

The Effects of BCDs in Unilateral Conductive Hearing Loss: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Methods
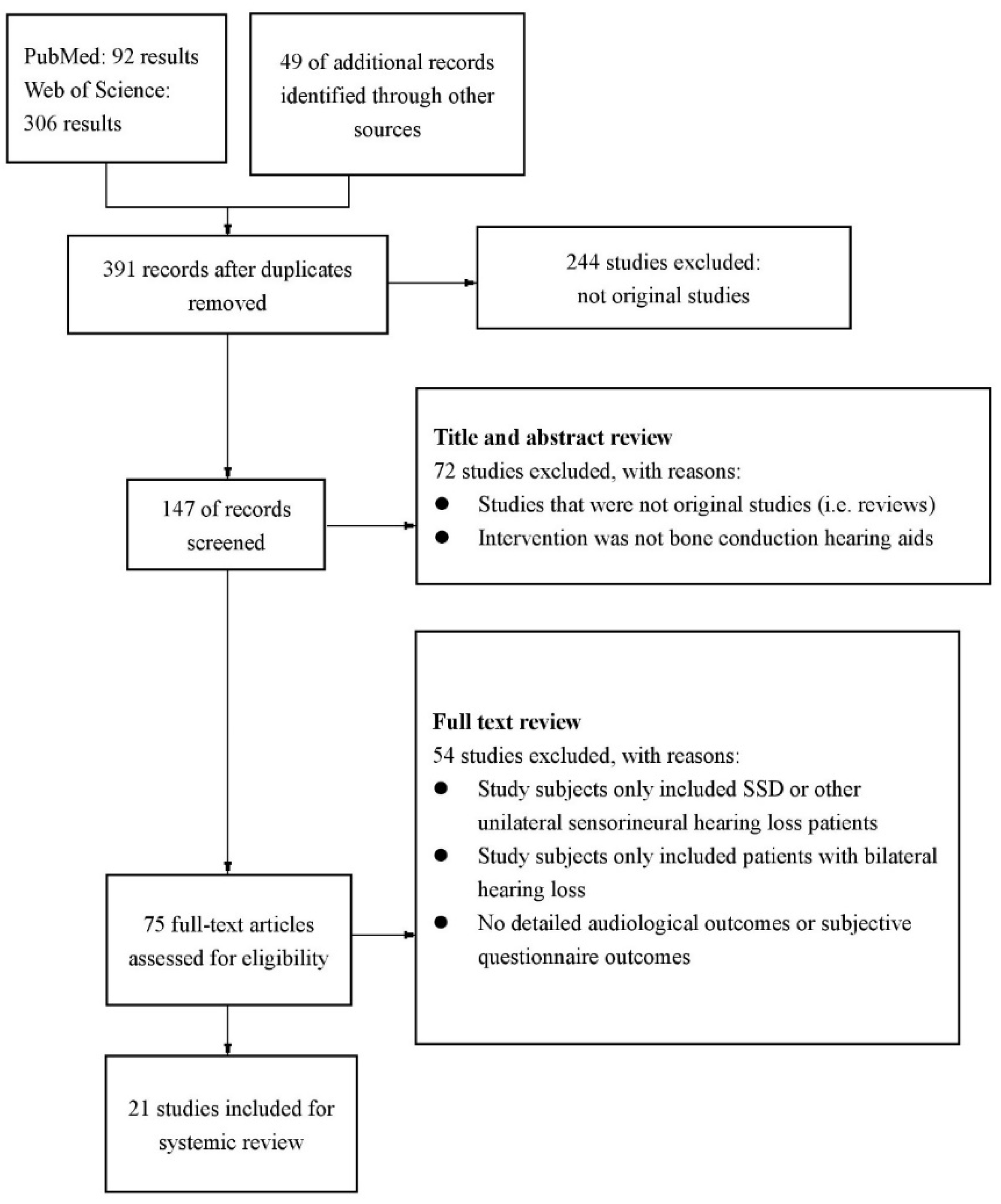
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Analysis
3. Results
3.1. General Characteristics of the Studies

{kind=link}
| Study (Year) | Study Design | Patient Characteristics | Bone-Conduction Hearing Device | ||
|---|---|---|---|---|---|
| Mean Age at Time of Study (Range) | N | Type of Unilateral Hearing Loss | |||
| Brotto (2023) [16] | prospective | 9 (6–11) | 10 | conductive | BAHA |
| Luque (2023) [17] | retrospective | 10 (5–17) | 9 | conductive | Baha Attract system |
| Marszał (2022) [10] | prospective | 41.1 (22–50) | 7 | mixed or conductive | Baha Attract system |
| Cywka (2021) [9] | prospective | 1.2 (0.4–1.6) | 21 | mixed or conductive | Softband BCHA |
| Kuthubutheen (2020) [15] | prospective | 40.3 (11–70) | 12 | conductive | BAHA; ADHEAR |
| de Wolf (2011) [11] | retrospective | 9 (5–16) | 15 | conductive | BAHA |
| Kunst (2008) [18,19] | prospective | 17.25 (5–61) | 20 | conductive | BAHA |
| Priwin (2007) [8] | prospective | 9.4 (6–17) | 13 | conductive | BAHA |
| Hol (2005) [14] | prospective | 43.2 (16–66) | 18 | conductive | BAHA |
| Snik (2002) [20] | prospective | 39.4 (19–51) | 8 | conductive | BAHA |
| Wazen (2001) [21] | prospective | 45 (23–76) | 9 | mixed or conductive | BAHA |
| Nelissen (2016) [22] | retrospective | 7.8 (5–11) | 12 | conductive | Sophono and BAHA |
| Polonenko (2016) [23] | retrospective | 12.1 (5–17) | 9 | conductive | Sophono |
| Denoyelle (2015) [24] | prospective | 8.1 (5.1–10.8) | 15 | conductive | Sophono |
| Vogt (2018) [7] | prospective | 11.3 (3.5–17.9) | 9 | conductive | BoneBridge |
| Vyskocil (2017) [25] | prospective | 35.2 (14–50) | 5 | conductive | BoneBridge |
| Liu (2022) [6] | prospective | 7.45 (5–11) | 11 | conductive | ADHEAR |
| Liu (2021) [26] | retrospective | 7.8 (5–15) | 13 | conductive | ADHEAR |
| Hirth (2021) [27] | prospective | 7 (4.0–16.7) | 10 | conductive | ADHEAR |
| Osborne (2019) [13] | prospective | 9 (5–15) | 20 | conductive | ADHEAR and Ponto |
3.2. Audiological Outcomes
3.2.1. PTA and Sound Field Hearing Threshold Gain
3.2.2. Speech Recognition
3.2.3. Sound Localization
3.3. Subjective Outcomes
3.3.1. APHAB
3.3.2. GBI&GCBI
3.3.3. SSQ
3.3.4. IOI-HA
3.3.5. ADHEAR Use and Satisfaction Questionnaire
3.3.6. MAIS&MUSS
3.3.7. Other Subjective Questionnaire Outcomes
4. Discussion
4.1. Auditory Benefits and Wide Variations
4.2. Subjective Outcomes
4.3. Nuts and Bolts of Different BCDs
4.4. Advices for Clinical Intervention
