

Dynamics of Peripheral Blood Immune Cells during the Perioperative Period after Digestive System Resections: A Systematic Analysis of the Literature

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Characteristics
3.2. Gastric Cancer
3.3. Hepatocellular Carcinoma
3.4. Colorectal Cancer
3.5. Esophageal Cancer
3.6. Pancreatic Cancer

{kind=link}
{kind=link}
{kind=link}
| Reference | Study Population | Study Cell Type | Follow-Up Measurement Time-Points | Changing Tendency | Survivals | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patients | Amount | Study Type | Region | Treatment | Cell Marker | Cell Type | Cell Source | Method | ||||
| Gastric Cancer | ||||||||||||
| Takaya, S. et al., 2015 [27] | Gastric Cancer | 33 | PS | Japan | CS | N/A | Lymphocyte WBC | PB | FAC | POD 1, 3, 7, and POD 30 | Lymphocytes: Decreased on POD 1 and then increased, returned to preoperative level on POD 30. Increased on POD 1, then returned to preoperative level on POD 30 | N/A |
| Fujii, K. et al., 2003 [25] | Gastric cancer | 20 Including: LS: 10 and CS: 10 | PCS | Japan | CS MIS (LS) | Activated NK cell: CD57+. Activated lymphocyte: HLA-DR+. | WBC Lymphocyte CD3+ CD4+ CD8+ CD57+ HLA-DR+ | PBMC | FAC | POD 1, 3, and POD 7 | WBC: increased on POD 1, then returned to preoperative level on POD 7 Lymphocyte: decreased on POD 1, then maintained a low level CD3+, CD4+, CD8+, CD57+, and HLA-DR+: decreased on POD 1, then returned to preoperative level on POD 7 | N/A |
| Miyatani, K. et al., 2018 [16] | Gastric cancer | 280 | RS | Japan | CS | N/A | NLR | PB | Cell count | POM 1 | POM 1: Both Pre NLR high and POM 1 NLR high Either Pre NLR high or POM 1 NLR high Both Pre NLR low and POM 1 NLR low | 5 years survival: 58.1% 75.1% 92.8% |
| Hepatocellular Carcinoma | ||||||||||||
| Lee W-Ch. et al. 2019, [29] | HCC | 19 | PS | Taiwan | CS | CD8+ CD8+ /CD4+ CD4+/Foxp3+ CD33+/HLA-DR- | T cells T helper Tregs MDSC | PBMC | FAC | PreOP, POD 7 and POM 1 | CD4+ not altered by resection but CD8+ decreased. Tregs were not altered but MDSC were decreased at POM1 | OS: 1 y 79.8% 3 y 68.4% |
| Chen, T. et al., 2012 [28] | HCC | 36 | PCS | China | CS | CD4+CD25+CD127– CD19+IL-10+ | Tregs Bregs Lymphocytes | PBMC | FAC | POD 1 and POD 7 | Tregs and Bregs: increased on POD 1, especially on POD 7 Lymphocytes: decreased on POD 1 and returned to preoperative level on POD 7 | N/A |
| Peng, W. et al., 2014 [21] | HCC | 189 | RS | China | CS | N/A | NLR | N/A | N/M | POM 1 | POM 1: Increased group: 80 patients Decreased group: 109 patients | Increased group: Poor OS and RFS than NLR decreased group |
| Colorectal Carcinoma | ||||||||||||
