
Biological Markers to Predict Outcome in Mechanically Ventilated Patients with Severe COVID-19 Living at High Altitude





Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Criteria of Inclusion
2.2. Data Collection
2.3. Statistical Analysis
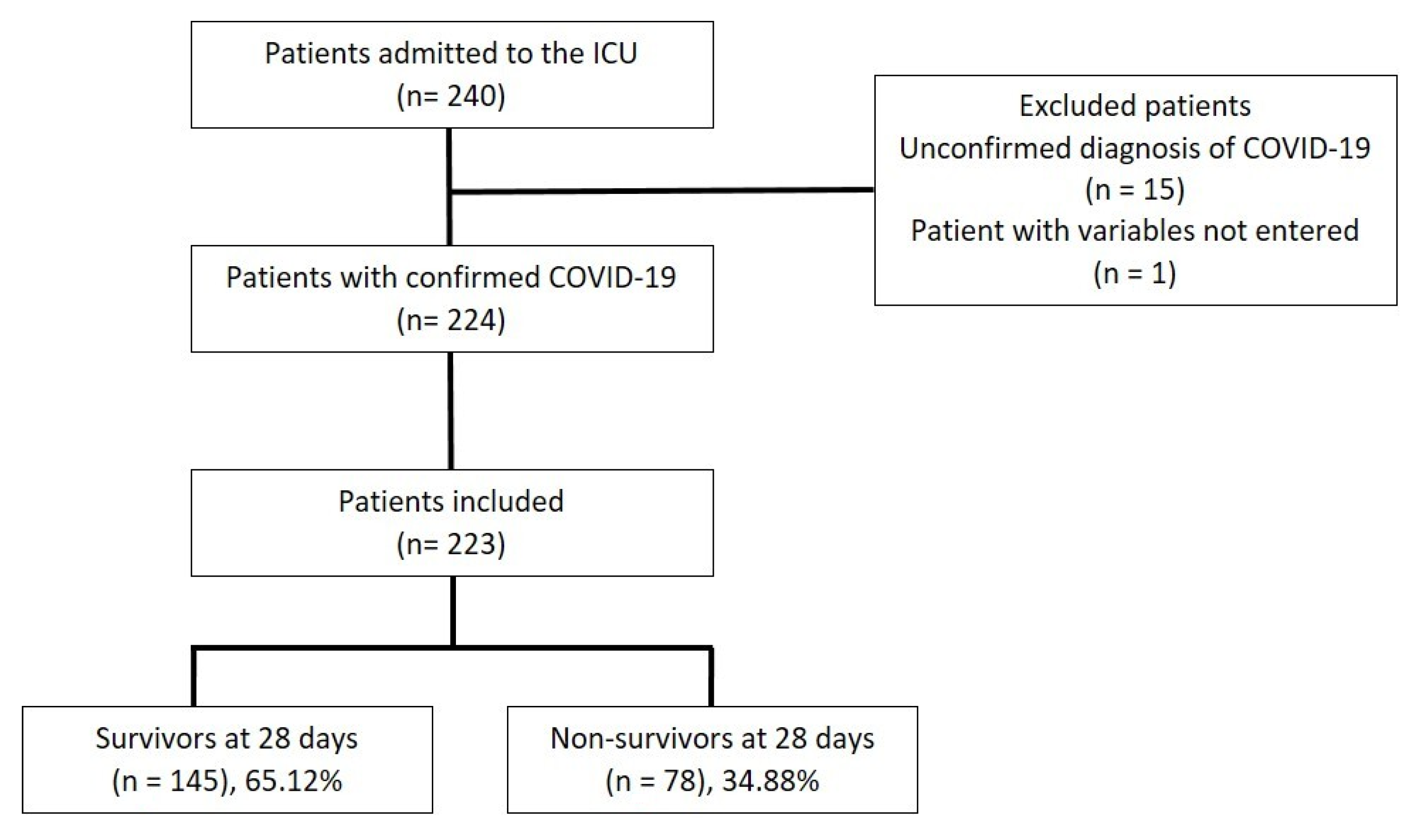
3. Results
3.1. Demographic and Clinical Characteristics of Patients with Severe COVID-19
3.2. Inflammatory and Hematological Markers in Patients with Severe COVID-19
3.3. Predictors of 28-Day Mortality
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bos, L.D.J.; Laffey, J.G.; Ware, L.B.; Heijnen, N.F.L.; Sinha, P.; Patel, B.; Jabaudon, M.; Bastarache, J.A.; McAuley, D.F.; Summers, C.; et al. Towards a Biological Definition of ARDS: Are Treatable Traits the Solution? Intensive Care Med. Exp. 2022, 10, 8. [Google Scholar] [CrossRef] [PubMed]
- Battaglini, D.; Al-Husinat, L.; Normando, A.G.; Leme, A.P.; Franchini, K.; Morales, M.; Pelosi, P.; Rocco, P.R. Personalized Medicine Using Omics Approaches in Acute Respiratory Distress Syndrome to Identify Biological Phenotypes. Respir. Res. 2022, 23, 318. [Google Scholar] [CrossRef] [PubMed]
- Battaglini, D.; Lopes-Pacheco, M.; Castro-Faria-Neto, H.C.; Pelosi, P.; Rocco, P.R.M. Laboratory Biomarkers for Diagnosis and Prognosis in COVID-19. Front. Immunol. 2022, 13, 857573. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider Cytokine Storm Syndromes and Immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Quincy Brown, J.; Vander Heide, R.S. Pulmonary and Cardiac Pathology in African American Patients with COVID-19: An Autopsy Series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhang, J.; Yang, Y.; Ma, H.; Li, Z.; Zhang, J.; Cheng, J.; Zhang, X.; Zhao, Y.; Xia, Z.; et al. The Role of Interleukin-6 in Monitoring Severe Case of Coronavirus Disease 2019. EMBO Mol. Med. 2020, 12, e12421. [Google Scholar] [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated Levels of IL-6 and CRP Predict the Need for Mechanical Ventilation in COVID-19. J. Allergy Clin. Immunol. 2020, 146, 128–136.e4. [Google Scholar] [CrossRef] [PubMed]
- Vélez-Paez, J.L.; Montalvo, M.P.; Jara, F.E.; Aguayo-Moscoso, S.; Tercero-Martínez, W.; Saltos, L.S.; Jiménez-Alulima, G.; Irigoyen-Mogro, E.; Castro-Reyes, E.; Mora-Coello, C.; et al. Predicting Mortality in Critically Ill Patients with COVID-19 in the ICU from a Secondary-Level Hospital in Ecuador. Rev. Bionatura 2022, 7, 1. [Google Scholar] [CrossRef]