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Neumann, K.; Thomas, J.P.; Voelter, C.; Dazert, S. A new adhesive bone conduction hearing system effectively treats conductive hearing loss in children. Int. J. Pediatr. Otorhinolaryngol. 2019, 122, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Tjellström, A.; Granström, G. Long-term follow-up with the bone-anchored hearing aid: A review of the first 100 patients between 1977 and 1985. Ear Nose Throat J. 1994, 73, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Maier, H.; Lenarz, T.; Agha-Mir-Salim, P.; Agterberg, M.J.H.; Anagiotos, A.; Arndt, S.; Ball, G.; Bance, M.; Maurizio, B.; Baumann, U.; et al. Consensus Statement on Bone Conduction Devices and Active Middle Ear Implants in Conductive and Mixed Hearing Loss. Otol. Neurotol. 2022, 43, 513–529. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Liu, Y.; Zhao, C.; Yang, L.; Chen, P.; Yang, J.; Wang, D.; Ren, R.; Li, Y.; Zhao, S.; Gong, S. Characteristics of sound localization in children with unilateral microtia and atresia and predictors of localization improvement when using a bone conduction device. Front. Neurosci. 2022, 16, 973735. [Google Scholar] [CrossRef]
- Vogt, K.; Frenzel, H.; Ausili, S.A.; Hollfelder, D.; Wollenberg, B.; Snik, A.F.M.; Agterberg, M.J.H. Improved directional hearing of children with congenital unilateral conductive hearing loss implanted with an active bone-conduction implant or an active middle ear implant. Hear. Res. 2018, 370, 238–247. [Google Scholar] [CrossRef]
- Priwin, C.; Jönsson, R.; Hultcrantz, M.; Granström, G. BAHA in children and adolescents with unilateral or bilateral conductive hearing loss: A study of outcome. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 135–145. [Google Scholar] [CrossRef]
- Cywka, K.B.; Krol, B.; Skarzynski, P.H. Effectiveness of Bone Conduction Hearing Aids in Young Children with Congenital Aural Atresia and Microtia. Med. Sci. Monit. 2021, 27, e933915-1. [Google Scholar] [CrossRef]
- Marszal, J.; Bartkowiak, E.; Miechowicz, I.; Wierzbicka, M.; Gawecki, W. The Baha Attract System Implantations Significantly Improve the Quality of Life of Hearing-Impaired Patients in Long-Term Observations. J. Int. Adv. Otol. 2022, 18, 225–231. [Google Scholar] [CrossRef]
- De Wolf, M.J.F.; Hol, M.K.S.; Mylanus, E.A.M.; Snik, A.F.M.; Cremers, C.W.R.J. Benefit and Quality of Life After Bone-Anchored Hearing Aid Fitting in Children with Unilateral or Bilateral Hearing Impairment. Arch. Otolaryngol.-Head Neck Surg. 2011, 137, 130–138. [Google Scholar] [CrossRef]
- Priwin, C.; Jönsson, R.; Magnusson, L.; Hultcrantz, M.; Granström, G. Audiological evaluation and self-assessed hearing problems in subjects with single-sided congenital external ear malformations and associated conductive hearing loss. Int. J. Audiol. 2007, 46, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Osborne, M.S.; Child-Hymas, A.; Gill, J.; Lloyd, M.S.; McDermott, A.L. First Pediatric Experience with a Novel, Adhesive Adapter Retained, Bone Conduction Hearing Aid System. Otol. Neurotol. 2019, 40, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Hol, M.K.S.; Snik, A.F.M.; Mylanus, E.A.M.; Cremers, C. Does the bone-anchored hearing aid have a complementary effect on audiological and subjective outcomes in patients with unilateral conductive hearing loss? Audiol. Neuro-Otol. 2005, 10, 159–168. [Google Scholar] [CrossRef]
