
Dietary Inflammatory Index and All-Cause Mortality in Older Adults with Hypertension: Results from NHANES
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Exposure and Outcome Definitions
2.3. Covariates
2.4. Statistic Analysis
3. Results
3.1. Baseline Characteristics of Study Participants
3.2. Associations between DII and Mortality
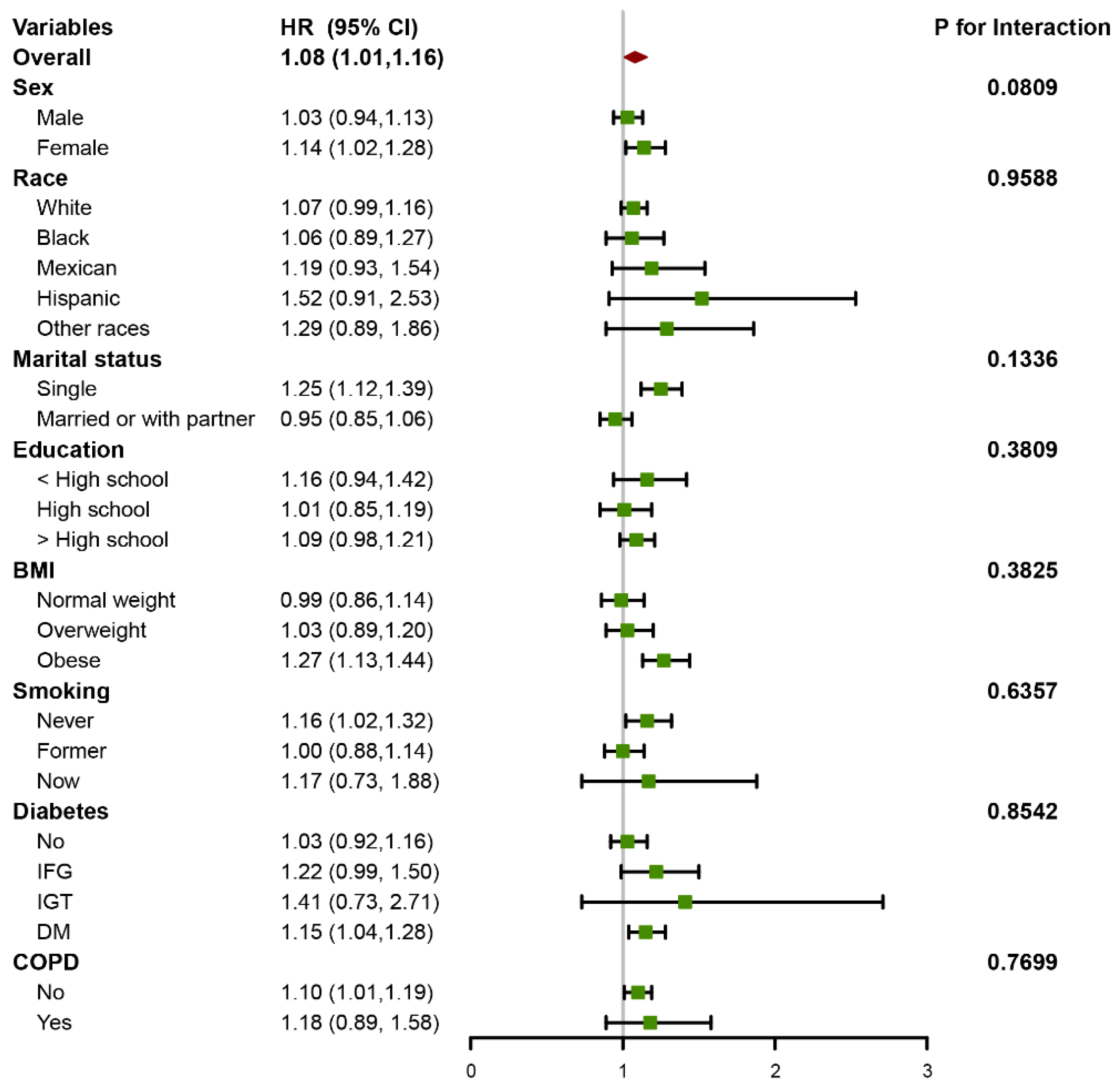
3.3. Subgroup Analyses and Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Ong, K.L.; Cheung, B.M.; Man, Y.B.; Lau, C.P.; Lam, K.S. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999–2004. Hypertension 2007, 49, 69–75. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Evans, J.C.; Levy, D. Hypertension in adults across the age spectrum: Current outcomes and control in the community. JAMA 2005, 294, 466–472. [Google Scholar] [CrossRef]
- Hebert, J.R.; Shivappa, N.; Wirth, M.D.; Hussey, J.R.; Hurley, T.G. Perspective: The Dietary Inflammatory Index (DII)-Lessons Learned, Improvements Made, and Future Directions. Adv. Nutr. 2019, 10, 185–195. [Google Scholar] [CrossRef]
- Cavicchia, P.P.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Hebert, J.R. A new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive protein. J. Nutr. 2009, 139, 2365–2372. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Wang, Y.B.; Shivappa, N.; Hebert, J.R.; Page, A.J.; Gill, T.K.; Melaku, Y.A. Association between Dietary Inflammatory Index, Dietary Patterns, Plant-Based Dietary Index and the Risk of Obesity. Nutrients 2021, 13, 1536. [Google Scholar] [CrossRef]
- Tan, Q.Q.; Du, X.Y.; Gao, C.L.; Xu, Y. Higher Dietary Inflammatory Index Scores Increase the Risk of Diabetes Mellitus: A Meta-Analysis and Systematic Review. Front. Endocrinol. 2021, 12, 693144. [Google Scholar] [CrossRef]
- Shivappa, N.; Godos, J.; Hebert, J.R.; Wirth, M.D.; Piuri, G.; Speciani, A.F.; Grosso, G. Dietary Inflammatory Index and Cardiovascular Risk and Mortality-A Meta-Analysis. Nutrients 2018, 10, 200. [Google Scholar] [CrossRef]
- Han, Y.Y.; Forno, E.; Shivappa, N.; Wirth, M.D.; Hebert, J.R.; Celedon, J.C. The Dietary Inflammatory Index and Current Wheeze Among Children and Adults in the United States. J. Allergy Clin. Immunol. Pract. 2018, 6, 834–841. [Google Scholar] [CrossRef]
- Fowler, M.E.; Akinyemiju, T.F. Meta-analysis of the association between dietary inflammatory index (DII) and cancer outcomes. Int. J. Cancer 2017, 141, 2215–2227. [Google Scholar] [CrossRef]
