
A Prospective Study of the Assessment of the Efficacy of a Biodegradable Poly(l-lactic acid/ε-caprolactone) Membrane for Guided Bone Regeneration


Abstract
:1. Introduction
2. Materials and Methods
- (1)
- Patients requiring GBR because of insufficient bone volume in the edentulous region where dental implants are required to be placed.
- (2)
- Age range: 20–90 years.
- (3)
- Patients who understood the consent document and agreed to participate in the study at their discretion.
- (1)
- Patients suffering from severe hematological disorders.
- (2)
- Patients with abnormalities in the organs of calcium metabolism, such as the kidneys and digestive organs, or suspected connective tissue diseases.
- (3)
- Patients who were difficult to follow up during the study for various reasons.
- (4)
- Patients whose social and domestic circumstances precluded compliance with the requirements of this study.
- (5)
- Smokers.
- (6)
- Patients in need of surrogates.
- (7)
- Patients deemed to be inappropriate for participation in this study.
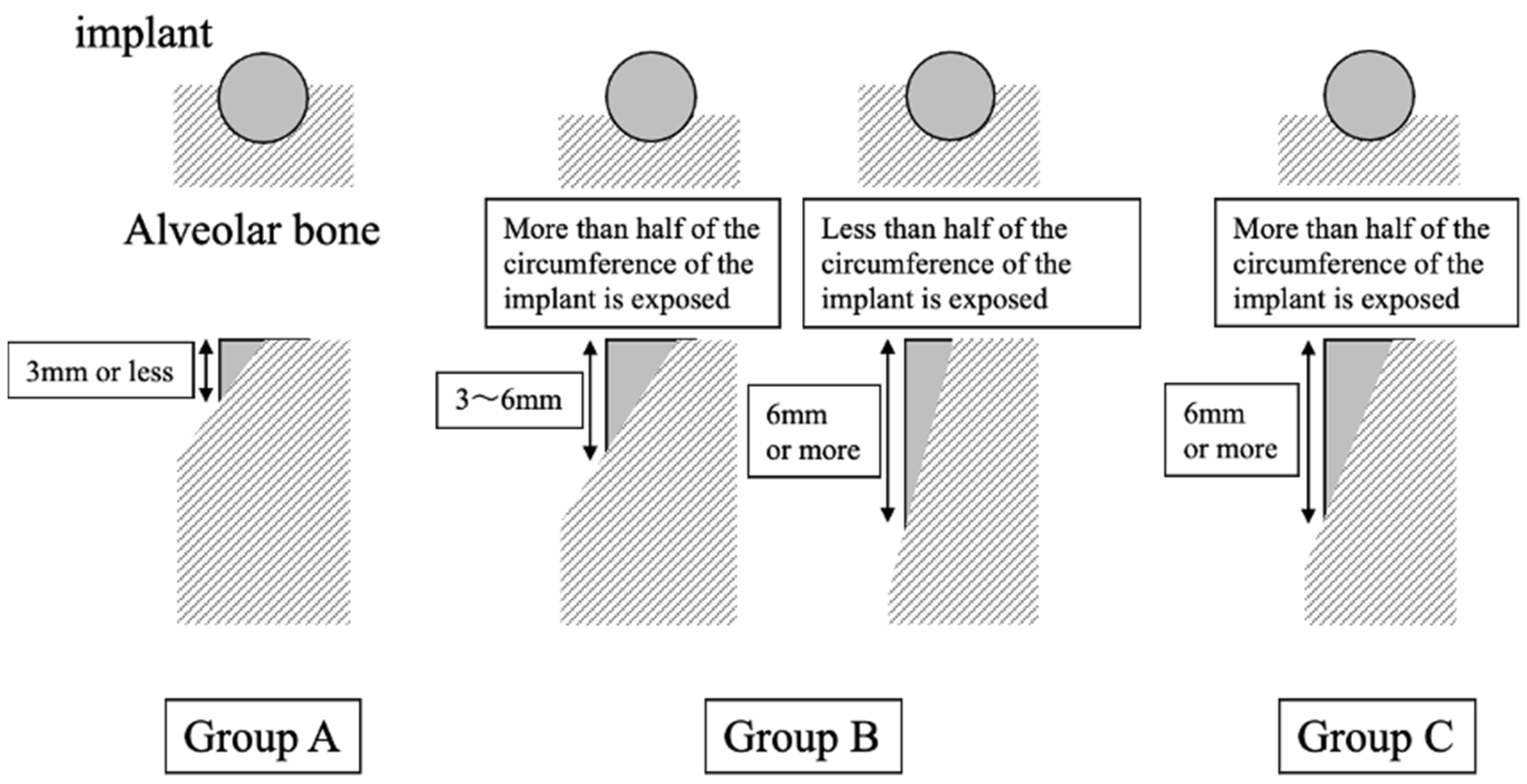
- Group A: The implant exposure was less than 3 mm vertically, and less than half of the implant was horizontally.
