, 17, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Saylik, M.; Gokkus, K.; Sahin, M.S. Factors affecting Baker cyst volume, with emphasis on cartilage lesion degree and effusion in the young and middle-aged population. BMC Musculoskelet. Disord. 2021, 22, 851. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S. WOMAC Osteoarthritis Index—Additional dimensions for use in subjects with post-traumatic osteoarthritis of the knee. Osteoarthr. Cartil. 1999, 7, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Kandemirli, G.C.; Basaran, M.; Kandemirli, S.; Inceoglu, L.A. Assessment of knee osteoarthritis by ultrasonography and its association with knee pain. J. Back Musculoskelet. Rehabil. 2020, 33, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Salca, A.; Stoica, N.; Dogaru, G. Treatment of knee OSTEOARTHRITIS in Spa Health resorts: Where do we stand? Balneo Res. J. 2015, 6, 184–194. [Google Scholar] [CrossRef]
- Silisteanu, S.C.; Antonescu, E.; Totan, M. Study on the importance of medical treatment and physical methods in recovering patients with knee osteoarthritis. Balneo Res. 2019, 10, 90–97. [Google Scholar] [CrossRef]
- Sukenik, S.; Flusser, D.; Codish, S.; Abu-Shakra, M. Balneotherapy at the Dead Sea area for knee osteoarthritis. Isr. Med. Assoc. J. 1999, 1, 83–85. [Google Scholar]
