
Clinical Benefit of First-Pass Recanalization Is Time-Dependent in Endovascular Treatment of Acute Ischemic Stroke
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
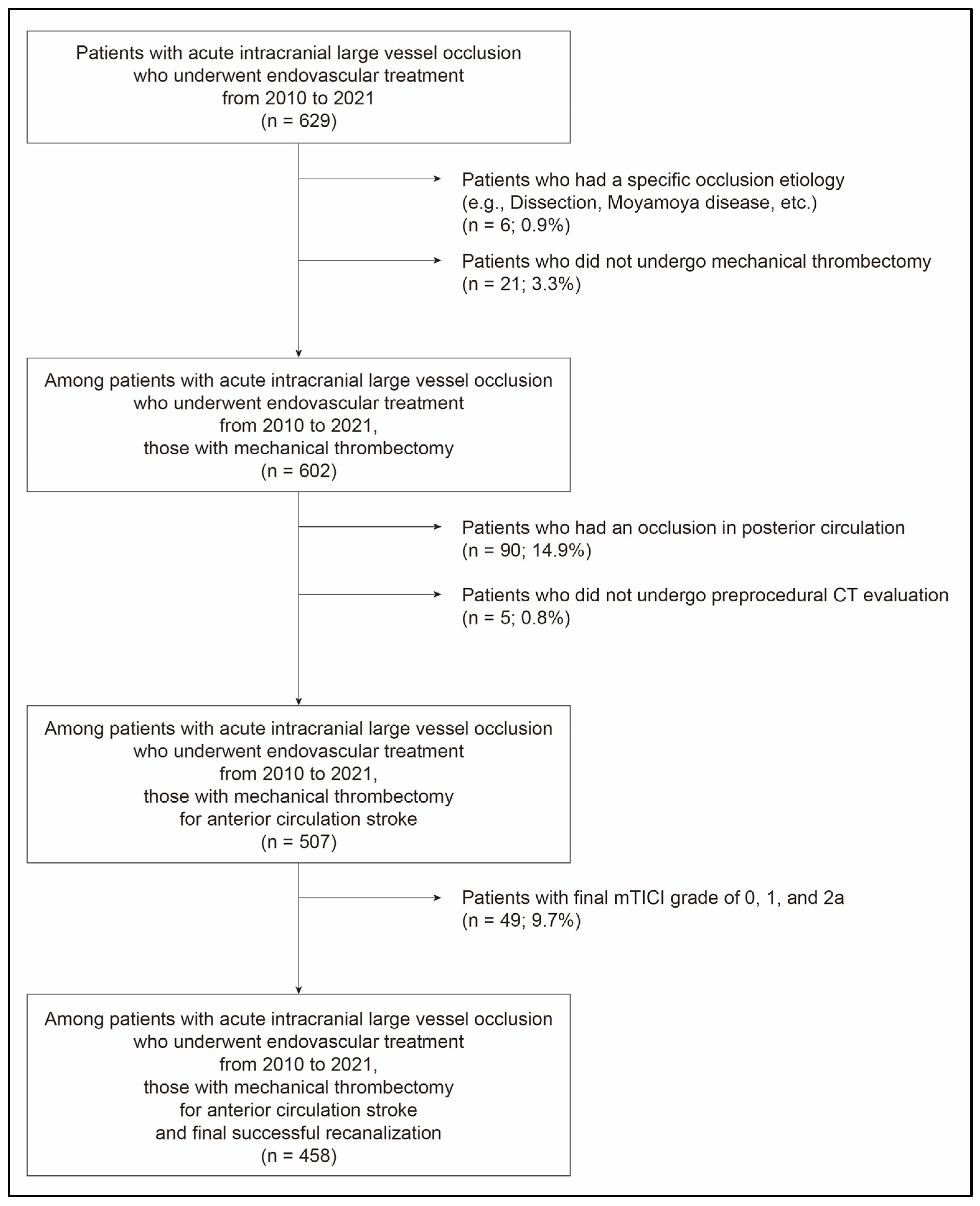
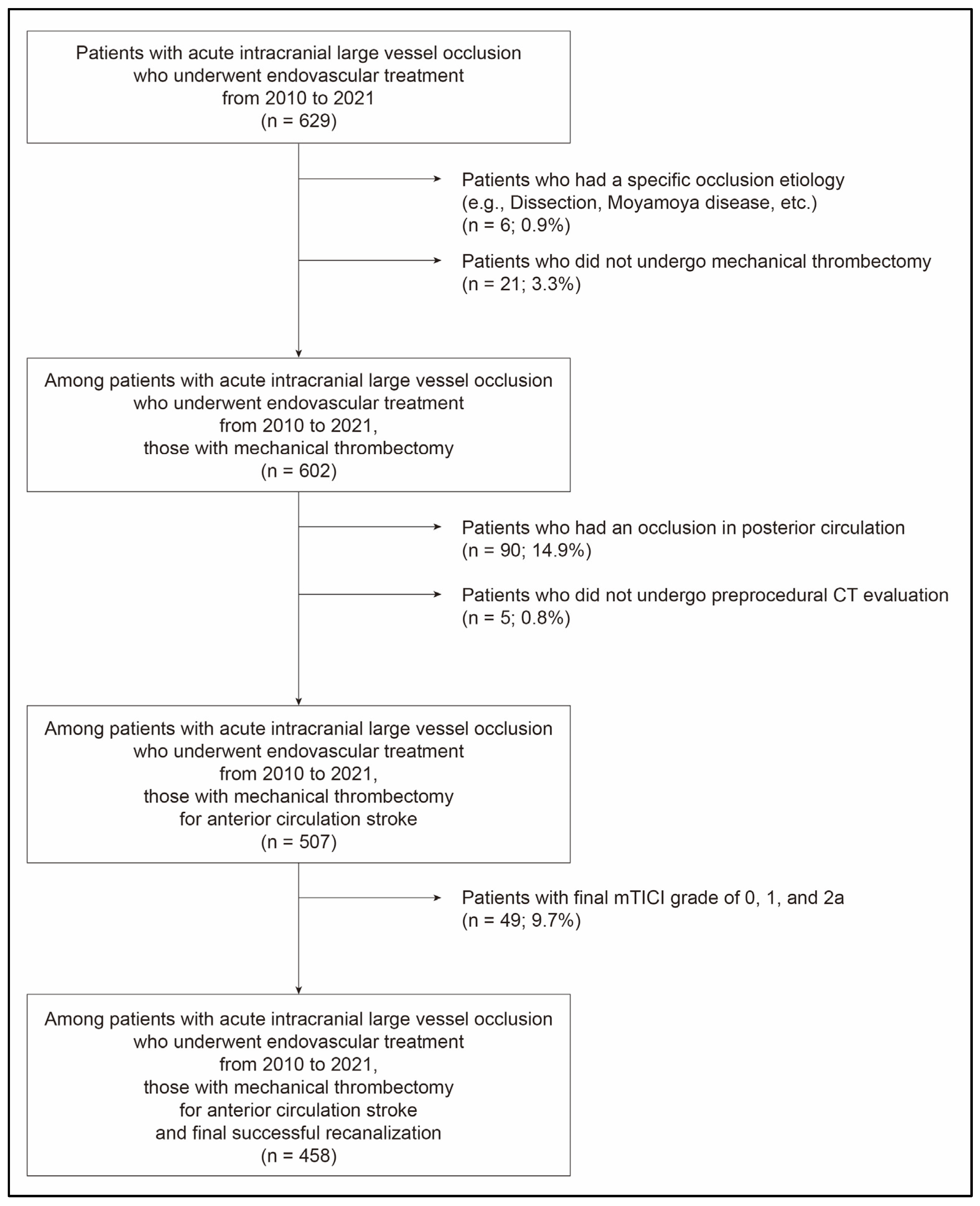
2.1. Study Population
2.2. Mechanical Thrombectomy Procedure
2.3. Study Variables and Outcomes
2.4. Statistical Analysis
3. Results
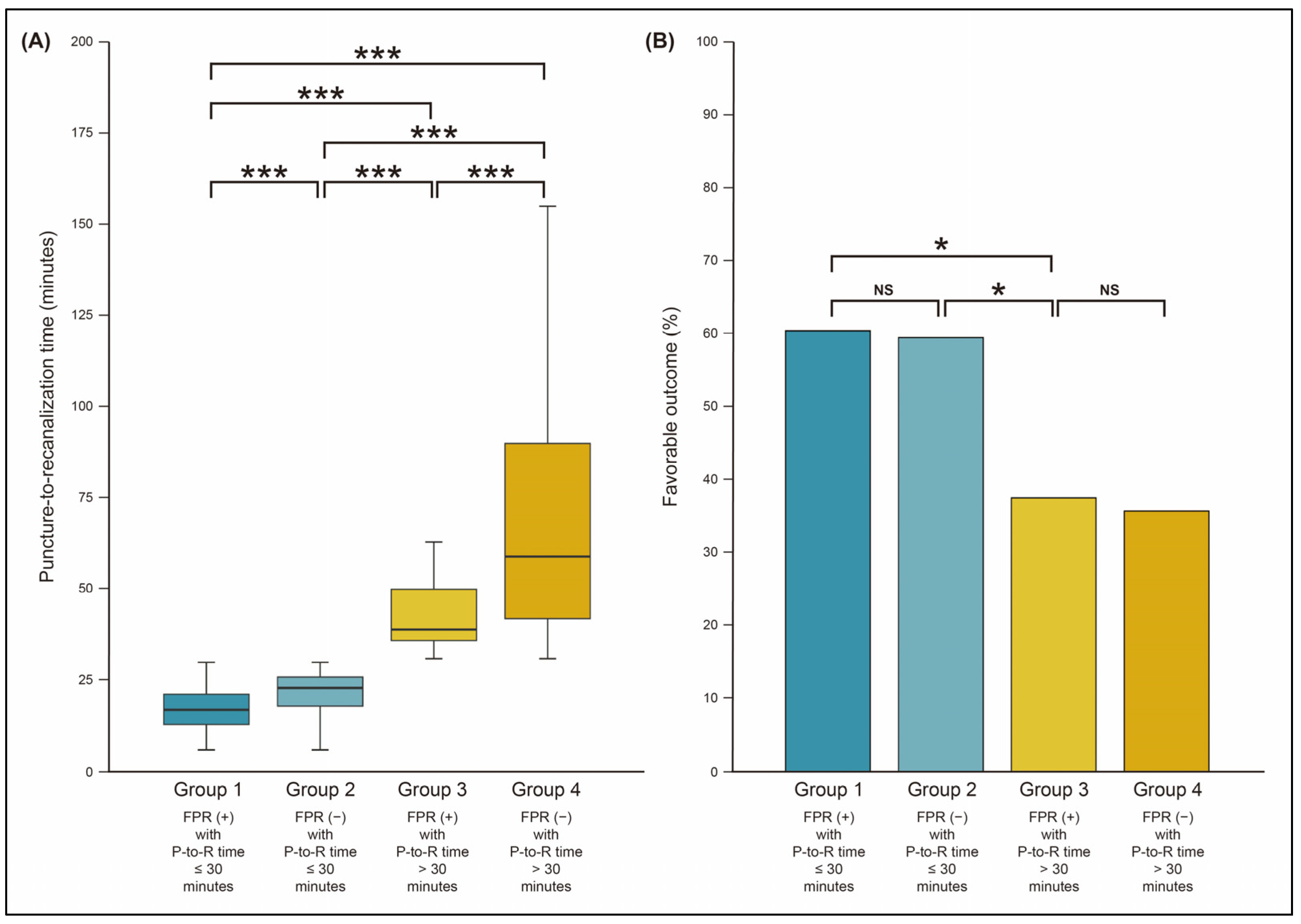
3.1. Recanalization Status by FPR and P-to-R Time
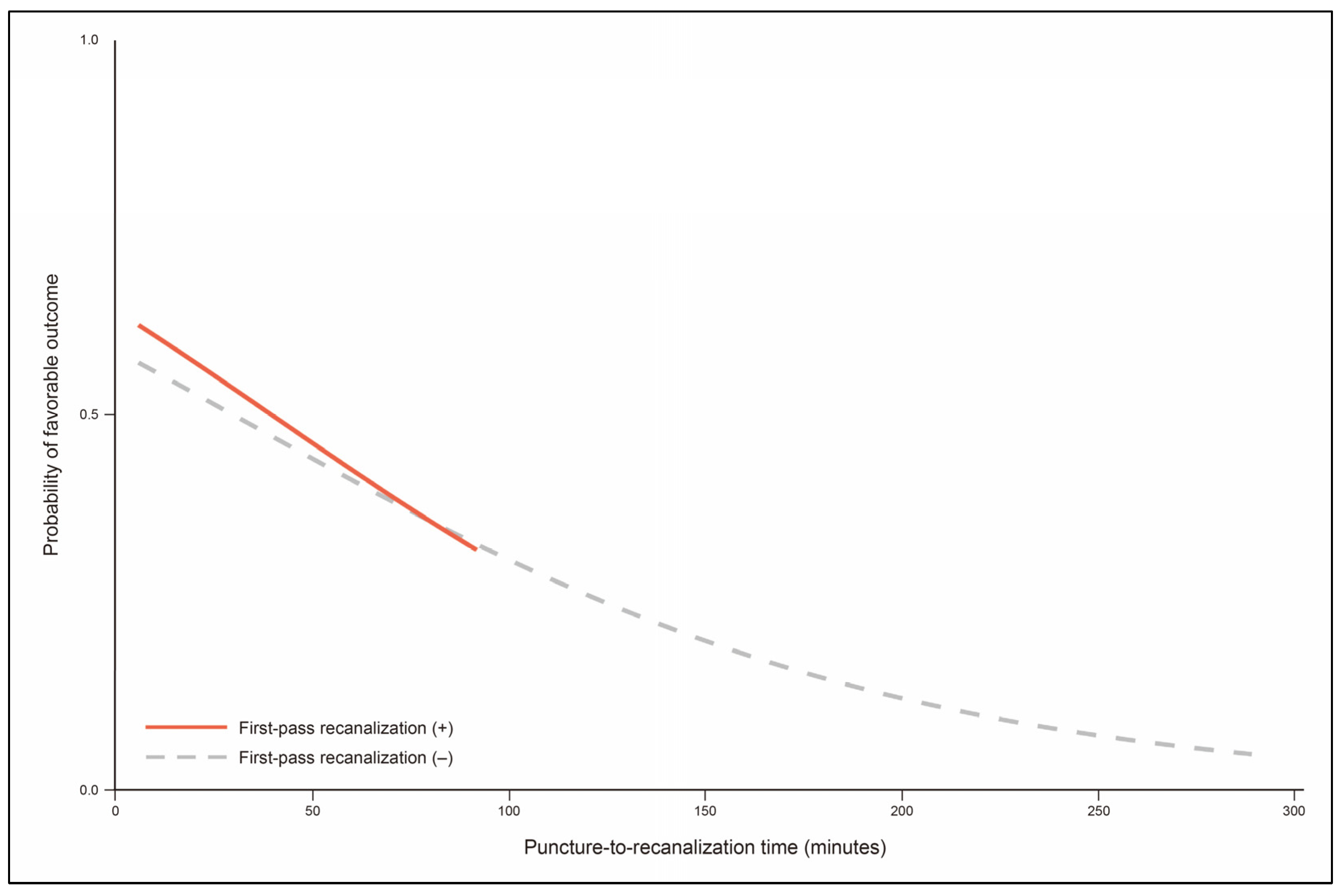
3.2. Endovascular and Functional Outcomes According to Recanalization Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef] [PubMed]
- Yoo, A.J.; Simonsen, C.Z.; Prabhakaran, S.; Chaudhry, Z.A.; Issa, M.A.; Fugate, J.E.; Linfante, I.; Liebeskind, D.S.; Khatri, P.; Jovin, T.G.; et al. Refining angiographic biomarkers of revascularization: Improving outcome prediction after intra-arterial therapy. Stroke 2013, 44, 2509–2512. [Google Scholar] [CrossRef] [PubMed]
- Kaesmacher, J.; Dobrocky, T.; Heldner, M.R.; Bellwald, S.; Mosimann, P.J.; Mordasini, P.; Bigi, S.; Arnold, M.; Gralla, J.; Fischer, U. Systematic review and meta-analysis on outcome differences among patients with TICI2b versus TICI3 reperfusions: Success revisited. J. Neurol. Neurosurg. Psychiatry 2018, 89, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Tung, E.L.; McTaggart, R.A.; Baird, G.L.; Yaghi, S.; Hemendinger, M.; Dibiasio, E.L.; Hidlay, D.T.; Tung, G.A.; Jayaraman, M.V. Rethinking Thrombolysis in Cerebral Infarction 2b: Which Thrombolysis in Cerebral Infarction Scales Best Define Near Complete Recanalization in the Modern Thrombectomy Era? Stroke 2017, 48, 2488–2493. [Google Scholar] [CrossRef]
- Goyal, M.; Fargen, K.M.; Turk, A.S.; Mocco, J.; Liebeskind, D.S.; Frei, D.; Demchuk, A.M. 2C or not 2C: Defining an improved revascularization grading scale and the need for standardization of angiography outcomes in stroke trials. J. Neurointerv. Surg. 2014, 6, 83–86. [Google Scholar] [CrossRef]
