
ANRIL rs4977574 Gene Polymorphism in Women with Recurrent Pregnancy Loss
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. DNA Isolation and Detection of ANRIL rs4977574 Gene Polymorphism
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
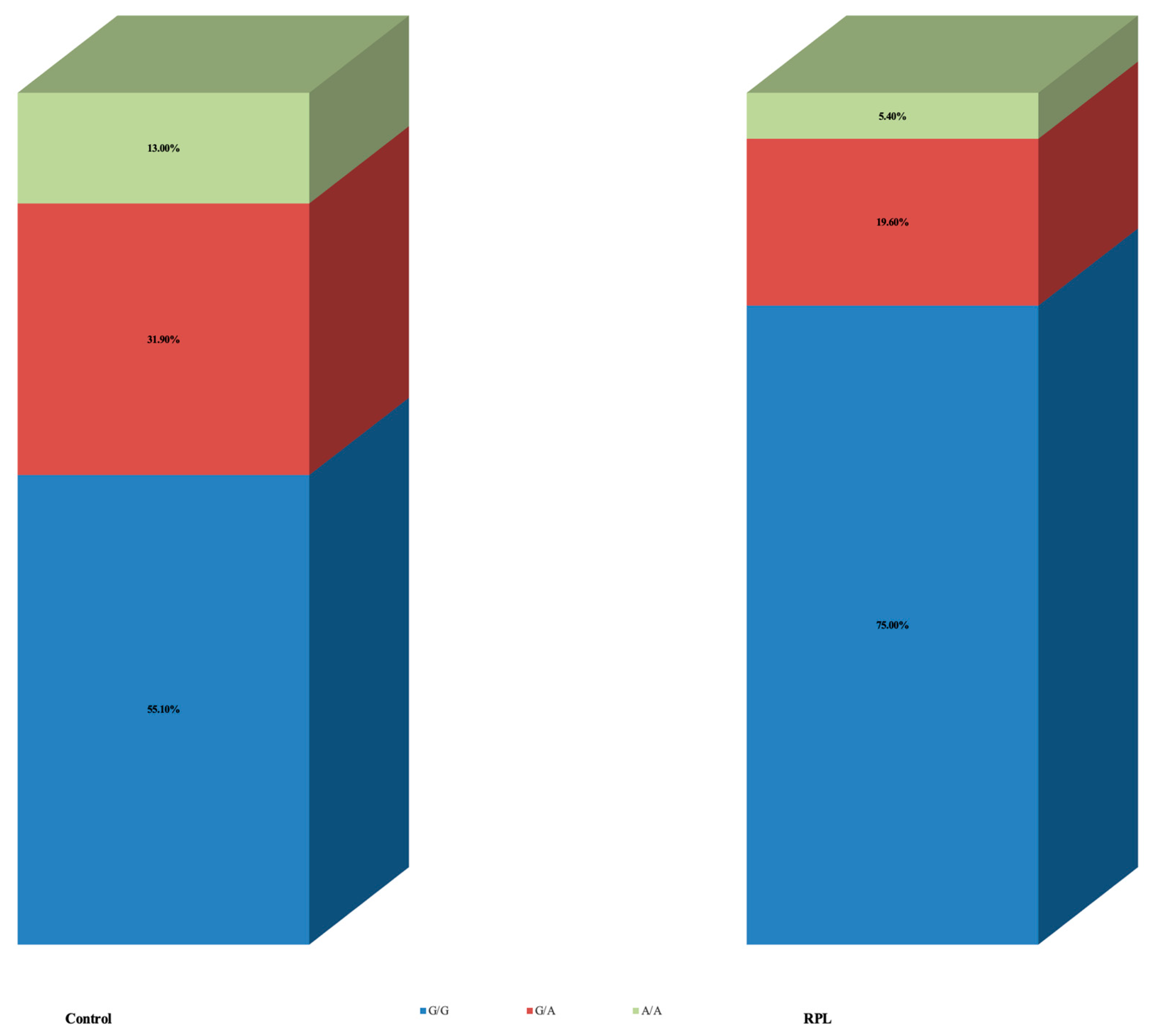
3.2. ANRIL rs4977574 Gene Polymorphism in RPL and Control Groups
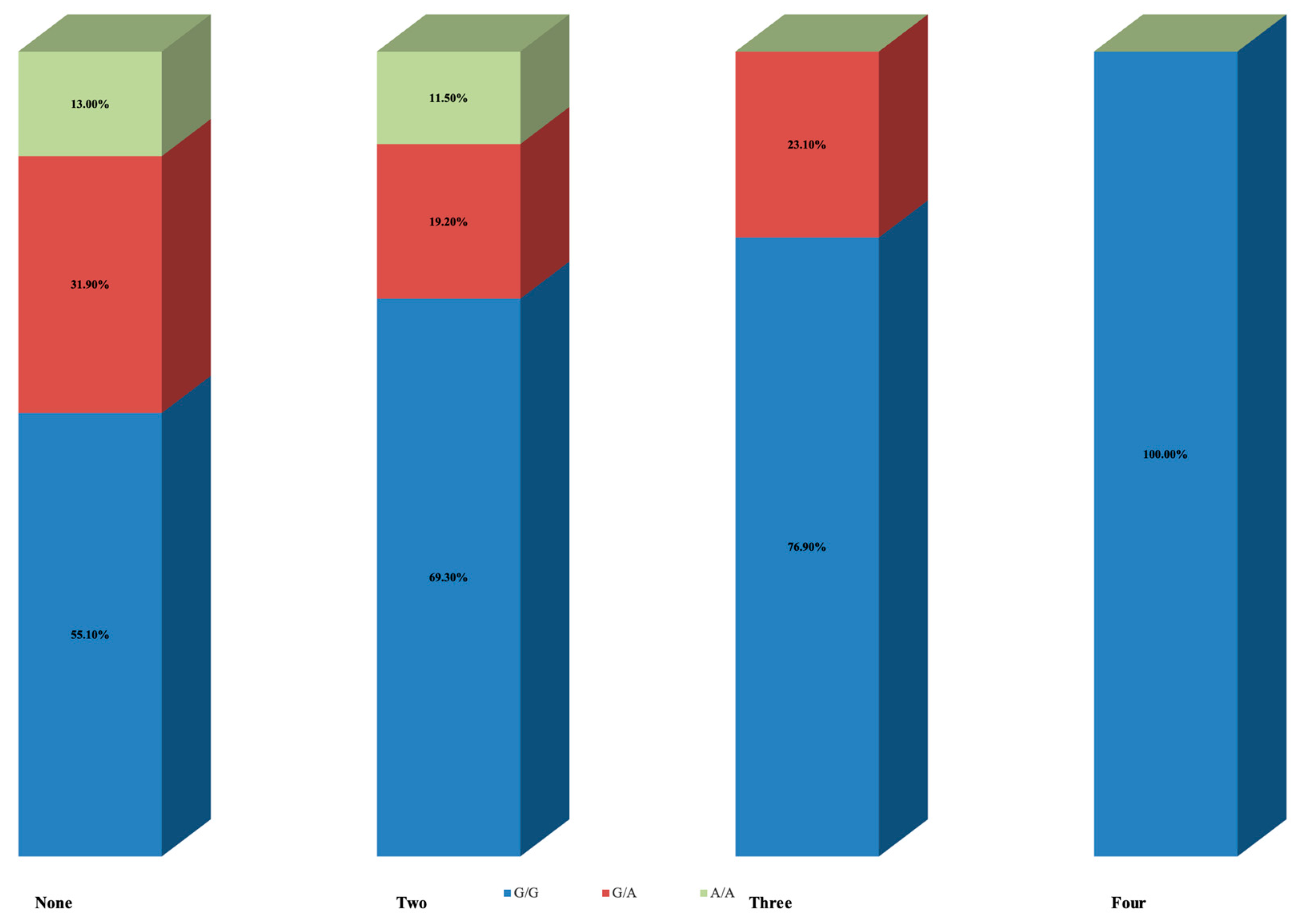
3.3. ANRIL rs4977574 Gene Polymorphism Depending on Number of Pregnancy Losses
3.4. ANRIL rs4977574 Gene Polymorphism in Women with 2 and 3 Pregnancy Losses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rasmark Roepke, E.; Matthiesen, L.; Rylance, R.; Christiansen, O.B. Is the incidence of recurrent pregnancy loss increasing? A retrospective register-based study in Sweden. Acta Obstet. Gynecol. Scand. 2017, 96, 1365–1372. [Google Scholar] [CrossRef] [PubMed]
- Magnus, M.C.; Wilcox, A.J.; Morken, N.H.; Weinberg, C.R.; Haberg, S.E. Role of maternal age and pregnancy history in risk of miscarriage: Prospective register based study. BMJ 2019, 364, l869. [Google Scholar] [CrossRef]
- The ESHRE Guideline Group on RPL; Bender Atik, R.; Christiansen, O.B.; Elson, J.; Kolte, A.M.; Lewis, S.; Middeldorp, S.; Nelen, W.; Peramo, B.; Quenby, S.; et al. ESHRE guideline: Recurrent pregnancy loss. Hum. Reprod. Open 2018, 2018, hoy004. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Evidence-based treatments for couples with unexplained infertility: A guideline. Fertil. Steril. 2020, 113, 305–322. [Google Scholar] [CrossRef]
- Preston, F.E.; Rosendaal, F.R.; Walker, I.D.; Briet, E.; Berntorp, E.; Conard, J.; Fontcuberta, J.; Makris, M.; Mariani, G.; Noteboom, W.; et al. Increased fetal loss in women with heritable thrombophilia. Lancet 1996, 348, 913–916. [Google Scholar] [CrossRef]
- Kutteh, W.H.; Triplett, D.A. Thrombophilias and recurrent pregnancy loss. Semin. Reprod. Med. 2006, 24, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Bates, S.M.; Middeldorp, S.; Rodger, M.; James, A.H.; Greer, I. Guidance for the treatment and prevention of obstetric-associated venous thromboembolism. J. Thromb. Thrombolysis 2016, 41, 92–128. [Google Scholar] [CrossRef]