- Kuthubutheen, J.; Broadbent, C.; Marino, R.; Távora-Vieira, D. The Use of a Novel, Nonsurgical Bone Conduction Hearing Aid System for the Treatment of Conductive Hearing Loss. Otol. Neurotol. 2020, 41, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Brotto, D.; Sorrentino, F.; Cazzador, D.; Maritan, F.; Montino, S.; Agostinelli, A.; Zanoletti, E.; Martini, A.; Bovo, R.; Trevisi, P. Benefits of bone conduction hearing aid in children with unilateral aural atresia. Acta Otorhinolaryngol. Ital. 2023, 43, 221–226. [Google Scholar] [CrossRef]
- Luque, C.G.; Liu, A.Q.; Pauwels, J.; Leitmeyer, K.; Chadha, N.K. Patient reported outcome measures in unilateral aural atresia treated using a transcutaneous bone conduction implant (The Cochlear Baha Attract®). Int. J. Pediatr. Otorhinolaryngol. 2023, 165, 111451. [Google Scholar] [CrossRef]
- Kunst, S.J.W.; Leijendeckers, J.M.; Mylanus, E.A.M.; Hol, M.K.S.; Snik, A.F.M.; Cremers, C.W.R.J. Bone-anchored hearing aid system application for unilateral congenital conductive hearing impairment: Audiometric results. Otol. Neurotol. 2008, 29, 2–7. [Google Scholar] [CrossRef]
- Kunst, S.J.W.; Hol, M.K.S.; Mylanus, E.A.M.; Leijendeckers, J.M.; Snik, A.F.M.; Cremers, C.W.R.J. Subjective benefit after BAHA system application in patients with congenital unilateral conductive hearing impairment. Otol. Neurotol. 2008, 29, 353–358. [Google Scholar] [CrossRef]
- Snik, A.F.M.; Mylanus, E.A.M.; Cremers, C.W.R.J. The bone-anchored hearing aid in patients with a unilateral air-bone gap. Otol. Neurotol. 2002, 23, 61–66. [Google Scholar] [CrossRef]
- Wazen, J.J.; Spitzer, J.; Ghossaini, S.N.; Kacker, A.; Zschommler, A. Results of the bone-anchored hearing aid in unilateral hearing loss. Laryngoscope 2001, 111, 955–958. [Google Scholar] [CrossRef]
- Nelissen, R.C.; Agterberg, M.J.H.; Hol, M.K.S.; Snik, A.F.M. Three-year experience with the Sophono in children with congenital conductive unilateral hearing loss: Tolerability, audiometry, and sound localization compared to a bone-anchored hearing aid. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3149–3156. [Google Scholar] [CrossRef] [PubMed]
- Polonenko, M.J.; Carinci, L.; Gordon, K.A.; Papsin, B.C.; Cushing, S.L. Hearing Benefit and Rated Satisfaction in Children with Unilateral Conductive Hearing Loss Using a Transcutaneous Magnetic-Coupled Bone-Conduction Hearing Aid. J. Am. Acad. Audiol. 2016, 27, 790–804. [Google Scholar] [CrossRef] [PubMed]
- Denoyelle, F.; Coudert, C.; Thierry, B.; Parodi, M.; Mazzaschi, O.; Vicaut, E.; Tessier, N.; Loundon, N.; Garabedian, E.-N. Hearing rehabilitation with the closed skin bone-anchored implant Sophono Alpha1: Results of a prospective study in 15 children with ear atresia. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Vyskocil, E.; Liepins, R.; Kaider, A.; Blineder, M.; Hamzavi, S. Sound Localization in Patients with Congenital Unilateral Conductive Hearing Loss with a Transcutaneous Bone Conduction Implant. Otol. Neurotol. 2017, 38, 318–324. [Google Scholar] [CrossRef]