- Nejati, P.; Farzinmehr, A.; Moradi-Lakeh, M. The effect of exercise therapy on knee osteoarthritis: A randomized clinical trial. Med. J. Islam Repub. Iran 2015, 29, 186. [Google Scholar] [PubMed]
- Handy, J.R. Popliteal cysts in adults: A review. Semin. Arthritis Rheum. 2001, 31, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Kan, H.S.; Chan, P.K.; Chiu, K.Y.; Yan, C.H.; Yeung, S.S.; Ng, Y.L.; Shiu, K.W.; Ho, T. Non-surgical treatment of knee osteoarthritis. Hong Kong Med. J. 2019, 25, 127–133. [Google Scholar] [CrossRef]
- Balik, M.S.; Turan, A.; Celik, F.B. Is There A Relationship between Three-Dimensionally Measured Baker’s Cyst Volume and Knee Pathologies? Eurasian J. Med. 2019, 51, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Eker Büyükşireci, D.; Büyükşireci, M.; Komut, E. Evaluation of the effects of dexamethasone iontophoresis, galvanic current, and conservative treatment on pain and disability in patients with knee osteoarthritis and Baker’s cyst. Turk. J. Phys. Med. Rehabil. 2022, 68, 509–516. [Google Scholar] [CrossRef]
- Menant, J.C.; Weber, F.; Lo, J. Poor functional performance predicts falls but not syncopal episodes in aged care residents. J. Gerontol. Biol. Sci. Med. Sci. 2011, 66, 590–596. [Google Scholar]
- Manlapaz, D.G.; Sole, G.; Jayakaran, P.; Chapple, C.M. Risk Factors for Falls in Adults with Knee Osteoarthritis: A Systematic Review. PM R 2019, 11, 745–757. [Google Scholar] [CrossRef] [PubMed]