- Jauniaux, E.; Farquharson, R.G.; Christiansen, O.B.; Exalto, N. Evidence-based guidelines for the investigation and medical treatment of recurrent miscarriage. Hum. Reprod. 2006, 21, 2216–2222. [Google Scholar] [CrossRef]
- Murugappan, G.; Leonard, S.A.; Farland, L.V.; Lau, E.S.; Shadyab, A.H.; Wild, R.A.; Schnatz, P.; Carmichael, S.L.; Stefanick, M.L.; Parikh, N.I. Association of infertility with atherosclerotic cardiovascular disease among postmenopausal participants in the Women’s Health Initiative. Fertil. Steril. 2022, 117, 1038–1046. [Google Scholar] [CrossRef] [PubMed]
- Samani, N.J.; Erdmann, J.; Hall, A.S.; Hengstenberg, C.; Mangino, M.; Mayer, B.; Dixon, R.J.; Meitinger, T.; Braund, P.; Wichmann, H.E.; et al. Genomewide association analysis of coronary artery disease. N. Engl. J. Med. 2007, 357, 443–453. [Google Scholar] [CrossRef]
- Burd, C.E.; Jeck, W.R.; Liu, Y.; Sanoff, H.K.; Wang, Z.; Sharpless, N.E. Expression of linear and novel circular forms of an INK4/ARF-associated non-coding RNA correlates with atherosclerosis risk. PLoS Genet. 2010, 6, e1001233. [Google Scholar] [CrossRef]
- Hubberten, M.; Bochenek, G.; Chen, H.; Hasler, R.; Wiehe, R.; Rosenstiel, P.; Jepsen, S.; Dommisch, H.; Schaefer, A.S. Linear isoforms of the long noncoding RNA CDKN2B-AS1 regulate the c-myc-enhancer binding factor RBMS1. Eur. J. Hum. Genet. 2019, 27, 80–89. [Google Scholar] [CrossRef]
- Rivera, N.V.; Carreras-Torres, R.; Roncarati, R.; Viviani-Anselmi, C.; De Micco, F.; Mezzelani, A.; Koch, W.; Hoppmann, P.; Kastrati, A.; Stewart, A.F.; et al. Assessment of the 9p21.3 locus in severity of coronary artery disease in the presence and absence of type 2 diabetes. BMC Med. Genet. 2013, 14, 11. [Google Scholar] [CrossRef]
- Broadbent, H.M.; Peden, J.F.; Lorkowski, S.; Goel, A.; Ongen, H.; Green, F.; Clarke, R.; Collins, R.; Franzosi, M.G.; Tognoni, G.; et al. Susceptibility to coronary artery disease and diabetes is encoded by distinct, tightly linked SNPs in the ANRIL locus on chromosome 9p. Hum. Mol. Genet. 2008, 17, 806–814. [Google Scholar] [CrossRef]
- Burdon, K.P.; Macgregor, S.; Hewitt, A.W.; Sharma, S.; Chidlow, G.; Mills, R.A.; Danoy, P.; Casson, R.; Viswanathan, A.C.; Liu, J.Z.; et al. Genome-wide association study identifies susceptibility loci for open angle glaucoma at TMCO1 and CDKN2B-AS1. Nat. Genet. 2011, 43, 574–578. [Google Scholar] [CrossRef]