- LeCouffe, N.E.; Kappelhof, M.; Treurniet, K.M.; Lingsma, H.F.; Zhang, G.; van den Wijngaard, I.R.; van Es, A.; Emmer, B.J.; Majoie, C.; Roos, Y.; et al. 2B, 2C, or 3: What Should Be the Angiographic Target for Endovascular Treatment in Ischemic Stroke? Stroke 2020, 51, 1790–1796. [Google Scholar] [CrossRef]
- Baek, J.H.; Kim, B.M.; Heo, J.H.; Nam, H.S.; Kim, Y.D.; Park, H.; Bang, O.Y.; Yoo, J.; Kim, D.J.; Jeon, P.; et al. Number of Stent Retriever Passes Associated with Futile Recanalization in Acute Stroke. Stroke 2018, 49, 2088–2095. [Google Scholar] [CrossRef]
- Yoo, A.J.; Soomro, J.; Andersson, T.; Saver, J.L.; Ribo, M.; Bozorgchami, H.; Dabus, G.; Liebeskind, D.S.; Jadhav, A.; Mattle, H.; et al. Benchmarking the Extent and Speed of Reperfusion: First Pass TICI 2c-3 Is a Preferred Endovascular Reperfusion Endpoint. Front. Neurol. 2021, 12, 669934. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Castonguay, A.C.; Linfante, I.; Gupta, R.; Martin, C.O.; Holloway, W.E.; Mueller-Kronast, N.; English, J.D.; Dabus, G.; Malisch, T.W.; et al. First Pass Effect: A New Measure for Stroke Thrombectomy Devices. Stroke 2018, 49, 660–666. [Google Scholar] [CrossRef]
- Abbasi, M.; Liu, Y.; Fitzgerald, S.; Mereuta, O.M.; Arturo Larco, J.L.; Rizvi, A.; Kadirvel, R.; Savastano, L.; Brinjikji, W.; Kallmes, D.F. Systematic review and meta-analysis of current rates of first pass effect by thrombectomy technique and associations with clinical outcomes. J. Neurointerv. Surg. 2021, 13, 212–216. [Google Scholar] [CrossRef]
