
Mental Symptoms, Life Satisfaction and Sexual Orientation: A Gender Analysis



Abstract
1. Introduction
- Homosexual and bisexual women and men will present more mental symptoms than heterosexual women and men.
- Homosexual and bisexual women and men will present less life satisfaction than heterosexual women and men.
- Homosexual and bisexual women and men will present less self-esteem than heterosexual women and men.
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Mental Symptoms
2.2.2. Life Satisfaction
2.2.3. Self-Esteem
2.2.4. Masculine/Instrumental and Feminine/Expressive Traits
2.2.5. Traditional Gender Role Attitudes
2.2.6. Demographic and Sexual Orientation Data Collection Sheet
2.3. Statistical Analyses
3. Results
3.1. Differential Analyses
3.2. Correlations between Study Variables and with Age and Educational Level
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
Appendix A

{kind=link}
{kind=link}
| Men (n = 302) | Women (n = 316) | χ2-Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Educational level | |||||
| Elementary studies | 28 | 9.8 | 31 | 10.0 | 0.22 |
| High school degree or professional training | 199 | 69.6 | 209 | 67.9 | |
| University degree | 59 | 20.6 | 68 | 22.1 | |
| Non-data | 16 | 8 | |||
| Occupation | |||||
| Employed | 80 | 26.5 | 86 | 27.6 | 3.47 |
| Unemployed | 32 | 10.6 | 20 | 6.4 | |
| Student | 190 | 62.9 | 206 | 66.0 | |
| Non-data | 0 | 4 | |||
| Marital status | |||||
| Never married unpartnered | 141 | 49.8 | 131 | 42.0 | 5.49 |
| Never married with partner | 133 | 47.0 | 165 | 52.9 | |
| Married/cohabiting | 9 | 3.2 | 14 | 4.5 | |
| Separated/divorced | 0 | 0.0 | 2 | 0.6 | |
| Non-data | 19 | 4 | |||
| M | SD | M | SD | t-Value | |
| Age | 25.01 | 6.77 | 25.61 | 8.24 | −0.99 |
References
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of mental disorders in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Campion, J.; Javed, A.; Lund, C.; Sartorius, N.; Saxena, S.; Marmot, M.; Allan, J.; Udomratn, P. Public mental health: Required actions to address implementation failure in the context of COVID-19. Lancet Psychiatry 2022, 9, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Leiva-Peña, V.; Rubí-González, P.; Vicente-Parada, B. Social determinants of mental health: Public policies based on the biopsychosocial model in Latin American countries. Rev. Panam. Salud Publica 2021, 45, e158. [Google Scholar] [CrossRef] [PubMed]
- Commission on the Social Determinants of Health (CSDH). Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. Final Report of the Commission on Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008; Available online: https://apps.who.int/iris/bitstream/handle/10665/43943/9789241563703_eng.pdf;jsessionid=2BB0F29794C15D3B112B3C72775FFC40?sequence=1 (accessed on 30 April 2023).
- World Health Organization (WHO). Social Determinants of Health. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 30 June 2023).
- Ferrer, R. Social determinants of health. In Chronic Illness Care: Principles and Practice; Daaleman, T.P., Helton, M.R., Eds.; Springer: Cham, Switzerland, 2018; pp. 435–449. [Google Scholar]
- Government of Canada. Social Determinants of Health and Health Inequalities. Available online: https://www.canada.ca/en/public-health/services/health-promotion/population-health/what-determines-health.html (accessed on 30 June 2023).