| Helvind, N. M. et al., 2013 [30] | CRC | 263 Including LS: 162 and RAS: 101 | RS | The Netherlands | MIS (LS and RAS) | N/A | WBC | N/A | N/M | POD 1, POD 2 and POD 3 | LS: Pre to POD 1: increased POD 1 to POD 3: decreased RAS: Pre to POD 2: increased POD 2 to POD 3: decreased | N/A |
| Kubo, T. et al., 2014 [23] | CRC | 524 | RS | Japan | CS | N/A | NLR | PB | Cell count | POD 1 and POD 3 | Divided patients (include Pre, POD 1, and POD 3) into high NLR group and low NLR group | High perioperative NLR score: worse CSS and DFS |
| Shibata, J. et al., 2015 [19] | CRC | 46 Including: RAS: 15; LS: 23; CS: 8 | PS | Japan | CS MIS (RAS) | CD3−/CD56+ CD3+/CD8+ CD3+/CD4+ CD3-/CD19+ | NK cells CTL Th B lymphocytes | PB | FAC | POD 1, POD 3, and POD 6 | NK cells, CTL, and Th: from Pre to POD 1: decreased, POD 3 and POD 6: increased. B lymphocytes: no significant change | N/A |
| Ordemann, J. et al., 2001 [31] | CRC | 40 Include LS: 20 and CS: 20 | RCT | Germany | CS MIS (LS) | N/A | WBC CD4+ lymphocytes CD8+ lymphocytes CD4+/CD8+ ratio | PB | FACS | POD 1, 2, 4, and POD 7 | WBC: increased on POD 1, then returned to preoperative level on POD 7. CD4+ lymphocytes, CD8+ lymphocytes and CD4+/CD8+ ratio: no significant change after surgery | N/A |
| Leung, K.L. et al., 2003 [26] | CRC | 40, Including LS: 20 and CS 20 | RCT | Hong Kong | CS MIS (LS) | T cell: CD3+ T cell activation: CD3+ HLA-Dr+ Non-MHC restricted NK cell: CD3−CD16+CD56+ MHC-restricted NK-like cell: CD3+CD16+CD56+. Helper T cell: CD3+CD4+. Cytotoxic T cell: CD3+CD8+. NK cell: CD3−CD16+CD56+ | T cells T cell activation Non-MHC restricted NK cells MHC-restricted NK-like cells Helper T cells Cytotoxic T cells NK cells WBC Lymphocytes B cells | PB | Cell count | POD 1, POD 3, and POD 8 | WBC: increased on POD 1, then returned to preoperative level on POD 8. Lymphocytes, T cells, B cells, Non-MHC restricted NK cells, NK cells, Natural Killer-like T cells, Cytotoxic T cell, Helper T cells, T cell activation: decreased on POD 1, then returned to preoperative level on POD 8 | N/A |
| Wang, Y. et al., 2017 [17] | CRC | 7 | PCS | China | CS | N/A | T lymphocyte % NK lymphocyte % NKT lymphocyte % | PBMC | FAC | POW 1 | POW 1: N.S. | N/A |
| Ling, L. et al., 2015 [20] | CRC | 31 | PCS | China | CS | Th1: IL-17-IL-22-IFN-γ+CD4+. Th17: IL-17+IL-22-IFN-γ-CD4+. Th22: IL-17-IL-22+IFN-γ-CD4+ | Th1 Th17 Th22 IL-17+IL-22+IFN-γ-CD4+ T cells | PB | FAC | POD 14 | Th1%: POD 14: N.S. Th17%, Th22%, and IL-17+IL-22+IFN-γ-CD4+ T cells%: POD 14 were significantly higher than Pre | N/A |
| Esophageal Cancer | ||||||||||||
| Maas, K.W. et al., 2014 [32] | Esophageal cancer | 27 Including CS: 13 and LS: 14 | RCT | The Netherlands | CS MIS (LS) | N/A | WBC | PB | N/M | POD 1, POD 3, POD 4, and POD 7 | Increased on POD 1, then decreased until to POD 4. But CS group increased on POD 7 | N/A |
