

The Impact of Recirculation on Extracorporeal Gas Exchange and Patient Oxygenation during Veno-Venous Extracorporeal Membrane Oxygenation—Results of an Observational Clinical Trial


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. ECMO Management and Patient Interventions
2.3. Patient Monitoring and Gas-Transfer Calculation
2.4. Recirculation Measurement and Protocol
2.5. Outcome Measures
2.6. Data Collection and Statistical Analysis
3. Results
3.1. ECMO Flow and Recirculation
3.2. Recirculation and ECMO Oxygenator Transfer
3.3. ECMO Blood Flow, Recirculation, ECMO Oxygen Delivery and Arterial Patient Saturation
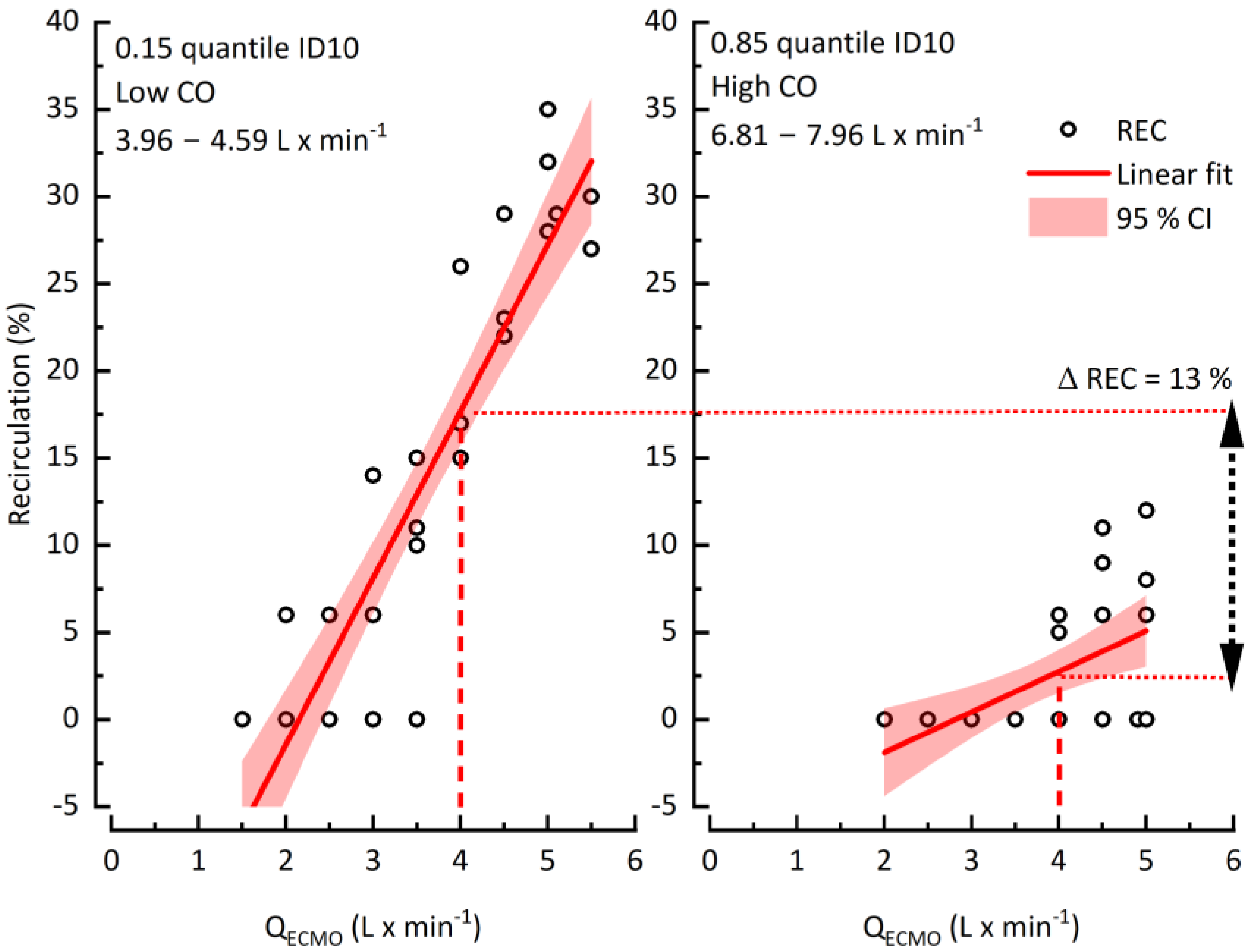
3.4. Cardiac Output and Its Impact on Recirculation
4. Discussion
4.1. Recirculation, Gas Transfer and Patient Oxygenation
4.2. Recirculation and Patient CO
4.3. Clinical Relevance
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frenckner, B.; Palmer, P.; Linden, V. Extracorporeal respiratory support and minimally invasive ventilation in severe ARDS. Minerva Anestesiol. 2002, 68, 381–386. [Google Scholar] [PubMed]
- Charbit, J.; Deras, P.; Courvalin, E.; Laumon, T.; Dagod, G.; Martinez, O.; Capdevila, X. Structural recirculation and refractory hypoxemia under femoro-jugular veno-venous extracorporeal membrane oxygenation. Artif. Organs 2021, 45, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Taccone, F.S.; Guarracino, F. Recent developments in the management of persistent hypoxemia under veno-venous ECMO. Intensive Care Med. 2015, 41, 508–510. [Google Scholar] [CrossRef]
- Messai, E.; Bouguerra, A.; Guarracino, F.; Bonacchi, M. Low Blood Arterial Oxygenation During Venovenous Extracorporeal Membrane Oxygenation: Proposal for a Rational Algorithm-Based Management. J. Intensive Care Med. 2016, 31, 553–560. [Google Scholar] [CrossRef]
- Xie, A.; Yan, T.D.; Forrest, P. Recirculation in venovenous extracorporeal membrane oxygenation. J. Crit. Care 2016, 36, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Fortenberry, J.D.; Pettignano, R.; Dykes, F. Principles and Practice of venovenous ECMO. In ECMO Extracorporeal Cardiopulmonary Support in Critical Care, 3rd ed.; Van Meurs, K., Lally, K.P., Peek, G., Zwischenberger, J.B., Eds.; ELSO Extracorporeal Life Support Organisation: Ann Arbor, MI, USA, 2005. [Google Scholar]
- Schmidt, M.; Tachon, G.; Devilliers, C.; Muller, G.; Hekimian, G.; Brechot, N.; Merceron, S.; Luyt, C.E.; Trouillet, J.L.; Chastre, J.; et al. Blood oxygenation and decarboxylation determinants during venovenous ECMO for respiratory failure in adults. Intensive Care Med. 2013, 39, 838–846. [Google Scholar] [CrossRef]