- Cugino, D.; Gianfagna, F.; Santimone, I.; de Gaetano, G.; Donati, M.B.; Iacoviello, L.; Di Castelnuovo, A. Type 2 diabetes and polymorphisms on chromosome 9p21: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Emanuele, E.; Lista, S.; Ghidoni, R.; Binetti, G.; Cereda, C.; Benussi, L.; Maletta, R.; Bruni, A.C.; Politi, P. Chromosome 9p21.3 genotype is associated with vascular dementia and Alzheimer’s disease. Neurobiol. Aging 2011, 32, 1231–1235. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.; Hsieh, C.H.; Alonso, L.C. ANRIL: A lncRNA at the CDKN2A/B Locus With Roles in Cancer and Metabolic Disease. Front. Endocrinol. 2018, 9, 405. [Google Scholar] [CrossRef] [PubMed]
- Ramdas, W.D.; van Koolwijk, L.M.; Lemij, H.G.; Pasutto, F.; Cree, A.J.; Thorleifsson, G.; Janssen, S.F.; Jacoline, T.B.; Amin, N.; Rivadeneira, F.; et al. Common genetic variants associated with open-angle glaucoma. Hum. Mol. Genet. 2011, 20, 2464–2471. [Google Scholar] [CrossRef]
- Schaefer, A.S.; Richter, G.M.; Groessner-Schreiber, B.; Noack, B.; Nothnagel, M.; El Mokhtari, N.E.; Loos, B.G.; Jepsen, S.; Schreiber, S. Identification of a shared genetic susceptibility locus for coronary heart disease and periodontitis. PLoS Genet. 2009, 5, e1000378. [Google Scholar] [CrossRef]
- Uno, S.; Zembutsu, H.; Hirasawa, A.; Takahashi, A.; Kubo, M.; Akahane, T.; Aoki, D.; Kamatani, N.; Hirata, K.; Nakamura, Y. A genome-wide association study identifies genetic variants in the CDKN2BAS locus associated with endometriosis in Japanese. Nat. Genet. 2010, 42, 707–710. [Google Scholar] [CrossRef]
- Consortium, E.P. An integrated encyclopedia of DNA elements in the human genome. Nature 2012, 489, 57–74. [Google Scholar] [CrossRef] [PubMed]
- Nanda, V.; Downing, K.P.; Ye, J.; Xiao, S.; Kojima, Y.; Spin, J.M.; DiRenzo, D.; Nead, K.T.; Connolly, A.J.; Dandona, S.; et al. CDKN2B Regulates TGFbeta Signaling and Smooth Muscle Cell Investment of Hypoxic Neovessels. Circ. Res. 2016, 118, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Papait, R.; Kunderfranco, P.; Stirparo, G.G.; Latronico, M.V.; Condorelli, G. Long noncoding RNA: A new player of heart failure? J. Cardiovasc. Transl. Res. 2013, 6, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Zollbrecht, C.; Grassl, M.; Fenk, S.; Hocherl, R.; Hubauer, U.; Reinhard, W.; Esslinger, U.B.; Ebert, S.; Langmann, T.; Stark, K.; et al. Expression pattern in human macrophages dependent on 9p21.3 coronary artery disease risk locus. Atherosclerosis 2013, 227, 244–249. [Google Scholar] [CrossRef]
