

Efficiency and Impact of Hypnoanalgesia for Cardiac Catheterisation in Paediatric Population
 , ,
, ,
Abstract
:1. Introduction
2. Objective
3. Methods
3.1. Study Design and Population
3.2. Hospitalisation Management
3.3. Study Outcomes
3.4. Statistics
4. Results
4.1. Patient Data (Table 1)

{kind=link}
| Patients | Age (years) | Sex | Weight (kg) | Procedure Indication | Hypnosis Indication | Anxiety before Procedure | Clinical Hypnosis Success | Patient/ Family Satisfaction | ANI Score (mean) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 16 | F | 48 | ASD closure | Family choice | Low | Yes | Neutral | 49 |
| 2 | 8 | M | 21 | Diagnostic catheterisation/pulmonary hypertension | Reliable haemodynamic assessment | Moderate | Yes | Yes | |
| 3 | 7 | F | 18 | ASD closure | Family choice | Important | Yes | Yes | 86 |
| 4 | 11 | M | 48 | Diagnostic catheterisation/pulmonary hypertension | GACI | - | Yes | Yes | 75 |
| 5 | 16 | F | 74 | ASD closure | Family choice | Important | Yes | Yes | 52 |
| 6 | 4 | M | 20 | PDA closure | Family choice | Low | Yes | Yes | 70 |
| 7 | 16 | F | 50 | Coronarography | GACI | Moderate | Yes | Yes | 69 |
| 8 | 7 | F | 21 | ASD closure | Family choice | Low | Yes | Yes | 92 |
| 9 | 12 | F | 43 | Diagnostic catheterisation/aortic coarctation | Reliable haemodynamic assessment | Low | Yes | Yes | 67 |
| 10 | 16 | M | 79 | Electrostimulation procedure | Family choice | Low | Yes | Yes | |
| 11 | 4 | M | 15 | PDA closure | Family choice | Moderate | No | No answer | |
| 12 | 8 | F | 46 | Diagnostic catheterisation/anomalous pulmonary venous return/aortic coarctation | Reliable haemodynamic assessment/GACI | Low | Yes | Yes | 79 |
| 13 | 14 | F | 25 | Diagnostic catheterisation/Fontan failure | Reliable haemodynamic assessment/GACI | - | Yes | Yes | 88 |
| 14 | 12 | F | 47 | PDA closure | Family choice | - | Yes | No answer | 64 |
| 15 | 6 | M | 19 | ASD closure | Family choice | Low | Yes | Yes | 81 |
| 16 | 11 | M | 30 | ASD closure | Family choice | Low | Yes | Yes | 97 |
4.2. Feasibility and Security
4.3. Efficiency
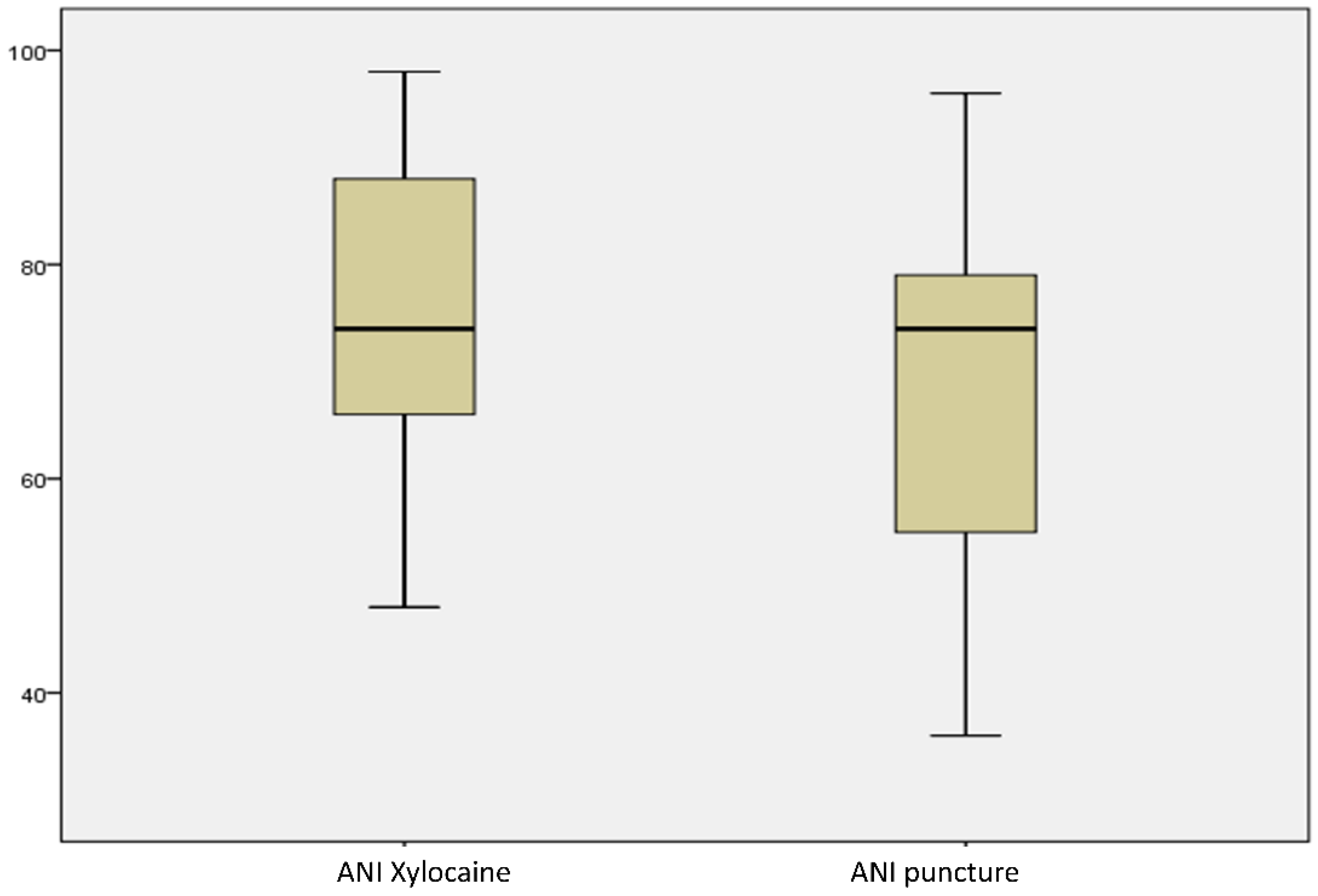
4.4. Effectiveness of the Hypnoanalgesia on Pain Control
5. Discussion
5.1. Feasibility and Safety of CC under Hypnoanalgesia
5.2. Efficiency of the Hypnoanalgesia in the Haemodynamic Assessment
5.3. Efficiency of the Hypnoanalgesia in Pain and Stress Management
5.4. Hypnoanalgesia Limits
5.5. Study Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CC | cardiac catheterisation |
| GA | general anaesthesia |
| VAS | visual analogue scale |
| ANI | analgesia nociception index |
| ASD | atrial septal defect |
| PDA | persistent ductus arteriosus |
References