- American Psychological Association. Guidelines for psychological practice with lesbian, gay, and bisexual clients. Am. Psychol. 2012, 67, 10–42. [Google Scholar] [CrossRef]
- Manandhar, M.; Hawkes, S.; Buse, K.; Nosratid, E.; Magar, V. Gender, health and the 2030 agenda for sustainable development. Bull. World Health Organ. 2018, 96, 644–653. [Google Scholar] [CrossRef]
- Heise, L.; Greene, M.E.; Opper, N.; Stavropoulou, M.; Harper, C.; Nascimento, M.; Zewdie, D. Gender inequality and restrictive gender norms: Framing the challenges to health. Lancet 2019, 393, 2440–2454. [Google Scholar] [CrossRef]
- Sen, G.; Östlin, P. Gender inequity in health: Why it exists and how we can change it. Glob. Public Health 2008, 3, 1–12. [Google Scholar] [CrossRef]
- Bem, S.L. The Lenses of Gender. Transforming the Debate on Sexual Inequality; Yale University Press: New Haven, CT, USA, 1993. [Google Scholar]
- Helgeson, V.S. Gender and personality. In APA Handbook of Personality and Social Psychology; Mikulincer, M., Shaver, P., Eds.; American Psychological Association: Washington, DC, USA, 2015; Volume 4, pp. 515–534. [Google Scholar]
- Eagly, A.H.; Nater, C.; Miller, D.I.; Kaufmann, M.; Sczesny, S. Gender stereotypes have changed: A cross-temporal meta-analysis of U.S. public opinion polls from 1946 to 2018. Am. Psychol. 2020, 75, 301–315. [Google Scholar] [CrossRef]
- Germani, A.; Delvecchio, E.; Li, J.B.; Mazzeschi, C. the horizontal and vertical individualism and collectivism scale: Early evidence on validation in an Italian sample. J. Child Fam. Stud. 2020, 29, 904–911. [Google Scholar] [CrossRef]
- Kahalon, R.; Shnabel, N.; Becker, J.C. Positive stereotypes, negative outcomes: Reminders of the positive components of complementary gender stereotypes impair performance in counter-stereotypical tasks. Br. J. Soc. Psychol. 2018, 57, 482–502. [Google Scholar] [CrossRef]
- Weber, A.M.; Cislaghi, B.; Meausoone, V.; Abdalla, S.; Mejía-Guevara, I.; Loftus, P.; Hallgren, E.; Seff, I.; Stark, L.; Victora, C.G.; et al. Gender norms and health: Insights from global survey data. Lancet 2019, 393, 2455–2468. [Google Scholar] [CrossRef] [PubMed]
- Darmstadt, G.L.; Heise, L.; Gupta, G.R.; Henry, S.; Cislaghi, B.; Greene, M.E.; Hawkes, S.; Hay, K.; Heymann, J.; Klugman, J.; et al. Why now for a Series on gender equality, norms, and health? Lancet 2019, 393, 2374–2377. [Google Scholar] [CrossRef] [PubMed]
- Krivoshchekov, V.; Gulevich, O.; Blagov, I. Traditional Masculinities and Men’s Sexism: A Meta-Analysis. Psychol. Men Masc. 2023. online. [Google Scholar] [CrossRef]