- Group B: (1) The implant exposure was between 3 and 6 mm vertically and horizontally, with more than half of the implants. (2) Implant exposure greater than 6 mm and less than half of the implant horizontally.
- Group C: Implant exposure was more than 6 mm vertically and horizontally in more than half of the implants, in which case primary stability was not considered to be obtained. In this group, the first step was bone augmentation by GBR, and implant placement was performed during the second surgery.
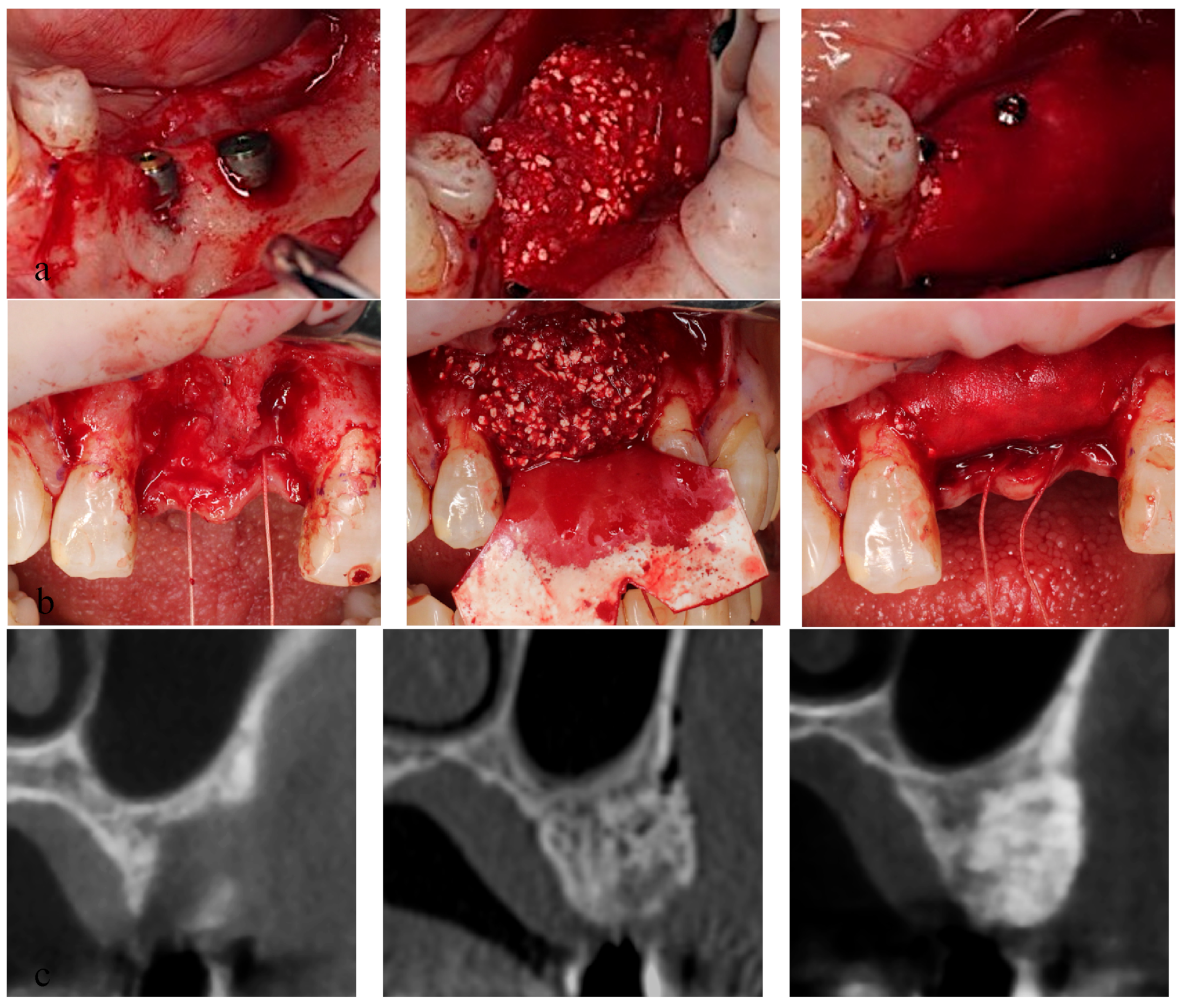
2.1. Surgical Procedures (Figure 2)
- Groups A and B: The mucoperiosteal flap was elevated and alveolar bone atrophy or defects were observed. Following implant placement using a surgical guide, the exposed implant region was covered with a bone graft material mixture, and the materials were enveloped by the GBR membrane. The GBR membrane was fixed with tuck pins (tru TACK®, ACE surgical, AZ, USA) to maintain the graft materials at the place in group B but not in group A. After a tension-reducing periosteal incision was made, the wound was closed without tension.
- Group C: Bone augmentation was performed as in group B but without implant placement.
- Bone augmentation using GBR was performed simultaneously with implant insertion in groups A and B.
- Bone augmentation by GBR was performed prior to implant insertion in group C.
- CT images of group C (before, left, right, middle, and 150 days after GBR; right).
2.2. Follow-Up
2.3. Assessment
- (1)
- Adverse events: Events that could be related to the GBR membrane were identified as adverse events that occurred during the study period from GBR to the second surgery.
- (2)
- (3)
- 150 ± 14 days after GBR (T2). The absorbance rate of the augmented bone was calculated using T1-T2/T1.
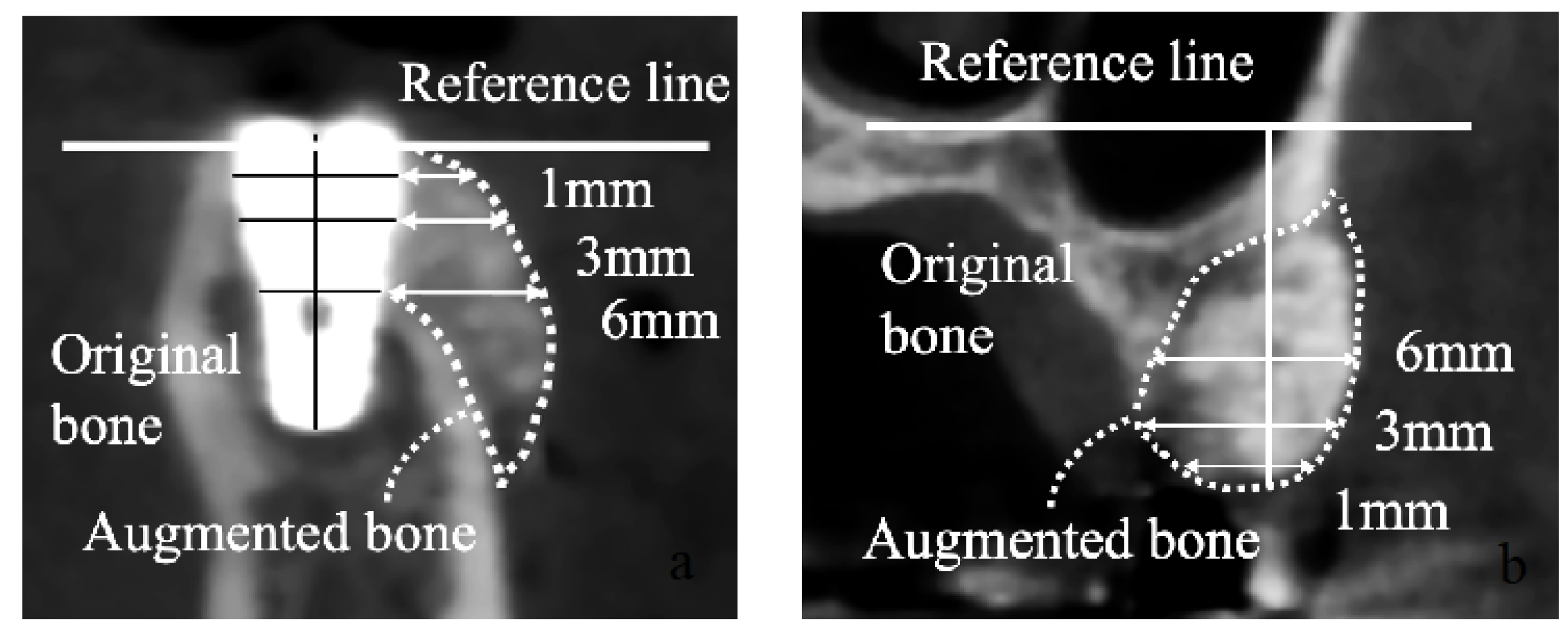
- Groups A and B: The platform level was designated as the reference line. The augmented bone width was calculated horizontally at 1, 3, and 6 mm from the reference line.