| Tan, J.H. et al., 2016 [18] | Esophageal cancer | 228 Including: VATS: 52; CS: 176 | RS | China | CS MIS (VATS) | N/A | CD3+ cells CD4+ cells CD8+ cells CD4+/CD8+ ratio NK cells | PB | FAC | POD 1 and POD 7 | CD3+ cells, CD4+ cells, NK cells and CD4+/CD8+ ratio: VATS: POD 1: decreased, then returned to preoperative level on POD 7 CS: POD 1: decreased, then increased, but POD 7 still lower than Pre CD8+ T cells: N.S. | N/A |
| Shi, J. et al., 2014 [22] | Esophageal cancer | 60 | PCS | China | CS | CD5+CD19+ | Bregs | PBMC | FAC | POD 1 and POD 7 | From POD 1 to POD 7: decreased. | N/A |
| Pancreatic Cancer | ||||||||||||
| Tezuka, k. et al., 2012 [24] | Pancreatic cancer | 53 | RS | Japan | CS | N/A | WBC | N/A | N/M | POD 1, 2, 3, 5, 7, POW 2, POM 1, and POM 3 | Pre to POD 2: increased, then decreased until POM 3 | N/A |
| Takahashi, K. et al., 2006 [14] | Pancreatic cancer | 20 | PCS | Japan | CS | CD11c+ DCs CD11c− DCs CD14−/CD56+ CD3+/CD4+ CD3+/CD8+ | Cdc1 Cdc2 NK cells CD4+ T lymphocytes CD8+ T lymphocytes Cdc1/cDC2 ratio | PB | FAC | POM 12 | cDC1 and cDC1/cDC2 ratio increased in POM 12. cDC2: N.S. CD4+ T lymphocytes, CD8+ T lymphocytes, and NK cells: no significant change in POM 12 | cDC1 count and cDC1/cDC2 ratio normalized in POM 12: no obvious local recurrence or distant metastasis |
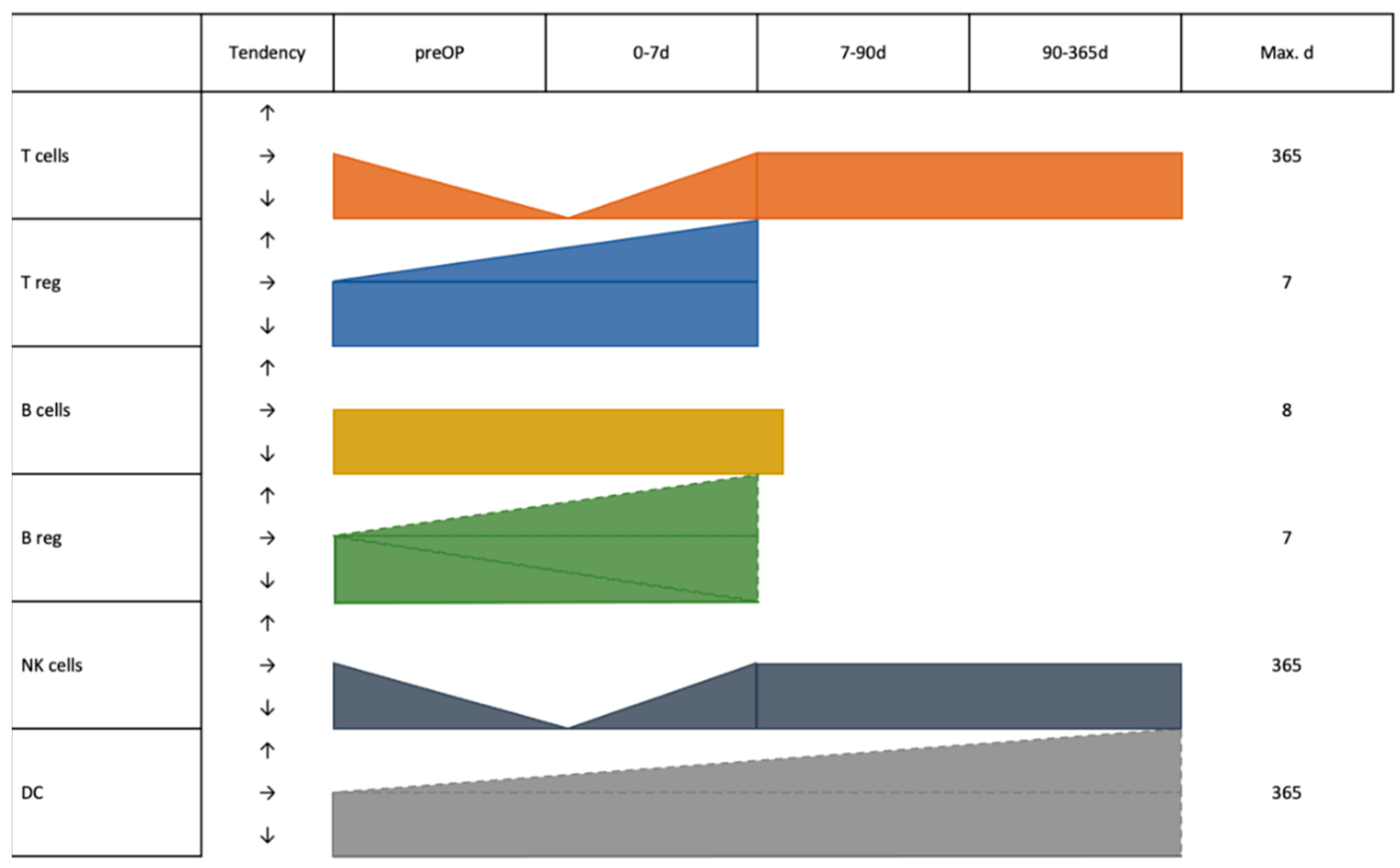
3.7. Cell Subsets across Entities
4. Discussion
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Bregs | Regulatory B cells |
| CD | Cluster of differentiation |
| CRC | Colorectal cancer |
| DCs | Dendritic cells |
| HCC | Hepatocellular carcinoma |
| MDSC | Myeloid derived suppressor cells |
| NK | Natural killer cells |
| NLR | Neutrophil-lymphocyte ratio |
| PB | Peripheral blood |
| POD | Postoperation day |
| POM | Postoperation month |
| Th | Helper T cells |
| Tregs | Regulatory T cells |
| WBC | White blood cells |
References
- Chen, Z.; Zhang, P.; Xu, Y.; Yan, J.; Liu, Z.; Lau, W.B.; Lau, B.; Li, Y.; Zhao, X.; Wei, Y.; et al. Surgical stress and cancer progression: The twisted tango. Mol. Cancer 2019, 18, 132. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Shan, F.; Li, Z.; Gao, J.; Li, Y.; Shen, L.; Ji, J.; Lu, M. A prospective study on the changes and clinical significance of pre-operative and post-operative circulating tumor cells in resectable gastric cancer. J. Transl. Med. 2018, 16, 171. [Google Scholar] [CrossRef] [PubMed]
- Ou, H.; Huang, Y.; Xiang, L.; Chen, Z.; Fang, Y.; Lin, Y.; Cui, Z.; Yu, S.; Li, X.; Yang, D. Circulating Tumor Cell Phenotype Indicates Poor Survival and Recurrence After Surgery for Hepatocellular Carcinoma. Dig. Dis. Sci. 2018, 63, 2373–2380. [Google Scholar] [CrossRef] [PubMed]