- Broman, M.; Frenckner, B.; Bjallmark, A.; Broome, M. Recirculation during veno-venous extra-corporeal membrane oxygenation—A simulation study. Int. J. Artif. Organs 2015, 38, 23–30. [Google Scholar] [CrossRef]
- Locker, G.J.; Losert, H.; Schellongowski, P.; Thalhammer, F.; Knapp, S.; Laczika, K.F.; Burgmann, H.; Staudinger, T.; Frass, M.; Muhm, M. Bedside exclusion of clinically significant recirculation volume during venovenous ECMO using conventional blood gas analyses. J. Clin. Anesth. 2003, 15, 441–445. [Google Scholar] [CrossRef]
- Sreenan, C.; Osiovich, H.; Cheung, P.Y.; Lemke, R.P. Quantification of recirculation by thermodilution during venovenous extracorporeal membrane oxygenation. J. Pediatr. Surg. 2000, 35, 1411–1414. [Google Scholar] [CrossRef]
- Clements, D.; Primmer, J.; Ryman, P.; Marr, B.; Searles, B.; Darling, E. Measurements of recirculation during neonatal veno-venous extracorporeal membrane oxygenation: Clinical application of the ultrasound dilution technique. J. Extra-Corpor. Technol. 2008, 40, 184–187. [Google Scholar]
- Darling, E.M.; Crowell, T.; Searles, B.E. Use of dilutional ultrasound monitoring to detect changes in recirculation during venovenous extracorporeal membrane oxygenation in swine. ASAIO J. 2006, 52, 522–524. [Google Scholar] [CrossRef]
- van Heijst, A.F.; van der Staak, F.H.; de Haan, A.F.; Liem, K.D.; Festen, C.; Geven, W.B.; van de Bor, M. Recirculation in double lumen catheter veno-venous extracorporeal membrane oxygenation measured by an ultrasound dilution technique. ASAIO J. 2001, 47, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.; Primmer, J.; Searles, B.E.; Darling, E.M. The potential of accurate SvO2 monitoring during venovenous extracorporeal membrane oxygenation: An in vitro model using ultrasound dilution. Perfusion 2007, 22, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.L.; Gelfond, J.; Zarzabal, L.A.; Darling, E. Calculating mixed venous saturation during veno-venous extracorporeal membrane oxygenation. Perfusion 2009, 24, 333–339. [Google Scholar] [CrossRef]
- Nunes, L.B.; Mendes, P.V.; Hirota, A.S.; Barbosa, E.V.; Maciel, A.T.; Schettino, G.P.P.; Costa, E.L.V.; Azevedo, L.C.P.; Park, M.; Group, E. Severe hypoxemia during veno-venous extracorporeal membrane oxygenation: Exploring the limits of extracorporeal respiratory support. Clinics 2014, 69, 173–178. [Google Scholar] [CrossRef]
- Zanella, A.; Salerno, D.; Scaravilli, V.; Giani, M.; Castagna, L.; Magni, F.; Carlesso, E.; Cadringher, P.; Bombino, M.; Grasselli, G.; et al. A mathematical model of oxygenation during venovenous extracorporeal membrane oxygenation support. J. Crit. Care 2016, 36, 178–186. [Google Scholar] [CrossRef]
