
How to Estimate the Probability of Tolerance Long-Term in Liver Transplant Recipients

 ,
,  , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Patients and Methods
3. Statistical Analysis
4. Results
4.1. Levels of Tolerance Definition Accuracy
4.2. Parameters Associated with Tolerance
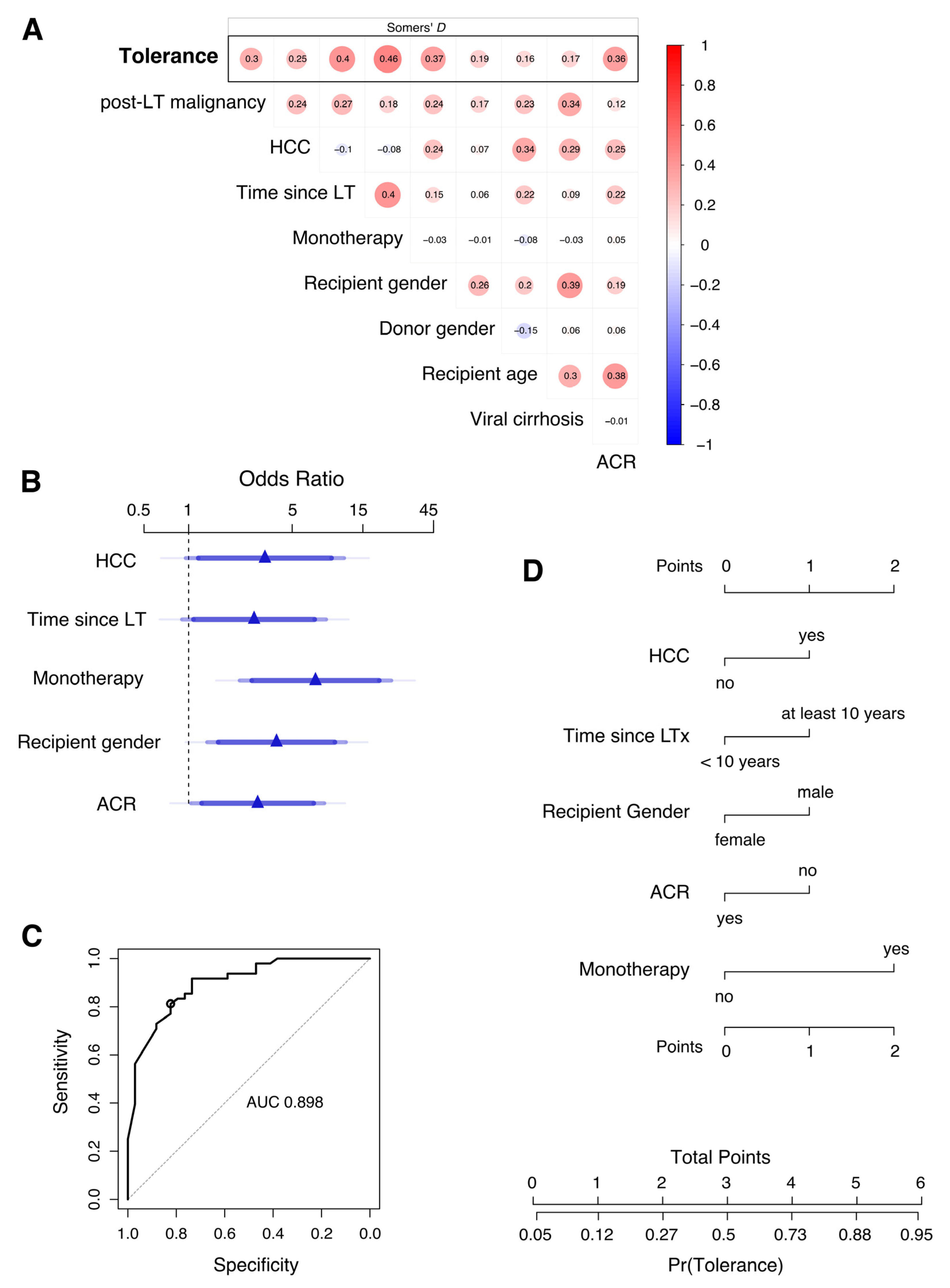
4.3. Multivariable Analysis and Clinical Prediction of Tolerant Patients
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACR | acute cellular rejection |
| AUC | area under the curve |
| CNI | calcineurin inhibitor |
| ESLD | end stage liver disease |
| EVL | everolimus |
| IS | immunosuppression |
| HBV | hepatitis B virus |
| HCC | hepatocellular carcinoma |
| HCV | hepatitis C virus |
| LT | liver transplantation |
| MMF | mycophenolate mofetil |
| Re-LT | retransplantation |
References
- Adam, R.; Karam, V.; Cailliez, V.; Grady, J.G.O.; Mirza, D.; Cherqui, D.; Klempnauer, J.; Salizzoni, M.; Pratschke, J.; Jamieson, N.; et al. 2018 Annual Report of the European Liver Transplant Registry (ELTR)-50-year evolution of liver transplantation. Transpl. Int. 2018, 31, 1293–1317. [Google Scholar] [CrossRef]
- Charlton, M.R. Roadmap for improving patient and graft survival in the next 10 years. Liver Transplant. 2016, 22, 71–78. [Google Scholar] [CrossRef]
- Starzl, T.E. Cell migration and chimerism—A unifying concept in transplantation—With particular reference to HLA matching and tolerance induction. Transplant. Proc. 1993, 25, 8–12. [Google Scholar] [PubMed]
- Sánchez–Fueyo, A.; Strom, T.B. Immunologic Basis of Graft Rejection and Tolerance Following Transplantation of Liver or Other Solid Organs. Gastroenterology 2011, 140, 51–64.e2. [Google Scholar] [CrossRef]
- Jadlowiec, C.C.; Morgan, P.E.; Nehra, A.K.; Hathcock, M.A.; Kremers, W.K.; Heimbach, J.K.; Wiesner, R.H.; Taner, T. Not All Cellular Rejections Are the Same: Differences in Early and Late Hepatic Allograft Rejection. Liver Transplant. 2019, 25, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Levitsky, J.; Goldberg, D.; Smith, A.R.; Mansfield, S.A.; Gillespie, B.W.; Merion, R.M.; Lok, A.S.; Levy, G.; Kulik, L.; Abecassis, M.; et al. Acute Rejection Increases Risk of Graft Failure and Death in Recent Liver Transplant Recipients. Clin. Gastroenterol. Hepatol. 2017, 15, 584–593.e582. [Google Scholar] [CrossRef] [PubMed]