- Peach, G.; Kim, C.; Zacharakis, E.; Purkayastha, S.; Ziprin, P. Prognostic significance of circulating tumour cells following surgical resection of colorectal cancers: A systematic review. Br. J. Cancer 2010, 102, 1327–1334. [Google Scholar] [CrossRef]
- Decker, D.; Tolba, R.; Springer, W.; Lauschke, H.; Hirner, A.; von Ruecker, A. Abdominal surgical interventions: Local and systemic consequences for the immune system--a prospective study on elective gastrointestinal surgery. J. Surg. Res. 2005, 126, 12–18. [Google Scholar] [CrossRef]
- Gryglewski, A.; Richter, P.; Majewska-Szczepanik, M.; Szczepanik, M. Post-operative complications in patients with a significant post-operative decrease in γδT cells. ANZ J. Surg. 2019, 90, 62–66. [Google Scholar] [CrossRef]
- Shankar Hari, M.; Summers, C. Major surgery and the immune system: From pathophysiology to treatment. Curr. Opin. Crit. Care 2018, 24, 588–593. [Google Scholar] [CrossRef]
- Torrance, H.D.T.; Longbottom, E.R.; Vivian, M.E.; Lalabekyan, B.; Abbott, T.E.F.; Ackland, G.L.; Hinds, C.J.; Pearse, R.M.; O’Dwyer, M.J. Post-operative immune suppression is mediated via reversible, Interleukin-10 dependent pathways in circulating monocytes following major abdominal surgery. PLoS ONE 2018, 13, e0203795. [Google Scholar] [CrossRef]
- Kumar, B.V.; Connors, T.J.; Farber, D.L. Human T Cell Development, Localization, and Function throughout Life. Immunity 2018, 48, 202–213. [Google Scholar] [CrossRef]
- Allman, D.; Pillai, S. Peripheral B cell subsets. Curr. Opin. Immunol. 2008, 20, 149–157. [Google Scholar] [CrossRef]
- Mauri, C.; Bosma, A. Immune regulatory function of B cells. Annu. Rev. Immunol. 2012, 30, 221–241. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.C.; Lanier, L.L. NK cell development, homeostasis and function: Parallels with CD8(+) T cells. Nat. Rev. Immunol. 2011, 11, 645–657. [Google Scholar] [CrossRef]
- Guermonprez, P.; Valladeau, J.; Zitvogel, L.; Thery, C.; Amigorena, S. Antigen presentation and T cell stimulation by dendritic cells. Annu. Rev. Immunol. 2002, 20, 621–667. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Toyokawa, H.; Takai, S.; Satoi, S.; Yanagimoto, H.; Terakawa, N.; Araki, H.; Kwon, A.H.; Kamiyama, Y. Surgical influence of pancreatectomy on the function and count of circulating dendritic cells in patients with pancreatic cancer. Cancer Immunol. Immunother. CII 2006, 55, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Brivio, F.; Gilardi, R.; Bucocev, R.; Ferrante, R.; Rescaldani, R.; Vigore, L.; Fumagalli, L.; Nespoli, A.; Lissoni, P. Surgery-induced decline in circulating dendritic cells in operable cancer patients: A possible explanation of postoperative immunosuppression. Hepato-Gastroenterol. 2000, 47, 1337–1339. [Google Scholar]