- Jadhav, A.P.; Desai, S.M.; Zaidat, O.O.; Nogueira, R.G.; Jovin, T.G.; Haussen, D.C.; Mueller-Kronast, N.; Liebeskind, D.S. First Pass Effect with Neurothrombectomy for Acute Ischemic Stroke: Analysis of the Systematic Evaluation of Patients Treated with Stroke Devices for Acute Ischemic Stroke Registry. Stroke 2022, 53, e30–e32. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.M. Causes and Solutions of Endovascular Treatment Failure. J. Stroke 2017, 19, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.H.; Hwang, Y.H. Frontline Contact Aspiration Treatment for Emergent Large Vessel Occlusion: A Review Focused on Practical Techniques. J. Stroke 2019, 21, 10–22. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.M.; Baek, J.H.; Heo, J.H.; Nam, H.S.; Kim, Y.D.; Yoo, J.; Kim, D.J.; Jeon, P.; Baik, S.K.; Suh, S.H.; et al. Collateral status affects the onset-to-reperfusion time window for good outcome. J. Neurol. Neurosurg. Psychiatry 2018, 89, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, A.P.; Desai, S.M.; Budzik, R.F.; Gupta, R.; Baxter, B.; English, J.D.; Bartolini, B.M.; Krajina, A.; Haussen, D.C.; Nogueira, R.G.; et al. First pass effect in patients with large vessel occlusion strokes undergoing neurothrombectomy: Insights from the Trevo Retriever Registry. J. Neurointerv. Surg. 2021, 13, 619–622. [Google Scholar] [CrossRef]
- Bruggeman, A.A.E.; Kappelhof, M.; den Hartog, S.J.; Burke, J.F.; Berkhemer, O.A.; van Es, A.; van Zwam, W.H.; Dippel, D.W.J.; Coutinho, J.M.; Marquering, H.A.; et al. Successful reperfusion in relation to the number of passes: Comparing outcomes of first pass expanded Treatment in Cerebral Ischemia (eTICI) 2B with multiple-pass eTICI 3. J. Neurointerv. Surg. 2022, 15, 120–126. [Google Scholar] [CrossRef]
- den Hartog, S.J.; Zaidat, O.; Roozenbeek, B.; van Es, A.; Bruggeman, A.A.E.; Emmer, B.J.; Majoie, C.; van Zwam, W.H.; van den Wijngaard, I.R.; van Doormaal, P.J.; et al. Effect of First-Pass Reperfusion on Outcome After Endovascular Treatment for Ischemic Stroke. J. Am. Heart Assoc. 2021, 10, e019988. [Google Scholar] [CrossRef]