- Mat, S.; Tan, M.P.; Kamaruzzaman, S.B.; Ng, C.T. Physical therapies for improving balance and reducing falls risk in osteoarthritis of the knee: A systematic review. Age Ageing 2015, 44, 16–24. [Google Scholar] [CrossRef]
- Park, G.Y.; Kwon, D.R.; Kwon, D.G. Clinical, Radiographic, and Ultrasound Findings Between Simple and Complicated Baker’s Cysts. Am. J. Phys. Med. Rehabil. 2020, 99, 7–12. [Google Scholar] [CrossRef]
- Osteras, H.; Kjeken, I.; Smedslund, G. Exercise for hand osteoarthritis. Cochrane Database Syst. Rev. 2017, 1, CD010388. [Google Scholar]
- Hautmann, M.G.; Jung, E.M.; Beyer, L.P.; Süß, C.; Steger, F.; Weber, M.; Pohl, F.; Kölbl, O.; Putz, F.J. Is low dose radiotherapy an effective treatment for Baker’s cyst? Strahlenther Onkol. 2019, 195, 69–76. [Google Scholar] [CrossRef]
- Roos, E.M.; Klässbo, M.; Lohmander, L.S. WOMAC osteoarthritis index. Reliability, validity, and responsiveness in patients with arthroscopically assessed osteoarthritis. Scand. J. Rheumatol. 1999, 28, 210–215. [Google Scholar]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a self-administered outcome measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Oo, W.M.; Linklater, J.M.; Bennell, K.L.; Pryke, D.; Yu, S.; Fu, K.; Wang, X.; Duong, V.; Hunter, D.J. Are OMERACT Knee Osteoarthritis Ultrasound Scores Associated with Pain Severity, Other Symptoms, and Radiographic and Magnetic Resonance Imaging Findings? J. Rheumatol. 2021, 48, 270–278. [Google Scholar] [CrossRef]