- Zhong, Q.; Peng, J. Mean Platelet Volume/Platelet Count Ratio Predicts Severe Pneumonia of COVID-19. J. Clin. Lab. Anal. 2021, 35, e23607. [Google Scholar] [CrossRef]
- Sertbas, M.; Dağcı, S.; Kizilay, V.; Yazıcı, Z.; Elçi, E.; Özaydın, Ö.; Elarslan, S.; Şaylan, B.; Dayan, A.; Sertbas, Y.; et al. Mean Platelet Volume as an Early Predictor for The Complication of Coronavirus Disease 19. Haydarpaşa Numune Med. J. 2021, 6, 177–182. [Google Scholar]
- Vélez-Páez, J.L.; Tercero-Martínez, W.; Jiménez-Alulima, G.; Navarrete-Domínguez, J.; Cornejo-Loor, L.; Castro-Bustamante, C.; Cabanillas-Lazo, M.; Barboza, J.J.; Rodriguez-Morales, A.J. Neutrophil-to-Lymphocyte Ratio and Mean Platelet Volume in the Diagnosis of Bacterial Infections in COVID-19 Patients. A Preliminary Analysis from Ecuador. Infez. Med. 2021, 29, 530–537. [Google Scholar] [CrossRef]
- Liu, Y.; Du, X.; Chen, J.; Jin, Y.; Peng, L.; Wang, H.H.X.; Luo, M.; Chen, L.; Zhao, Y. Neutrophil-to-Lymphocyte Ratio as an Independent Risk Factor for Mortality in Hospitalized Patients with COVID-19. J. Infect. 2020, 81, e6–e12. [Google Scholar] [CrossRef] [PubMed]
- Ma, A.; Cheng, J.; Yang, J.; Dong, M.; Liao, X.; Kang, Y. Neutrophil-to-Lymphocyte Ratio as a Predictive Biomarker for Moderate-Severe ARDS in Severe COVID-19 Patients. Crit. Care 2020, 24, 288. [Google Scholar] [CrossRef] [PubMed]
- Basbus, L.; Lapidus, M.I.; Martingano, I.; Puga, M.C.; Pollán, J. Neutrophil to lymphocyte ratio as a prognostic marker in COVID-19. Medicina 2020, 80 (Suppl. S3), 31–36. [Google Scholar]
- Ramos-Peñafiel, C.O.; Santos-González, B.; Flores-López, E.N.; Galván-Flores, F.; Hernández-Vázquez, L.; Santoyo-Sánchez, A.; Montes de Oca-Yemha, R.; Bejarano-Rosales, M.; Rosas-González, É.; Olarte-Carrillo, I.; et al. Usefulness of the Neutrophil-to-Lymphocyte, Monocyte-to-Lymphocyte and Lymphocyte-to-Platelet Ratios for the Prognosis of COVID-19-Associated Complications. Gac. Méd. Méx. 2020, 156, 413–419. [Google Scholar] [CrossRef]
- Liu, J.; Liu, Y.; Xiang, P.; Pu, L.; Xiong, H.; Li, C.; Zhang, M.; Tan, J.; Xu, Y.; Song, R.; et al. Neutrophil-to-Lymphocyte Ratio Predicts Critical Illness Patients with 2019 Coronavirus Disease in the Early Stage. J. Transl. Med. 2020, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Mateu Campos, M.L.; Ferrándiz Sellés, A.; Gruartmoner de Vera, G.; Mesquida Febrer, J.; Sabatier Cloarec, C.; Poveda Hernández, Y.; García Nogales, X. Techniques available for hemodynamic monitoring. Advantages and limitations. Med. Intensiv. 