- Ben Hassen, W.; Tordjman, M.; Boulouis, G.; Bretzner, M.; Bricout, N.; Legrand, L.; Benzakoun, J.; Edjlali, M.; Seners, P.; Cordonnier, C.; et al. Benefit of first-pass complete reperfusion in thrombectomy is mediated by limited infarct growth. Eur. J. Neurol. 2021, 28, 124–131. [Google Scholar] [CrossRef]
- Mokin, M.; Primiani, C.T.; Castonguay, A.C.; Nogueira, R.G.; Haussen, D.C.; English, J.D.; Satti, S.R.; Chen, J.; Farid, H.; Borders, C.; et al. First Pass Effect in Patients Treated with the Trevo Stent-Retriever: A TRACK Registry Study Analysis. Front. Neurol. 2020, 11, 83. [Google Scholar] [CrossRef]
- Garcia-Tornel, A.; Requena, M.; Rubiera, M.; Muchada, M.; Pagola, J.; Rodriguez-Luna, D.; Deck, M.; Juega, J.; Rodriguez-Villatoro, N.; Boned, S.; et al. When to Stop. Stroke 2019, 50, 1781–1788. [Google Scholar] [CrossRef] [PubMed]
- Nikoubashman, O.; Dekeyzer, S.; Riabikin, A.; Keulers, A.; Reich, A.; Mpotsaris, A.; Wiesmann, M. True First-Pass Effect. Stroke 2019, 50, 2140–2146. [Google Scholar] [CrossRef] [PubMed]
- Jindal, G.; Carvalho, H.P.; Wessell, A.; Le, E.; Naragum, V.; Miller, T.R.; Wozniak, M.; Shivashankar, R.; Cronin, C.A.; Schrier, C.; et al. Beyond the first pass: Revascularization remains critical in stroke thrombectomy. J. Neurointerv. Surg. 2019, 11, 1095–1099. [Google Scholar] [CrossRef]
- Arai, D.; Ishii, A.; Chihara, H.; Ikeda, H.; Miyamoto, S. Histological examination of vascular damage caused by stent retriever thrombectomy devices. J. Neurointerv. Surg. 2016, 8, 992–995. [Google Scholar] [CrossRef] [PubMed]
- Chueh, J.Y.; Puri, A.S.; Wakhloo, A.K.; Gounis, M.J. Risk of distal embolization with stent retriever thrombectomy and ADAPT. J. Neurointerv. Surg. 2016, 8, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Ben Hassen, W.; Touloupas, C.; Benzakoun, J.; Boulouis, G.; Bretzner, M.; Bricout, N.; Legrand, L.; Rodriguez, C.; Le Berre, A.; Seners, P.; et al. Impact of Repeated Clot Retrieval Attempts on Infarct Growth and Outcome After Ischemic Stroke. Neurology 2021, 97, e444–e453. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| n = 458 | |