- Benítez, C.; Londoño, M.-C.; Miquel, R.; Manzia, T.-M.; Abraldes, J.G.; Lozano, J.-J.; Martínez-Llordella, M.; López, M.; Angelico, R.; Bohne, F.; et al. Prospective multicenter clinical trial of immunosuppressive drug withdrawal in stable adult liver transplant recipients. Hepatology 2013, 58, 1824–1835. [Google Scholar] [CrossRef]
- Haagsma, E.B.; Hagens, V.E.; Schaapveld, M.; van den Berg, A.P.; de Vries, E.G.; Klompmaker, I.J.; Slooff, M.J.; Jansen, P.L. Increased cancer risk after liver transplantation: A population-based study. J. Hepatol. 2001, 34, 84–91. [Google Scholar] [CrossRef]
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F., Jr.; Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Wolfe, R.A.; Goodrich, N.P.; Bayakly, A.R.; Clarke, C.A.; et al. Spectrum of Cancer Risk Among US Solid Organ Transplant Recipients. JAMA 2011, 306, 1891–1901. [Google Scholar] [CrossRef]
- Åberg, F.; Pukkala, E.; Höckerstedt, K.; Sankila, R.; Isoniemi, H. Risk of malignant neoplasms after liver transplantation: A population-based study. Liver Transplant. 2008, 14, 1428–1436. [Google Scholar] [CrossRef]
- Pesthy, S.; Wegener, E.; Saidy, R.R.O.; Timmermann, L.; Uluk, D.; Aydin, M.; Dziodzio, T.; Schoening, W.; Lurje, G.; Öllinger, R.; et al. Reducing Immunosuppression in Patients with De Novo Lung Carcinoma after Liver Transplantation Could Significantly Prolong Survival. Cancers 2022, 14, 2748. [Google Scholar] [CrossRef] [PubMed]
- Saidy, R.R.O.; Postel, M.P.; Pflüger, M.J.; Schoening, W.; Öllinger, R.; Gül-Klein, S.; Schmelzle, M.; Tacke, F.; Pratschke, J.; Eurich, D. Minimization of Immunosuppressive Therapy Is Associated with Improved Survival of Liver Transplant Patients with Recurrent Hepatocellular Carcinoma. Cancers 2021, 13, 1617. [Google Scholar] [CrossRef] [PubMed]
- Timmermann, L.; Globke, B.; Lurje, G.; Schmelzle, M.; Schöning, W.; Öllinger, R.; Pratschke, J.; Eberspächer, B.; Drosten, C.; Hofmann, J.; et al. Humoral Immune Response following SARS-CoV-2 Vaccination in Liver Transplant Recipients. Vaccines 2021, 9, 1422. [Google Scholar] [CrossRef]
- Feng, S.; Bucuvalas, J. Tolerance after liver transplantation: Where are we? Liver Transpl. 2017, 23, 1601–1614. [Google Scholar] [CrossRef] [PubMed]
- Pons, J.A.; Revilla-Nuin, B.; Baroja-Mazo, A.; Ramírez, P.; Martínez-Alarcón, L.; Sánchez-Bueno, F.; Robles, R.; Rios, A.; Aparicio, P.; Parrilla, P. FoxP3 in Peripheral Blood Is Associated With Operational Tolerance in Liver Transplant Patients During Immunosuppression Withdrawal. Transplantation 2008, 86, 1370–1378. [Google Scholar] [CrossRef]
