
Misinterpreting Diarrhea-Predominant Irritable Bowel Syndrome and Functional Diarrhea: Pathophysiological Highlights

 , , , ,
, , , ,  ,
,  , and
, and 
Abstract
:
1. Introduction
- Lymphocytic Colitis (LC), in the presence of an increased number of intraepithelial lymphocytes (≥20 per 100 surface epithelial cells) combined with an increased inflammatory infiltrate in the lamina propria and a not significantly thickened collagenous band (<10 mm).
- Collagenous Colitis (CC), in the presence of a thickened subepithelial collagenous band (≥10 mm) combined with an increased inflammatory infiltrate in the lamina propria.
2. Methods
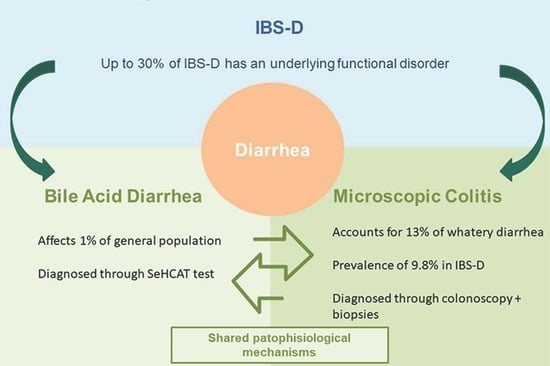
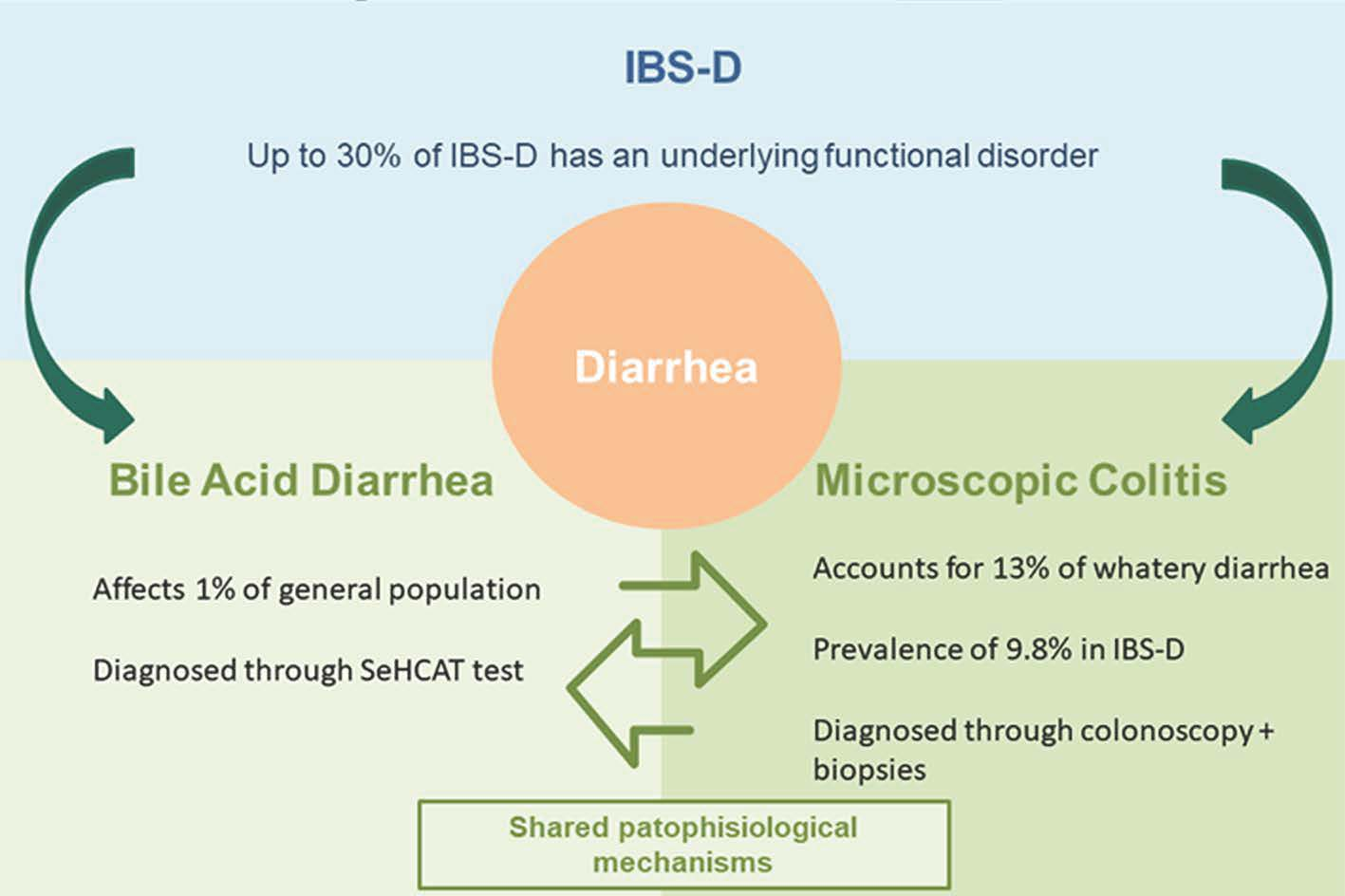
3. Bile Acid Diarrhea and Microscopic Colitis in the Current Literature
3.1. Clinical Studies on BAM and MC
3.2. Bile Acid Malabsorbtion and Bile Acid Diarrhea
- Type I: secondary to ileal dysfunction, i.e., failure to reabsorb bile acids in the ileum because of resection, bypass or Crohn’s disease.
