

The Influence of SARS-CoV-2 Infection on Acute Myocardial Infarction Outcomes
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
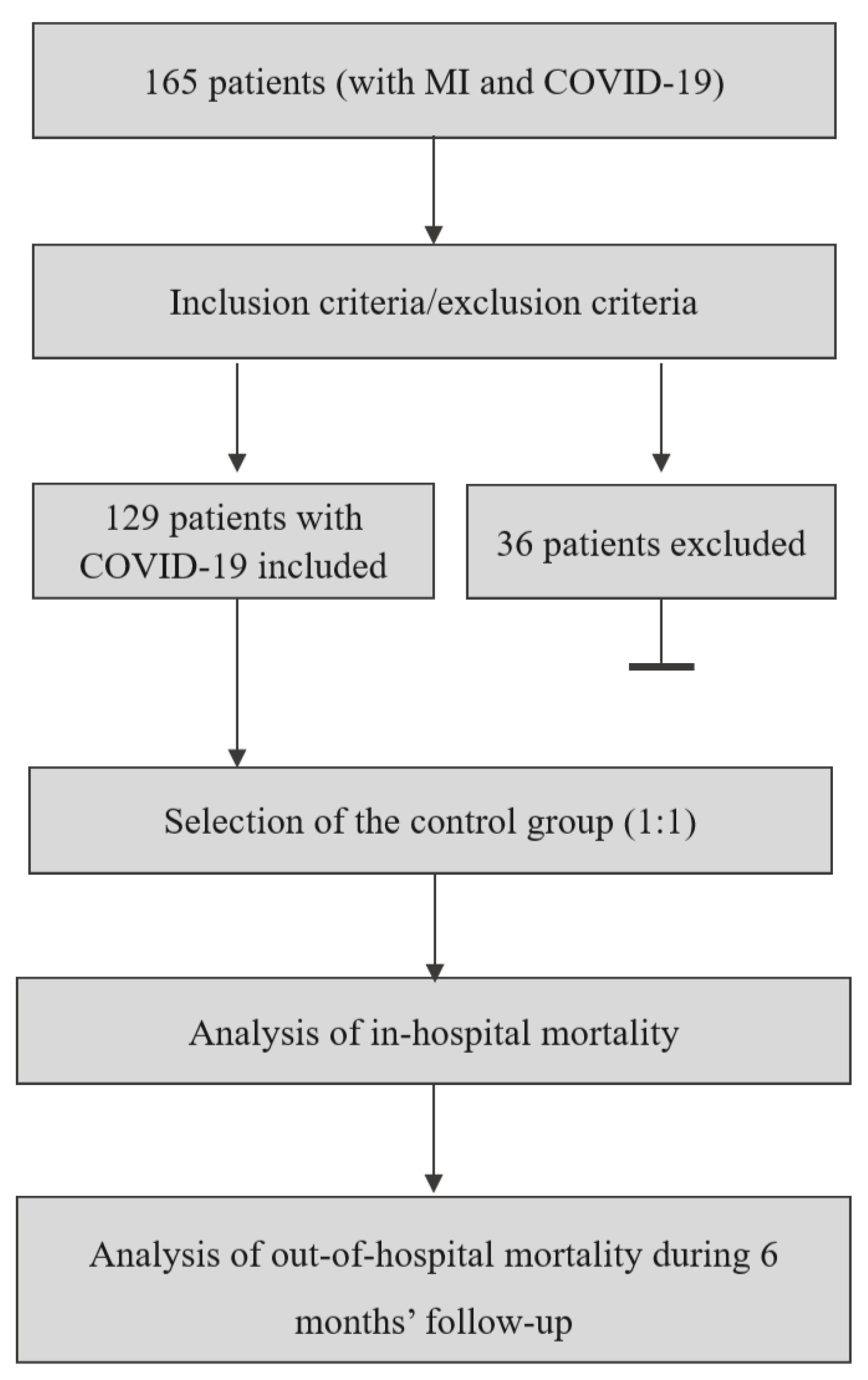
2.1. Study Group
- Confirmed MI, according to the ESC Fourth Universal Definition of Myocardial Infarction;
- Active SARS-CoV-2 infection confirmed during hospitalization by PCR testing;
- Age > 18 years.
- Any coexisting disease potentially limiting lifetime during observation (e.g., any end-stage organ failure or end-stage cancer);
- Minimum follow-up duration not met;
- Lack of primary clinical data necessary for matching, e.g., glomerular filtration rate (GFR) or ejection fraction (EF).