- Jin, W.; Wu, W.; Yang, K.; Shen, F.; Fu, N.; Feng, Y.; Fu, Y. The Single Nucleotide Polymorphisms of Chromosome 9p21 and CD147 Were Relevant with the Carotid Plaque Risk in Acute Cerebral Infarction Patients Among Chinese Han Population. J. Mol. Neurosci. 2020, 70, 1282–1292. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Song, L.; Jiang, L.; Tang, X.; Xu, L.; Gao, Z.; Zhao, X.; Xu, J.; Gao, R.; Yuan, J. Susceptible gene polymorphism in patients with three-vessel coronary artery disease. BMC Cardiovasc. Disord. 2020, 20, 172. [Google Scholar] [CrossRef]
- Lu, Z.; Zhang, Y.; Maimaiti, Y.; Feng, Y.; Sun, J.; Zhuang, J.; Zeng, L.; Fu, Y. Variants on Chromosome 9p21 Confer Risks of Noncardioembolic Cerebral Infarction and Carotid Plaque in the Chinese Han Population. J. Atheroscler. Thromb. 2015, 22, 1061–1070. [Google Scholar] [CrossRef]
- Sakalar, C.; Gurbuz, E.; Kalay, N.; Kaya, M.G. Higher frequency of rs4977574 (the G Allele) on chromosome 9p21.3 in patients with myocardial infarction as revealed by PCR-RFLP analysis. Tohoku J. Exp. Med. 2013, 230, 171–176. [Google Scholar] [CrossRef]
- Xu, B.; Fang, Z.; He, S.; Wang, J.; Yang, X. ANRIL polymorphism rs4977574 is associated with increased risk of coronary artery disease in Asian populations: A meta-analysis of 12,005 subjects. Medicine 2018, 97, e12641. [Google Scholar] [CrossRef]
- Lasek-Bal, A.; Kula, D.; Urbanek, T.; Puz, P.; Szymszal, J.; Jarzab, M.; Halczok, M.; Cyplinska, R.; Bal, W.; Labuz-Roszak, B.; et al. The Association of SNPs Located in the CDKN2B-AS1 and LPA Genes With Carotid Artery Stenosis and Atherogenic Stroke. Front. Neurol. 2019, 10, 1170. [Google Scholar] [CrossRef]
- Congrains, A.; Kamide, K.; Oguro, R.; Yasuda, O.; Miyata, K.; Yamamoto, E.; Kawai, T.; Kusunoki, H.; Yamamoto, H.; Takeya, Y.; et al. Genetic variants at the 9p21 locus contribute to atherosclerosis through modulation of ANRIL and CDKN2A/B. Atherosclerosis 2012, 220, 449–455. [Google Scholar] [CrossRef]