- Charisis, S.; Ntanasi, E.; Yannakoulia, M.; Anastasiou, C.A.; Kosmidis, M.H.; Dardiotis, E.; Gargalionis, A.N.; Patas, K.; Chatzipanagiotou, S.; Mourtzinos, I.; et al. Diet Inflammatory Index and Dementia Incidence: A Population-Based Study. Neurology 2021, 97, e2381–e2391. [Google Scholar] [CrossRef]
- Wirth, M.D.; Sevoyan, M.; Hofseth, L.; Shivappa, N.; Hurley, T.G.; Hebert, J.R. The Dietary Inflammatory Index is associated with elevated white blood cell counts in the National Health and Nutrition Examination Survey. Brain Behav. Immun. 2018, 69, 296–303. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018, 138, e426–e483. [Google Scholar] [CrossRef]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R., 3rd; Simons-Morton, D.G.; et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef]
- Filippou, C.D.; Thomopoulos, C.G.; Kouremeti, M.M.; Sotiropoulou, L.I.; Nihoyannopoulos, P.I.; Tousoulis, D.M.; Tsioufis, C.P. Mediterranean diet and blood pressure reduction in adults with and without hypertension: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2021, 40, 3191–3200. [Google Scholar] [CrossRef]
- Caillon, A.; Schiffrin, E.L. Role of Inflammation and Immunity in Hypertension: Recent Epidemiological, Laboratory, and Clinical Evidence. Curr. Hypertens. Rep. 2016, 18, 21. [Google Scholar] [CrossRef]
- MacDonald, C.J.; Laouali, N.; Madika, A.L.; Mancini, F.R.; Boutron-Ruault, M.C. Dietary inflammatory index, risk of incident hypertension, and effect modification from BMI. Nutr. J. 2020, 19, 62. [Google Scholar] [CrossRef]
- Curtin, L.R.; Mohadjer, L.K.; Dohrmann, S.M.; Kruszon-Moran, D.; Mirel, L.B.; Carroll, M.D.; Hirsch, R.; Burt, V.L.; Johnson, C.L. National Health and Nutrition Examination Survey: Sample design, 2007–2010. Vital. Health Stat 2 2013, 160, 1–23. [Google Scholar]
- Zipf, G.; Chiappa, M.; Porter, K.S.; Ostchega, Y.; Lewis, B.G.; Dostal, J. National health and nutrition examination survey: Plan and operations, 1999–2010. Vital Health Stat 1 2013, 56, 1–37. [Google Scholar]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hebert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef]
- Chen, T.C.; Clark, J.; Riddles, M.K.; Mohadjer, L.K.; Fakhouri, T.H.I. National Health and Nutrition Examination Survey, 2015–2018: Sample Design and Estimation Procedures. Vital Health Stat 2 2020, 184, 1–35. [Google Scholar]
- Madhur, M.S.; Elijovich, F.; Alexander, M.R.; Pitzer, A.; Ishimwe, J.; Van Beusecum, J.P.; Patrick, D.M.; Smart, C.D.; Kleyman, T.R.; Kingery, J.; et al. Hypertension: Do Inflammation and Immunity Hold the Key to Solving this Epidemic? Circ. Res. 2021, 128, 908–933. [Google Scholar] [CrossRef]