- Liu, Y.; Zhao, C.; Yang, J.; Chen, P.; Gao, M.; Wang, D.; Zhao, S. Audiological and subjective benefit with a new adhesive bone conduction hearing aid in children with congenital unilateral microtia and atresia. Eur. Arch. Oto-Rhino-Laryngol. 2021, 279, 4289–4301. [Google Scholar] [CrossRef]
- Hirth, D.; Weiss, R.; Stöver, T.; Kramer, S. Audiological benefit and subjective satisfaction with the ADHEAR hearing system in children with unilateral conductive hearing loss. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 2781–2788. [Google Scholar] [CrossRef]
- Legris, E.; Roux, S.; Aoustin, J.M.; Galvin, J.; Bakhos, D. Cortical auditory responses according to hearing rehabilitation in unilateral hearing loss. Eur. Ann. Otorhinolaryngol.-Head Neck Dis. 2019, 136, 439–445. [Google Scholar] [CrossRef]
- Ha, J.; Kim, H.; Lee, J.H.; Park, H.Y. Sound localization in patients with a unilateral hearing aid: Discordance between the right and left ears. Laryngoscope Investig. Otolaryngol. 2022, 7, 599–603. [Google Scholar] [CrossRef]
- Dun, C.A.J.; Agterberg, M.J.H.; Cremers, C.W.R.J.; Hol, M.K.S.; Snik, A.F.M. Bilateral Bone Conduction Devices: Improved Hearing Ability in Children with Bilateral Conductive Hearing Loss. Ear Hear. 2013, 34, 806–808. [Google Scholar] [CrossRef]
- Cox, R.M.; Alexander, G.C. The Abbreviated Profile of Hearing Aid Benefit. Ear Hear. 1995, 16, 176–186. [Google Scholar] [CrossRef]
- Robinson, K.; Gatehouse, S.; Browning, G.G. Measuring patient benefit from otorhinolaryngological surgery and therapy. Ann. Otol. Rhinol. Laryngol. 1996, 105, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Dutt, S.N.; McDermott, A.-L.; Jelbert, A.; Reid, A.P.; Proops, D.W. The Glasgow benefit inventory in the evaluation of patient satisfaction with the bone-anchored hearing aid: Quality of life issues. J. Laryngol. Otol. 2002, 116, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Kubba, H.; Swan, I.R.C.; Gatehouse, S. The Glasgow Children’s Benefit Inventory: A new instrument for assessing health-related benefit after an intervention. Ann. Otol. Rhinol. Laryngol. 2004, 113, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Gatehouse, S.; Noble, W. The Speech, Spatial and Qualities of Hearing Scale (SSQ). Int. J. Audiol. 2004, 43, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Robbins, A.M.; Renshaw, J.J.; Berry, S.W. Evaluating meaningful auditory integration in profoundly hearing-impaired children. Am. J. Otol. 1991, 12, 144–150. [Google Scholar]
- Chung, S.M.; Stephens, S.D. Factors influencing binaural hearing aid use. Br. J. Audiol. 1986, 20, 129–140. [Google Scholar] [CrossRef]
- Kompis, M.; Pfiffner, F.; Krebs, M.; Caversaccio, M.-D. Factors influencing the decision for Baha in unilateral deafness: The Bern benefit in single-sided deafness questionnaire. Adv. Oto-Rhino-Laryngol. 2011, 71, 103–111. [Google Scholar] [CrossRef]
- Newman, C.W.; Weinstein, B.E.; Jacobson, G.P.; Hug, G.A. The Hearing Handicap Inventory for Adults: Psychometric adequacy and audiometric correlates. Ear Hear. 1990, 11, 430–433. [Google Scholar] [CrossRef]