- Miyatani, K.; Saito, H.; Kono, Y.; Murakami, Y.; Kuroda, H.; Matsunaga, T.; Fukumoto, Y.; Osaki, T.; Ashida, K.; Fujiwara, Y. Combined analysis of the pre- and postoperative neutrophil-lymphocyte ratio predicts the outcomes of patients with gastric cancer. Surg. Today 2018, 48, 300–307. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, J.; Gao, W.; Song, B.; Shao, Q.; Zhao, L.; Zhang, Y.; Wang, Q.; Zhang, Y.; Qu, X. Preoperative Tim3 expression on peripheral NK cells is correlated with pathologic TNM staging in colorectal cancer. Mol. Med. Rep. 2017, 15, 3810–3818. [Google Scholar] [CrossRef]
- Tan, J.T.; Zhong, J.H.; Yang, Y.; Mao, N.Q.; Liu, D.S.; Huang, D.M.; Zhao, Y.X.; Zuo, C.T. Comparison of postoperative immune function in patients with thoracic esophageal cancer after video-assisted thoracoscopic surgery or conventional open esophagectomy. Int. J. Surg. (Lond. Engl.) 2016, 30, 155–160. [Google Scholar] [CrossRef]
- Shibata, J.; Ishihara, S.; Tada, N.; Kawai, K.; Tsuno, N.H.; Yamaguchi, H.; Sunami, E.; Kitayama, J.; Watanabe, T. Surgical stress response after colorectal resection: A comparison of robotic, laparoscopic, and open surgery. Tech. Coloproctology 2015, 19, 275–280. [Google Scholar] [CrossRef]
- Ling, L.; Zhao, P.; Yan, G.; Chen, M.; Zhang, T.; Wang, L.; Jiang, Y. The frequency of Th17 and Th22 cells in patients with colorectal cancer at pre-operation and post-operation. Immunol. Investig. 2015, 44, 56–69. [Google Scholar] [CrossRef]
- Peng, W.; Li, C.; Wen, T.F.; Yan, L.N.; Li, B.; Wang, W.T.; Yang, J.Y.; Xu, M.Q. Neutrophil to lymphocyte ratio changes predict small hepatocellular carcinoma survival. J. Surg. Res. 2014, 192, 402–408. [Google Scholar] [CrossRef]
- Shi, J.; Li, S.; Zhou, Y.; Wang, L.; Wen, J.; Wang, Y.; Kang, Z. Perioperative changes in peripheral regulatory B cells of patients with esophageal cancer. Mol. Med. Rep. 2014, 10, 1525–1530. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Ono, S.; Ueno, H.; Shinto, E.; Yamamoto, J.; Hase, K. Impact of the perioperative neutrophil-to-lymphocyte ratio on the long-term survival following an elective resection of colorectal carcinoma. Int. J. Color. Dis. 2014, 29, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Tezuka, K.; Kimura, W.; Hirai, I.; Moriya, T.; Watanabe, T.; Yano, M. Postoperative hematological changes after spleen-preserving distal pancreatectomy with preservation of the splenic artery and vein. Dig. Surg. 2012, 29, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Fujii, K.; Sonoda, K.; Izumi, K.; Shiraishi, N.; Adachi, Y.; Kitano, S. T lymphocyte subsets and Th1/Th2 balance after laparoscopy-assisted distal gastrectomy. Surg. Endosc. 2003, 17, 1440–1444. [Google Scholar] [CrossRef]