2012, 36, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Abdelsalam, M.; Althaqafi, R.M.M.; Assiri, S.A.; Althagafi, T.M.; Althagafi, S.M.; Fouda, A.Y.; Ramadan, A.; Rabah, M.; Ahmed, R.M.; Ibrahim, Z.S.; et al. Clinical and Laboratory Findings of COVID-19 in High-Altitude Inhabitants of Saudi Arabia. Front. Med. 2021, 8, 670195. [Google Scholar] [CrossRef]
- Ballaz, S.J.; Pulgar-Sánchez, M.; Chamorro, K.; Fernández-Moreira, E.; Ramírez, H.; Mora, F.X.; Fors, M. Common Laboratory Tests as Indicators of COVID-19 Severity on Admission at High Altitude: A Single-Center Retrospective Study in Quito (ECUADOR). Clin. Chem. Lab. Med. 2021, 59, e326–e329. [Google Scholar] [CrossRef]
- Yuan, X.; Huang, W.; Ye, B.; Chen, C.; Huang, R.; Wu, F.; Wei, Q.; Zhang, W.; Hu, J. Changes of Hematological and Immunological Parameters in COVID-19 Patients. Int. J. Hematol. 2020, 112, 553–559. [Google Scholar] [CrossRef]
- Hunter, C.A.; Jones, S.A. IL-6 as a Keystone Cytokine in Health and Disease. Nat. Immunol. 2015, 16, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Meduri, G.U.; Headley, S.; Kohler, G.; Stentz, F.; Tolley, E.; Umberger, R.; Leeper, K. Persistent Elevation of Inflammatory Cytokines Predicts a Poor Outcome in ARDS. Plasma IL-1 Beta and IL-6 Levels Are Consistent and Efficient Predictors of Outcome over Time. Chest 1995, 107, 1062–1073. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.; Fatima, R.; Assaly, R. Elevated Interleukin-6 and Severe COVID-19: A Meta-Analysis. J. Med. Virol. 2020, 92, 2283–2285. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group Tocilizumab in Patients Admitted to Hospital with COVID-19 (RECOVERY): A Randomised, Controlled, Open-Label, Platform Trial. Lancet 2021, 397, 1637–1645. [CrossRef] [PubMed]
- Min, C.-K.; Cheon, S.; Ha, N.-Y.; Sohn, K.M.; Kim, Y.; Aigerim, A.; Shin, H.M.; Choi, J.-Y.; Inn, K.-S.; Kim, J.-H.; et al. Comparative and Kinetic Analysis of Viral Shedding and Immunological Responses in MERS Patients Representing a Broad Spectrum of Disease Severity. Sci. Rep. 2016, 6, 25359. [Google Scholar] [CrossRef] [PubMed]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.A.; Yang, J.C.; Kitano, M.; Dudley, M.E.; Laurencot, C.M.; Rosenberg, S.A. Case Report of a Serious Adverse Event Following the Administration of T Cells Transduced with a Chimeric Antigen Receptor Recognizing ERBB2. Mol. Ther. 2010, 18, 843–851. [Google Scholar] [CrossRef]