- Pérez-Sanz, F.; Revilla-Nuin, B.; Martínez-Alarcón, L.; Herrero, J.I.; Ramírez, P.; Pons, J.A.; Baroja-Mazo, A. Tolerance Biomarkers in Liver Transplantation: Independent External Validation of the Predictive Strength of SENP6 and FEM1C Gene Expression. Transplantation 2019, 103, 1887–1892. [Google Scholar] [CrossRef]
- Levitsky, J.; Kandpal, M.; Guo, K.; Zhao, L.; Kurian, S.; Whisenant, T.; Abecassis, M. Prediction of Liver Transplant Rejection With a Biologically Relevant Gene Expression Signature. Transplantation 2021, 106, 1004–1011. [Google Scholar] [CrossRef]
- Taner, T. Liver transplantation: Rejection and tolerance. Liver Transplant. 2017, 23, S85–S88. [Google Scholar] [CrossRef]
- Feng, S.; Ekong, U.D.; Lobritto, S.J.; Demetris, A.J.; Roberts, J.P.; Rosenthal, P.; Alonso, E.M.; Philogene, M.C.; Ikle, D.; Poole, K.M.; et al. Complete Immunosuppression Withdrawal and Subsequent Allograft Function Among Pediatric Recipients of Parental Living Donor Liver Transplants. JAMA 2012, 307, 283–293. [Google Scholar] [CrossRef]
- Demetris, A.J.; Batts, K.P.; Dhillon, A.P.; Ferrell, L.; Fung, J.; Geller, S.A.; Hart, J.; Hayry, P.; Hofmann, W.J.; Hubscher, S.; et al. Banff schema for grading liver allograft rejection: An international consensus document. Hepatology 1997, 25, 658–663. [Google Scholar]
- Desmet, V.J.; Gerber, M.; Hoofnagle, J.H.; Manns, M.; Scheuer, P.J. Classification of chronic hepatitis: Diagnosis, grading and staging. Hepatology 1994, 19, 1513–1520. [Google Scholar] [CrossRef] [PubMed]
- Goldin, R.D.; Goldin, J.G.; Burt, A.D.; Dhillon, P.A.; Hubscher, S.; Wyatt, J.; Patel, N. Intra-observer and inter-observer variation in the histopathological assessment of chronic viral hepatitis. J. Hepatol. 1996, 25, 649–654. [Google Scholar] [CrossRef]
- Tannapfel, A.; Denk, H.; Dienes, H.-P.; Langner, C.; Schirmacher, P.; Trauner, M.; Flott-Rahmel, B. Histopathological diagnosis of non-alcoholic and alcoholic fatty liver disease. Virchows Arch. 2011, 458, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F. Regression Modeling Strategies, with Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Taner, T.; Bruner, J.B.; Emamaullee, J.; Bonaccorsi-Riani, E.; Zarrinpar, A. New Approaches to the Diagnosis of Rejection and Prediction of Tolerance in Liver Transplantation. Transplantation 2022, 106, 1952–1962. [Google Scholar] [CrossRef] [PubMed]