2.2. Study Objectives and Endpoints
2.3. Methods
2.4. Statistical Analysis
2.5. Sample Size Determination
2.6. Rationale for Study Design
3. Results
3.1. Study Group
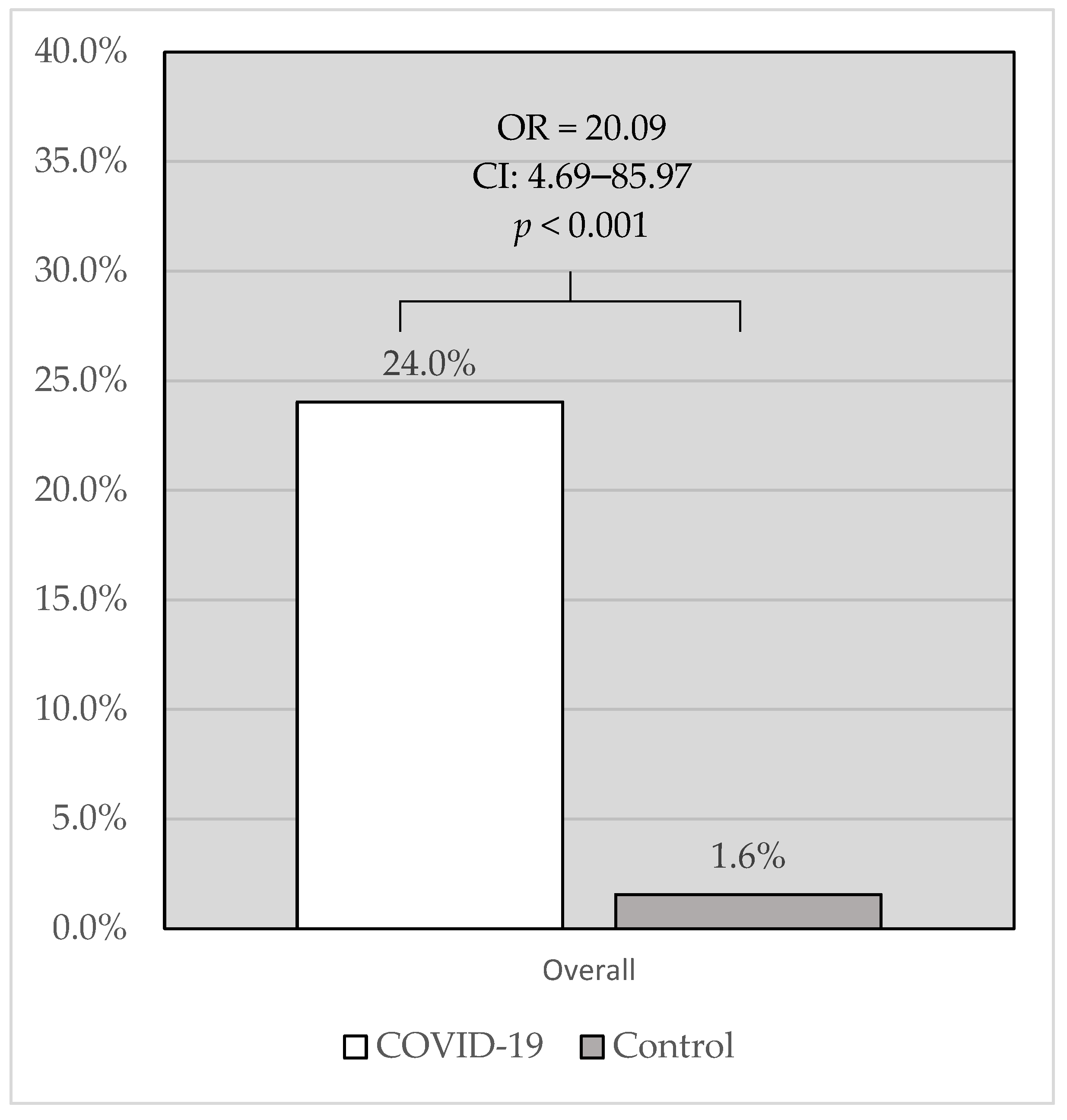
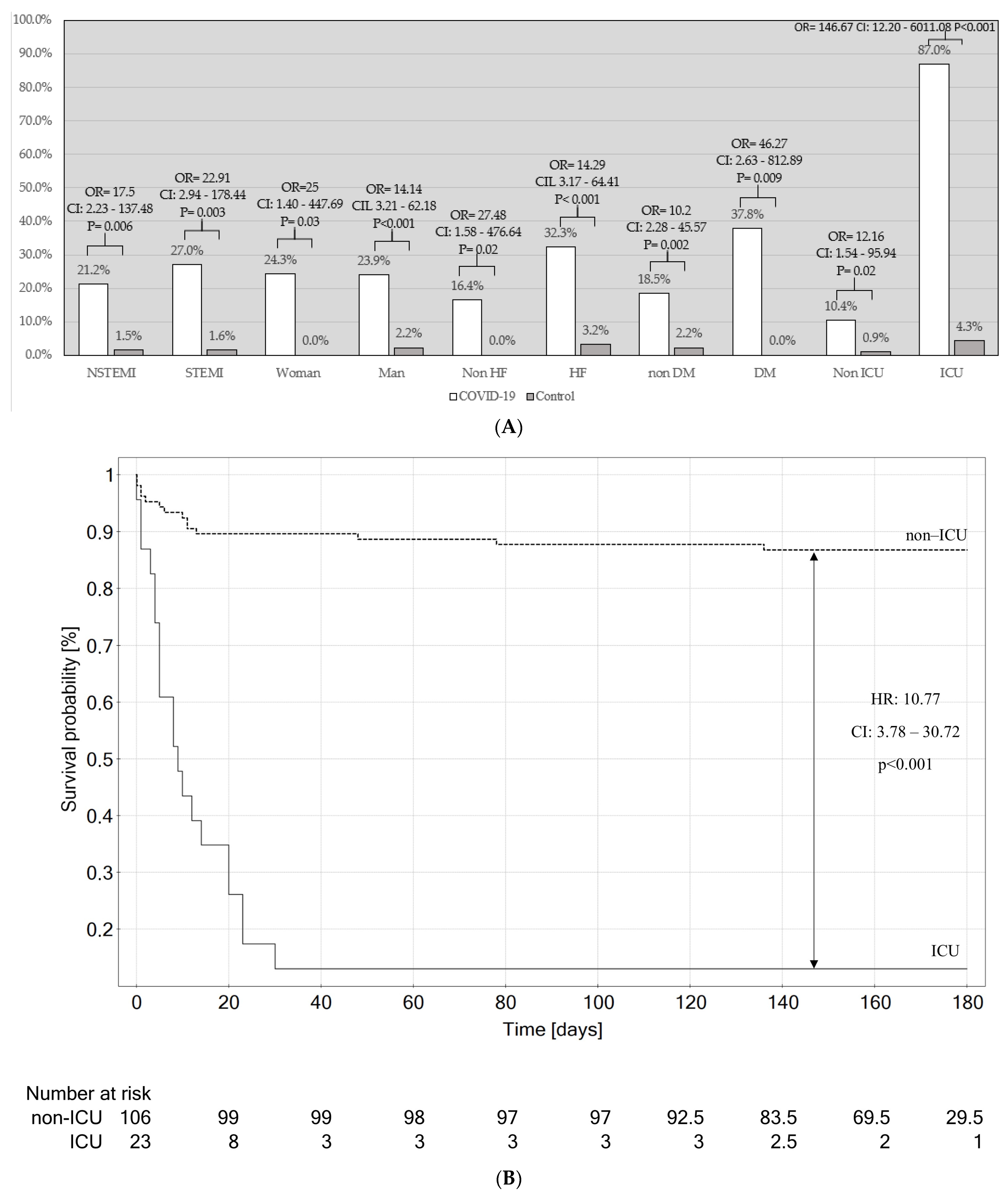
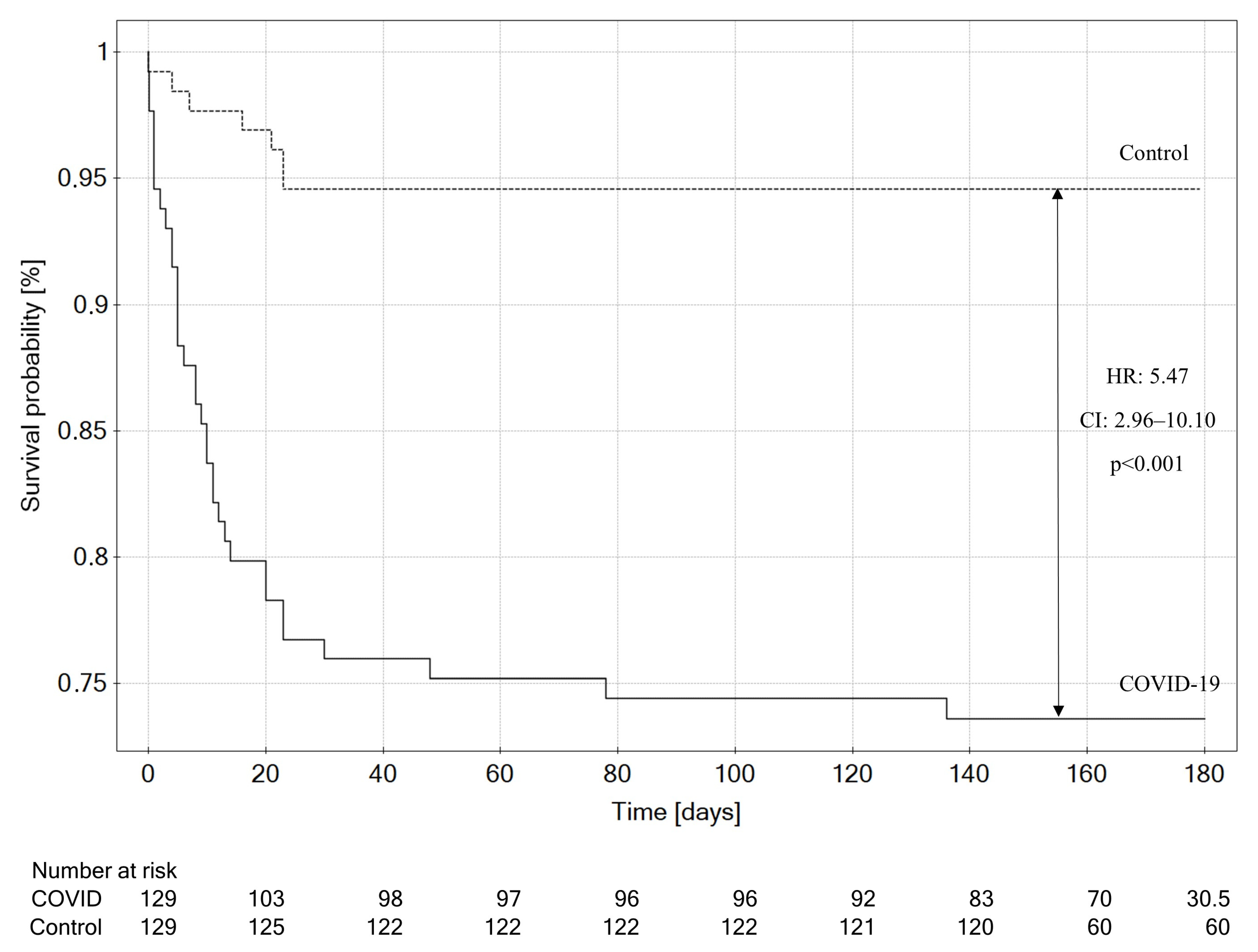
3.2. In-Hospital Mortality and Survival Analysis
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siddiqi, H.K.; Mehra, M.R. COVID-19 Illness in Native and Immunosuppressed States: A Clinical–Therapeutic Staging Proposal. J. Heart Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef]
- Schmitz, T.; Meisinger, C.; Kirchberger, I.; Thilo, C.; Amann, U.; Baumeister, S.E.; Linseisen, J. Impact of COVID-19 Pandemic Lockdown on Myocardial Infarction Care. Eur. J. Epidemiol. 2021, 36, 619–627. [Google Scholar] [CrossRef]
- Gylfason, A.D.; Bjarnason, A.; Helgason, K.O.; Rognvaldsson, K.G.; Armannsdottir, B.; Gudmundsdottir, I.J.; Gottfredsson, M. Effects of the COVID-19 pandemic and associated non-pharmaceutical interventions on diagnosis of myocardial infarction and selected infections in Iceland 2020. Laeknabladid 2022, 108, 182–188. [Google Scholar] [CrossRef]
- Impact of the COVID-19 Pandemic on Patient Delay and Clinical Outcomes for Patients with Acute Myocardial Infarction. Available online: https://pubmed.ncbi.nlm.nih.gov/35638194/ (accessed on 19 June 2023).