- Hay, K.; McDougal, L.; Percival, V.; Henry, S.; Klugman, J.; Wurie, H.; Raven, J.; Shabalala, F.; Fielding-Miller, R.; Dey, A.; et al. Disrupting gender norms in health systems: Making the case for change. Lancet 2019, 393, 2535–2549. [Google Scholar] [CrossRef]
- Herek, G.M.; McLemore, K.A. Sexual prejudice. Annu. Rev. Psychol. 2013, 64, 309–333. [Google Scholar] [CrossRef]
- Rubin, G. Thinking Sex: Notes for a Radical Theory of the Politics of Sexuality. In Social Perspectives in Lesbian and Gay Studies; Nardi, P.M., Schneider, B.E., Eds.; Routledge: New York, NY, USA, 1984; pp. 100–133. [Google Scholar]
- Herek, G.M.; Gillis, J.R.; Cogan, J. Internalized stigma among sexual minority adults: Insights from a social psychological perspective. Stigma Health 2015, 1, 18–34. [Google Scholar] [CrossRef]
- Gulevich, O.; Krivoshchekov, V.; Sorokina, A. Gender identification and attitudes toward gay people: Gender and sexuality differences and similarities. Curr. Psychol. 2023, 42, 7197–7210. [Google Scholar] [CrossRef]
- Herek, G.M. Heterosexuals’ Attitudes toward Lesbians and Gay Men: Correlates and Gender Differences. J. Sex Res. 1988, 25, 451–477. [Google Scholar] [CrossRef]
- Shannon, N.D.; Theodore, N.G. Gender Ideology: Components, Predictors, and Consequences. Annu. Rev. Sociol. 2009, 35, 87–105. [Google Scholar] [CrossRef]
- Brassel, S.T.; Anderson, V.N. Who thinks outside the gender box? Feminism, gender self-esteem, and attitudes toward trans people. Sex Roles 2020, 82, 447–462. [Google Scholar] [CrossRef]
- Perez-Arche, H.; Miller, D.J. What predicts attitudes toward transgender and nonbinary people? An exploration of gender, authoritarianism, social dominance, and gender ideology. Sex Roles 2021, 85, 172–189. [Google Scholar] [CrossRef]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef]
- Eldahan, A.I.; Pachankis, J.E.; Rendina, J.H.; Ventuneac, A.; Grov, C.; Parsons, J.T. Daily minority stress and affect among gay and bisexual men: A 30-day diary study. J. Affect. Disord. 2016, 190, 828–835. [Google Scholar] [CrossRef]
- Livingston, N.A.; Flentje, A.; Brennan, J.; Mereish, E.H.; Reed, O.; Cochran, B.N. Real-time associations between discrimination and anxious and depressed mood among sexual and gender minorities: The moderating effects of lifetime victimization and identity concealment. Psychol. Sex Orientat. Gend. Divers. 2020, 7, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Flores, A.R.; Langton, L.; Meyer, I.H.; Romero, A.P. Victimization rates and traits of sexual and gender minorities in the United States: Results from the National Crime Victimization Survey, 2017. Sci. Adv. 2020, 6, eaba6910. [Google Scholar] [CrossRef] [PubMed]