- Group C: The nasal floor and mandibular margin were designated as the reference lines for the maxilla and mandible, respectively. The augmented bone height was calculated from the reference line to the edge of the augmented bone. The alveolar bone width was calculated at 1, 3, and 6 mm from the reference lines.
- (4)
- ISQ values: The ISQ values were evaluated during the second surgery using Osstell in groups A and B. The evaluation was performed on both the labial/buccal and lingual/palatal sides. The average ISQ value of both sides was determined as the ISQ value of the implant.
- (5)
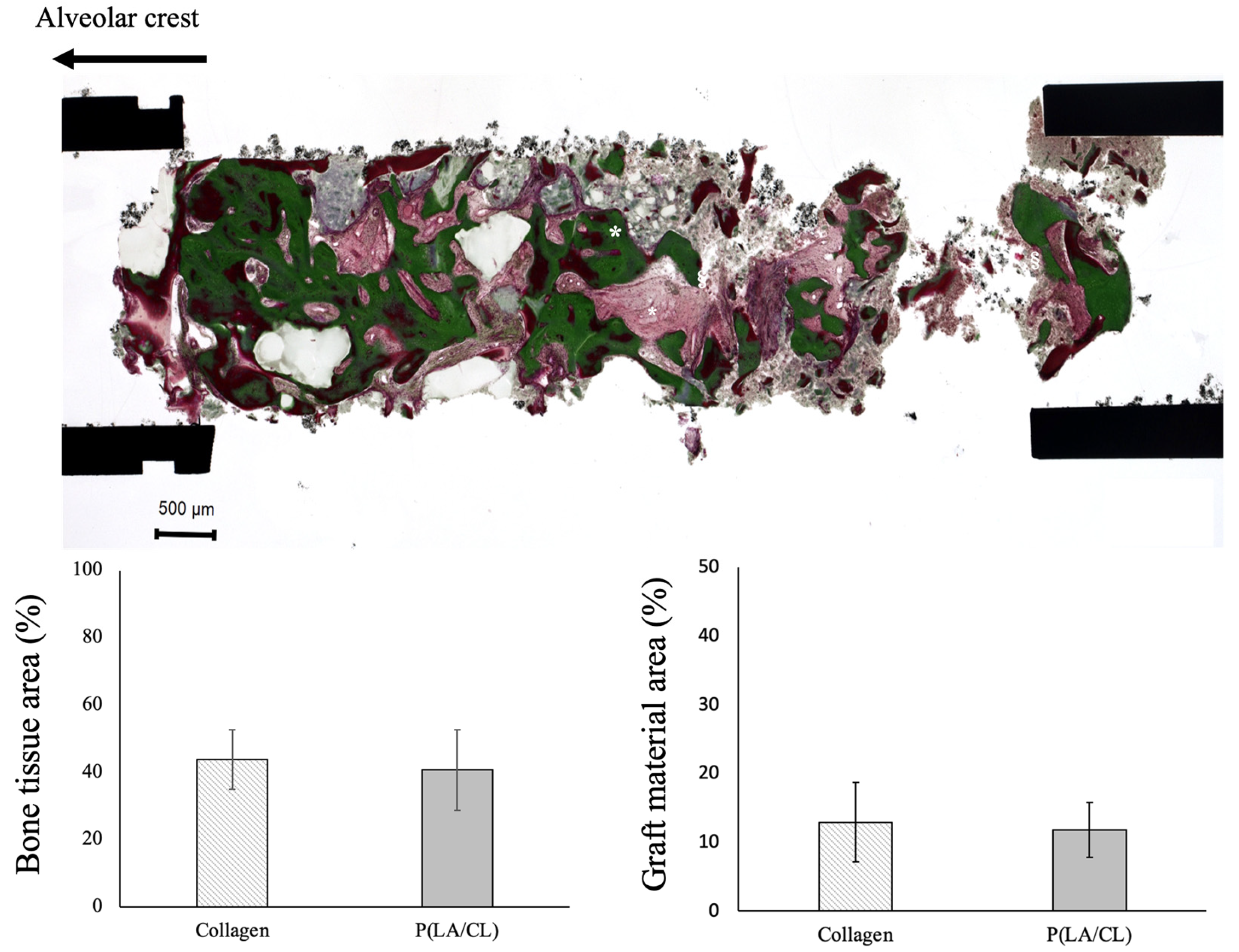
- Histology of the bone biopsy specimen in group C: To evaluate the bone tissue area, Villanueva–Goldner staining was performed (Kureha Special Laboratory, Fukushima, Japan). The bone tissue area was analyzed using the ImageJ software (NIH, Bethesda, MD, USA). The ratio of the bone tissue area to the total specimen obtained by biopsy was measured by combining the green area indicating mature bone and the dark red area indicating osteoids as the bone tissue area.
2.4. Statistical Analysis
3. Results
3.1. Patients and Sites
3.2. Adverse Events
3.3. ISQ Values
3.4. CT Evaluation
3.4.1. Group A
3.4.2. Group B
3.4.3. Group C
3.4.4. All Groups
3.5. Histological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bornstein, M.M.; Halbritter, S.; Harnisch, H.; Weber, H.P.; Buser, D. A retrospective analysis of patients referred for implant placement to a specialty clinic: Indications, surgical procedures, and early failures. Int. J. Oral. Maxillofac. Implant. 2008, 23, 1109–1116. [Google Scholar]