- Pourasghari, H.; Tavolinejad, H.; Soleimanpour, S.; Abdi, Z.; Arabloo, J.; Bragazzi, N.L.; Behzadifar, M.; Rashedi, S.; Omidi, N.; Ayoubian, A.; et al. Hospitalization, Major Complications and Mortality in Acute Myocardial Infarction Patients during the COVID-19 Era: A Systematic Review and Meta-Analysis. Int. J. Cardiol. Heart Vasc. 2022, 41, 101058. [Google Scholar] [CrossRef]
- Wang, S.Y.; Seghieri, C.; Vainieri, M.; Groene, O. Changes in Acute Myocardial Infarction, Stroke, and Heart Failure Hospitalizations during COVID-19 Pandemic in Tuscany—An Interrupted Time Series Study. Int. J. Public Health 2022, 67, 1604319. [Google Scholar] [CrossRef]
- Griewing, S.; Gremke, N.; Kreutz, J.; Schieffer, B.; Timmermann, L.; Markus, B. Chronological Development of Cardiovascular Disease in Times of COVID-19: A Retrospective Analysis of Hospitalized Diseases of the Circulatory System and COVID-19 Patients of a German University Hospital. J. Cardiovasc. Dev. Dis. 2022, 9, 325. [Google Scholar] [CrossRef]
- Zeymer, U.; Ahmadli, V.; Schneider, S.; Werdan, K.; Weber, M.; Hohenstein, S.; Hindricks, G.; Desch, S.; Bollmann, A.; Thiele, H. Effects of the COVID-19 Pandemic on Acute Coronary Syndromes in Germany during the First Wave: The COVID-19 Collateral Damage Study. Clin. Res. Cardiol. 2023, 112, 539–549. [Google Scholar] [CrossRef]
- Sturkenboom, H.N.; van Hattem, V.A.E.; Nieuwland, W.; Paris, F.M.A.; Magro, M.; Anthonio, R.L.; Algin, A.; Lipsic, E.; Bruwiere, E.; Van den Branden, B.J.L.; et al. COVID-19-Mediated Patient Delay Caused Increased Total Ischaemic Time in ST-Segment Elevation Myocardial Infarction. Neth. Heart J. 2022, 30, 96–105. [Google Scholar] [CrossRef]
- McNamara, D.A.; VanOosterhout, S.; Klungle, D.; Busman, D.; Parker, J.L.; Kampfschulte, A.; Jovinge, S.; Wohns, D.; Madder, R.D. Pandemic-Associated Delays in Myocardial Infarction Presentation in Predominantly Rural Counties with Low COVID-19 Prevalence. Am. J. Cardiol. 2022, 169, 18–23. [Google Scholar] [CrossRef]
- Granström, J.; Lantz, P.; Lidin, M.; Wahlström, M.; Nymark, C. Perceptions of Delay When Afflicted by an Acute Myocardial Infarction during the First Wave of the COVID-19 Pandemic. Eur. J. Cardiovasc. Nurs. 2023, 22, 89–97. [Google Scholar] [CrossRef]
- Janke, A.T.; Gettel, C.J.; Haimovich, A.; Kocher, K.E.; Krumholz, H.M.; Venkatesh, A.K. Changes in Emergency Department Arrival Times for Acute Myocardial Infarction during the COVID-19 Pandemic Suggest Delays in Care Seeking. Circ. Cardiovasc. Qual. Outcomes 2022, 15, e008402. [Google Scholar] [CrossRef]
- Mao, Q.; Zhao, J.; Li, Y.; Xie, L.; Xiao, H.; Wang, K.; Qiu, Y.; Chen, J.; Xu, Q.; Xu, Z.; et al. Impact of COVID-19 Pandemic on Mechanical Reperfusion in ST-Segment-Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention: A Multicenter Retrospective Study from a Non-Epicenter Region. Front. Cardiovasc. Med. 2021, 8, 698923. [Google Scholar] [CrossRef]
- Budrys, P.; Lizaitis, M.; Cerlinskaite-Bajore, K.; Bajoras, V.; Rodevic, G.; Martinonyte, A.; Dieckus, L.; Badaras, I.; Serpytis, P.; Gurevicius, R.; et al. Increase of Myocardial Ischemia Time and Short-Term Prognosis of Patients with Acute Myocardial Infarction during the First COVID-19 Pandemic Wave. Medicina 2021, 57, 1296. [Google Scholar] [CrossRef]
- Kobayashi, S.; Sakakura, K.; Jinnouchi, H.; Taniguchi, Y.; Tsukui, T.; Watanabe, Y.; Yamamoto, K.; Seguchi, M.; Wada, H.; Fujita, H. Comparison of Door-to-Balloon Time and in-Hospital Outcomes in Patients with ST-Elevation Myocardial Infarction between before versus after COVID-19 Pandemic. Cardiovasc. Interv. Ther. 2022, 37, 641–650. [Google Scholar] [CrossRef]
- Lechner, I.; Reindl, M.; Tiller, C.; Holzknecht, M.; Troger, F.; Fink, P.; Mayr, A.; Klug, G.; Bauer, A.; Metzler, B.; et al. Impact of COVID-19 Pandemic Restrictions on ST-Elevation Myocardial Infarction: A Cardiac Magnetic Resonance Imaging Study. Eur. Heart J. 2022, 43, 1141–1153. [Google Scholar] [CrossRef]
- Tokarek, T.; Dziewierz, A.; Zeliaś, A.; Malinowski, K.P.; Rakowski, T.; Dudek, D.; Siudak, Z. Impact of COVID-19 Pandemic on Patients with ST-Segment-Elevation Myocardial Infarction Complicated by Out-of-Hospital Cardiac Arrest. Int. J. Environ. Res. Public Health 2022, 20, 337. [Google Scholar] [CrossRef]
- Zając, P.; Kaziród-Wolski, K.; Sielski, J.; Wolska, M.; Malinowski, K.P.; Siudak, Z. COVID-19 as an Independent Predictor of Aspiration Thrombectomy in STEMI. National Data from the ORPKI Register in the Years 2020–2022. Postep. Kardiol Interwencyjnej 2023, 19, 119–126. [Google Scholar] [CrossRef]
- Katsoularis, I.; Fonseca-Rodríguez, O.; Farrington, P.; Lindmark, K.; Fors Connolly, A.-M. Risk of Acute Myocardial Infarction and Ischaemic Stroke Following COVID-19 in Sweden: A Self-Controlled Case Series and Matched Cohort Study. Lancet 2021, 398, 599–607. [Google Scholar] [CrossRef]
- Wienbergen, H.; Retzlaff, T.; Schmucker, J.; Marin, L.A.M.; Rühle, S.; Garstka, D.; Osteresch, R.; Fach, A.; Hambrecht, R. Impact of COVID-19 Pandemic on Presentation and Outcome of Consecutive Patients Admitted to Hospital Due to ST-Elevation Myocardial Infarction. Am. J. Cardiol. 2021, 151, 10–14. [Google Scholar] [CrossRef]
- Impact of COVID-19 Outbreak on Patients with ST-Segment Elevation Myocardial Infarction (STEMI) in Turkey: Results from TURSER Study (TURKISH St-Segment Elevation Myocardial Infarction Registry). Available online: https://pubmed.ncbi.nlm.nih.gov/34050883/ (accessed on 19 June 2023).