- King, M.; Semlyen, J.; Tai, S.S.; Killaspy, H.; Osborn, D.; Popelyuk, D.; Nazareth, I. A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry 2008, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, A.; McManus, S.; Brugha, T.S.; Bebbington, P.; King, M. Mental health of the non-heterosexual population of England. Br. J. Psychiatry. 2011, 198, 143–148. [Google Scholar] [CrossRef]
- Campo-Arias, A.; Vanegas-García, J.L.; Herazo, E. Sexual orientation and social anxiety disorder: A systematic review. Rev. Chil. Neuro-Psiquiat. 2017, 55, 93–102. [Google Scholar] [CrossRef][Green Version]
- Kidd, G.; Marston, L.; Nazareth, I.; Osborn, D.; Pitman, A. Suicidal thoughts, suicide attempt and non-suicidal self-harm amongst lesbian, gay and bisexual adults compared with heterosexual adults: Analysis of data from two nationally representative English household surveys. Soc. Psychiatry Psychiatr. Epidemiol. 2023. [Google Scholar] [CrossRef]
- Wittgens, C.; Fischer, M.M.; Buspavanich, P.; Theobald, S.; Schweizer, K.; Trautmann, S. Mental health in people with minority sexual orientations: A meta-analysis of population-based studies. Acta Psychiatr. Scand. 2022, 145, 357–372. [Google Scholar] [CrossRef]
- Helminen, E.C.; Ducar, D.M.; Scheer, J.R.; Parke, K.L.; Morton, M.L.; Felver, J.C. Self-Compassion, Minority Stress, and Mental Health in Sexual and Gender Minority Populations: A Meta-Analysis and Systematic Review. Clin. Psychol. 2023, 30, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Bridge, L.; Smith, P.; Rimes, K.A. Sexual orientation differences in the self-esteem of men and women: A systematic review and meta-analysis. Psychol. Sex Orientat. Gend. Divers. 2019, 6, 433–446. [Google Scholar] [CrossRef]
- Hudson, S.T.J.; Ghani, A. Sexual Orientation and Race Intersectionally Reduce the Perceived Gendered Nature of Normative Stereotypes in the United States. Psychol. Women Q. 2023. [Google Scholar] [CrossRef]
- Kite, M.E.; Deaux, K. Gender belief systems: Homosexuality and the implicit inversion theory. Psychol. Women Q. 1987, 11, 83–96. [Google Scholar] [CrossRef]
- Clarke, H.M.; Arnold, K.A. Diversity in gender stereotypes? A comparison of heterosexual, gay and lesbian perspectives. Can. J. Adm. Sci. 2017, 34, 149–158. [Google Scholar] [CrossRef]
- Martin, C.L.; Cook, R.D.; Andrews, N.C.Z. Reviving androgyny: A modern day perspective on flexibility of gender identity and behaviour. Sex Roles 2017, 76, 592–603. [Google Scholar] [CrossRef]