- Ronca, V.; Wootton, G.; Milani, C.; Cain, O. The Immunological Basis of Liver Allograft Rejection. Front. Immunol. 2020, 11, 2155. [Google Scholar] [CrossRef] [PubMed]
- Takatsuki, M.; Uemoto, S.; Inomata, Y.; Egawa, H.; Kiuchi, T.; Fujita, S.; Hayashi, M.; Kanematsu, T.; Tanaka, K. Weaning of immunosuppression in living donor liver transplant recipients1. Transplantation 2001, 72, 449–454. [Google Scholar] [CrossRef]
- Shaked, A.; DesMarais, M.R.; Kopetskie, H.; Feng, S.; Punch, J.D.; Levitsky, J.; Reyes, J.; Klintmalm, G.B.; Demetris, A.J.; Burrell, B.E.; et al. Outcomes of immunosuppression minimization and withdrawal early after liver transplantation. Am. J. Transplant. 2019, 19, 1397–1409. [Google Scholar] [CrossRef]
- Bohne, F.; Martinez-Llordella, M.; Lozano, J.J.; Miquel, R.; Benítez, C.; Londoño, M.C.; Manzia, T.M.; Angelico, R.; Swinkels, D.W.; Tjalsma, H.; et al. Intra-graft expression of genes involved in iron homeostasis predicts the development of operational tolerance in human liver transplantation. J. Clin. Investig. 2012, 122, 368–382. [Google Scholar] [CrossRef] [PubMed]
- Vionnet, J.; Miquel, R.; Abraldes, J.G.; Wall, J.; Kodela, E.; Lozano, J.-J.; Ruiz, P.; Navasa, M.; Marshall, A.; Nevens, F.; et al. Non-invasive alloimmune risk stratification of long-term liver transplant recipients. J. Hepatol. 2021, 75, 1409–1419. [Google Scholar] [CrossRef]
- Clavien, P.A.; Lesurtel, M.; Bossuyt, P.M.; Gores, G.J.; Langer, B.; Perrier, A. Recommendations for liver transplantation for hepatocellular carcinoma: An in-ternational consensus conference report. Lancet Oncol. 2012, 13, e11–e22. [Google Scholar] [CrossRef]
- Yokoyama, I.; Carr, B.; Saitsu, H.; Iwatsuki, S.; Starzl, T.E. Accelerated growth rates of recurrent hepatocellular carcinoma after liver transplantation. Cancer 1991, 68, 2095–2100. [Google Scholar] [CrossRef]
- Shinozuka, H.; Warty, V.S.; Masuhara, M.; Murase, N.; Iwatsuki, S. Effect of FK 506 on experimental liver carcinogenesis. Transplant. Proc. 1991, 23, 3197–3199. [Google Scholar] [PubMed]
- Mazzucotelli, V.; Piselli, P.; Verdirosi, D.; Cimaglia, C.; Cancarini, G.; Serraino, D.; Sandrini, S. De novo cancer in patients on dialysis and after renal transplantation: North-western Italy, 1997–2012. J. Nephrol. 2017, 30, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Lerut, J.; Iesari, S.; Foguenne, M.; Lai, Q. Hepatocellular cancer and recurrence after liver transplantation: What about the impact of immunosuppression? Transl. Gastroenterol. Hepatol. 2017, 2, 80. [Google Scholar] [CrossRef]