- Rattka, M.; Winsauer, C.; Stuhler, L.; Thiessen, K.; Baumhardt, M.; Stephan, T.; Rottbauer, W.; Imhof, A. Outcomes of Patients with ST-Segment Myocardial Infarction Admitted during the COVID-19 Pandemic. Herz 2022, 47, 258–264. [Google Scholar] [CrossRef]
- One-Year Outcomes of Patients with ST-Segment Elevation Myocardial Infarction during the COVID-19 Pandemic. Available online: https://pubmed.ncbi.nlm.nih.gov/34448103/ (accessed on 19 June 2023).
- De Luca, G.; Algowhary, M.; Uguz, B.; Oliveira, D.C.; Ganyukov, V.; Zimbakov, Z.; Cercek, M.; Jensen, L.O.; Loh, P.H.; Calmac, L.; et al. COVID-19 Pandemic, Mechanical Reperfusion and 30-Day Mortality in ST Elevation Myocardial Infarction. Heart 2022, 108, 458–466. [Google Scholar] [CrossRef]
- Fox, D.K.; Waken, R.J.; Johnson, D.Y.; Hammond, G.; Yu, J.; Fanous, E.; Maddox, T.M.; Joynt Maddox, K.E. Impact of the COVID-19 Pandemic on Patients without COVID-19 with Acute Myocardial Infarction and Heart Failure. J. Am. Heart Assoc. 2022, 11, e022625. [Google Scholar] [CrossRef]
- Asher, E.; Alexander Fardman, M.; Shmueli, H.; Orvin, K.; Oren, D.; Kofman, N.; Mohsen, J.; Moady, G.; Taha, L.; Rubinshtein, R.; et al. Outcomes among Patients Admitted for Non-ST Segment Myocardial Infarction in the Pre Pandemic and Pandemic COVID-19 Era–Israel Nationwide Study. Int. J. Qual. Health Care 2022, 34, mzac085. [Google Scholar] [CrossRef]
- Kontos, M.C.; Rennyson, S.L.; Chen, A.Y.; Alexander, K.P.; Peterson, E.D.; Roe, M.T. The Association of Myocardial Infarction Process of Care Measures and In-Hospital Mortality: A Report from the NCDR®. Am. Heart J. 2014, 168, 766–775. [Google Scholar] [CrossRef]
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—3 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---3-march-2020 (accessed on 19 June 2023).
- Marik, P.E.; Iglesias, J.; Varon, J.; Kory, P. COVID-19 in-Hospital Mortality: A Concise Worldwide Review. J. Comm. Med. Public Health Rep. 2021, 2, 1–8. [Google Scholar] [CrossRef]
- Alharbi, A.; Franz, A.; Alfatlawi, H.; Wazzan, M.; Alsughayer, A.; Eltahawy, E.; Assaly, R. Impact of COVID-19 Pandemic on the Outcomes of Acute Coronary Syndrome. Curr. Probl. Cardiol. 2023, 48, 101575. [Google Scholar] [CrossRef]
- Markson, F.E.; Akuna, E.; Lim, C.Y.; Khemani, L.; Amanullah, A. The Impact of COVID-19 on Hospitalization Outcomes of Patients with Acute Myocardial Infarction in the USA. Am. Heart J. Plus 2023, 32, 100305. [Google Scholar] [CrossRef]
- Saad, M.; Kennedy, K.F.; Imran, H.; Louis, D.W.; Shippey, E.; Poppas, A.; Wood, K.E.; Abbott, J.D.; Aronow, H.D. Association between COVID-19 Diagnosis and In-Hospital Mortality in Patients Hospitalized with ST-Segment Elevation Myocardial Infarction. JAMA 2021, 326, 1940–1952. [Google Scholar] [CrossRef]
- Little, C.D.; Kotecha, T.; Candilio, L.; Jabbour, R.J.; Collins, G.B.; Ahmed, A.; Connolly, M.; Kanyal, R.; Demir, O.M.; Lawson, L.O.; et al. COVID-19 Pandemic and STEMI: Pathway Activation and Outcomes from the Pan-London Heart Attack Group. Open Heart 2020, 7, e001432. [Google Scholar] [CrossRef]
- Choudry, F.A.; Hamshere, S.M.; Rathod, K.S.; Akhtar, M.M.; Archbold, R.A.; Guttmann, O.P.; Woldman, S.; Jain, A.K.; Knight, C.J.; Baumbach, A.; et al. High Thrombus Burden in Patients with COVID-19 Presenting with ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2020, 76, 1168–1176. [Google Scholar] [CrossRef]
- Garcia, S.; Dehghani, P.; Grines, C.; Davidson, L.; Nayak, K.R.; Saw, J.; Waksman, R.; Blair, J.; Akshay, B.; Garberich, R.; et al. Initial Findings from the North American COVID-19 Myocardial Infarction Registry. J. Am. Coll. Cardiol. 2021, 77, 1994–2003. [Google Scholar] [CrossRef]
- Kite, T.A.; Ludman, P.F.; Gale, C.P.; Wu, J.; Caixeta, A.; Mansourati, J.; Sabate, M.; Jimenez-Quevedo, P.; Candilio, L.; Sadeghipour, P.; et al. International Prospective Registry of Acute Coronary Syndromes in Patients with COVID-19. J. Am. Coll. Cardiol. 2021, 77, 2466–2476. [Google Scholar] [CrossRef]