- Matud, M.P.; Bethencourt, J.M.; Ibáñez, I.; Fortes, D.; Díaz, A. Gender Differences in Psychological Well-Being in Emerging Adulthood. Appl. Res. Qual. Life 2022, 17, 1001–1017. [Google Scholar] [CrossRef]
- Pérez, J.I.; Matud, M.P. Gender, Stress, and Well-Being in Adulthood. J. Clin. Med. 2022, 12, 110. [Google Scholar] [CrossRef]
- Goldberg, D.P.; Hillier, V.F. A scaled version of the General Health Questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Madden, D. Gender Differences in Mental Well-Being: A Decomposition Analysis. Soc. Indic. Res. 2010, 99, 101–114. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.; Larsen, R.J.; Griffin, S. The satisfaction with Life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Pavot, W.; Diener, E. Review of the Satisfaction With Life Scale. In Assessing Well-Being; Diener, E., Ed.; Springer: Dordrecht, The Netherlands, 2009; Volume 39, pp. 101–117. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self Image; Princeton University Press: Princeton, MA, USA, 1965. [Google Scholar]
- Bem, S.L. Bem Sex Role Inventory Professional Manual; Consulting Psychologists Press: Palo Alto, CA, USA, 1981. [Google Scholar]
- Matud, M.P. Diseño y Validación de un Programa de Intervención Psicológica con Mujeres Maltratadas por su Pareja; Research report; Women’s Institute, Ministry of Labor and Social Affairs: Madrid, Spain, 2004. [Google Scholar]
- Klysing, A. Prototypicality at the intersection of gender and sexual orientation. Br. J. Soc. Psychol. 2023, 62, 1506–1533. [Google Scholar] [CrossRef] [PubMed]
- Matud, M.P.; Aguilera, L. Sex roles and mental health in a sample of the general Spanish population. Salud Ment. 2009, 32, 53–58. [Google Scholar]
- Kosakowska-Berezecka, N.; Bosson, J.K.; Jurek, P.; Besta, T.; Olech, M.; Vandello, J.A.; Bender, M.; Dandy, J.; Hoorens, V.; Jasinskaja-Lahti, I.; et al. Gendered Self-views across 62 countries: A test of competing models. Soc. Psychol. Person. Sci. 2023, 14, 808–824. [Google Scholar] [CrossRef]
- Matud, M.P.; Ibáñez, I.; Fortes, D.; Bethencourt, J.M. Adolescent stress, psychological distress and well-being: A gender analysis. Child Youth Serv. 2023, in press. [Google Scholar] [CrossRef]


| Heterosexuals (n = 309) | Homosexuals or Bisexuals (n = 309) | χ2-Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Educational level | |||||
| Elementary studies | 29 | 9.4 | 30 | 10.4 | 0.17 |
| High school degree or professional training | 212 | 69.1 | 196 | 68.3 | |
| University degree | 66 | 21.5 | 61 | 21.3 | |