- Martínez-Llordella, M.; Lozano, J.J.; Puig-Pey, I.; Orlando, G.; Tisone, G.; Lerut, J.; Benítez, C.; Pons, J.A.; Parrilla, P.; Ramírez, P.; et al. Using transcriptional profiling to develop a diagnostic test of operational tolerance in liver transplant recipients. J. Clin. Investig. 2008, 118, 2845–2857. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Llordella, M.; Puig-Pey, I.; Orlando, G.; Ramoni, M.; Tisone, G.; Rimola, A.; Lerut, J.; Latinne, D.; Margarit, C.; Bilbao, I.; et al. Multiparameter immune profiling of operational tolerance in liver trans-plantation. Am. J. Transplant. 2007, 7, 309–319. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Indication for LT; n (%) | ALD | 13 (15.9) |
| HCV | 36 (43.9) | |
| HBV | 13 (15.9) | |
| Cholestatic liver disease | 6 (7.3) | |
| others | 14 (17.1) | |
| Re-LT | 10 (12.2) | |
| Mode of liver failure; n (%) | acute | 5 (6.1) |
| cirrhosis | 53 (64.6) | |
| HCC in cirrhosis | 24 (29.3) | |
| Last immuno- suppressive medication; n (%) | CNI mono | 42 (51.2) |
| CNI/MMF | 23 (28.0) | |
| MMF mono | 13 (15.9) | |
| CNI/EVL | 2 (2.4) | |
| EVL mono | 2 (2.4) | |
| Results of IS discontinuation; n (%) | impossible | 24 (29.3) |
| possible but IS reinstitution | 10 (12.2) | |
| tolerance | 48 (58.5) | |
| Mode of weaning; n (%) | On their own | 15 (18.3) |
| Controlled | 48 (58.5) | |
| Controlled (tumor) | 19 (23.2) |
| Side Effects of IS | Proportion of Patients; n = 82 |
|---|---|
| Arterial hypertension | 22 (26.8) |
| Kidney dysfunction > CKD G3a/b | 22 (26.8) |
| Diabetes mellitus | 19 (23.2) |
| Infections | 40 (48.8) |
| Gastrointestinal disturbances | 12 (14.6) |
| Neurological complications | 13 (15.9) |
| Tumor | 29 (35.4) |
| Skin tumors | 8 (9.8) |
| Lymphomas | 6 (7.3) |
| Solid tumors | 15 (18.3) |
| Before | After | p | |||
|---|---|---|---|---|---|
| Fibrosis stage | tolerant | 0 | 9 (18.8) | 6 (15.4) | 1.000 |
| F-stage available: Before weaning; n = 48 After 1 IS-free year; n = 39 | 1 | 23 (47.9) | 22 (56.4) | ||
| 2 | 11 (22.9) | 8 (20.5) | |||
| 3 | 5 (10.4) | 3 (7.7) | |||
| 4 | 0 (0.0) | 0 (0.0) | |||
| intolerant | 0 | 5 (15.2) | 5 (19.2) | 0.206 | |