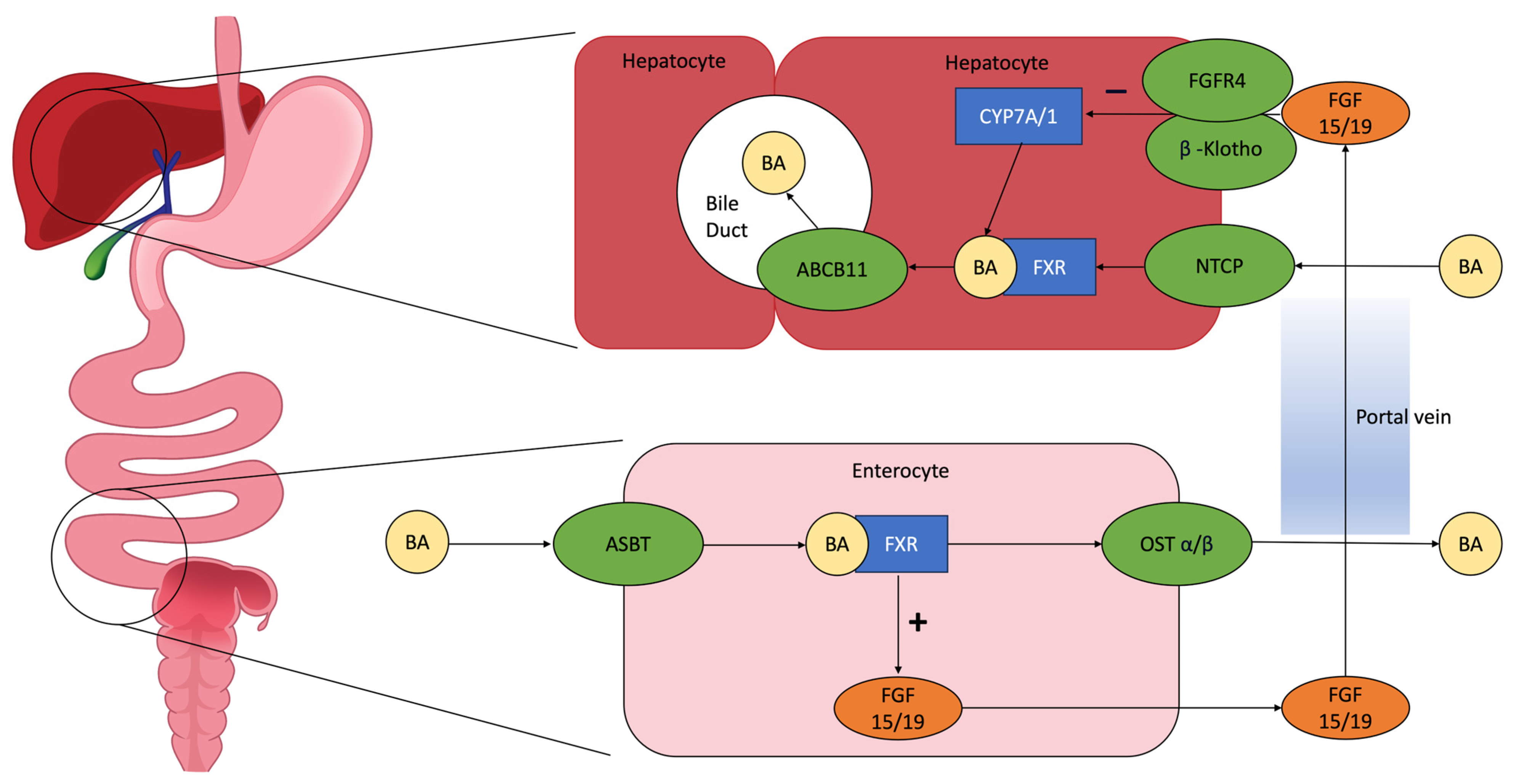
- Type II: primary idiopathic condition, in which there are decreased plasma levels of ileal fibroblast growth factor 19 (FGF19). FGF19 is produced by ileal enterocytes as a response to excess bile acids in the terminal ileum, causing a negative feedback loop on hepatic bile acids synthesis through the farnesoid X receptor (FXR) and reducing bile acids synthesis.