- Choudry, F.A.; Rathod, K.S.; Baumbach, A.; Mathur, A.; Jones, D.A. Long-Term Outcomes of COVID-19-Associated ST-Elevation Myocardial Infarction Treated with Primary PCI. Cardiovasc. Revasc. Med. 2022, 43, 133–135. [Google Scholar] [CrossRef]
- Dehghani, P.; Schmidt, C.W.; Garcia, S.; Okeson, B.; Grines, C.L.; Singh, A.; Patel, R.A.G.; Wiley, J.; Htun, W.W.; Nayak, K.R.; et al. North American COVID-19 Myocardial Infarction (NACMI) Risk Score for Prediction of In-Hospital Mortality. J. Soc. Cardiovasc. Angiogr. Interv. 2022, 1, 100404. [Google Scholar] [CrossRef]
- De Luca, G.; Debel, N.; Cercek, M.; Jensen, L.O.; Vavlukis, M.; Calmac, L.; Johnson, T.; Ferrer, G.R.; Ganyukov, V.; Wojakowski, W.; et al. Impact of SARS-CoV-2 Positivity on Clinical Outcome among STEMI Patients Undergoing Mechanical Reperfusion: Insights from the ISACS STEMI COVID 19 Registry. Atherosclerosis 2021, 332, 48–54. [Google Scholar] [CrossRef]
- Goel, A.; Malik, A.H.; Bandyopadhyay, D.; Isath, A.; Gupta, R.; Hajra, A.; Shrivastav, R.; Virani, S.S.; Fonarow, G.C.; Lavie, C.J.; et al. Impact of COVID-19 on Outcomes of Patients Hospitalized with STEMI: A Nationwide Propensity-Matched Analysis. Curr. Probl. Cardiol. 2023, 48, 101547. [Google Scholar] [CrossRef]
- Clinical Characteristics and Outcomes of Adults with a History of Heart Failure Hospitalized for COVID-19|Circulation: Heart Failure. Available online: https://www.ahajournals.org/doi/full/10.1161/CIRCHEARTFAILURE.121.008354 (accessed on 22 June 2023).
- Yonas, E.; Alwi, I.; Pranata, R.; Huang, I.; Lim, M.A.; Gutierrez, E.J.; Yamin, M.; Siswanto, B.B.; Virani, S.S. Effect of Heart Failure on the Outcome of COVID-19—A Meta Analysis and Systematic Review. Am. J. Emerg. Med. 2021, 46, 204–211. [Google Scholar] [CrossRef]
- Heart Failure in COVID-19 Patients: Prevalence, Incidence and Prognostic Implications—Rey-2020-European Journal of Heart Failure-Wiley Online Library. Available online: https://onlinelibrary.wiley.com/doi/full/10.1002/ejhf.1990 (accessed on 22 June 2023).
- Kubica, J.; Ostrowska, M.; Stolarek, W.; Kasprzak, M.; Grzelakowska, K.; Krys, J.; Kubica, A.; Adamski, P.; Podhajski, P.; Navarese, E.P.; et al. Impact of COVID-19 Pandemic on Acute Heart Failure Admissions and Mortality: A Multicentre Study (COV-HF-SIRIO 6 Study). ESC Heart Fail 2022, 9, 721–728. [Google Scholar] [CrossRef]
- Arutyunov, G.P.; Tarlovskaya, E.I.; Arutyunov, A.G.; Lopatin, Y.M. ACTIV Investigators Impact of Heart Failure on All-Cause Mortality in COVID-19: Findings from the Eurasian International Registry. ESC Heart Fail 2023, 10, 1013–1024. [Google Scholar] [CrossRef]
- Gu, H.; Cirillo, C.; Nabeebaccus, A.A.; Sun, Z.; Fang, L.; Xie, Y.; Demir, O.; Desai, N.; He, L.; Lü, Q.; et al. First-Phase Ejection Fraction, a Measure of Preclinical Heart Failure, Is Strongly Associated with Increased Mortality in Patients with COVID-19. Hypertension 2021, 77, 2014–2022. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Gupta, M.; KAtoch, N.; Garg, K.; Garg, B. A Systematic Review and Meta-Analysis of Diabetes Associated Mortality in Patients with COVID-19. Int. J. Endocrinol. Metab. 2021, 19, e113220. [Google Scholar] [CrossRef] [PubMed]
- Van Aerde, N.; Van den Berghe, G.; Wilmer, A.; Gosselink, R.; Hermans, G. COVID-19 Consortium Intensive Care Unit Acquired Muscle Weakness in COVID-19 Patients. Intensive Care Med. 2020, 46, 2083–2085. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Kaziród-Wolski, K.; Sielski, J.; Sidło, J.; Januszek, R.; Siudak, Z. The Most Relevant Factors Affecting the Perioperative Death Rate in Patients with Acute Coronary Syndrome and COVID-19, Based on Annual Follow-Up in the ORPKI Registry. Biomedicines 2021, 9, 1813. [Google Scholar] [CrossRef]
- Comparison between COVID-19 Outcomes in the First 3 Waves of the Pandemic: A Reference Hospital Report. Available online: https://www.mp.pl/paim/issue/article/16286 (accessed on 27 August 2023).