| F-stage available: Before weaning; n = 33 Before IS reinstitution; n = 26 | 1 | 19 (57.6) | 12 (46.2) | ||
| 2 | 8 (24.2) | 7 (26.9) | |||
| 3 | 1 (3.0) | 2 (7.7) | |||
| 4 | 0 (0.0) | 0 (0.0) | |||
| tolerant | 0 | 11 (22.9) | 7 (20.0) | 0.593 | |
| Inflammation grade | I-grade available: Before weaning; n = 48 After 1 IS-free year; n = 35 | 1 | 22 (45.8) | 22 (62.9) | |
| 2 | 14 (29.2) | 5 (14.3) | |||
| 3 | 1 (2.1) | 1 (2.9) | |||
| 4 | 0 (0.0) | 0 (0.0) | |||
| intolerant | 0 | 9 (27.3) | 0 (0.0) | <0.001 | |
| I-grade available Before weaning; n = 33 Before IS-reinstitution; n = 26 | 1 | 19 (57.6) | 14 (53.8) | ||
| 2 | 4 (12.1) | 12 (46.2) | |||
| 3 | 1 (3.0) | 0 (0.0) | |||
| 4 | 0 (0.0) | 0 (0.0) | |||
| Content of fat | tolerant | <5% | 25 (52.1) | 24 (68.6) | 0.039 |
| Content of fat available Before weaning; n = 48 Before IS reinstitution; n = 35 | 5–33% | 17 (35.4) | 10 (28.6) | ||
| 33–66% | 2 (4.2) | 1 (2.9) | |||
| >66% | 4 (8.3) | 0 (0.0) | |||
| intolerant | <5% | 23 (69.7) | 21 (80.8) | 0.157 | |
| Content of fat available Before weaning; n = 33 Before IS reinstitution; n = 26 | 5–33% | 9 (27.3) | 4 (15.4) | ||
| 33–66% | 1 (3.0) | 1 (3.8) | |||
| >66% | 0 (0.0) | 0 (0.0) |
| Parameters | Units | Entire Cohort n = 82 | Tolerant Patients n = 48 | Intolerant Patients n = 34 | p-Value |
|---|---|---|---|---|---|
| R-age at LT | Years (min–max) | 52.4 (13–67) | 53.2 (15.5–66.6) | 51.6 (13.0–63.3) | 0.221 |
| D-age at LT | Years (min–max) | 42.5 (12–89) | 42.0 (12.0–71.0) | 47.5 (12.0–89.0) | 0.970 |
| Time since LT | Years (min–max) | 12.6 (0.4–30.7) | 13.8 (5.5–30.7) | 9.2 (0.4–29.0) | 0.002 |
| R-gender | female n (%) | 33 (40.2) | 12 (25.0) | 21 (61.8) | 0.001 |
| male n (%) | 49 (59.8) | 36 (75.0) | 13 (38.2) | ||
| D-gender | female n (%) | 32 (39.0) | 15 (31.3) | 17 (50.0) | 0.110 |
| male n (%) | 50 (61.0) | 33 (68.8) | 17 (50.0) | ||
| HCC | yes; n (%) | 24 (29.3) | 19 (39.6) | 5 (17.4) | 0.025 |
| no; n (%) | 58 (70.7) | 29 (60.4) | 29 (85.3) | ||
| Viral cirrhosis | yes; n (%) | 49 (59.8) | 32 (66.7) | 17 (50.0) | 0.171 |
| no; n (%) | 33 (40.2) | 16 (33.3) | 17 (50.0) | ||
| ACR | yes; n (%) | 38 (46.3) | 15 (31.3) | 23 (67.6) | 0.002 |
| no; n (%) | 44 (53.7) | 33 (68.8) | 11 (32.4) | ||
| Post transplant malignancy | yes; n (%) | 29 (35.4) | 23 (47.9) | 6 (17.6) | 0.005 |
| no; n (%) | 53 (64.6) | 25 (52.1) | 28 (82.4) | ||
| Malignancy (any) | yes; n (%) | 40 (48.8) | 31 (64.6) | 9 (26.5) | <0.001 |