| Demographics and stroke risk factors | |
| Age (years) | 69.7 (±12.6) |
| Men | 226 (49.3) |
| Hypertension | 312 (68.1) |
| Diabetes | 135 (29.5) |
| Dyslipidemia | 104 (22.7) |
| Current smoking | 70 (15.3) |
| Coronary artery occlusive disease | 97 (21.2) |
| Atrial fibrillation | 265 (57.9) |
| Clinical conditions | |
| Initial NIHSS score | 15.0 [11.0; 19.0] |
| Intravenous tPA administration | 176 (38.4) |
| Location of occlusion | |
| Internal carotid artery | 173 (37.8) |
| Middle cerebral artery | 285 (62.2) |
| ASPECTS | 8.0 [6.0; 9.0] |
| Good leptomeningeal collaterals | 291 (63.5) |
| O-to-P time (minutes) | 270.0 [160.0; 559.0] |
| Use of balloon guide catheter | 377 (82.3) |
| Endovascular outcomes | |
| Time to successful recanalization | |
| P-to-R time (minutes) | 37.0 [22.2; 63.0] |
| O-to-R time (minutes) | 341.0 [208.0; 599.0] |
| First-pass recanalization | 136 (29.7) |
| Number of passes of thrombectomy device | 2.3 (±1.5) |
| Favorable outcome | 208 (45.4) |
| First-Pass Recanalization (+) (n = 136) | First-Pass Recanalization (–) (n = 322) | Total (n = 458) | |
|---|---|---|---|
| P-to-R time ≤ 30 min | 96 (21.0) | 84 (18.3) | 180 (39.3) |
| P-to-R time > 30 min | 40 (8.7) | 238 (52.0) | 278 (60.7) |
| Group 1 FPR (+) with P-to-R ≤ 30 min (n = 96) | Group 2 FPR (−) with P-to-R ≤ 30 min (n = 84) | Group 3 FPR (+) with P-to-R > 30 min (n = 40) | Group 4 FPR (−) with P-to-R > 30 min (n = 238) | p-Value * | |
|---|---|---|---|---|---|
| Demographics and stroke risk factors | |||||
| Age (years) | 70.7 (±13.9) | 65.7 (±12.8) | 73.7 (±9.42) | 70.0 (±12.2) | 0.535 |
| Men | 46 (47.9) | 40 (47.6) | 20 (50.0) | 120 (50.4) | 0.611 |
| Hypertension | 68 (70.8) | 52 (61.9) | 30 (75.0) | 162 (68.1) | 0.993 |