- Wang, H.L.; Boyapati, L. “PASS” principles for predictable bone regeneration. Implant. Dent. 2006, 15, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Rakhmatia, Y.D.; Ayukawa, Y.; Furuhashi, A.; Koyano, K. Current barrier membranes: Titanium mesh and other membranes for guided bone regeneration in dental applications. J. Prosthodont. Res. 2013, 57, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Omar, O.; Elgali, I.; Dahlin, C.; Thomsen, P. Barrier membranes: More than the barrier effect? J. Clin. Periodontol. 2019, 46, 103–123. [Google Scholar] [CrossRef]
- Lee, S.W.; Kim, S.G. Membranes for the guided bone regeneration. Maxillofac. Plast. Reconstr. Surg. 2014, 36, 239–246. [Google Scholar] [CrossRef]
- Selvig, K.A.; Kersten, B.G.; Chamberlain, A.D.; Wikesjö, U.M.; Nilvéus, R.E. Regenerative surgery of intrabony periodontal defects using ePTFE barrier membranes: Scanning electron microscopic evaluation of retrieved membranes versus clinical healing. J. Periodontol. 1992, 63, 974–978. [Google Scholar] [CrossRef]
- Zellin, G.; Gritli-Linde, A.; Linde, A. Healing of mandibular defects with different biodegradable and non-biodegradable membranes: An experimental study in rats. Biomaterials 1995, 16, 601–609. [Google Scholar] [CrossRef]
- Chiapsaco, M.; Zaniboni, M. Clinical outcomes of GBR procedures to correct peri-implant dehiscences and fenestrations: A systematic review. Clin. Oral. Implant. Res. 2009, 20, 113–123. [Google Scholar] [CrossRef]
- Vuddhakanok, S.; Solt, C.W.; Mitchell, J.C.; Foreman, D.W.; Alger, F.A. Histologic evaluation of periodontal attachment apparatus following the insertion of a biodegradable copolymer barrier in humans. J. Periodontol. 1993, 64, 202–210. [Google Scholar] [CrossRef]
- Hutmacher, D.; Hurzeler, M.B.; Schliephake, A. A review of material properties of biodegradable and bioresorbable polymers and devices for GTR and GBR applications. Int. J. Oral. Maxillofac. Implant. 1996, 11, 667–678. [Google Scholar]