| no; n (%) | 42 (51.2) | 17 (35.4) | 25 (73.5) | ||
| Monotherapy | yes; n (%) | 56 (68.3) | 41 (85.4) | 15 (44.1) | <0.001 |
| no; n (%) | 26 (31.7) | 7 (14.6) | 19 (55.9) | ||
| CNI mono | yes; n (%) | 41 (50.0) | 28 (58.3) | 13 (38.2) | 0.116 |
| no; n (%) | 41 (50.0) | 20 (41.7) | 21 (61.8) | ||
| CNI/MMF | yes; n (%) | 24 (29.3) | 6 (12.5) | 18 (52.9) | <0.001 |
| no; n (%) | 58 (70.7) | 42 (87.5) | 16 (47.1) | ||
| MMF mono | yes; n (%) | 13 (15.9) | 12 (25.0) | 1 (2.9) | 0.012 |
| no; n (%) | 69 (84.1) | 36 (75.0) | 33 (97.1) |
| Factor | χ2 | p-Value | OR (95% CI) |
|---|---|---|---|
| Time since LT | 2.65 | 0.103 | 2.77 (0.905–8.46) |
| post-LT malignancy | 0.70 | 0.401 | |
| HCC | 2.89 | 0.089 | 3.27 (0.958–11.19) |
| monotherapy | 9.11 | 0.003 | 7.18 (2.22–23.3) |
| recipient gender | 4.11 | 0.043 | 3.92 (1.34–11.5) |
| donor gender | 0.58 | 0.446 | |
| recipient age | 0.38 | 0.539 | |
| viral cirrhosis | 0.04 | 0.837 | |
| ACR | 4.67 | 0.031 | 2.92 (1.04–8.22) |
| TOTAL (d.f.) | 26.35 (7.01) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eurich, D.; Schlickeiser, S.; Ossami Saidy, R.R.; Uluk, D.; Rossner, F.; Postel, M.; Schoening, W.; Oellinger, R.; Lurje, G.; Pratschke, J.; et al. How to Estimate the Probability of Tolerance Long-Term in Liver Transplant Recipients. J. Clin. Med. 2023, 12, 6546. https://doi.org/10.3390/jcm12206546
Eurich D, Schlickeiser S, Ossami Saidy RR, Uluk D, Rossner F, Postel M, Schoening W, Oellinger R, Lurje G, Pratschke J, et al. How to Estimate the Probability of Tolerance Long-Term in Liver Transplant Recipients. Journal of Clinical Medicine. 2023; 12(20):6546. https://doi.org/10.3390/jcm12206546
Chicago/Turabian StyleEurich, Dennis, Stephan Schlickeiser, Ramin Raul Ossami Saidy, Deniz Uluk, Florian Rossner, Maximilian Postel, Wenzel Schoening, Robert Oellinger, Georg Lurje, Johann Pratschke, and et al. 2023. "How to Estimate the Probability of Tolerance Long-Term in Liver Transplant Recipients" Journal of Clinical Medicine 12, no. 20: 6546. https://doi.org/10.3390/jcm12206546
APA StyleEurich, D., Schlickeiser, S., Ossami Saidy, R. R., Uluk, D., Rossner, F., Postel, M., Schoening, W., Oellinger, R., Lurje, G., Pratschke, J., Reinke, P., & Gruen, N. (2023). How to Estimate the Probability of Tolerance Long-Term in Liver Transplant Recipients. Journal of Clinical Medicine, 12(20), 6546. https://doi.org/10.3390/jcm12206546