- Leung, K.L.; Tsang, K.S.; Ng, M.H.; Leung, K.J.; Lai, P.B.; Lee, J.F.; Lau, W.Y. Lymphocyte subsets and natural killer cell cytotoxicity after laparoscopically assisted resection of rectosigmoid carcinoma. Surg. Endosc. 2003, 17, 1305–1310. [Google Scholar] [CrossRef]
- Takaya, S.; Saito, H.; Ikeguchi, M. Upregulation of Immune Checkpoint Molecules, PD-1 and LAG-3, on CD4+ and CD8+ T Cells after Gastric Cancer Surgery. Yonago Acta Med. 2015, 58, 39–44. [Google Scholar]
- Chen, T.; Song, D.; Min, Z.; Wang, X.; Gu, Y.; Wei, B.; Yao, J.; Chen, K.; Jiang, Z.; Xie, H.; et al. Perioperative dynamic alterations in peripheral regulatory T and B cells in patients with hepatocellular carcinoma. J. Transl. Med. 2012, 10, 14. [Google Scholar] [CrossRef]
- Lee, W.C.; Wang, Y.C.; Cheng, C.H.; Wu, T.H.; Lee, C.F.; Wu, T.J.; Chou, H.S.; Chan, K.M. Myeloid-derived suppressor cells in the patients with liver resection for hepatitis B virus-related hepatocellular carcinoma. Sci. Rep. 2019, 9, 2269. [Google Scholar] [CrossRef]
- Helvind, N.M.; Eriksen, J.R.; Mogensen, A.; Tas, B.; Olsen, J.; Bundgaard, M.; Jakobsen, H.L.; Gogenur, I. No differences in short-term morbidity and mortality after robot-assisted laparoscopic versus laparoscopic resection for colonic cancer: A case-control study of 263 patients. Surg. Endosc. 2013, 27, 2575–2580. [Google Scholar] [CrossRef]
- Ordemann, J.; Jacobi, C.A.; Schwenk, W.; Stosslein, R.; Muller, J.M. Cellular and humoral inflammatory response after laparoscopic and conventional colorectal resections. Surg. Endosc. 2001, 15, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Maas, K.W.; Biere, S.S.; van Hoogstraten, I.M.; van der Peet, D.L.; Cuesta, M.A. Immunological changes after minimally invasive or conventional esophageal resection for cancer: A randomized trial. World J. Surg. 2014, 38, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.; Zou, C.; Pan, L.; Liang, W.; Qian, H.; Xu, W.; Jiang, P.; Zhang, X. Long noncoding RNAs in digestive system cancers: Functional roles, molecular mechanisms, and clinical implications (Review). Oncol. Rep. 2016, 36, 1207–1218. [Google Scholar] [CrossRef]
- Wang, Y.H.; Ji, J.; Weng, H.; Wang, B.C.; Wang, F.B. MiR-139 in digestive system tumor diagnosis and detection: Bioinformatics and meta-analysis. Clin. Chim. Acta 2018, 485, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Carrick, J.B.; Begg, A.P. Peripheral blood leukocytes. Vet. Clin. N. Am. Equine Pract. 2008, 24, 239–259. [Google Scholar] [CrossRef]
- Al-Shayyab, M.H.; Al-Omiri, M.K.; Ryalat, S.; Qabbaah, K.; Baqain, Z.H. Leukocytosis is common after orthognathic surgery: A retrospective study. J. Stomatol. Oral. Maxillofac. Surg. 2019, 120, 443–449. [Google Scholar] [CrossRef]