- Zhao, L.; Li, N.; Wang, K.; Shi, C.; Zhang, L.; Luan, Y. A review of polypeptide-based polymersomes. Biomaterials 2014, 35, 1284–1301. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, T.; Ohba, S.; Natatani, Y.; Asahina, I. Clinical study of guided bone regeneration with resorbable polylactide-co-glycolide acid membrane. Odontology 2018, 106, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Abe, G.; Sasaki, J.; Katata, C.; Hohno, T.; Tsuboi, R.; Kitagawa, H.; Imazato, S. Fabricarion of novel poly (l-lactic acid/ε-caprolactone) bilayer membrane for GBR. Dent. Mater. 2020, 36, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Ogata, K.; Ohba, S.; Sumita, Y.; Asahina, I. Safety and feasibility assessment of biodegradable poly (l-lactic acid/ε-caprolactone) membrane for guided bone regeneration: A case series of first-in-human pilot study. J. Dent. Sci. 2022, 17, 368–376. [Google Scholar] [CrossRef]
- Carini, F.; Longoni, S.; Amosso, E.; Paleari, J.; Carini, S.; Porcaro, G. Bone augmentation with TiMesh. Autologous bone versus autologous bone and bone substitutes. A systematic review. Ann. Stomatol. 2014, 2, 27–36. [Google Scholar]
- Urban, I.A.; Nagursky, H.; Lozada, J.L. Horizontal ridge augmentation with a resorbable membrane and particulated autogenous bone with or without anorganic bovine bone-derived mineral: A retrospective case series in 22 patients. Int. J. Oral. Maxillofac. Implant. 2011, 26, 404–414. [Google Scholar]
- López, A.B.; Martínez, J.B.; Pelayo, J.L.; García, C.C.; Diago, M.P. Resonance frequency analysis of dental implant stability during the healing period. Med. Oral. Patol. Oral. Cir. Bucal 2008, 13, e244–e247. [Google Scholar]
- Ohba, S.; Sumita, Y.; Nakatani, Y.; Noda, S.; Asahina, I. Alveolar bone preservation by a hydroxyapatite/collagen composite material after tooth extraction. Clin. Oral. Investig. 2019, 23, 2413–2419. [Google Scholar] [CrossRef]
- Cucchi, A.; Sartori, M.; Parrilli, A.; Aldini, N.N. Histological and histomorphometric analysis of bone tissue after guided bone regeneration with non-resorbable membrane vs resorbable membranes and titanium mesh. Clin. Implant. Dent. Relat. Res. 2019, 21, 693–701. [Google Scholar] [CrossRef]