| Diabetes | 33 (34.4) | 20 (23.8) | 18 (45.0) | 64 (26.9) | 0.372 |
| Dyslipidemia | 27 (28.1) | 23 (27.4) | 10 (25.0) | 44 (18.5) | 0.028 |
| Current smoking | 8 (8.3) | 16 (19.0) | 5 (12.5) | 41 (17.2) | 0.121 |
| Coronary artery occlusive disease | 17 (17.7) | 12 (14.3) | 14 (35.0) | 54 (22.7) | 0.139 |
| Atrial fibrillation | 64 (66.7) | 49 (58.3) | 20 (50.0) | 132 (55.5) | 0.079 |
| Clinical conditions | |||||
| Initial NIHSS score | 15.0 [12.0; 19.0] | 14.0 [9.8; 18.2] | 16.0 [11.0; 19.0] | 16.0 [10.2; 19.0] | 0.308 |
| Intravenous tPA administration | 34 (35.4) | 38 (45.2) | 14 (35.0) | 90 (37.8) | 0.914 |
| Location of occlusion | 0.028 | ||||
| Internal carotid artery | 30 (31.2) | 27 (32.1) | 15 (37.5) | 101 (42.4) | |
| Middle cerebral artery | 66 (68.8) | 57 (67.9) | 25 (62.5) | 137 (57.6) | |
| ASPECTS | 8.0 [6.0; 9.3] | 8.0 [7.0; 9.0] | 8.0 [7.0; 10.0] | 8.0 [6.0; 9.0] | 0.199 |
| Good leptomeningeal collaterals | 60 (62.5) | 53 (63.1) | 22 (55.0) | 156 (65.5) | 0.576 |
| O-to-P time (minutes) | 226.0 [144.0; 562.0] | 322.0 [155.0; 526.0] | 292.0 [178.0; 508.0] | 266.0 [168.0; 613.0] | 0.225 |
| Use of balloon guide catheter | 90 (93.8) | 81 (96.4) | 26 (65.0) | 180 (75.6) | <0.001 |
| Endovascular outcomes | |||||
| Time to recanalization | |||||
| P-to-R time (minutes) | 17.0 [13.0; 21.2] | 23.0 [18.0; 26.0] | 39.0 [36.0; 50.0] | 60.0 [42.0; 94.8] | <0.001 |
| O-to-R time (minutes) | 245.0 [162.0; 576.0] | 338.0 [174.0; 550.0] | 342.0 [224.0; 546.0] | 362.0 [254.0; 663.0] | <0.001 |
| Number of passes of thrombectomy device | 1.0 (± 0.0) | 2.1 (± 0.84) | 1.0 (± 0.0) | 3.2 (± 1.5) | <0.001 |
| Favorable outcome | 58 (60.4) | 50 (59.5) | 15 (37.5) | 85 (35.7) | <0.001 |
| Favorable Outcome (–) (n = 250) | Favorable Outcome (+) (n = 208) | p-Value | |
|---|---|---|---|
| Demographics and stroke risk factors | |||
| Age (years) | 72.4 (±11.9) | 66.4 (±12.7) | <0.001 |