- Bevers, K.; Bijlsma, J.W.; Vriezekolk, J.E.; Van den Ende, C.H.; den Broeder, A.A. The course of ultrasonographic abnormalities in knee osteoarthritis: 1 year follow up. Osteoarthr. Cartil. 2014, 22, 1651–1656. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vacuum | Control | p | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | Mean | Median | Min–Max | Std Dev | n | % | Mean | Median | Min–Max | Std Dev | ||
| Sex | 0.124 | ||||||||||||
| Male | 10 | 31.25 | 5 | 15.15 | |||||||||
| Female | 22 | 68.75 | 28 | 84.85 | |||||||||
| Age (years) | 58.66 | 43–77 | 8.71 | 61.36 | 43–75 | 8.34 | 0.181 | ||||||
| Studies | 0.343 | ||||||||||||
| High school | 2 | 6.25 | 0 | 0 | |||||||||
| College | 2 | 6.25 | 2 | 6.06 | |||||||||
| Unspecified | 28 | 87.5 | 31 | 93.94 | |||||||||
| Occupation | 0.395 | ||||||||||||
| No occupation | 3 | 9.38 | 2 | 6.06 | |||||||||
| Employee | 15 | 46.88 | 11 | 33.33 | |||||||||
| Retired | 14 | 43.75 | 20 | 60.61 | |||||||||
| Environment | 0.415 | ||||||||||||
| Urban | 26 | 81.25 | 24 | 72.73 | |||||||||
| Rural | 6 | 18.75 | 9 | 27.27 | |||||||||
| Degree of functional deficit | 0.120 | ||||||||||||
| Minimum | 26 | 81.25 | 31 | 93.94 | |||||||||
| Moderate | 6 | 18.75 | 2 | 6.06 | |||||||||
| BMI (kg/m2) | 29 | 28.58 | 22.99–42.9 | 4.67 | 28.78 | 27.92 | 21.97–38.28 | 3.98 | 0.840 | ||||