| Non-data | 2 | 22 | |||
| Occupation | |||||
| Employed | 82 | 26.5 | 84 | 27.5 | 0.09 |
| Unemployed | 26 | 8.5 | 26 | 8.5 | |
| Student | 201 | 65.0 | 195 | 63.9 | |
| Non-data | 0 | 4 | |||
| Marital status | |||||
| Never married unpartnered | 142 | 46.7 | 130 | 44.7 | 0.29 |
| Never married with partner | 149 | 49.1 | 149 | 51.2 | |
| Married/cohabiting | 12 | 3.9 | 11 | 3.8 | |
| Separated/divorced | 1 | 0.3 | 1 | 0.3 | |
| Non-data | 5 | 18 | |||
| M | SD | M | SD | t-Value | |
| Age | 25.14 | 7.52 | 25.50 | 7.59 | −0.59 |
| Symptoms | Heterosexuals | Homosexuals or Bisexuals | ANOVA | ||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | Effect | F Ratio | ηp2 | |
| Somatic | |||||||
| Men | 5.02 | 4.16 | 5.61 | 3.84 | Sex. Orient. | 4.09 * | 0.007 |
| Women | 5.82 | 3.57 | 6.52 | 4.24 | Gender | 7.15 ** | 0.012 |
| Interaction Gender × Sexual orientation | G × SO | 0.03 | 0.000 | ||||
| Anxiety and insomnia | |||||||
| Men | 5.44 | 4.82 | 6.15 | 4.90 | Sex. Orient. | 2.42 | 0.004 |
| Women | 6.37 | 4.67 | 6.91 | 5.53 | Gender | 4.40 * | 0.007 |
| Interaction Gender × Sexual orientation | G × SO | 0.04 | 0.000 | ||||
| Social dysfunction | |||||||
| Men | 7.20 | 3.64 | 7.59 | 2.77 | Sex. Orient. | 5.23 * | 0.009 |
| Women | 6.91 | 3.10 | 7.74 | 3.51 | Gender | 0.07 | 0.000 |
| Interaction Gender × Sexual orientation | G × SO | 0.71 | 0.000 | ||||
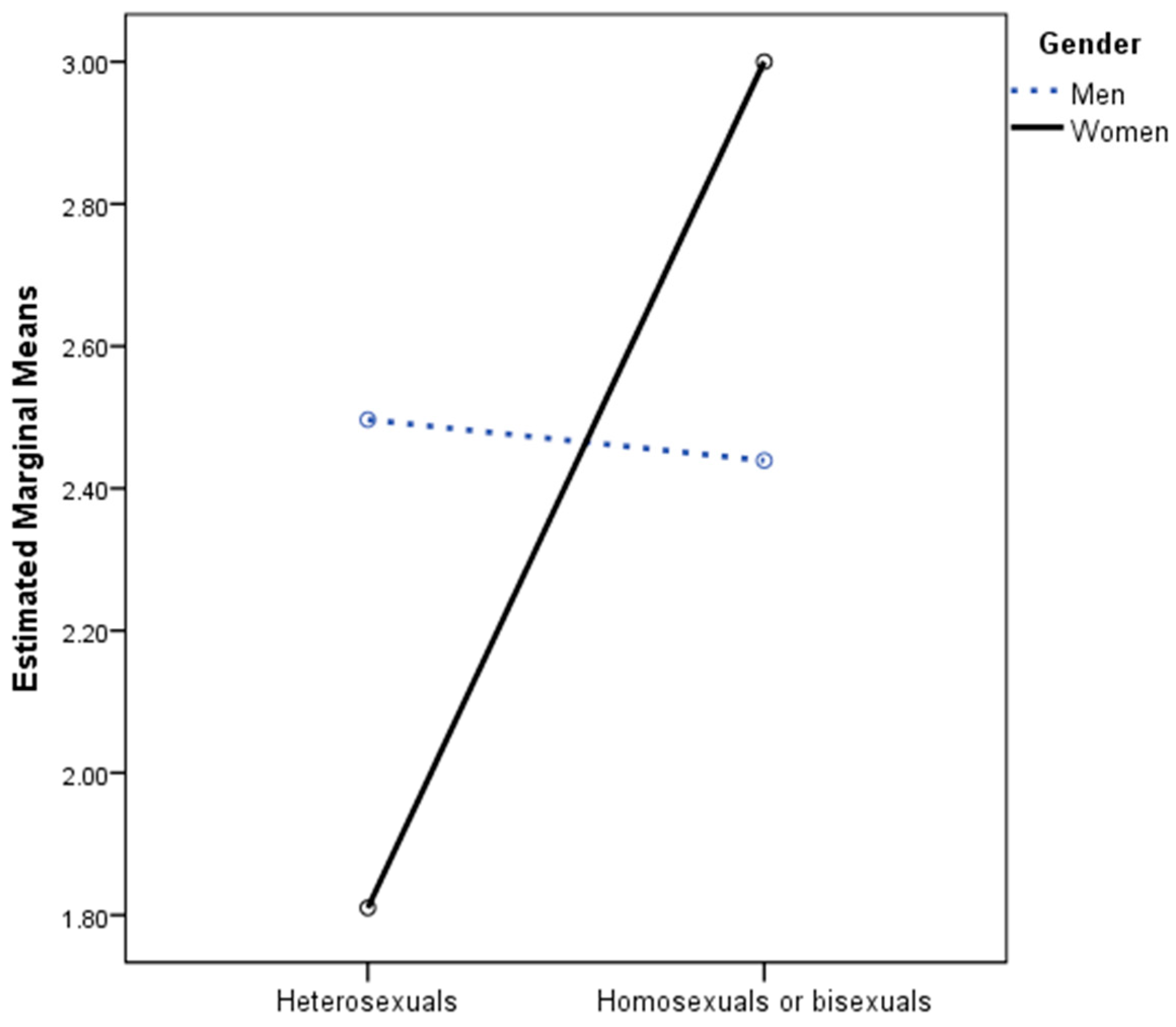
| Severe depression | |||||||
| Men | 2.50 | 4.21 | 2.44 | 3.61 | Sex. Orient. | 3.19 | 0.005 |
| Women | 1.81 | 3.10 | 3.00 | 4.66 | Gender | 0.04 | 0.000 |
| Interaction Gender × Sexual orientation | G × SO | 3.86 * | 0.006 | ||||
| Heterosexuals | Homosexuals or Bisexuals | |||
|---|---|---|---|---|
| M | SD | M | SD | |
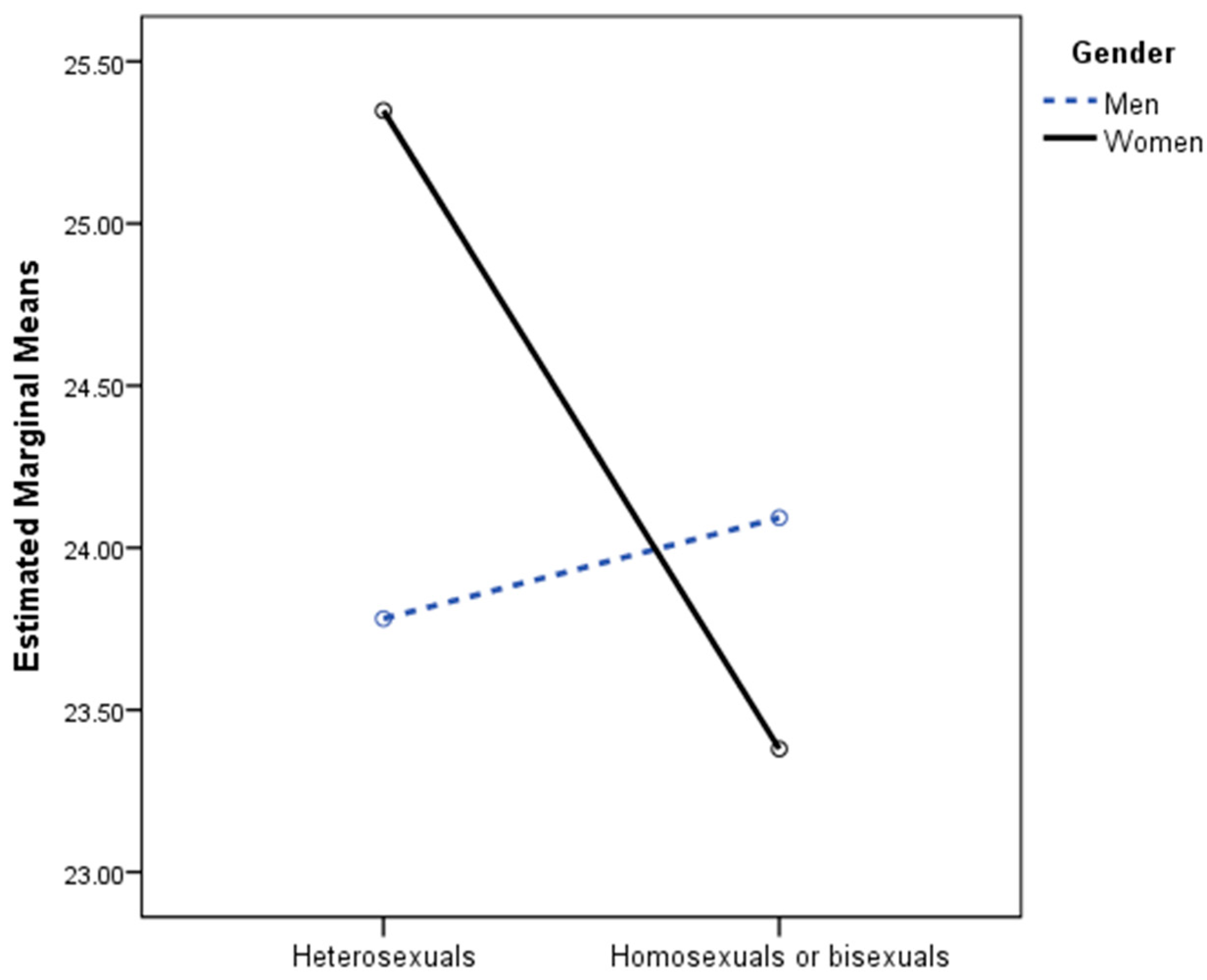
| Life satisfaction | ||||
| Men | 23.78 | 6.40 | 24.09 | 6.30 |
| Women | 25.35 | 6.09 | 23.38 | 7.12 |
| Self-esteem | ||||
| Men | 22.04 | 5.49 | 20.90 | 5.97 |
| Women | 21.52 | 5.00 | 20.41 | 6.37 |
| Variable | Heterosexuals | Homosexuals or Bisexuals | ANOVA | ||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | Effect | F Ratio | ηp2 | |
| Masculine/instrumental trait | |||||||
| Men | 49.52 | 7.42 | 48.59 | 8.44 | Sex. Orient. | 2.63 | 0.004 |
| Women | 50.34 | 7.51 | 49.17 | 8.66 | Gender | 1.19 | 0.002 |
| Interaction Gender × Sexual orientation | G × SO | 1.17 | 0.002 | ||||
| Feminine/expressive trait | |||||||
| Men | 54.83 | 9.43 | 55.67 | 9.47 | Sex. Orient. | 0.01 | 0.000 |
| Women | 58.66 | 7.84 | 57.98 | 7.94 | Gender | 19.25 *** | 0.031 |