- Fleisher, T.A.; Oliveira, J.B. Functional and molecular evaluation of lymphocytes. J. Allergy Clin. Immunol. 2004, 114, 227–234; quiz 235. [Google Scholar] [CrossRef]
- Shaul, M.E.; Fridlender, Z.G. Cancer-related circulating and tumor-associated neutrophils-subtypes, sources and function. FEBS J. 2018, 285, 4316–4342. [Google Scholar] [CrossRef]
- Valipour, B.; Velaei, K.; Abedelahi, A.; Karimipour, M.; Darabi, M.; Charoudeh, H.N. NK cells: An attractive candidate for cancer therapy. J. Cell Physiol. 2019, 234, 19352–19365. [Google Scholar] [CrossRef]
- Ni Choileain, N.; Redmond, H.P. Cell response to surgery. Arch. Surg. 2006, 141, 1132–1140. [Google Scholar] [CrossRef]
- Li, T.Y.; Yang, Y.; Zhou, G.; Tu, Z.K. Immune suppression in chronic hepatitis B infection associated liver disease: A review. World J. Gastroenterol. 2019, 25, 3527–3537. [Google Scholar] [CrossRef]
- Schoenberg, M.B.; Zhu, T.; Hao, J.; Bucher, J.N.; Li, X.; Li, X.; Han, Y.; Koliogiannis, D.; Svihla, M.; Guba, M.O.; et al. Highly differential count of circulating and tumor infiltrating immune cells in patients with non-HCV/non-HBV hepatocellular carcinoma. Cancer Immunol. Immunother. 2022, 71, 1103–1113. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoenberg, M.B.; Han, Y.; Li, X.; Li, X.; Bucher, J.N.; Börner, N.; Koch, D.; Guba, M.O.; Werner, J.; Bazhin, A.V. Dynamics of Peripheral Blood Immune Cells during the Perioperative Period after Digestive System Resections: A Systematic Analysis of the Literature. J. Clin. Med. 2023, 12, 718. https://doi.org/10.3390/jcm12020718
Schoenberg MB, Han Y, Li X, Li X, Bucher JN, Börner N, Koch D, Guba MO, Werner J, Bazhin AV. Dynamics of Peripheral Blood Immune Cells during the Perioperative Period after Digestive System Resections: A Systematic Analysis of the Literature. Journal of Clinical Medicine. 2023; 12(2):718. https://doi.org/10.3390/jcm12020718
Chicago/Turabian StyleSchoenberg, Markus Bo, Yongsheng Han, Xiaokang Li, Xinyu Li, Julian Nikolaus Bucher, Nikolaus Börner, Dominik Koch, Markus Otto Guba, Jens Werner, and Alexandr V. Bazhin. 2023. "Dynamics of Peripheral Blood Immune Cells during the Perioperative Period after Digestive System Resections: A Systematic Analysis of the Literature" Journal of Clinical Medicine 12, no. 2: 718. https://doi.org/10.3390/jcm12020718
APA StyleSchoenberg, M. B., Han, Y., Li, X., Li, X., Bucher, J. N., Börner, N., Koch, D., Guba, M. O., Werner, J., & Bazhin, A. V. (2023). Dynamics of Peripheral Blood Immune Cells during the Perioperative Period after Digestive System Resections: A Systematic Analysis of the Literature. Journal of Clinical Medicine, 12(2), 718. https://doi.org/10.3390/jcm12020718