| Men | 111 (44.4) | 115 (55.3) | 0.020 |
| Hypertension | 177 (70.8) | 135 (64.9) | 0.178 |
| Diabetes | 80 (32.0) | 55 (26.4) | 0.194 |
| Dyslipidemia | 47 (18.8) | 57 (27.4) | 0.029 |
| Current smoking | 32 (12.8) | 38 (18.3) | 0.105 |
| Coronary artery occlusive disease | 42 (16.8) | 55 (26.4) | 0.012 |
| Atrial fibrillation | 154 (61.6) | 111 (53.4) | 0.076 |
| Clinical conditions | |||
| Initial NIHSS score | 17.0 [14.0; 20.0] | 13.0 [9.0; 16.0] | <0.001 |
| Intravenous tPA administration | 84 (33.6) | 92 (44.2) | 0.020 |
| Location of occlusion | 0.005 | ||
| Internal carotid artery | 109 (43.6) | 64 (30.8) | |
| Middle cerebral artery | 141 (56.4) | 144 (69.2) | |
| ASPECTS | 7.0 [5.0; 9.0] | 9.0 [8.0; 10.0] | <0.001 |
| Good leptomeningeal collaterals | 132 (52.8) | 159 (76.4) | <0.001 |
| O-to-P time (minutes) | 272.0 [159.0; 645.0] | 266.0 [164.0; 508.0] | 0.432 |
| Use of balloon guide catheter | 195 (78.0) | 182 (87.5) | 0.008 |
| Endovascular outcomes | |||
| Time to successful recanalization | |||
| P-to-R time (minutes) | 42.5 [25.2; 74.0] | 29.0 [19.0; 49.2] | <0.001 |
| O-to-R time (minutes) | 354.0 [222.0; 670.0] | 315.0 [195.0; 547.0] | 0.041 |
| FPR | 63 (25.2) | 73 (35.1) | 0.021 |
| Number of passes of thrombectomy device | 2.6 (± 1.6) | 2.1 (±1.3) | <0.001 |
| Recanalization status | <0.001 | ||
| Group 1: FPR (+) with P-to-R time ≤ 30 min | 38 (15.2) | 58 (27.9) | |
| Group 2: FPR (–) with P-to-R time ≤ 30 min | 34 (13.6) | 50 (24.0) | |
| Group 3: FPR (+) with P-to-R time > 30 min | 25 (10.0) | 15 (7.2) | |
| Group 4: FPR (–) with P-to-R time > 30 min | 153 (61.2) | 85 (40.9) |
| aOR (95% CI) | p-Value | |
|---|---|---|
| Age (per year) | 0.96 (0.94–0.98) | <0.001 *** |
| Men | 1.35 (0.85–2.16) | 0.202 |
| Hypertension | 0.92 (0.55–1.54) | 0.740 |
| Dyslipidemia | 1.31 (0.77–2.23) | 0.313 |
| Coronary artery occlusive disease | 3.10 (1.75–5.48) | <0.001 *** |