| Kellgren–Lawrence | 2.56 | 3 | 1–4 | 0.91 | 2.61 | 3 | 1–4 | 0.93 | 0.932 | ||||
| Vacuum | Control | p | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Std Dev | Min–Max | Percentiles 25–75 | Mean | Median | Std Dev | Min–Max | Percentiles 25–75 | ||
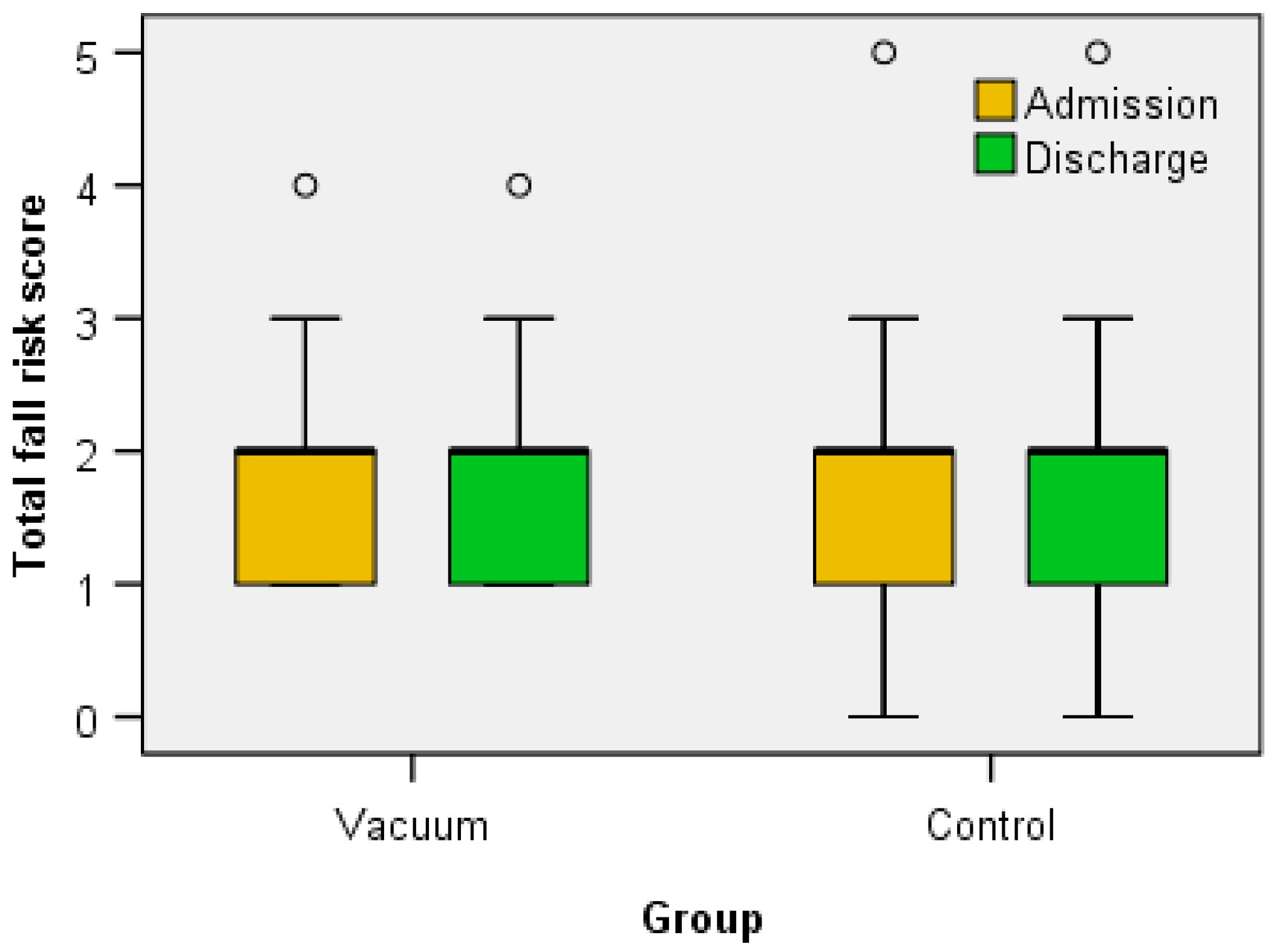
| Fall risk score | |||||||||||
| Admission | 1.78 | 2 | 0.71 | 1–4 | 1–2 | 1.75 | 2 | 0.67 | 1–4 | 1–2 | 0.516 |
| Discharge | 1.75 | 2 | 0.67 | 1–4 | 1–2 | 1.7 | 2 | 0.88 | 0.00–5 | 1–2 | 0.601 |
| p admission/discharge | 0.317 | 0.999 | |||||||||
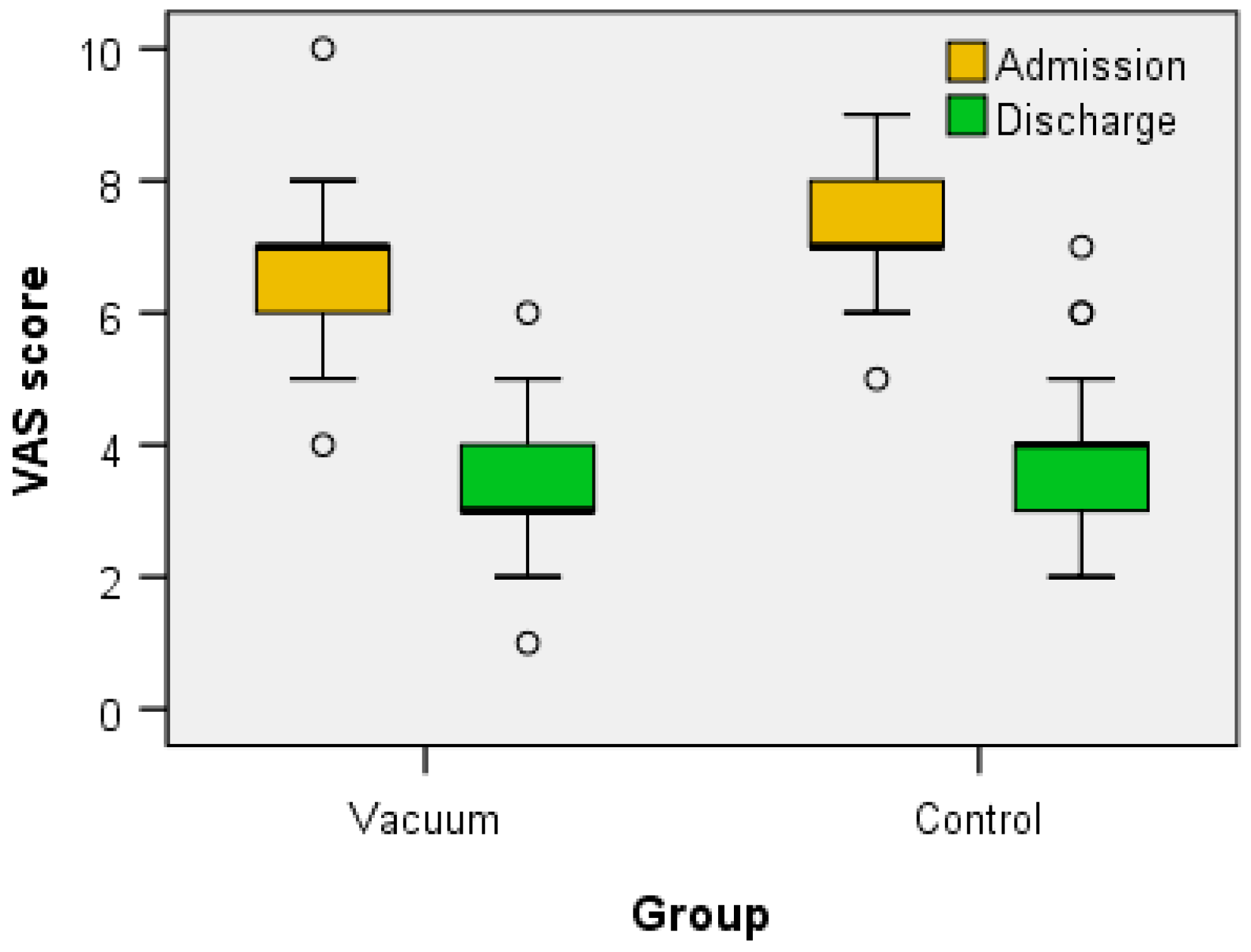
| VAS scale | |||||||||||
| Admission | 6.66 | 7 | 1.04 | 4–10 | 6–7 | 7.15 | 7 | 0.76 | 5–9 | 7–8 | 0.009 |
| Discharge | 3.31 | 3 | 1.09 | 1–6 | 3–4 | 3.88 | 4 | 1.08 | 2–7 | 3–4 | 0.032 |
| p admission/discharge | 0.009 | 0.032 | |||||||||
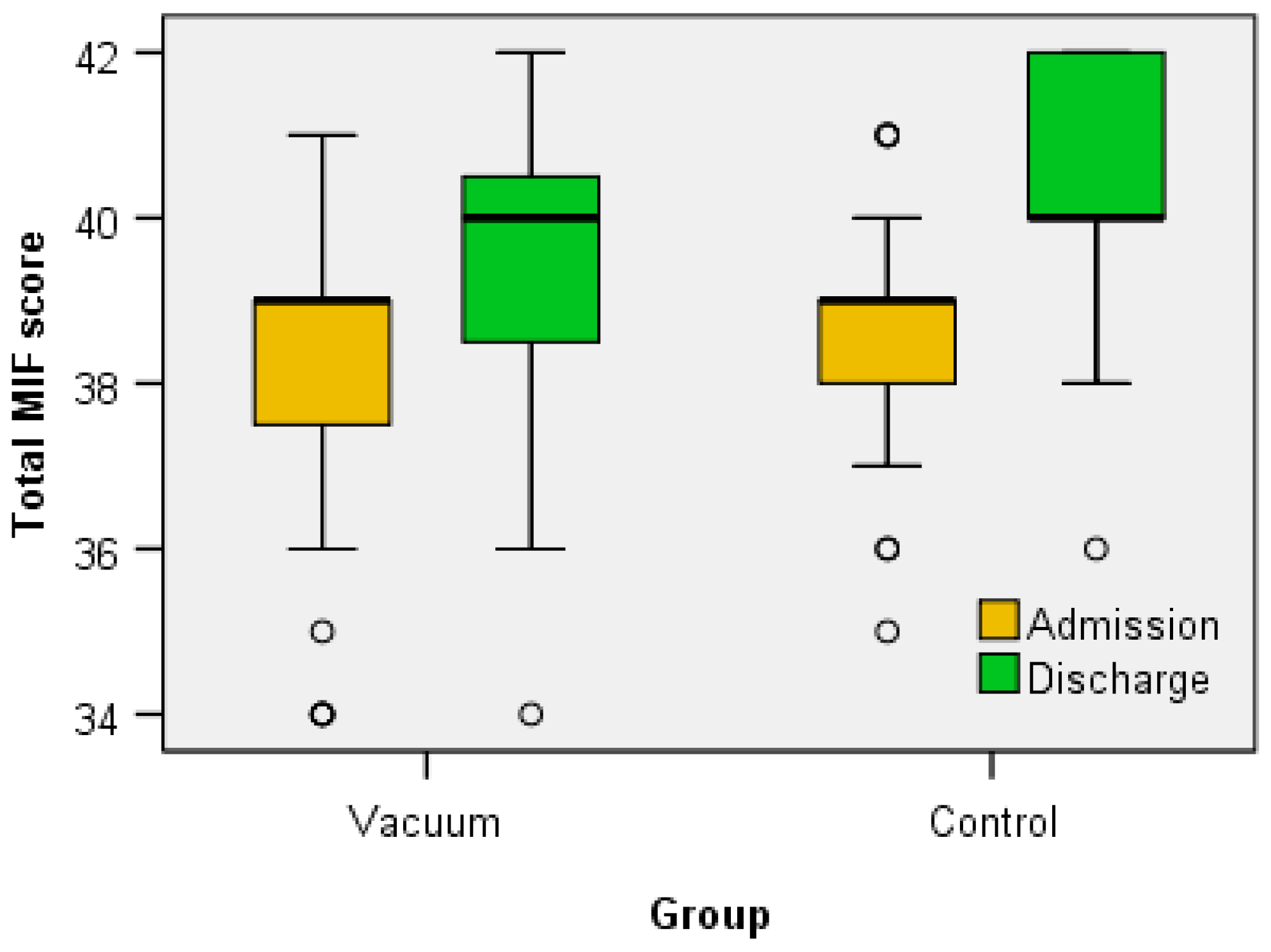
| FIM score | |||||||||||
| Admission | 38.09 | 39 | 1.97 | 34–41 | 37.25–39 | 38.67 | 39 | 1.29 | 35–41 | 38–39 | 0.474 |
| Discharge | 39.41 | 40 | 1.83 | 34–42 | 38.25–40.75 | 40.21 | 40 | 1.43 | 36–42 | 40–42 | 0.077 |
| p admission/discharge | 0.000 | 0.000 | |||||||||
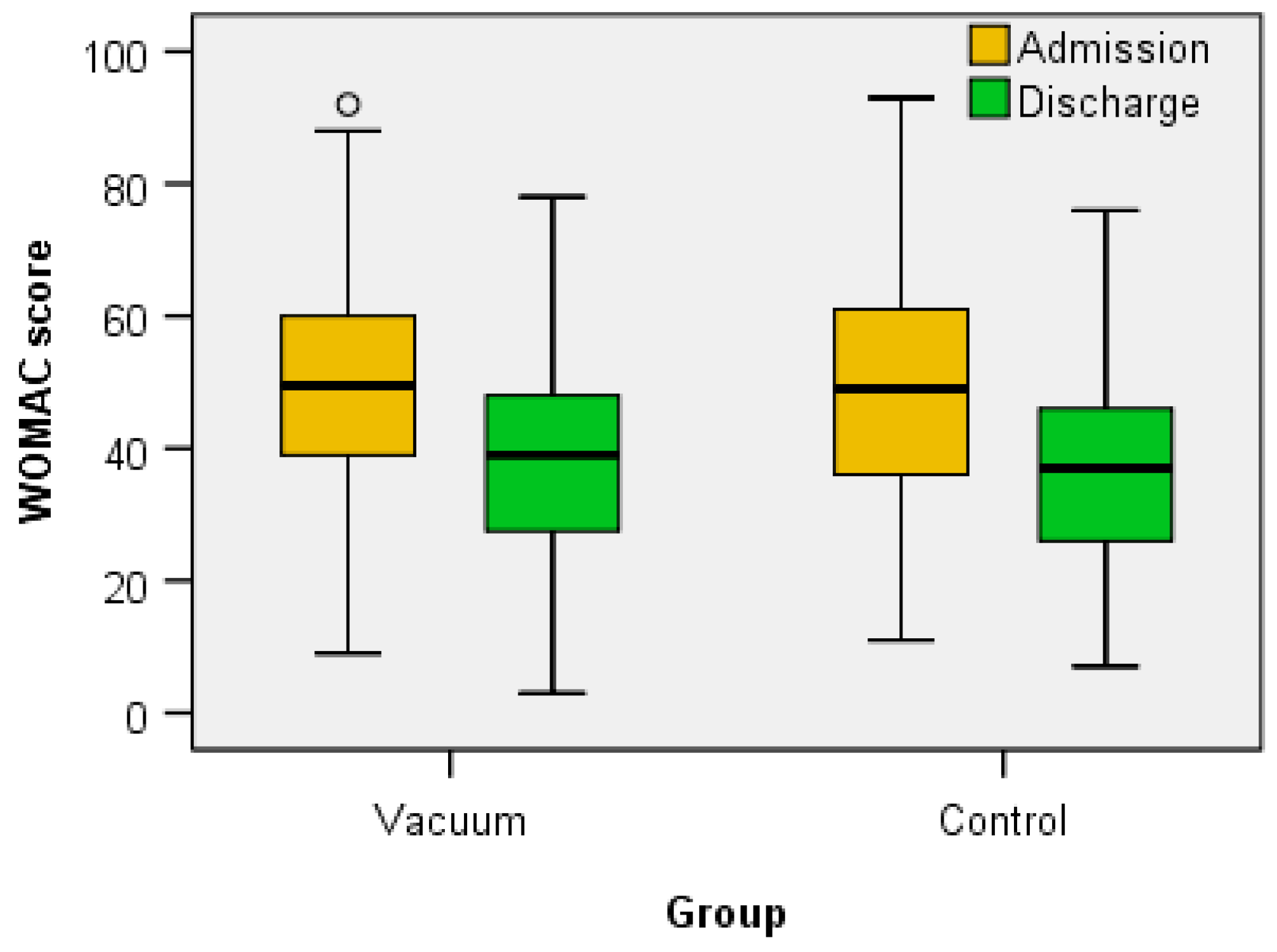
| WOMAC | |||||||||||
| Admission | 48.53 | 49.5 | 19.58 | 9–92 | 38.5–60 | 51.06 | 49 | 20.45 | 11–93 | 35.5–64.5 | 0.844 |
| Discharge | 37.28 | 39 | 19.18 | 3–78 | 27.25–48 | 37.03 | 37 | 16.4 | 7–76 | 25.5–47 | 0.718 |