- Wang, T.J.; Gona, P.; Larson, M.G.; Levy, D.; Benjamin, E.J.; Tofler, G.H.; Jacques, P.F.; Meigs, J.B.; Rifai, N.; Selhub, J.; et al. Multiple biomarkers and the risk of incident hypertension. Hypertension 2007, 49, 432–438. [Google Scholar] [CrossRef]
- Jayedi, A.; Rahimi, K.; Bautista, L.E.; Nazarzadeh, M.; Zargar, M.S.; Shab-Bidar, S. Inflammation markers and risk of developing hypertension: A meta-analysis of cohort studies. Heart 2019, 105, 686–692. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Zhang, J.; Ma, Y.; Liese, A.D.; Agalliu, I.; Hingle, M.; Hou, L.; Hurley, T.G.; Jiao, L.; et al. Construct validation of the dietary inflammatory index among postmenopausal women. Ann. Epidemiol. 2015, 25, 398–405. [Google Scholar] [CrossRef]
- Shivappa, N.; Hebert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef]
- Steinberg, D.; Bennett, G.G.; Svetkey, L. The DASH Diet, 20 Years Later. JAMA 2017, 317, 1529–1530. [Google Scholar] [CrossRef]
- Wu, P.Y.; Chen, K.M.; Tsai, W.C. The Mediterranean Dietary Pattern and Inflammation in Older Adults: A Systematic Review and Meta-analysis. Adv. Nutr. 2021, 12, 363–373. [Google Scholar] [CrossRef]
- Ndanuko, R.N.; Tapsell, L.C.; Charlton, K.E.; Neale, E.P.; Batterham, M.J. Dietary Patterns and Blood Pressure in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2016, 7, 76–89. [Google Scholar] [CrossRef]
- Mell, B.; Jala, V.R.; Mathew, A.V.; Byun, J.; Waghulde, H.; Zhang, Y.; Haribabu, B.; Vijay-Kumar, M.; Pennathur, S.; Joe, B. Evidence for a link between gut microbiota and hypertension in the Dahl rat. Physiol. Genom. 2015, 47, 187–197. [Google Scholar] [CrossRef]
- Zhernakova, A.; Kurilshikov, A.; Bonder, M.J.; Tigchelaar, E.F.; Schirmer, M.; Vatanen, T.; Mujagic, Z.; Vila, A.V.; Falony, G.; Vieira-Silva, S.; et al. Population-based metagenomics analysis reveals markers for gut microbiome composition and diversity. Science 2016, 352, 565–569. [Google Scholar] [CrossRef]
- Bartolomaeus, H.; Balogh, A.; Yakoub, M.; Homann, S.; Marko, L.; Hoges, S.; Tsvetkov, D.; Krannich, A.; Wundersitz, S.; Avery, E.G.; et al. Short-Chain Fatty Acid Propionate Protects From Hypertensive Cardiovascular Damage. Circulation 2019, 139, 1407–1421. [Google Scholar] [CrossRef]