- Nakagawa, T.; Kudoh, K.; Fukuda, N.; Kasugai, S.; Tachikawa, N.; Koyano, K.; Matsushita, S.; Sasaki, M.; Ishikawa, K.; Miyamoto, Y. Application of low-crystalline carbonate apatite granules in 2-stage sinus floor augmentation: A prospective clinical trial and histomorphometric evaluation. J. Periodontal Implant. Sci. 2019, 49, 382–396. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Raines, R.T. Review collagen-based biomaterials for wound healing. Biopolymers 2014, 101, 821–833. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Bosshardt, D.; Buser, D. Effect of two different bioabsorbable collagen membranes on guided bone regeneration: A comparative histomorphometric study in the dog mandible. J. Periodontol. 2007, 78, 1943–1953. [Google Scholar] [CrossRef] [PubMed]
- Abe, G.L.; Tsuboi, R.; Kitagawa, H.; Sasaki, J.; Li, A.; Kohno, T.; Imazato, S. Poly(lactic acid/caprolactone) bilayer membrane blocks bacterial penetration. J. Periodont Res. 2022, 57, 510–518. [Google Scholar] [CrossRef] [PubMed]
- McGinnis, M.; Larsen, P.; Miloro, M.; Beck, M. Comparison of resorbable and nonresorbable guided bone regeneration materials: A preliminary study. Int. J. Oral. Maxillofac. Implant. 1998, 13, 30–35. [Google Scholar]
- Török, B.; Török, R.; Ehrenfest, D.M.D.; Agop-Forna, D.; Dascalu, C.; Forna, N.C. Study of immediate implants placed in mandibular alveolar bone reconstructed with screw-guided bone regeneration technique: A 24-months follow-up. Appl. Sci. 2021, 11, 6054. [Google Scholar] [CrossRef]
- Di Carlo, S.; Grasso, E.; Pranno, N.; De Angelis, F.; Di Gioia, C.; Jedlinski, M.; Tornese, A.; Lomelo, P.; Brauner, E. A retrospective analysis of treatment outcomes following guided bone regeneration at sites exhibiting severe alveolar ridge atrophy. J. Craniofac Surg. 2021, 32, e572–e578. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Total Sites (Number of Patients) | Collagen (Number of Patients) | P(LA/CL) (Number of Patients) |