- Jarinova, O.; Stewart, A.F.; Roberts, R.; Wells, G.; Lau, P.; Naing, T.; Buerki, C.; McLean, B.W.; Cook, R.C.; Parker, J.S.; et al. Functional analysis of the chromosome 9p21.3 coronary artery disease risk locus. Arterioscler. Thromb. Vasc. Biol. 2009, 29, 1671–1677. [Google Scholar] [CrossRef]
- Zhou, X.; Han, X.; Wittfeldt, A.; Sun, J.; Liu, C.; Wang, X.; Gan, L.M.; Cao, H.; Liang, Z. Long non-coding RNA ANRIL regulates inflammatory responses as a novel component of NF-kappaB pathway. RNA Biol. 2016, 13, 98–108. [Google Scholar] [CrossRef]
- Bai, Y.; Nie, S.; Jiang, G.; Zhou, Y.; Zhou, M.; Zhao, Y.; Li, S.; Wang, F.; Lv, Q.; Huang, Y.; et al. Regulation of CARD8 expression by ANRIL and association of CARD8 single nucleotide polymorphism rs2043211 (p.C10X) with ischemic stroke. Stroke 2014, 45, 383–388. [Google Scholar] [CrossRef]
- Thomas, A.A.; Feng, B.; Chakrabarti, S. ANRIL: A Regulator of VEGF in Diabetic Retinopathy. Investig. Ophthalmol. Vis. Sci. 2017, 58, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Aguilo, F.; Di Cecilia, S.; Walsh, M.J. Long Non-coding RNA ANRIL and Polycomb in Human Cancers and Cardiovascular Disease. Curr. Top. Microbiol. Immunol. 2016, 394, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Katsiki, N.; Tziomalos, K.; Chatzizisis, Y.; Elisaf, M.; Hatzitolios, A.I. Effect of HMG-CoA reductase inhibitors on vascular cell apoptosis: Beneficial or detrimental? Atherosclerosis 2010, 211, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Xu, T.Y.; Guan, Y.F.; Zhao, Y.; Li, Z.Y.; Lan, X.H.; Wang, X.; Yang, P.Y.; Kang, Z.M.; Vanhoutte, P.M.; et al. Vascular smooth muscle cell apoptosis is an early trigger for hypothyroid atherosclerosis. Cardiovasc. Res. 2014, 102, 448–459. [Google Scholar] [CrossRef] [PubMed]
- Gil, J.; Peters, G. Regulation of the INK4b-ARF-INK4a tumour suppressor locus: All for one or one for all. Nat. Rev. Mol. Cell Biol. 2006, 7, 667–677. [Google Scholar] [CrossRef]
- Rudiger, N.S.; Gregersen, N.; Kielland-Brandt, M.C. One short well conserved region of Alu-sequences is involved in human gene rearrangements and has homology with prokaryotic chi. Nucleic Acids Res. 1995, 23, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Chi, J.S.; Li, J.Z.; Jia, J.J.; Zhang, T.; Liu, X.M.; Yi, L. Long non-coding RNA ANRIL in gene regulation and its duality in atherosclerosis. J. Huazhong Univ. Sci. Technol. Med. Sci. 2017, 37, 816–822. [Google Scholar] [CrossRef] [PubMed]