- Ge, X.; Zheng, L.; Zhuang, R.; Yu, P.; Xu, Z.; Liu, G.; Xi, X.; Zhou, X.; Fan, H. The Gut Microbial Metabolite Trimethylamine N-Oxide and Hypertension Risk: A Systematic Review and Dose-Response Meta-analysis. Adv. Nutr. 2020, 11, 66–76. [Google Scholar] [CrossRef]
- Poll, B.G.; Cheema, M.U.; Pluznick, J.L. Gut Microbial Metabolites and Blood Pressure Regulation: Focus on SCFAs and TMAO. Physiology 2020, 35, 275–284. [Google Scholar] [CrossRef]
- Zmora, N.; Suez, J.; Elinav, E. You are what you eat: Diet, health and the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 35–56. [Google Scholar] [CrossRef]
- Wang, D.D.; Nguyen, L.H.; Li, Y.; Yan, Y.; Ma, W.; Rinott, E.; Ivey, K.L.; Shai, I.; Willett, W.C.; Hu, F.B.; et al. The gut microbiome modulates the protective association between a Mediterranean diet and cardiometabolic disease risk. Nat. Med. 2021, 27, 333–343. [Google Scholar] [CrossRef]
- Rinott, E.; Meir, A.Y.; Tsaban, G.; Zelicha, H.; Kaplan, A.; Knights, D.; Tuohy, K.; Scholz, M.U.; Koren, O.; Stampfer, M.J.; et al. The effects of the Green-Mediterranean diet on cardiometabolic health are linked to gut microbiome modifications: A randomized controlled trial. Genome Med. 2022, 14, 29. [Google Scholar] [CrossRef]
- Ravindrarajah, R.; Hazra, N.C.; Hamada, S.; Charlton, J.; Jackson, S.H.D.; Dregan, A.; Gulliford, M.C. Systolic Blood Pressure Trajectory, Frailty, and All-Cause Mortality >80 Years of Age: Cohort Study Using Electronic Health Records. Circulation 2017, 135, 2357–2368. [Google Scholar] [CrossRef]
- Marcos-Perez, D.; Sanchez-Flores, M.; Proietti, S.; Bonassi, S.; Costa, S.; Teixeira, J.P.; Fernandez-Tajes, J.; Pasaro, E.; Laffon, B.; Valdiglesias, V. Association of inflammatory mediators with frailty status in older adults: Results from a systematic review and meta-analysis. Geroscience 2020, 42, 1451–1473. [Google Scholar] [CrossRef]
- Resciniti, N.V.; Lohman, M.C.; Wirth, M.D.; Shivappa, N.; Hebert, J.R. Dietary Inflammatory Index, Pre-Frailty and Frailty among Older US Adults: Evidence from the National Health and Nutrition Examination Survey, 2007–2014. J. Nutr. Health Aging 2019, 23, 323–329. [Google Scholar] [CrossRef]
- Jayanama, K.; Theou, O.; Godin, J.; Cahill, L.; Shivappa, N.; Hebert, J.R.; Wirth, M.D.; Park, Y.M.; Fung, T.T.; Rockwood, K. Relationship between diet quality scores and the risk of frailty and mortality in adults across a wide age spectrum. BMC Med. 2021, 19, 64. [Google Scholar] [CrossRef]