- Cox, R.M.; Alexander, G.C. Measuring Satisfaction with Amplification in Daily Life: The SADL scale. Ear Hear. 1999, 20, 306–320. [Google Scholar] [CrossRef]
- Agterberg, M.J.H.; Hol, M.K.S.; Cremers, C.W.R.J.; Mylanus, E.A.M.; van Opstal, A.J.; Snik, A.F.M. Conductive Hearing Loss and Bone Conduction Devices: Restored Binaural Hearing? In Implantable Bone Conduction Hearing Aids; Karger Publishers: Basel, Switzerland, 2011; Volume 71, pp. 84–91. [Google Scholar]
- Keating, P.; Rosenior-Patten, O.; Dahmen, J.C.; Bell, O.; King, A.J. Behavioral training promotes multiple adaptive processes following acute hearing loss. eLife 2016, 5, e12264. [Google Scholar] [CrossRef]
- Chen, S.Y.; Mancuso, D.; Lalwani, A.K. Skin Necrosis After Implantation with the BAHA Attract: A Case Report and Review of the Literature. Otol. Neurotol. 2017, 38, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Sambur, I.M.; Chandrasekhar, S.S.; Govindaraj, S. Traumatic wound breakdown following baha™ implant. Laryngoscope 2010, 120, S218. [Google Scholar] [CrossRef] [PubMed]
- Nelissen, R.C.; Stalfors, J.; de Wolf, M.J.F.; Flynn, M.C.; Wigren, S.; Eeg-Olofsson, M.; Green, K.; Rothera, M.P.; Mylanus, E.A.M.; Hol, M.K.S. Long-Term Stability, Survival, and Tolerability of a Novel Osseointegrated Implant for Bone Conduction Hearing: 3-Year Data from a Multicenter, Randomized, Controlled, Clinical Investigation. Otol. Neurotol. 2014, 35, 1486–1491. [Google Scholar] [CrossRef] [PubMed]
- Nelissen, R.C.; den Besten, C.A.; Mylanus, E.A.M.; Hol, M.K.S. Stability, survival, and tolerability of a 4.5-mm-wide bone-anchored hearing implant: 6-month data from a randomized controlled clinical trial. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Hol, M.K.S.; Nelissen, R.C.; Agterberg, M.J.H.; Cremers, C.W.R.J.; Snik, A.F.M. Comparison between a new implantable transcutaneous bone conductor and percutaneous bone-conduction hearing implant. Otol. Neurotol. 2013, 34, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Willenborg, K.; Lenarz, T.; Busch, S. Surgical and audiological outcomes with a new transcutaneous bone conduction device with reduced transducer thickness in children. Eur. Arch. Oto-Rhino-Laryngol. 2023, 280, 4381–4389. [Google Scholar] [CrossRef] [PubMed]
- Dahm, V.; Baumgartner, W.-D.; Liepins, R.; Arnoldner, C.; Riss, D. First Results with a New, Pressure-free, Adhesive Bone Conduction Hearing Aid. Otol. Neurotol. 2018, 39, 748–754. [Google Scholar] [CrossRef]
- Lieu, J.E. Unilateral hearing loss in children: Speech-language and school performance. B-Ent 2013, 21, 107–115. [Google Scholar]
- Kesser, B.W.; Krook, K.; Gray, L.C. Impact of unilateral conductive hearing loss due to aural atresia on academic performance in children. Laryngoscope 2013, 123, 2270–2275. [Google Scholar] [CrossRef]
- Bell, R.; Mouzourakis, M.; Wise, S.R. Impact of unilateral hearing loss in early development. Curr. Opin. Otolaryngol. Head Neck Surg. 2022, 30, 344–350. [Google Scholar] [CrossRef]