- Ferguson, N.D.; Fan, E.; Camporota, L.; Antonelli, M.; Anzueto, A.; Beale, R.; Brochard, L.; Brower, R.; Esteban, A.; Gattinoni, L.; et al. The Berlin definition of ARDS: An expanded rationale, justification, and supplementary material. Intensive Care Med. 2012, 38, 1573–1582. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Tonetti, T.; Quintel, M. How best to set the ventilator on extracorporeal membrane lung oxygenation. Curr. Opin. Crit. Care 2017, 23, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Terragni, P.P.; Del Sorbo, L.; Mascia, L.; Urbino, R.; Martin, E.L.; Birocco, A.; Faggiano, C.; Quintel, M.; Gattinoni, L.; Ranieri, V.M. Tidal Volume Lower than 6 ml/kg Enhances Lung Protection Role of Extracorporeal Carbon Dioxide Removal. Anesthesiology 2009, 111, 826–835. [Google Scholar] [CrossRef]
- Haller, M.; Zollner, C.; Manert, W.; Briegel, J.; Kilger, E.; Polasek, J.; Hummel, T.; Forst, H.; Peter, K. Thermodilution cardiac output may be incorrect in patients on venovenous extracorporeal lung assist. Am. J. Respir. Crit. Care Med. 1995, 152, 1812–1817. [Google Scholar] [CrossRef]
- Tonna, J.E.; Abrams, D.; Brodie, D.; Greenwood, J.C.; RUBIO Mateo-Sidron, J.A.; Usman, A.; Fan, E. Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO J. 2021, 67, 601–610. [Google Scholar] [CrossRef]
- Togo, K.; Takewa, Y.; Katagiri, N.; Fujii, Y.; Kishimoto, S.; Date, K.; Miyamoto, Y.; Tatsumi, E. Impact of bypass flow rate and catheter position in veno-venous extracorporeal membrane oxygenation on gas exchange in vivo. J. Artif. Organs 2015, 18, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Bliss, D. Refinement of a novel empirical formula to determine the “true” mixed venous saturation in patients undergoing veno-venous extracorporeal life support. ASAIO J. 2010, 56, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Bliss, D.W.; Chambers, S.; Fazzalari, F.; Hirschl, R.; Bartlett, R.H. Determination of native mixed venous saturation during venovenous extracorporeal circulation. ASAIO J. 1995, 41, 838–841. [Google Scholar] [CrossRef]
- Messai, E.; Bouguerra, A.; Harmelin, G.; Di Lascio, G.; Cianchi, G.; Bonacchi, M. A new formula for determining arterial oxygen saturation during venovenous extracorporeal oxygenation. Intensive Care Med. 2013, 39, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Costa, E.L.; Maciel, A.T.; Silva, D.P.; Friedrich, N.; Barbosa, E.V.; Hirota, A.S.; Schettino, G.; Azevedo, L.C. Determinants of oxygen and carbon dioxide transfer during extracorporeal membrane oxygenation in an experimental model of multiple organ dysfunction syndrome. PLoS ONE 2013, 8, e54954. [Google Scholar] [CrossRef]