| Interaction Gender × Sexual orientation | G × SO | 0.03 | 0.000 | ||||
| Traditional gender role attitudes | |||||||
| Men | 42.17 | 15.77 | 39.68 | 17.38 | Sex. Orient. | 1.71 | 0.003 |
| Women | 34.54 | 13.57 | 33.90 | 12.61 | Gender | 31.23 *** | 0.048 |
| Interaction Gender × Sexual orientation | G × SO | 0.60 | 0.001 | ||||
| Heterosexuals | Homosexuals or Bisexuals | |||||||
|---|---|---|---|---|---|---|---|---|
| Women | Men | Women | Men | |||||
| Age | Education a | Age | Education a | Age | Education a | Age | Education a | |
| Somatic symptoms | −0.06 | −0.09 | −0.01 | −0.01 | −0.07 | −0.17 * | −0.17 * | −0.17 |
| Anxiety and insomnia symptoms | −0.10 | −0.10 | −0.04 | 0.01 | −0.17 * | −0.19 * | −0.22 ** | −0.13 |
| Social dysfunction | −0.20 * | 0.00 | 0.04 | 0.01 | −0.02 | −0.18 * | −0.17 * | −0.08 |
| Severe depression symptoms | −0.14 | −0.15 | −0.09 | −0.04 | −0.09 | −0.16 * | −0.19 * | −0.17 * |
| Life satisfaction | 0.14 | 0.06 | −0.12 | −0.06 | 0.00 | 0.03 | 0.14 | 0.09 |
| Self-esteem | 0.14 | 0.01 | 0.17 * | 0.09 | 0.20 * | 0.22 * | 0.24 ** | 0.12 |
| Masculine/instrumental trait | 0.13 | 0.19 * | −0.01 | 0.04 | −0.01 | 0.06 | 0.15 | 0.15 |
| Feminine/expressive trait | 0.19 * | −0.10 | 0.12 | 0.18 * | −0.03 | 0.03 | 0.05 | 0.11 |
| Traditional gender role attitudes | 0.30 *** | −0.09 | 0.09 | −0.02 | 0.18 * | 0.04 | 0.00 | 0.07 |
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|
| Heterosexual women | ||||||||
| 1. Somatic symptoms | 0.56 *** | 0.39 *** | 0.47 *** | −0.37 *** | −0.45 *** | 0.02 | 0.04 | 0.09 |
| 2. Anxiety and insomnia symptoms | 0.42 *** | 0.54 *** | −0.41 *** | −0.43 *** | −0.05 | −0.01 | 0.13 | |
| 3. Social dysfunction | 0.49 *** | −0.50 *** | −0.47 *** | −0.28 *** | −0.15 | −0.04 | ||
| 4. Severe depression symptoms | −0.49 *** | −0.63 *** | −0.07 | −0.17 * | 0.09 | |||
| 5. Life satisfaction | 0.63 *** | 0.30 *** | 0.25 ** | −0.12 | ||||
| 6. Self-esteem | 0.25 ** | 0.26 ** | −0.09 | |||||
| 7. Masculine/instrumental trait | 0.33 *** | −0.07 | ||||||
| 8. Feminine/expressive trait | 0.13 | |||||||
| 9. Traditional gender role attitudes | ||||||||
| Lesbian or bisexual women | ||||||||
| 1. Somatic symptoms | 0.77 *** | 0.56 *** | 0.58 *** | −0.38 *** | −0.47 *** | −0.09 | 0.04 | −0.06 |
| 2. Anxiety and insomnia symptoms | 0.55 *** | 0.59 *** | −0.43 *** | −0.45 *** | −0.05 | 0.07 | 0.01 | |
| 3. Social dysfunction | 0.69 *** | −0.49 *** | −0.55 *** | −0.16 * | −0.08 | 0.07 | ||
| 4. Severe depression symptoms | −0.54 *** | −0.66 *** | −0.16 | −0.05 | 0.06 | |||