|---|---|---|---|
| A | 7 (7) | 3 (3) | 4 (4) |
| B | 10 (7) | 4 (4) | 6 (3) |
| C | 8 (6) | 3 (3) | 5 (3) |
| Total | 25 (20) | 10 (10) | 15 (10) |
| 1 mm | 3 mm | 6 mm | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T1 (mm) | T2 (mm) | Absorbable Ratio (%) | T1 (mm) | T2 (mm) | Absorbable Ratio (%) | T1 (mm) | T2 (mm) | Absorbable Ratio (%) | |
| Collagen | 3.8 ± 2.1 | 2.3 ± 2.0 | 40.9 ± 36.7 | 4.3 ± 3.1 | 2.9 ± 2.7 | 29.4 ± 30.1 | 4.7 ± 4.4 | 4.4 ± 4.2 | 11.1 ± 22.0 * |
| P(LA/CL) | 3.4 ± 2.2 | 2.6 ± 2.4 | 26.2 ± 27.4 | 5.0 ± 3.2 | 4.1 ± 3.1 | 17.1 ± 19.7 | 6.1 ± 4.2 | 5.3 ± 3.8 | 13.3 ± 16.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shido, R.; Ohba, S.; Tominaga, R.; Sumita, Y.; Asahina, I. A Prospective Study of the Assessment of the Efficacy of a Biodegradable Poly(l-lactic acid/ε-caprolactone) Membrane for Guided Bone Regeneration. J. Clin. Med. 2023, 12, 5994. https://doi.org/10.3390/jcm12185994
Shido R, Ohba S, Tominaga R, Sumita Y, Asahina I. A Prospective Study of the Assessment of the Efficacy of a Biodegradable Poly(l-lactic acid/ε-caprolactone) Membrane for Guided Bone Regeneration. Journal of Clinical Medicine. 2023; 12(18):5994. https://doi.org/10.3390/jcm12185994
Chicago/Turabian StyleShido, Rena, Seigo Ohba, Risa Tominaga, Yoshinori Sumita, and Izumi Asahina. 2023. "A Prospective Study of the Assessment of the Efficacy of a Biodegradable Poly(l-lactic acid/ε-caprolactone) Membrane for Guided Bone Regeneration" Journal of Clinical Medicine 12, no. 18: 5994. https://doi.org/10.3390/jcm12185994
APA StyleShido, R., Ohba, S., Tominaga, R., Sumita, Y., & Asahina, I. (2023). A Prospective Study of the Assessment of the Efficacy of a Biodegradable Poly(l-lactic acid/ε-caprolactone) Membrane for Guided Bone Regeneration. Journal of Clinical Medicine, 12(18), 5994. https://doi.org/10.3390/jcm12185994