- Walker, K.A.; Sharrett, A.R.; Wu, A.; Schneider, A.L.C.; Albert, M.; Lutsey, P.L.; Bandeen-Roche, K.; Coresh, J.; Gross, A.L.; Windham, B.G.; et al. Association of Midlife to Late-Life Blood Pressure Patterns With Incident Dementia. JAMA 2019, 322, 535–545. [Google Scholar] [CrossRef]
- Ou, Y.N.; Tan, C.C.; Shen, X.N.; Xu, W.; Hou, X.H.; Dong, Q.; Tan, L.; Yu, J.T. Blood Pressure and Risks of Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of 209 Prospective Studies. Hypertension 2020, 76, 217–225. [Google Scholar] [CrossRef]
- O’Donnell, M.; Mente, A.; Yusuf, S. Sodium intake and cardiovascular health. Circ. Res. 2015, 116, 1046–1057. [Google Scholar] [CrossRef]
- Filippini, T.; Violi, F.; D’Amico, R.; Vinceti, M. The effect of potassium supplementation on blood pressure in hypertensive subjects: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 230, 127–135. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | DII < 0 | DII > 0 | p-Value |
|---|---|---|---|---|
| Age, years | 73.06 ± 0.15 | 72.58 ± 0.30 | 73.20 ± 0.17 | 0.071 |
| RIP | 2.98 ± 0.07 | 3.45 ± 0.12 | 2.84 ± 0.06 | <0.001 |
| HbA1c, % | 6.04 ± 0.02 | 5.97 ± 0.05 | 6.06 ± 0.03 | 0.132 |
| ALT, IU/L | 21.66 ± 0.33 | 22.71 ± 0.93 | 21.35 ± 0.35 | 0.187 |
| AST, IU/L | 24.65 ± 0.32 | 25.15 ± 0.81 | 24.49 ± 0.38 | 0.493 |
| Cr, mg/dL | 1.03 ± 0.01 | 0.98 ± 0.02 | 1.04 ± 0.01 | 0.004 |
| UA, mg/dL | 5.76 ± 0.04 | 5.73 ± 0.09 | 5.77 ± 0.04 | 0.658 |
| TG, mg/dL | 157.69 ± 2.74 | 153.18 ± 5.82 | 159.04 ± 3.34 | 0.414 |
| TC, mg/dL | 186.24 ± 1.33 | 178.77 ± 2.71 | 188.48 ± 1.51 | 0.003 |
| Sodium, mg/day | 3057.03 ± 36.85 | 3757.25 ± 113.52 | 2847.15 ± 29.32 | <0.001 |
| Potassium, mg/day | 2573.34 ± 26.14 | 3429.53 ± 63.18 | 2316.71 ± 25.57 | <0.001 |
| eGFR, mL/min/1.73 m2 | 68.73 ± 0.42 | 72.15 ± 0.95 | 67.71 ± 0.46 | <0.001 |
| Sex, n (%) | <0.001 | |||
| Male | 1208 (47.73) | 314 (56.23) | 894 (38.74) | <0.001 |
| Female | 1323 (52.27) | 207 (43.77) | 1116 (61.26) | |
| Race, n (%) | ||||
| White | 1340 (52.94) | 281 (82.64) | 1059 (79.66) | 0.002 |
| Black | 535 (21.14) | 89 (5.73) | 446 (8.83) | |
| Mexican | 214 (8.46) | 48 (3.09) | 166 (3.22) | |
| Hispanic | 228 (9.01) | 34 (2.08) | 194 (3.77) | |
| Other races | 214 (8.46) | 69 (6.46) | 145 (4.53) | |
| Marital status, n (%) | ||||
| Single | 1136 (44.88) | 180 (29.24) | 956 (42.18) | <0.001 |
| Married or with partner | 1395 (55.12) | 341 (70.76) | 1054 (57.82) | |
| Education, n (%) | ||||
| <High school | 634 (25.05) | 104 (11.96) | 530 (18.30) | 0.002 |
| High school | 627 (24.77) | 107 (21.71) | 520 (26.68) | |