- Çalışkan, S.; Sungur, M.; Kaba, S.; Özsoy, E.; Koca, O.; Öztürk, M.İ. Neutrophil-to-Lymphocyte Ratio in Renal Cell Carcinoma Patients. Folia Med. 2018, 60, 553–557. [Google Scholar] [CrossRef]
- Ciccullo, A.; Borghetti, A.; Zileri Dal Verme, L.; Tosoni, A.; Lombardi, F.; Garcovich, M.; Biscetti, F.; Montalto, M.; Cauda, R.; Di Giambenedetto, S.; et al. Neutrophil-to-Lymphocyte Ratio and Clinical Outcome in COVID-19: A Report from the Italian Front Line. Int. J. Antimicrob. Agents 2020, 56, 106017. [Google Scholar] [CrossRef]
- Yang, A.-P.; Liu, J.-P.; Tao, W.-Q.; Li, H.-M. The Diagnostic and Predictive Role of NLR, d-NLR and PLR in COVID-19 Patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef]
- Akilli, N.B.; Yortanlı, M.; Mutlu, H.; Günaydın, Y.K.; Koylu, R.; Akca, H.S.; Akinci, E.; Dundar, Z.D.; Cander, B. Prognostic Importance of Neutrophil-Lymphocyte Ratio in Critically Ill Patients: Short- and Long-Term Outcomes. Am. J. Emerg. Med. 2014, 32, 1476–1480. [Google Scholar] [CrossRef]
- Ye, W.; Chen, G.; Li, X.; Lan, X.; Ji, C.; Hou, M.; Zhang, D.; Zeng, G.; Wang, Y.; Xu, C.; et al. Dynamic Changes of D-Dimer and Neutrophil-Lymphocyte Count Ratio as Prognostic Biomarkers in COVID-19. Respir. Res. 2020, 21, 169. [Google Scholar] [CrossRef]
- Prozan, L.; Shusterman, E.; Ablin, J.; Mitelpunkt, A.; Weiss-Meilik, A.; Adler, A.; Choshen, G.; Kehat, O. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in COVID-19 Compared with Influenza and Respiratory Syncytial Virus Infection. Sci. Rep. 2021, 11, 21519. [Google Scholar] [CrossRef]
- Martínez, F.; Boisier, D.; Vergara, C.; Vidal, J. Neutrophil to lymphocite ratio and inflammatory biomarkers as prognostic factors amongst patients with COVID-19: A prospective cohort study. Rev. Chil. Anest. 2022, 51, 80–87. [Google Scholar]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Gong, J.; Ou, J.; Qiu, X.; Jie, Y.; Chen, Y.; Yuan, L.; Cao, L.; Tan, J.; Xu, M.; Zheng, W.; et al. Multicenter Development and Validation of a Novel Risk Nomogram for Early Prediction of Severe 2019-Novel Coronavirus Pneumonia. 2020. Available online: https://search.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov/resource/es/ppcovidwho-637 (accessed on 27 November 2022).