- Yang, T.; Liu, Q.; Fan, X.; Hou, B.; Wang, J.; Chen, X. Altered regional activity and connectivity of functional brain networks in congenital unilateral conductive hearing loss. Neuroimage Clin. 2021, 32, 102819. [Google Scholar] [CrossRef] [PubMed]
- Liberman, M.C.; Liberman, L.D.; Maison, S.F. Chronic Conductive Hearing Loss Leads to Cochlear Degeneration. PLoS ONE 2015, 10, e0142341. [Google Scholar] [CrossRef] [PubMed]
- Bouhabel, S.; Arcand, P.; Saliba, I. Congenital aural atresia: Bone-anchored hearing aid vs. external auditory canal reconstruction. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Nadaraja, G.S.; Gurgel, R.K.; Kim, J.; Chang, K.W. Hearing outcomes of atresia surgery versus osseointegrated bone conduction device in patients with congenital aural atresia: A systematic review. Otol. Neurotol. 2013, 34, 1394–1399. [Google Scholar] [CrossRef] [PubMed]
| Study | Measures | Main Outcomes |
|---|---|---|
| Wazen (2001) [21] | PTA gain | 500-Hz: 41.9 dB 1000-Hz: 66.3 dB 2000-Hz: 49.4 dB 4000-Hz: 45.6 dB |
| Snik (2002) [20] | Sound localization | MAE (significant change ≥ 16°)
|
| Speech recognition | SRT (Significant improvement at 5% level)
| |
| Hol (2005) [14] | Sound localization | Patients with normal bilateral cochlear function (all with acquired UCHL) MAE (significant change ≥ 16°)
MAE (significant change ≥ 16°)
|
| Speech recognition | Patients with normal bilateral cochlear function SRT (Significant improvement at 5% level)
SRT (Significant improvement at 5% level)
| |
| Kunst (2008) [18] | Sound localization | (all with congenital UCHL) Adults: mean unaided MAE score = 37° (significant change ≥ 16°)
|
| Speech recognition | Adults: SRT (improvement of >1.6 dB was significant)
Children: SRT (improvement of >1.6 dB was significant)
| |
| Denoyelle (2015) [24] | PTA gain | Mean aided ACPTA of 33.49 ± 4.89 dB; mean gain 35.53 dB (p < 0.0001) at M6 Mean aided ACPTA of 36.43 ± 4.61 dB at M12 |
| Nelissen (2016) [22] | Sound localization | MAA test (all with congenital UCHL)
|
| Polonenko (2016) [23] | Speech recognition | mean aided SRT 51.40 ± 10.99; SRT gain (−7.80 ± 4.11) (p < 0.001) at M6 mean aided SRT of 39 ± 5.86 dB at M12 |
| Vyskocil (2017) [25] | Functional hearing gain Speech recognition Sound localization | Average: 25.7 dB (±2.6)
S90N−90: 9.0 dB (8.8–11.4 dB) mean RMS error decreased by a factor of 0.71 (p < 0.001) |
| Vogt (2018) [7] | Sound localization | MAE: mean unaided MAE = 35.5° Stimuli at the impaired side: improvement by 17° (p = 0.02) Stimuli at the normal side: no significant improvement or deterioration |
| Osborne (2019) [13] | PTA gain Sound field hearing gain | 31 dB HL 26.3 dB HL |
| Kuthubutheen (2020) [15] | PTA gain Speech recognition | 27.5 dB HL unaided SNR = 2.23 aided SNR = 0.64 |
| Liu (2021) [26] | Sound field hearing gain Speech recognition | 500-Hz: 24.2 ± 6.4 dB HL 1000-Hz: 27.7 ± 7.8 dB HL 2000-Hz: 26.9 ± 10.5 dB HL 4000-Hz: 22.7 ± 8.1 dB HL
|
| Hirth (2021) [27] | Functional hearing gain Speech recognition | 19.6 dB HL (p < 0.0039)