| Atrial fibrillation | 1.31 (0.80–2.14) | 0.287 |
| Initial NIHSS score | 0.90 (0.86–0.94) | <0.001 *** |
| Intravenous tPA administration | 1.90 (1.19–3.05) | 0.007 ** |
| Occlusion of middle cerebral artery | 1.22 (0.76–1.97) | 0.413 |
| ASPECTS | 1.31 (1.16–1.48) | <0.001 *** |
| Good leptomeningeal collaterals | 2.07 (1.22–3.49) | 0.007 ** |
| Use of balloon guide catheter | 1.98 (1.04–3.75) | 0.037 * |
| Recanalization status | ||
| Group 1: FPR (+) with P-to-R time ≤ 30 min | Reference | |
| Group 2: FPR (–) with P-to-R time ≤ 30 min | 0.57 (0.28–1.17) | 0.123 |
| Group 3: FPR (+) with P-to-R time > 30 min | 0.30 (0.12–0.76) | 0.011 * |
| Group 4: FPR (–) with P-to-R time > 30 min | 0.25 (0.14–0.48) | <0.001 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, J.-H.; Heo, J.H.; Nam, H.S.; Kim, B.M.; Kim, D.J.; Kim, Y.D. Clinical Benefit of First-Pass Recanalization Is Time-Dependent in Endovascular Treatment of Acute Ischemic Stroke. J. Clin. Med. 2023, 12, 6596. https://doi.org/10.3390/jcm12206596
Baek J-H, Heo JH, Nam HS, Kim BM, Kim DJ, Kim YD. Clinical Benefit of First-Pass Recanalization Is Time-Dependent in Endovascular Treatment of Acute Ischemic Stroke. Journal of Clinical Medicine. 2023; 12(20):6596. https://doi.org/10.3390/jcm12206596
Chicago/Turabian StyleBaek, Jang-Hyun, Ji Hoe Heo, Hyo Suk Nam, Byung Moon Kim, Dong Joon Kim, and Young Dae Kim. 2023. "Clinical Benefit of First-Pass Recanalization Is Time-Dependent in Endovascular Treatment of Acute Ischemic Stroke" Journal of Clinical Medicine 12, no. 20: 6596. https://doi.org/10.3390/jcm12206596
APA StyleBaek, J.-H., Heo, J. H., Nam, H. S., Kim, B. M., Kim, D. J., & Kim, Y. D. (2023). Clinical Benefit of First-Pass Recanalization Is Time-Dependent in Endovascular Treatment of Acute Ischemic Stroke. Journal of Clinical Medicine, 12(20), 6596. https://doi.org/10.3390/jcm12206596