- Ji, D.; Zhang, D.; Xu, J.; Chen, Z.; Yang, T.; Zhao, P.; Chen, G.; Cheng, G.; Wang, Y.; Bi, J.; et al. Prediction for Progression Risk in Patients with COVID-19 Pneumonia: The CALL Score. Clin. Infect. Dis. 2020, 71, 1393–1399. [Google Scholar] [CrossRef]
- Grommes, J.; Alard, J.-E.; Drechsler, M.; Wantha, S.; Mörgelin, M.; Kuebler, W.M.; Jacobs, M.; von Hundelshausen, P.; Markart, P.; Wygrecka, M.; et al. Disruption of Platelet-Derived Chemokine Heteromers Prevents Neutrophil Extravasation in Acute Lung Injury. Am. J. Respir. Crit. Care Med. 2012, 185, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T.A.; Brill, A.; Duerschmied, D.; Schatzberg, D.; Monestier, M.; Myers, D.D.; Wrobleski, S.K.; Wakefield, T.W.; Hartwig, J.H.; Wagner, D.D. Extracellular DNA Traps Promote Thrombosis. Proc. Natl. Acad. Sci. USA 2010, 107, 15880–15885. [Google Scholar] [CrossRef]
- Campos, A.; Scheveck, B.; Parikh, J.; Hernandez-Bojorge, S.; Terán, E.; Izurieta, R. Effect of Altitude on COVID-19 Mortality in Ecuador: An Ecological Study. BMC Public Health 2021, 21, 2079. [Google Scholar] [CrossRef] [PubMed]
- Giamarellos-Bourboulis, E.J.; Poulakou, G.; de Nooijer, A.; Milionis, H.; Metallidis, S.; Ploumidis, M.; Grigoropoulou, P.; Rapti, A.; Segala, F.V.; Balis, E.; et al. Development and Validation of SCOPE Score: A Clinical Score to Predict COVID-19 Pneumonia Progression to Severe Respiratory Failure. Cell Rep. Med. 2022, 3, 100560. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Features | All Patients | Survivors | Non-Survivors | p-Value |
|---|---|---|---|---|
| (n = 223) | (n = 145) | (n = 78) | ||
| Median age (Q1–Q3), years 1 | 51 (26–75) | 48 (25–72) | 56 (31–79) | 0.000 * |
| Sex, n (%) 2 | ||||
| Male | 157 (70.4) | 99 (68.3) | 58 (74.4) | 0.343 |
| Female | 66 (29.6) | 46 (31.7) | 20 (25.6) | |
| DM, n (%) 2 | 28 (12.6) | 16 (11.0) | 12 (15.4) | 0.350 |
| Hypertension, n (%) 2 | 32 (14.4) | 16 (11.0) | 16 (20.5) | 0.054 |
| Obesity, n (%) 2 | 74 (33.2) | 50 (34.5) | 24 (30.8) | 0.574 |
| APACHE II, 24 h 3 | 16 (12–20) | 16 (12–19.5) | 18 (14–22) | 0.010 * |
| SOFA 3 | ||||
| 24 h | 7 (5–9) | 7 (5–8) | 8 (6–11) | 0.001 * |
| 48 h | 5 (3–7) | 5 (3–7) | 7 (5–8) | 0.000 * |
| 72 h | 4 (3–7) | 4 (2–6) | 6 (4–8) | 0.000 * |
| Corticosteroid use, n (%) 2 | 201 (90.1) | 131 (90.3) | 70 (89.7) | 0.886 |
| Heparin use, n (%) 2 | 172 (77.5) | 109 (75.2) | 63 (81.8) | 0.259 |
| Hospitalization, days 3 | 10 (6–15) | 10 (6–14) | 12.5 (6.8–16.3) | 0.129 |
| Inflammatory Markers | All Patients | Survivors | Non-Survivors | p-Value |
|---|---|---|---|---|
| (n = 223) | (n = 145) | (n = 78) | ||
| D-dimer 24 h, ng/mL | 1161 (751.6–2684.5) | 1055 (733.8–1910.8) | 1318 (821.5–3257) | 0.085 |
| D-dimer 48 h, ng/mL | 1227 (718–2704) | 1221.5 (691.8–2099.2) | 1311 (813–4290) | 0.108 |
| Ferritin 24 h, ng/mL | 1137 (668.5–1650) | 1040.5 (614.5–1650) | 1348.5 (874.6–1650) | 0.088 |
| Ferritin 48 h, ng/mL | 1140 (802–1500) | 1075.8 (690.4–1500) | 1187.1 (916.8–1500) | 0.136 |