- Russ, M.; Steiner, E.; Boemke, W.; Busch, T.; Melzer-Gartzke, C.; Taher, M.; Badulak, J.; Weber-Carstens, S.; Swenson, E.R.; Francis, R.C.E.; et al. Extracorporeal Membrane Oxygenation Blood Flow and Blood Recirculation Compromise Thermodilution-Based Measurements of Cardiac Output. ASAIO J. 2022, 68, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Saugel, B.; Kouz, K.; Scheeren, T.W.L.; Greiwe, G.; Hoppe, P.; Romagnoli, S.; de Backer, D. Cardiac output estimation using pulse wave analysis—Physiology, algorithms, and technologies: A narrative review. Br. J. Anaesth. 2021, 126, 67–76. [Google Scholar] [CrossRef]
- Slagt, C.; Malagon, I.; Groeneveld, A.B. Systematic review of uncalibrated arterial pressure waveform analysis to determine cardiac output and stroke volume variation. Br. J. Anaesth. 2014, 112, 626–637. [Google Scholar] [CrossRef]
- Bond, O.; Pozzebon, S.; Franchi, F.; Zama Cavicchi, F.; Creteur, J.; Vincent, J.L.; Taccone, F.S.; Scolletta, S. Comparison of estimation of cardiac output using an uncalibrated pulse contour method and echocardiography during veno-venous extracorporeal membrane oxygenation. Perfusion 2020, 35, 397–401. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gehron, J.; Bandorski, D.; Mayer, K.; Böning, A. The Impact of Recirculation on Extracorporeal Gas Exchange and Patient Oxygenation during Veno-Venous Extracorporeal Membrane Oxygenation—Results of an Observational Clinical Trial. J. Clin. Med. 2023, 12, 416. https://doi.org/10.3390/jcm12020416
Gehron J, Bandorski D, Mayer K, Böning A. The Impact of Recirculation on Extracorporeal Gas Exchange and Patient Oxygenation during Veno-Venous Extracorporeal Membrane Oxygenation—Results of an Observational Clinical Trial. Journal of Clinical Medicine. 2023; 12(2):416. https://doi.org/10.3390/jcm12020416
Chicago/Turabian StyleGehron, Johannes, Dirk Bandorski, Konstantin Mayer, and Andreas Böning. 2023. "The Impact of Recirculation on Extracorporeal Gas Exchange and Patient Oxygenation during Veno-Venous Extracorporeal Membrane Oxygenation—Results of an Observational Clinical Trial" Journal of Clinical Medicine 12, no. 2: 416. https://doi.org/10.3390/jcm12020416
APA StyleGehron, J., Bandorski, D., Mayer, K., & Böning, A. (2023). The Impact of Recirculation on Extracorporeal Gas Exchange and Patient Oxygenation during Veno-Venous Extracorporeal Membrane Oxygenation—Results of an Observational Clinical Trial. Journal of Clinical Medicine, 12(2), 416. https://doi.org/10.3390/jcm12020416