| 5. Life satisfaction | 0.72 *** | 0.23 ** | 0.28 *** | −0.12 | ||||
| 6. Self-esteem | 0.24 ** | 0.17 ** | 0.03 | |||||
| 7. Masculine/instrumental trait | 0.32 *** | −0.01 | ||||||
| 8. Feminine/expressive trait | −0.04 | |||||||
| 9. Traditional gender role attitudes |
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|
| Heterosexual men | ||||||||
| 1. Somatic symptoms | 0.75 *** | 0.54 *** | 0.54 *** | −0.38 *** | −0.36 *** | −0.19 * | −0.20 * | −0.02 |
| 2. Anxiety and insomnia symptoms | 0.64 *** | 0.67 *** | −0.50 *** | −0.51 *** | −0.23 ** | −0.22 ** | −0.06 | |
| 3. Social dysfunction | 0.61 *** | −0.51 *** | −0.50 *** | −0.23 ** | −0.14 | −0.08 | ||
| 4. Severe depression symptoms | −0.62 *** | −0.66 *** | −0.22 ** | −0.21 ** | 0.00 | |||
| 5. Life satisfaction | 0.61 *** | 0.28 *** | 0.26 ** | 0.02 | ||||
| 6. Self-esteem | 0.39 *** | 0.36 *** | −0.07 | |||||
| 7. Masculine/instrumental trait | 0.34 *** | 0.03 | ||||||
| 8. Feminine/expressive trait | −0.30 *** | |||||||
| 9. Traditional gender role attitudes | ||||||||
| Gay or bisexual men | ||||||||
| 1. Somatic symptoms | 0.74 *** | 0.51 *** | 0.56 *** | −0.51 *** | −0.58 *** | −0.09 | −0.09 | 0.03 |
| 2. Anxiety and insomnia symptoms | 0.44 *** | 0.59 *** | −0.45 *** | −0.52 *** | 0.04 | −0.03 | 0.01 | |
| 3. Social dysfunction | 0.54 *** | −0.45 *** | −0.44 *** | −0.16 | −0.18 * | 0.02 | ||
| 4. Severe depression symptoms | −0.54 *** | −0.65 *** | −0.19 * | −0.19 * | 0.09 | |||
| 5. Life satisfaction | 0.72 *** | 0.38 *** | 0.27 ** | −0.13 | ||||
| 6. Self-esteem | 0.45 *** | 0.19 ** | −0.04 | |||||
| 7. Masculine/instrumental trait | 0.23 ** | 0.01 | ||||||
| 8. Feminine/expressive trait | −0.27 ** | |||||||
| 9. Traditional gender role attitudes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matías, R.; Matud, M.P. Mental Symptoms, Life Satisfaction and Sexual Orientation: A Gender Analysis. J. Clin. Med. 2023, 12, 6366. https://doi.org/10.3390/jcm12196366
Matías R, Matud MP. Mental Symptoms, Life Satisfaction and Sexual Orientation: A Gender Analysis. Journal of Clinical Medicine. 2023; 12(19):6366. https://doi.org/10.3390/jcm12196366
Chicago/Turabian StyleMatías, Roberto, and M. Pilar Matud. 2023. "Mental Symptoms, Life Satisfaction and Sexual Orientation: A Gender Analysis" Journal of Clinical Medicine 12, no. 19: 6366. https://doi.org/10.3390/jcm12196366
APA StyleMatías, R., & Matud, M. P. (2023). Mental Symptoms, Life Satisfaction and Sexual Orientation: A Gender Analysis. Journal of Clinical Medicine, 12(19), 6366. https://doi.org/10.3390/jcm12196366