- Schneuer, F.J.; Bentley, J.P.; Davidson, A.J.; Holland, A.J.; Badawi, N.; Martin, A.J.; Skowno, J.; Lain, S.J.; Nassar, N. The impact of general anesthesia on child development and school performance: A population-based study. Paediatr. Anaesth. 2018, 28, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Andropoulos, D.B. Effect of Anesthesia on the Developing Brain: Infant and Fetus. Fetal Diagn. Ther. 2018, 43, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Quinn, B.P.; Yeh, M.; Gauvreau, K.; Ali, F.; Balzer, D.; Barry, O.; Batlivala, S.; Berman, D.; Foerster, S.; Goldstein, B.; et al. Procedural Risk in Congenital Cardiac Catheterization (PREDIC3T). J. Am. Heart Assoc. 2022, 11, e022832. [Google Scholar] [CrossRef] [PubMed]
- Hansmann, G.; Koestenberger, M.; Alastalo, T.P.; Apitz, C.; Austin, E.D.; Bonnet, D.; Budts, W.; D’Alto, M.; Gatzoulis, M.A.; Hasan, B.S.; et al. 2019 updated consensus statement on the diagnosis and treatment of pediatric pulmonary hypertension: The European Pediatric Pulmonary Vascular Disease Network (EPPVDN), endorsed by AEPC, ESPR and ISHLT. J. Heart Lung Transplant. 2019, 38, 879–901. [Google Scholar] [CrossRef] [PubMed]
- Gorczyca, R.; Filip, R.; Walczak, E. Psychological aspects of pain. Ann. Agric. Environ. Med. 2013, 23–27. [Google Scholar]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: What do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef]
- Logier, R.; Jeanne, M.; De Jonckheere, J.; Dassonneville, A.; Delecroix, M.; Tavernier, B. PhysioDoloris: A monitoring device for analgesia/nociception balance evaluation using heart rate variability analysis. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentna, 31 August–4 September 2010; Volume 2010, pp. 1194–1197. [Google Scholar] [CrossRef]
- Boselli, E.; Daniela-Ionescu, M.; Bégou, G.; Bouvet, L.; Dabouz, R.; Magnin, C.; Allaouchiche, B. Prospective observational study of the non-invasive assessment of immediate postoperative pain using the analgesia/nociception index (ANI). Br. J. Anaesth. 2013, 111, 453–459. [Google Scholar] [CrossRef]
- Sawni, A.; Breuner, C.C. Clinical Hypnosis, an Effective Mind-Body Modality for Adolescents with Behavioral and Physical Complaints. Children 2017, 4, 19. [Google Scholar] [CrossRef]
- Lee, A.; Moulton, D.; Mckernan, L.; Russell, A.; Slaughter, J.C.; Acra, S.; Walker, L. Clinical Hypnosis in Pediatric Crohn’s Disease: A Randomized Controlled Pilot Study. J. Pediatr. Gastroenterol. Nutr. 2021, 72, e63–e70. [Google Scholar] [CrossRef] [PubMed]
- Lang, E.V.; Rosen, M.P. Cost analysis of adjunct hypnosis with sedation during outpatient interventional radiologic procedures. Radiology 2002, 222, 375–382. [Google Scholar] [CrossRef]
- Amedro, P.; Gavotto, A.; Gelibert, D.; Fraysse, V.; De La Villeon, G.; Vandenberghe, D.A.; Bredy, C. Feasibility of clinical hypnosis for transesophageal echocardiography in children and adolescents. Eur. J. Cardiovasc. Nurs. 2019, 18, 163–170. [Google Scholar] [CrossRef]
- Sriwatanakul, K.; Kelvie, W.; Lasagna, L.; Calimlim, J.F.; Weis, O.F.; Mehta, G. Studies with different types of visual analog scales for measurement of pain. Clin. Pharmacol. Ther. 1983, 34, 234–239. [Google Scholar] [CrossRef]