| p admission/discharge | 0.000 | 0.000 | |||||||||
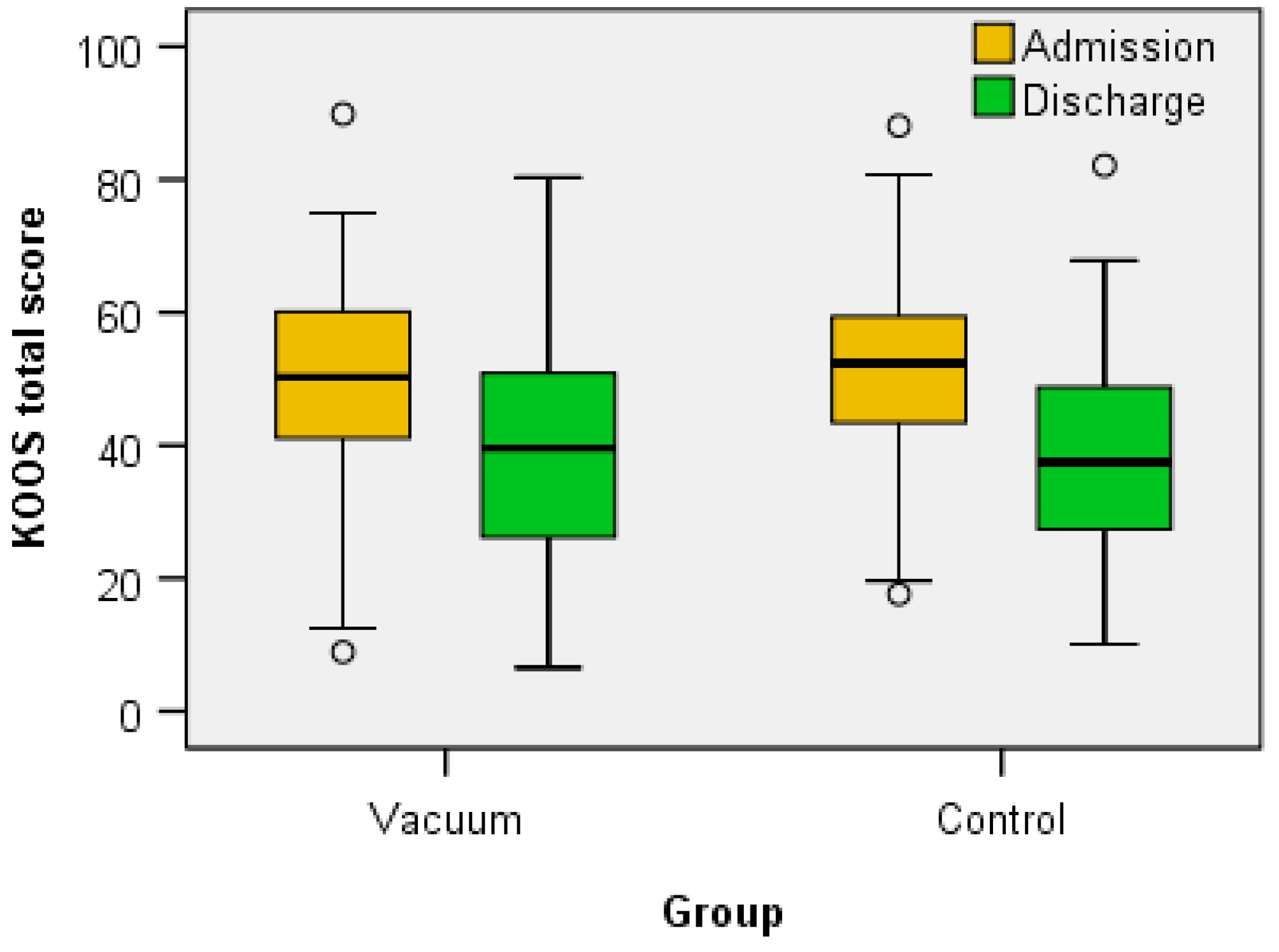
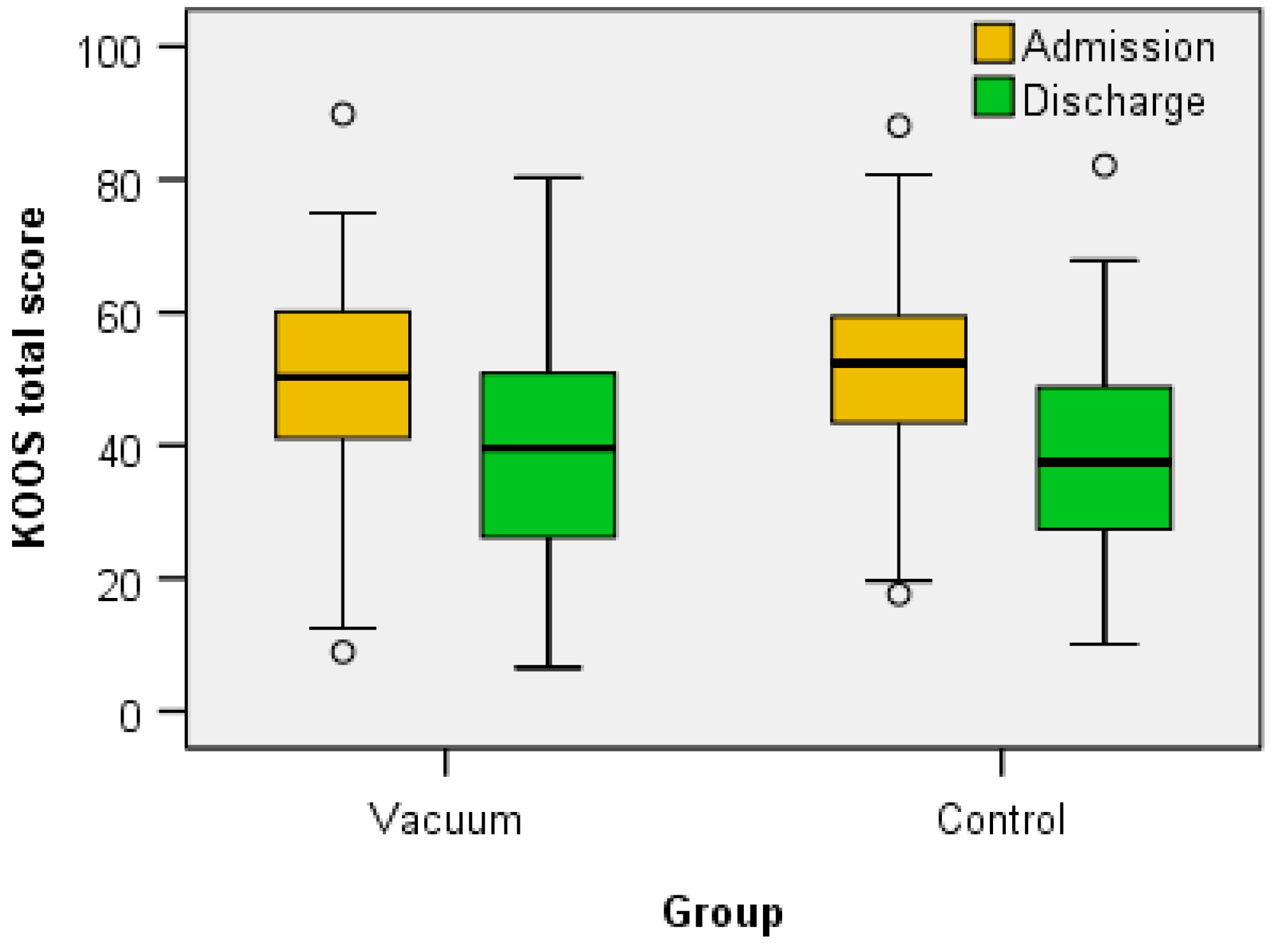
| KOOS total | |||||||||||
| Admission | 47.85 | 50.27 | 19.98 | 8.91–89.86 | 39.86–60.39 | 51.46 | 52.35 | 17.35 | 17.63–88.07 | 43.43–60.34 | 0.679 |
| Discharge | 37.63 | 39.56 | 18.54 | 6.54–80.33 | 24.38–51.01 | 38.6 | 37.47 | 15.66 | 10.10–82.11 | 27.06–49.08 | 0.990 |
| p admission/discharge | 0.000 | 0.000 | |||||||||
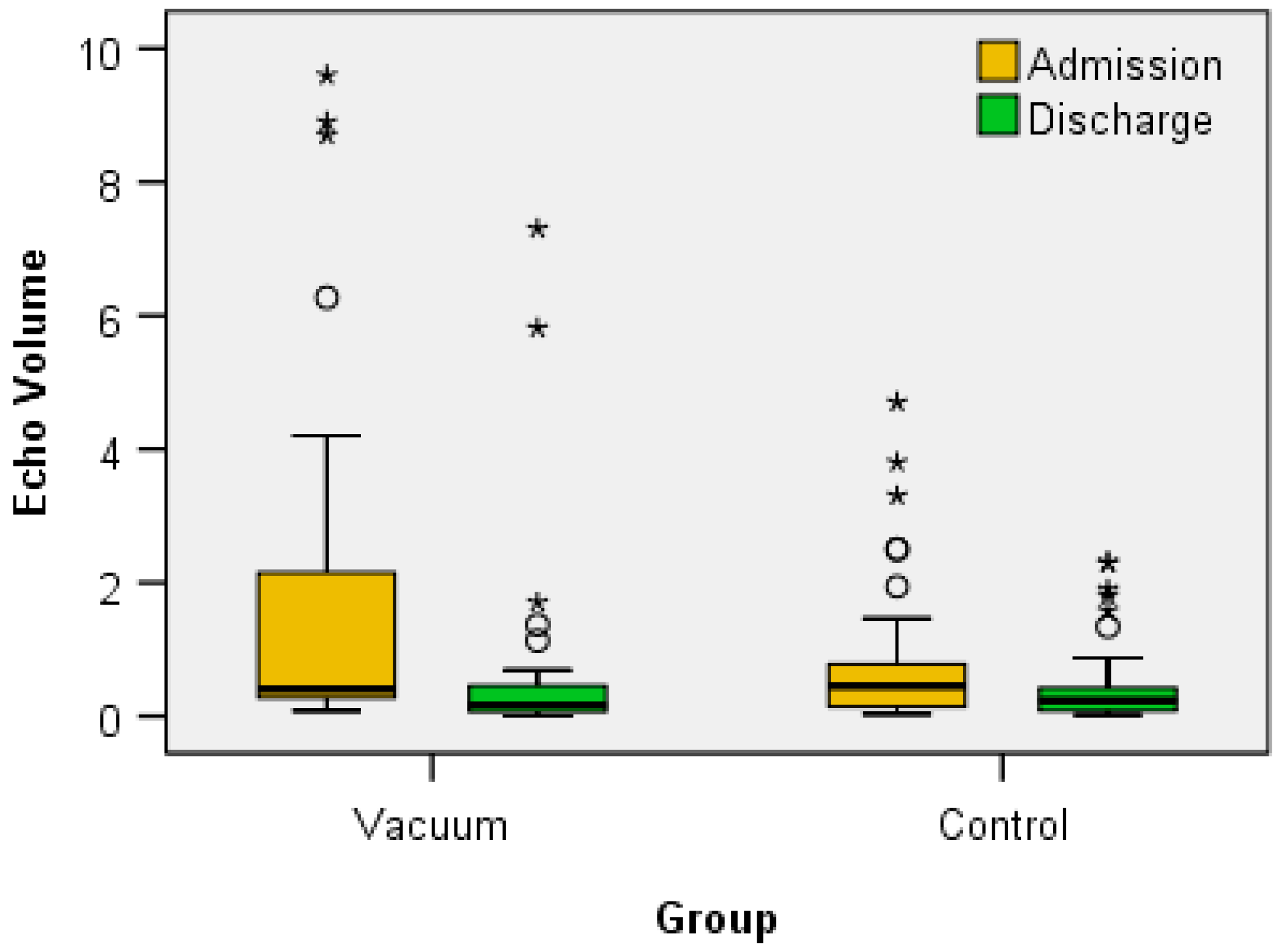
| Echo volume | |||||||||||
| Admission | 1.83 | 0.40 | 2.77 | 0.08–9.6 | 0.26–2.47 | 0.88 | 0.45 | 1.19 | 0.03–4.7 | 0.12–0.84 | 0.205 |
| Discharge | 0.70 | 0.17 | 1.6 | 0.00–7.3 | 0.07–0.48 | 0.51 | 0.23 | 0.69 | 0.02–2.3 | 0.08–0.55 | 0.599 |
| p admission/discharge | 0.000 | 0.003 | |||||||||
| Vacuum | Control | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Std Dev | Min–Max | Percentiles 25–75 | Mean | Median | Std Dev | Min–Max | Percentiles 25–75 | p | |
| KOOS symptoms | |||||||||||
| Admission | 7.36 | 7.44 | 3.28 | 1.78–15.47 | 4.76–9.81 | 8.14 | 8.92 | 3.54 | 2.38–14.8 | 4.46–10.71 | 0.357 |
| Discharge | 5.91 | 5.95 | 3.44 | 0.5–14.88 | 2.97–3.87 | 6.39 | 6.54 | 2.89 | 0.59–13.09 | 3.87–8.3 | 0.430 |
| p admission/discharge | 0.000 | 0.000 | |||||||||
| KOOS pain | |||||||||||
| Admission | 9.52 | 10.12 | 4.57 | 1.78–19.04 | 5.21–12.5 | 10.2 | 11.3 | 3.98 | 3.57–19.04 | 7.14–12.8 | 0.708 |