| >High school | 1270 (50.18) | 310 (66.33) | 960 (55.02) | |
| BMI, n (%) | ||||
| Normal weight | 565 (22.32) | 141 (24.44) | 424 (20.15) | 0.243 |
| Overweight | 924 (36.51) | 194 (36.66) | 730 (36.94) | |
| Obese | 1042 (41.17) | 186 (38.90) | 856 (42.92) | |
| Smoke, n (%) | ||||
| Never | 1240 (48.99) | 254 (44.90) | 986 (49.95) | 0.057 |
| Former | 1060 (41.88) | 234 (50.09) | 826 (42.85) | |
| Now | 231 (9.13) | 33 (5.01) | 198 (7.20) | |
| Hyperlipidemia, n (%) | ||||
| No | 376 (14.86) | 94 (14.75) | 282 (11.67) | 0.147 |
| Yes | 2155 (85.14) | 427 (85.25) | 1728 (88.33) | |
| Diabetes, n (%) | ||||
| No | 1256 (49.62) | 277 (54.97) | 979 (52.22) | 0.261 |
| IFG | 162 (6.4) | 38 (10.91) | 124 (8.25) | |
| IGT | 124 (4.9) | 22 (3.48) | 102 (4.50) | |
| DM | 989 (39.08) | 184 (30.64) | 805 (35.03) | |
| COPD, n (%) | ||||
| No | 2318 (91.58) | 484 (92.57) | 1834 (90.54) | 0.291 |
| Yes | 213 (8.42) | 37 (7.43) | 176 (9.46) | |
| Status, n (%) | ||||
| Alive | 2060 (81.39) | 447 (88.43) | 1613 (81.97) | 0.002 |
| Death | 471 (18.61) | 74 (11.57) | 397 (18.03) |
| DII | Model 1 HR (95% CI) | Model 2 HR (95% CI) | Model 3 HR (95% CI) |
|---|---|---|---|
| Continuous | 1.12 (1.05–1.19) | 1.11 (1.04–1.18) | 1.08 (1.01–1.16) |
| DII < 0 | Ref = 1.00 | Ref = 1.00 | Ref = 1.00 |
| DII > 1 | 1.64 (1.25–2.16) | 1.62 (1.21–2.16) | 1.54 (1.13–2.10) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, Y.; Li, P.; Zhang, Y.; Qiu, M.; Li, J.; Ma, S.; Yan, Y.; Li, Y.; Han, Y. Dietary Inflammatory Index and All-Cause Mortality in Older Adults with Hypertension: Results from NHANES. J. Clin. Med. 2023, 12, 506. https://doi.org/10.3390/jcm12020506
Cao Y, Li P, Zhang Y, Qiu M, Li J, Ma S, Yan Y, Li Y, Han Y. Dietary Inflammatory Index and All-Cause Mortality in Older Adults with Hypertension: Results from NHANES. Journal of Clinical Medicine. 2023; 12(2):506. https://doi.org/10.3390/jcm12020506
Chicago/Turabian StyleCao, Yang, Pengxiao Li, Yan Zhang, Miaohan Qiu, Jing Li, Sicong Ma, Yudong Yan, Yi Li, and Yaling Han. 2023. "Dietary Inflammatory Index and All-Cause Mortality in Older Adults with Hypertension: Results from NHANES" Journal of Clinical Medicine 12, no. 2: 506. https://doi.org/10.3390/jcm12020506
APA StyleCao, Y., Li, P., Zhang, Y., Qiu, M., Li, J., Ma, S., Yan, Y., Li, Y., & Han, Y. (2023). Dietary Inflammatory Index and All-Cause Mortality in Older Adults with Hypertension: Results from NHANES. Journal of Clinical Medicine, 12(2), 506. https://doi.org/10.3390/jcm12020506