- Hueso, M.; Cruzado, J.M.; Torras, J.; Navarro, E. ALUminating the Path of Atherosclerosis Progression: Chaos Theory Suggests a Role for Alu Repeats in the Development of Atherosclerotic Vascular Disease. Int. J. Mol. Sci. 2018, 19, 1734. [Google Scholar] [CrossRef]
- Li, Y.Y.; Wang, H.; Zhang, Y.Y. CDKN2B-AS1 gene rs4977574 A/G polymorphism and coronary heart disease: A meta-analysis of 40,979 subjects. J. Cell Mol. Med. 2021, 25, 8877–8889. [Google Scholar] [CrossRef] [PubMed]
- Kunnas, T.; Piesanen, J.; Nikkari, S.T. Association of a Chromosome Locus 9p21.3 CDKN2B-AS1 Variant rs4977574 with Hypertension: The TAMRISK Study. Genet. Test. Mol. Biomark. 2018, 22, 327–330. [Google Scholar] [CrossRef]
- Hindy, G.; Ericson, U.; Hamrefors, V.; Drake, I.; Wirfalt, E.; Melander, O.; Orho-Melander, M. The chromosome 9p21 variant interacts with vegetable and wine intake to influence the risk of cardiovascular disease: A population based cohort study. BMC Med. Genet. 2014, 15, 1220. [Google Scholar] [CrossRef]
- Hamrefors, V.; Hedblad, B.; Hindy, G.; Smith, J.G.; Almgren, P.; Engstrom, G.; Sjogren, M.; Gransbo, K.; Orho-Melander, M.; Melander, O. Smoking modifies the associated increased risk of future cardiovascular disease by genetic variation on chromosome 9p21. PLoS ONE 2014, 9, e85893. [Google Scholar] [CrossRef]
- Boots, C.; Stephenson, M.D. Does obesity increase the risk of miscarriage in spontaneous conception: A systematic review. Semin. Reprod. Med. 2011, 29, 507–513. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | All RPL | 2 Losses | 3 Losses | 4 Losses | p-Value * |
|---|---|---|---|---|---|
| (Ν = 56) | (Ν = 26) | (Ν = 26) | (Ν = 4) | ||
| Women’s age | |||||
| (years) | |||||
| Mean (SD) | 35.0 (5.7) | 33.1 (5.6) | 36.7 (5.2) | 35.8 (7.3) | |
| Median (IQR) | 35.0 (31.0, 40.0) | 33.0 (30.0, 38.0) | 38.0 (32.0, 41.0) | 34.0 (30.0, 43.3) | 0.019 |
| BMI | |||||
| (kg/m2) | |||||
| Mean (SD) | 23.0 (3.1) | 23.1 (3.2) | 22.8 (3.1) | 24.7 (0.4) | |
| Median (IQR) | 22.5 (20.3, 25.1) | 22.7 (20.7, 24.2) | 22.1 (20.2, 25.7) | 24.7 (24.7, -) | 0.914 |