- Oladunjoye, O.; Gallagher, M.; Wasser, T.; Oladunjoye, A.; Paladugu, S.; Donato, A. Mortality due to COVID-19 Infection: A Comparison of First and Second Waves. J. Community Hosp. Intern. Med. Perspect. 2021, 11, 747–752. [Google Scholar] [CrossRef]
- Gray, W.K.; Navaratnam, A.V.; Day, J.; Wendon, J.; Briggs, T.W.R. COVID-19 Hospital Activity and in-Hospital Mortality during the First and Second Waves of the Pandemic in England: An Observational Study. Thorax 2022, 77, 1113–1120. [Google Scholar] [CrossRef]
- Meschiari, M.; Cozzi-Lepri, A.; Tonelli, R.; Bacca, E.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Bedini, A.; Volpi, S.; Milic, J.; et al. First and Second Waves among Hospitalised Patients with COVID-19 with Severe Pneumonia: A Comparison of 28-Day Mortality over the 1-Year Pandemic in a Tertiary University Hospital in Italy. BMJ Open 2022, 12, e054069. [Google Scholar] [CrossRef]
- Harbuwono, D.S.; Handayani, D.O.T.L.; Wahyuningsih, E.S.; Supraptowati, N.; Ananda; Kurniawan, F.; Wafa, S.; Kristanti, M.; Pantoro, N.I.; Sinto, R.; et al. Impact of Diabetes Mellitus on COVID-19 Clinical Symptoms and Mortality: Jakarta’s COVID-19 Epidemiological Registry. Prim. Care Diabetes 2022, 16, 65–68. [Google Scholar] [CrossRef]
- Shang, L.; Shao, M.; Guo, Q.; Shi, J.; Zhao, Y.; Xiaokereti, J.; Tang, B. Diabetes Mellitus Is Associated with Severe Infection and Mortality in Patients with COVID-19: A Systematic Review and Meta-Analysis. Arch. Med. Res. 2020, 51, 700–709. [Google Scholar] [CrossRef]
- Schmitt, V.H.; Hobohm, L.; Munzel, T.; Wenzel, P.; Gori, T.; Keller, K. Clinical Impact of Diabetes Mellitus in Patients Hospitalized for Myocardial Infarction. Eur. Heart J. 2020, 41, ehaa946.1506. [Google Scholar] [CrossRef]
- Ahmed, B.; Davis, H.T.; Laskey, W.K. In-Hospital Mortality Among Patients with Type 2 Diabetes Mellitus and Acute Myocardial Infarction: Results from the National Inpatient Sample, 2000–2010. J. Am. Heart Assoc. 2014, 3, e001090. [Google Scholar] [CrossRef] [PubMed]
- Salinas-Botrán, A.; Sanz-Cánovas, J.; Pérez-Somarriba, J.; Pérez-Belmonte, L.M.; Cobos-Palacios, L.; Rubio-Rivas, M.; de-Cossío-Tejido, S.; Ramos-Rincón, J.M.; Méndez-Bailón, M.; Gómez-Huelgas, R.; et al. Clinical characteristics and risk factors for mortality upon admission in patients with heart failure hospitalized due to COVID-19 in Spain. Rev. Clin. Esp. 2022, 222, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, A.S.; Jering, K.S.; Vaduganathan, M.; Claggett, B.L.; Cunningham, J.W.; Rosenthal, N.; Signorovitch, J.; Thune, J.J.; Vardeny, O.; Solomon, S.D. Clinical Outcomes in Patients with Heart Failure Hospitalized with COVID-19. JACC Heart Fail. 2021, 9, 65–73. [Google Scholar] [CrossRef]
- Sokolski, M.; Reszka, K.; Suchocki, T.; Adamik, B.; Doroszko, A.; Drobnik, J.; Gorka-Dynysiewicz, J.; Jedrzejczyk, M.; Kaliszewski, K.; Kilis-Pstrusinska, K.; et al. History of Heart Failure in Patients Hospitalized Due to COVID-19: Relevant Factor of In-Hospital Complications and All-Cause Mortality up to Six Months. J. Clin. Med. 2022, 11, 241. [Google Scholar] [CrossRef]
- Alvarez-Garcia, J.; Lee, S.; Gupta, A.; Cagliostro, M.; Joshi, A.A.; Rivas-Lasarte, M.; Contreras, J.; Mitter, S.S.; LaRocca, G.; Tlachi, P.; et al. Prognostic Impact of Prior Heart Failure in Patients Hospitalized with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2334–2348. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COVID-19 (n = 129) | Control (n = 129) | p | |
|---|---|---|---|
| Clinical Characteristics | |||
| Men, n (%) | 92 (71.32%) | 92 (71.32%) | |
| Women, n (%) | 37 (28.68%) | 37 (28.68%) | |
| NSTEMI, n (%) | 66 (51.16%) | 66 (51.16%) | |
| STEMI, n (%) | 63 (48.84%) | 63 (48.84%) | |
| Age, years | 67 (61–75) | 67 (60–75) | 0.52 |
| EF, % | 45 (35–50) | 45 (35–50) | 0.93 |
| GFR, mL/min | 75.8 (53.5–94.5) | 80.14 (55.2–95.7) | 0.56 |
| Diabetes, n (%) | 37 (28.68%) | 37 (28.68%) | |
| Hypertension, n (%) | 86 (66.67%) | 100 (77.52%) | 0.05 |