in noise: 35% (n = 6, p < 0.0313)
signifcantly improved by 16.6 dB SPL to 52.8 ± 7.1 dB SPL using the hearing device (n = 9, p < 0.0195)
−1.7 ± 3.9 dB SNR aided |
| Functional hearing gain Speech recognition | 23.73 ± 3.47 dB HL (p < 0.01)
| |
| Liu (2022) [6] | Sound localization | (all with congenital UCHL)
|
| Luque (2023) [17] | PTA gain | 39.9 dB |
| Brotto (2023) [16] | PTA gain | 50.6 dB HL |
| Speech recognition |
S0N0+180 median SNR aided = −6.4 dB HL (significant improvement, p = 0.027) |
| Study | Questionnaire | Main Outcomes |
|---|---|---|
| Wazen (2001) [21] | HHIA | Preoperative: mean score = 25 (range, 10–40), falling in the “moderate” handicapped range. Postoperative: mean score = 10 (range, 0–14), falling in the borderline of “mild to moderate” handicap perception range. The reduction in handicap for the individual data for these unilaterally impaired listeners was dramatic. |
| Hol (2005) [14] | Chung and Stephens’ questionnaire | The majority of patients were using their BAHA 7 days a week for more than 8 h a day. The majority of the patients prefer using BAHA when listening to speech in both quiet and noisy situations. |
| Priwin (2007) [8] | MAIS&MUSS | Rare to occasional hearing aid use were reported in the UHL group. The aided and unaided scores was almost unchanged, and the aided verbal communication score even lowered. |
| IOI-HA | In the UCL with single sided BAHA amplification group, mean score all 7 items ≥3. High satisfaction rate and high quality of life were reported after fitted with hearing amplification. | |
| Kunst (2008) [19] | Chung and Stephens’ questionnaire | Most of the patients gave preference to using the BAHA system in several everyday situations. When asked whether they would recommend the BAHA to another patient with same hearing disability, all the patients gave a positive response. |
| GCBI | Overall benefit of +34 (children n = 10) | |
| SSQ | Unaided 4.5, aided 6.8 | |
| de Wolf (2011) [11] | Daily use | 47% were using their BAHA devices for more than 8 h a day, and 40% were using them for 4 to 8 h a day |
| GCBI | Total score 26 (mean = 22); physical health 16(mean = 19) | |
| APHAB | 27% experienced a significant overall benefit (scores of 10 + for each subdomain) | |
| HUI-3 | The overall mean utility score was 0.82 (0.12) | |
| Denoyelle (2015) [24] | MAIS&MUSS | At M12, all children used the implant 5 to 12 h daily (mean: 10 h) without cutaneous complications. Both children and parents reported being satisfied or very satisfied. The score for 7/10 questions in silence or noisy environment was statistically improved when wearing the device |
| Polonenko (2016) [23] | APHAB | only 3/8 children had minor changes in all three subscales and therefore significant overall benefit. All except two children reported a major change in at least one subscale, mainly background noise and reverberation |