| LDH 24 h, U/L | 820 (671.5–1001.5) | 773 (633–948) | 887 (745.3–1103.3) | 0.001 * |
| LDH 48 h, U/L | 686.5 (579–859.5) | 661 (559.8–820.8) | 770 (624.5–910.5) | 0.010 * |
| IL-6 24 h, pg/mL | 25.2 (12.2–65.1) | 21.6 (9.7–55.4) | 35.1 (15.0–107.0) | 0.001 * |
| Hematology Markers | All Patients | Survivors | Non-Survivors | p-Value |
|---|---|---|---|---|
| (n = 223) | (n = 145) | (n = 78) | ||
| MPV, 24 h | 8.9 (8.5–9.6) | 8.9 (8.5–9.5) | 8.9 (8.4–9.6) | 0.650 |
| MPV, 48 h | 8.9 (8.5–9.4) | 8.9 (8.5–9.4) | 9 (8.5–9.6) | 0.419 |
| MPV, 72 h | 9 (8.5–9.6) | 8.9 (8.6–9.5) | 9 (8.5–9.7) | 0.502 |
| Lymphocytes, 24 h (cells/mL) | 620 (410–900) | 660 (465–930) | 465 (340–712.5) | 0.000 * |
| Lymphocytes, 48 h (cells/mL) | 520 (400–820) | 620 (455–840) | 455 (290–607.5) | 0.000 * |
| Lymphocytes, 72 h (cells/mL) | 555 (350–882) | 630 (395–970) | 430 (300–600) | 0.000 * |
| NLR, 24 h | 15.6 (9.6–23.4) | 13.7 (8.4–20.1) | 21.7 (12.7–33.1) | 0.000 * |
| NLR, 48 h | 15.6 (9.8–22.7) | 13.1 (8.7–18.4) | 22.0 (14.3–29.5) | 0.000 * |
| NLR, 72 h | 15.4 (9.1–25.9) | 13.2 (7.8–21.3) | 20.6 (14.1–31.7) | 0.000 * |
| MPV/platelet, 24 h | 2.8 (2.2–3.6) | 2.7 (2.1–3.5) | 2.9 (2.4–4.1) | 0.052 |
| MPV/platelet, 48 h | 2.7 (2.1–3.6) | 2.6 (2–3.3) | 3.0 (2.3–4.3) | 0.004 * |
| MPV/platelet, 72 h | 2.7 (2.1–3.5) | 2.5 (2.0–3.3) | 3.1 (2.3–3.9) | 0.003 * |
| Variables | OR | 95% CI | p-Value |
|---|---|---|---|
| SOFA 24 h ≥ 8 | 1.0 | 0.4–2.8 | 0.990 |
| SOFA 48 h ≥ 6 | 1.1 | 0.3–3.8 | 0.825 |
| SOFA 72 h ≥ 4 | 1.7 | 0.5–5.7 | 0.395 |
| IL-6 24 h ≥ 11 ** | 8.3 | 1.5–44.6 | 0.014 * |
| LDH 24 h ≥ 781 | 1.7 | 0.6–4.4 | 0.301 |
| LDH 48 h ≥ 709 | 2.0 | 0.7–5.6 | 0.180 |
| NLR 24 h ≥ 22 ** | 3.8 | 1.3–10.9 | 0.015 * |
| NLR 48 h ≥ 18 | 0.8 | 0.3–2.5 | 0.746 |
| NLR 72 h ≥ 14 ** | 3.8 | 1.3–11.0 | 0.013 * |
| MPV/Platelets 48 h ≥ 4 | 1.6 | 0.4–6.1 | 0.470 |
| MPV/Platelets 72 h ≥ 3 | 1.4 | 0.5–4.0 | 0.480 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vélez-Páez, J.L.; Pelosi, P.; Battaglini, D.; Best, I. Biological Markers to Predict Outcome in Mechanically Ventilated Patients with Severe COVID-19 Living at High Altitude. J. Clin. Med. 2023, 12, 644. https://doi.org/10.3390/jcm12020644
Vélez-Páez JL, Pelosi P, Battaglini D, Best I. Biological Markers to Predict Outcome in Mechanically Ventilated Patients with Severe COVID-19 Living at High Altitude. Journal of Clinical Medicine. 2023; 12(2):644. https://doi.org/10.3390/jcm12020644
Chicago/Turabian StyleVélez-Páez, Jorge Luis, Paolo Pelosi, Denise Battaglini, and Ivan Best. 2023. "Biological Markers to Predict Outcome in Mechanically Ventilated Patients with Severe COVID-19 Living at High Altitude" Journal of Clinical Medicine 12, no. 2: 644. https://doi.org/10.3390/jcm12020644
APA StyleVélez-Páez, J. L., Pelosi, P., Battaglini, D., & Best, I. (2023). Biological Markers to Predict Outcome in Mechanically Ventilated Patients with Severe COVID-19 Living at High Altitude. Journal of Clinical Medicine, 12(2), 644. https://doi.org/10.3390/jcm12020644