| Hyperlipidemia, n (%) | 56 (43.41%) | 76 (58.91%) | 0.01 |
| Smoking, n (%) | 17 (13.18%) | 33 (25.58%) | 0.01 |
| Peripheral arterial disease, n (%) | 2 (1.55%) | 13 (10.08%) | 0.004 |
| Obesity, n (%) | 16 (12.4%) | 16 (12.4%) | |
| Previous stroke, n (%) | 8 (6.2%) | 13 (10.08%) | 0.19 |
| Atrial fibrillation, n (%) | 23 (17.83%) | 19 (14.73%) | 0.50 |
| Myocardial infarction, n (%) | 25 (19.38%) | 29 (22.48%) | 0.54 |
| Previous PTCA, n (%) | 20 (15.5%) | 26 (20.16%) | 0.33 |
| Previous CABG, n (%) | 8 (6.2%) | 5 (3.88%) | 0.39 |
| Procedural characteristics | |||
| Coronarography, n (%) | 125 (96.9%) | 128 (99.22%) | 0.18 |
| OMT, n (%) | 4 (3.1%) | 1 (0.78%) | 0.18 |
| CABG qualified, n (%) | 8 (6.2%) | 5 (3.88%) | 0.39 |
| PTCA, n (%) | 107 (82.95%) | 112 (86.82%) | 0.85 |
| Reached TIMI 3, n (%) | 91 (85.05%) | 105 (93.75%) | 0.02 |
| POBA, n (%) | (0%) | (0%) | |
| MVD, n (%) | 35 (27.13%) | 20 (15.5%) | 0.02 |
| LM, n (%) | 5 (3.88%) | 6 (4.65%) | 0.76 |
| LAD, n (%) | 41 (31.78%) | 49 (37.98%) | 0.30 |
| D1, n (%) | 4 (3.1%) | 4 (3.1%) | |
| CX, n (%) | 11 (8.53%) | 16 (12.4%) | 0.31 |
| OM, n (%) | 4 (3.1%) | 9 (6.98%) | 0.15 |
| RCA, n (%) | 25 (19.38%) | 29 (22.48%) | 0.54 |
| PDA, n (%) | 0 (0%) | 2 (1.55%) | 0.16 |
| IM, n (%) | 1 (0.78%) | 2 (1.55%) | 0.56 |
| Bridge, n (%) | 2 (1.55%) | 3 (2.33%) | 0.65 |
| Stent length, mm | 32 (20–51.5) | 25.5 (18–40) | 0.11 |
| Multisteps, n (%) | 4 (3.1%) | 12 (9.3%) | 0.04 |
| Hospitalization characteristics | |||
| Cardiogenic shock, n (%) | 18 (13.95%) | 8 (6.2%) | 0.04 |
| Pulmonary edema, n (%) | 9 (6.98%) | 23 (17.83%) | 0.008 |
| Respiratory failure, n (%) | 23 (17.83%) | 0 (0%) | <0.001 |
| Contrast-induced nephropathy, n (%) | 12 (9.3%) | 5 (3.88%) | 0.08 |
| Stroke, n (%) | 1 (0.78%) | 0 (0%) | 0.32 |
| Bleeding requiring transfusion, n (%) | 5 (3.88%) | 0 (0%) | 0.02 |
| Hospitalization time (days) | 10 (4–14) | 4 (3–5) | <0.001 |
| Time to death (days) | 8 (3.25–13.75) | 16 (6–22) | 0.28 |
| Transfer to another ward frequency, n (%) | 72 (55.81%) | 10 (7.75%) | <0.001 |
| Univariable Cox Regression | Multivariable Cox Regression | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | HR | −95% CI | +95% CI | p | HR | −95% CI | +95% CI | p |
| COVID-19 | 7.45 | 1.74 | 32.01 | 0.007 | 9.10 | 2.12 | 39.00 | 0.003 |
| Acute respiratory failure with mechanical ventilation | 6.73 | 3.29 | 13.78 | <0.001 | 6.80 | 3.32 | 13.94 | <0.001 |
| Sex | 1.20 | 0.56 | 2.61 | 0.64 | ||||
| Diabetes | 1.70 | 0.85 | 3.39 | 0.13 | ||||
| GFR, mL/min | 0.99 | 0.98 | 1.00 | 0.076 | ||||
| EF, % | 0.97 | 0.94 | 0.99 | 0.04 | 0.96 | 0.93 | 0.99 | 0.013 |
| Age, years | 1.01 | 0.98 | 1.04 | 0.40 | ||||
| MI type (STEMI vs. NSTEMI) | 1.29 | 0.64 | 2.58 | 0.47 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hrycek, E.; Walawska-Hrycek, A.; Hamankiewicz, M.; Milewski, K.; Nowakowski, P.; Buszman, P.; Żurakowski, A. The Influence of SARS-CoV-2 Infection on Acute Myocardial Infarction Outcomes. J. Clin. Med. 2023, 12, 5899. https://doi.org/10.3390/jcm12185899
Hrycek E, Walawska-Hrycek A, Hamankiewicz M, Milewski K, Nowakowski P, Buszman P, Żurakowski A. The Influence of SARS-CoV-2 Infection on Acute Myocardial Infarction Outcomes. Journal of Clinical Medicine. 2023; 12(18):5899. https://doi.org/10.3390/jcm12185899
Chicago/Turabian StyleHrycek, Eugeniusz, Anna Walawska-Hrycek, Maciej Hamankiewicz, Krzysztof Milewski, Przemysław Nowakowski, Piotr Buszman, and Aleksander Żurakowski. 2023. "The Influence of SARS-CoV-2 Infection on Acute Myocardial Infarction Outcomes" Journal of Clinical Medicine 12, no. 18: 5899. https://doi.org/10.3390/jcm12185899
APA StyleHrycek, E., Walawska-Hrycek, A., Hamankiewicz, M., Milewski, K., Nowakowski, P., Buszman, P., & Żurakowski, A. (2023). The Influence of SARS-CoV-2 Infection on Acute Myocardial Infarction Outcomes. Journal of Clinical Medicine, 12(18), 5899. https://doi.org/10.3390/jcm12185899