| Partner’s age | |||||
| (years) | |||||
| Mean (SD) | 37.9 (5.8) | 34.5 (3.7) | 40.7 (6.7) | 36.5 (0.7) | |
| Median (IQR) | 37.0 (34.0, 40.0) | 34.5 (31.8, 38.5) | 37 (36, 46) | 36.5 (36.0, -) | 0.027 |
| ANRIL rs4977574 Polymorphism | Controls (n = 69) | RPL (n = 56) | p-Value |
|---|---|---|---|
| G/G | 38 (55.1%) | 42 (75.0%) | |
| G/A | 22 (31.9%) | 11 (19.6%) | 0.062, for genotype |
| A/A | 9 (13.0%) | 3 (5.4%) | 0.021, for allele A |
| ANRIL rs4977574 Polymorphism | None (n = 69) | Two (n = 26) | Three (n = 26) | Four (n = 4) | p-Value |
|---|---|---|---|---|---|
| G/G | 38 (55.1%) | 18 (69.3%) | 20 (76.9%) | 4 (100%) | |
| G/A | 22 (31.9%) | 5 (19.2%) | 6 (23.1%) | 0 (0.0%) | 0.188, for genotype |
| A/A | 9 (13.0%) | 3 (11.5%) | 0 (0.0%) | 0 (0.0%) | 0.078, for allele A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cherouveim, P.; Mavrogianni, D.; Drakaki, E.; Potiris, A.; Zikopoulos, A.; Papamentzelopoulou, M.; Kouvoutsaki, K.; Machairiotis, N.; Karampitsakos, T.; Skentou, C.; et al. ANRIL rs4977574 Gene Polymorphism in Women with Recurrent Pregnancy Loss. J. Clin. Med. 2023, 12, 5944. https://doi.org/10.3390/jcm12185944
Cherouveim P, Mavrogianni D, Drakaki E, Potiris A, Zikopoulos A, Papamentzelopoulou M, Kouvoutsaki K, Machairiotis N, Karampitsakos T, Skentou C, et al. ANRIL rs4977574 Gene Polymorphism in Women with Recurrent Pregnancy Loss. Journal of Clinical Medicine. 2023; 12(18):5944. https://doi.org/10.3390/jcm12185944
Chicago/Turabian StyleCherouveim, Panagiotis, Despoina Mavrogianni, Eirini Drakaki, Anastasios Potiris, Athanasios Zikopoulos, Myrto Papamentzelopoulou, Konstantina Kouvoutsaki, Nikolaos Machairiotis, Theodoros Karampitsakos, Chara Skentou, and et al. 2023. "ANRIL rs4977574 Gene Polymorphism in Women with Recurrent Pregnancy Loss" Journal of Clinical Medicine 12, no. 18: 5944. https://doi.org/10.3390/jcm12185944
APA StyleCherouveim, P., Mavrogianni, D., Drakaki, E., Potiris, A., Zikopoulos, A., Papamentzelopoulou, M., Kouvoutsaki, K., Machairiotis, N., Karampitsakos, T., Skentou, C., Domali, E., Vrachnis, N., Drakakis, P., & Stavros, S. (2023). ANRIL rs4977574 Gene Polymorphism in Women with Recurrent Pregnancy Loss. Journal of Clinical Medicine, 12(18), 5944. https://doi.org/10.3390/jcm12185944