| Discharge | 7.19 | 8.33 | 3.85 | 0.00–16.07 | 3.72–9.96 | 7.53 | 7.14 | 3.66 | 0.59–13.09 | 5.3–10.11 | 0.849 |
| p admission/discharge | 0.000 | 0.000 | |||||||||
| KOOS ADL | |||||||||||
| Admission | 17.45 | 19.04 | 9.12 | 1.19–9.52 | 4.91–10.56 | 19.26 | 20.23 | 7.67 | 4.76–38.05 | 14.28–23.21 | 0.390 |
| Discharge | 13.24 | 13.99 | 7.74 | 0.00–11.9 | 3.13–8.77 | 14.13 | 13.69 | 6.92 | 2.38–35.71 | 9.52–18.45 | 0.769 |
| p admission/discharge | 0.000 | 0.000 | |||||||||
| KOOS sports | |||||||||||
| Admission | 7.68 | 8.03 | 3.25 | 1.19–11.9 | 4.91–10.56 | 7.89 | 8.92 | 2.77 | 1.78–11.9 | 6.25–9.22 | 0.911 |
| Discharge | 6.17 | 6.54 | 3.48 | 0.00–11.9 | 3.13–8.77 | 5.89 | 5.8 | 2.47 | 1.19–11.9 | 4.46–8.03 | 0.631 |
| p admission/discharge | 0.000 | 0.000 | |||||||||
| KOOS QoL | |||||||||||
| Admission | 5.76 | 5.65 | 2.22 | 1.19–11.9 | 4.91–10.56 | 5.9 | 5.95 | 1.62 | 2.3–8.92 | 5.35–7.14 | 0.900 |
| Discharge | 5.28 | 5.95 | 1.62 | 0.00–11.9 | 3.13–8.77 | 4.8 | 4.7 | 1.76 | 2.3–8.92 | 3.57–5.65 | 0.228 |
| p admission/discharge | 0.005 | 0.001 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ionescu, E.-V.; Stanciu, L.-E.; Bujduveanu, A.; Minea, M.; Oprea, D.; Petcu, A.; Iliescu, M.-G.; Ciortea, V.-M.; Popa, F.-L.; Gheorghe, E.; et al. Clinical Evidence Regarding the Dynamic of Baker Cyst Dimensions after Intermittent Vacuum Therapy as Rehabilitation Treatment in Patients with Knee Osteoarthritis. J. Clin. Med. 2023, 12, 6605. https://doi.org/10.3390/jcm12206605