- Kang, S.L.; Benson, L. Recent advances in cardiac catheterization for congenital heart disease. F1000Reserach 2018, 7, 370. [Google Scholar] [CrossRef]
- Takahashi, M.; Mouillet, G.; Khaled, A.; Boukantar, M.; Gallet, R.; Rubimbura, V.; Lim, P.; Dubois-Rande, J.L.; Teiger, E. Perioperative Outcomes of Adjunctive Hypnotherapy Compared with Conscious Sedation Alone for Patients Undergoing Transfemoral Transcatheter Aortic Valve Implantation. Int. Heart J. 2020, 61, 60–66. [Google Scholar] [CrossRef]
- Cong, X.; Wu, J.; Vittner, D.; Xu, W.; Hussain, N.; Galvin, S.; Fitzsimons, M.; McGrath, J.M.; Henderson, W.A. The impact of cumulative pain/stress on neurobehavioral development of preterm infants in the NICU. Early Hum. Dev. 2017, 108, 9–16. [Google Scholar] [CrossRef]
- Palabiyik, O.; Demir, G. Chronic Pain after Open Appendectomy and Its Effects on Quality of Life in Children Aged 8–18 Years. Pain. Res. Manag. 2021, 2021, 6643714. [Google Scholar] [CrossRef]
- Amedro, P.; Dorka, R.; Moniotte, S.; Guillaumont, S.; Fraisse, A.; Kreitmann, B.; Borm, B.; Bertet, H.; Barréa, C.; Ovaert, C.; et al. Quality of Life of Children with Congenital Heart Diseases: A Multicenter Controlled Cross-Sectional Study. Pediatr. Cardiol. 2015, 36, 1588–1601. [Google Scholar] [CrossRef]
- Linton, S.J.; Shaw, W.S. Impact of psychological factors in the experience of pain. Phys. Ther. 2011, 91, 700–711. [Google Scholar] [CrossRef] [PubMed]
| Patient/Family Satisfaction | Number |
|---|---|
| Very satisfied or satisfied | 13 |
| Neutral | 1 |
| Not satisfied | 0 |
| No answer | 2 |
| Total | 16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fontanges, P.-A.; Haudiquet, J.; De Jonkheere, J.; Delarue, A.; Domanski, O.; Rakza, T.; Hascoet, S.; Bichali, S.; Baudelet, J.B.; Godart, F.; et al. Efficiency and Impact of Hypnoanalgesia for Cardiac Catheterisation in Paediatric Population. J. Clin. Med. 2023, 12, 6410. https://doi.org/10.3390/jcm12196410
Fontanges P-A, Haudiquet J, De Jonkheere J, Delarue A, Domanski O, Rakza T, Hascoet S, Bichali S, Baudelet JB, Godart F, et al. Efficiency and Impact of Hypnoanalgesia for Cardiac Catheterisation in Paediatric Population. Journal of Clinical Medicine. 2023; 12(19):6410. https://doi.org/10.3390/jcm12196410
Chicago/Turabian StyleFontanges, Pierre-Alexandre, Julien Haudiquet, Julien De Jonkheere, Alexandre Delarue, Olivia Domanski, Thameur Rakza, Sebastien Hascoet, Said Bichali, Jean Benoit Baudelet, Francois Godart, and et al. 2023. "Efficiency and Impact of Hypnoanalgesia for Cardiac Catheterisation in Paediatric Population" Journal of Clinical Medicine 12, no. 19: 6410. https://doi.org/10.3390/jcm12196410
APA StyleFontanges, P.-A., Haudiquet, J., De Jonkheere, J., Delarue, A., Domanski, O., Rakza, T., Hascoet, S., Bichali, S., Baudelet, J. B., Godart, F., & Houeijeh, A. (2023). Efficiency and Impact of Hypnoanalgesia for Cardiac Catheterisation in Paediatric Population. Journal of Clinical Medicine, 12(19), 6410. https://doi.org/10.3390/jcm12196410