| SADL | Median ratings of satisfaction (global score = 5.0, positive effect = 5.3, service and cost = 6.5, negative features = 5.0, personal image = 4.7) did not significantly differ from 5, or “considerably satisfied” for all subscales (p > 0.05), indicating adequate satisfaction with the device. | |
| Osborne (2019) [13] | LAS | The mean LAS score increased by 4.5 from 4 ± 1.4 to 8.5 ± 1.4 p = 0.0001 (95% CI 5.23–3.53) |
| GCBI | Overall GCBI response scores increased following the use of the adhesive retained BC system for 4 weeks by33 ± 25, further analysis shows a positive score in all four dimensions. | |
| Kuthubutheen (2020) [15] | SSQ12 | The mean unaided SSQ score was 73 which significantly improved to 83.9 with the BCHA device and 90.1 with the ADHEAR |
| ADHEAR Use and Satisfaction Questionnaire | Daily use: 5–14 h (mean: 8.9 h) Most patients considered the device ”valuable”. | |
| Liu (2021) [26] | IOI-HA | The mean score of the IOI-HA was 4.0 ± 0.5 without any negative comments |
| BBSS | the total score of all 10 questions was 27.1 ± 10.1 | |
| ADHEAR use and satisfaction questionnaire | The hearing device provided benefits in speech recognition ability in different complex situations, with high satisfaction rates. | |
| Hirth (2021) [27] | SSQ | significant increase from 6.5 ± 1.8 to 7.8 ± 1.0 (p = 0.0313) |
| Cywka (2021) [9] | LittlEARS | the average score increased significantly from pre-treatment period. The average difference of UHL group was 5.91 (p < 0.001; e2 = 0.264) |
| Marszał (2022) [10] | GBI | total score:20.6 ± 18.6 (p = 0.026), improvement general scale: 35.7 ± 28.7 points (p = 0.016), improvement physical health subscale: −14.3± 31.1 (p = 0.270) deterioration |
| APHAB | mean gain = 34.0% (p = 0.008) | |
| Liu (2022) [6] | IOI-HA | mean overall IOI-HA score = 4.57 ± 0.73 |
| SSQ | significant increase from 6.33 ± 1.82 to 8.37 ± 1.05 (p < 0.01) | |
| Luque (2023) [17] | GCBI | the median GCBI score was +14.6, indicating overall positive benefit 89% patients had an overall quality of life benefit largest improvement was found in behavior subscale |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.-Y.; Ren, L.-J.; Xie, Y.-Z.; Fu, Y.-Y.; Zhu, Y.-Y.; Li, C.-L.; Zhang, T.-Y. The Effects of BCDs in Unilateral Conductive Hearing Loss: A Systematic Review. J. Clin. Med. 2023, 12, 5901. https://doi.org/10.3390/jcm12185901
Wang X-Y, Ren L-J, Xie Y-Z, Fu Y-Y, Zhu Y-Y, Li C-L, Zhang T-Y. The Effects of BCDs in Unilateral Conductive Hearing Loss: A Systematic Review. Journal of Clinical Medicine. 2023; 12(18):5901. https://doi.org/10.3390/jcm12185901
Chicago/Turabian StyleWang, Xin-Yue, Liu-Jie Ren, You-Zhou Xie, Yao-Yao Fu, Ya-Ying Zhu, Chen-Long Li, and Tian-Yu Zhang. 2023. "The Effects of BCDs in Unilateral Conductive Hearing Loss: A Systematic Review" Journal of Clinical Medicine 12, no. 18: 5901. https://doi.org/10.3390/jcm12185901
APA StyleWang, X.-Y., Ren, L.-J., Xie, Y.-Z., Fu, Y.-Y., Zhu, Y.-Y., Li, C.-L., & Zhang, T.-Y. (2023). The Effects of BCDs in Unilateral Conductive Hearing Loss: A Systematic Review. Journal of Clinical Medicine, 12(18), 5901. https://doi.org/10.3390/jcm12185901