Ionescu E-V, Stanciu L-E, Bujduveanu A, Minea M, Oprea D, Petcu A, Iliescu M-G, Ciortea V-M, Popa F-L, Gheorghe E, et al. Clinical Evidence Regarding the Dynamic of Baker Cyst Dimensions after Intermittent Vacuum Therapy as Rehabilitation Treatment in Patients with Knee Osteoarthritis. Journal of Clinical Medicine. 2023; 12(20):6605. https://doi.org/10.3390/jcm12206605
Chicago/Turabian StyleIonescu, Elena-Valentina, Liliana-Elena Stanciu, Andreea Bujduveanu, Mihaela Minea, Doinita Oprea, Adina Petcu, Madalina-Gabriela Iliescu, Viorela-Mihaela Ciortea, Florina-Ligia Popa, Emma Gheorghe, and et al. 2023. "Clinical Evidence Regarding the Dynamic of Baker Cyst Dimensions after Intermittent Vacuum Therapy as Rehabilitation Treatment in Patients with Knee Osteoarthritis" Journal of Clinical Medicine 12, no. 20: 6605. https://doi.org/10.3390/jcm12206605
APA StyleIonescu, E.-V., Stanciu, L.-E., Bujduveanu, A., Minea, M., Oprea, D., Petcu, A., Iliescu, M.-G., Ciortea, V.-M., Popa, F.-L., Gheorghe, E., Obada, B., & Oprea, C. (2023). Clinical Evidence Regarding the Dynamic of Baker Cyst Dimensions after Intermittent Vacuum Therapy as Rehabilitation Treatment in Patients with Knee Osteoarthritis. Journal of Clinical Medicine, 12(20), 6605. https://doi.org/10.3390/jcm12206605