- Type III: gastroenterological conditions interfering with the normal bile acids reabsorption (e.g., cholecystectomy, chronic pancreatitis, small intestinal bacterial overgrowth, colitis, celiac disease, radiation-induced enteritis, diabetes mellitus).
- Type IV: excessive hepatic bile acids synthesis: observed in patients with hypertriglyceridemia or using metformin [33].
3.3. Microscopic Colitis
3.4. Association between BAM and MC
4. Pathophysiological Mechanisms
4.1. Role of Farnesoid X Receptor (FXR)
- In enterocytes, it induces the synthesis of fibroblast growth factor 19 (FGF19), which inhibits CYP7A1, the hepatic enzyme that synthetizes bile acids, producing C4;
- A decreased bile acid intestinal absorption and an increase in the expression of organic solute transporters α and β in enterocytes, in order to prevent intracellular bile acid accumulation and its excretion to the portal system [24].
4.2. Role of Gut Microbiota
4.3. Role of Apical Sodium Dependent Bile Acid Transporter (ASBT)
4.4. Role of Takeda G-Protein-Coupled Receptor 5 (TGR5)
- Modulating intestinal inflammation. In a mice mode, the activation of TGR5 leads to an anti-inflammatory effect through a reduction in IL6, TNFα, INFγ and an increase in IL10.
- Maintaining intestinal barrier integrity. In a mice model, a deficit in TGR5 leads to an abnormal morphology of the colonic mucosa and increased intestinal permeability, with an altered molecular architecture of epithelial thigh junctions, increased expression and abnormal distribution of zonulin 1.
- Intestinal motility. It is expressed on enteric neurons and mediates the effects of bile acid on colonic motility. Confirming this hypothesis, a study by Alemi et al. showed that TGR5 overexpression in transgenic mice caused a more rapid colonic transit time and increased frequency of defecation [53].
5. Conclusions
- Exploring the exact prevalence of the association of BAM and MC in chronic watery diarrhea or in patients labelled as “functional” but refractory to conventional therapy;
- Clarifying the role of the most debated molecular actors (e.g., TGR5) involved in BAM pathophysiology and its relationships with MC.
- Understanding the relationship between BAM and MC in symptom generation, when both coexist in the same patients;
- Discovering the correct treatment strategy in these patients through randomized controlled clinical trials.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Savarino, E.; Zingone, F.; Barberio, B.; Marasco, G.; Akyuz, F.; Akpinar, H.; Barboi, O.; Bodini, G.; Bor, S.; Chiarioni, G.; et al. Functional Bowel Disorders with Diarrhoea: Clinical Guidelines of the United European Gastroenterology and European Society for Neurogastroenterology and Motility. United Eur. Gastroenterol. J. 2022, 10, 556–584. [Google Scholar] [CrossRef] [PubMed]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e3. [Google Scholar] [CrossRef] [PubMed]
- Lacy, B.E.; Mearin, F.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407.e5. [Google Scholar] [CrossRef] [PubMed]
- Oka, P.; Parr, H.; Barberio, B.; Black, C.J.; Savarino, E.V.; Ford, A.C. Global Prevalence of Irritable Bowel Syndrome according to Rome III or IV Criteria: A Systematic Review and Meta-Analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 908–917. [Google Scholar] [CrossRef]
- Bassotti, G. Irritable Bowel Syndrome: A Multifaceted World Still to Discover. J. Clin. Med. 2022, 11, 4103. [Google Scholar] [CrossRef]
- Zamani, M.; Alizadeh-Tabari, S.; Zamani, V. Systematic Review with Meta-Analysis: The Prevalence of Anxiety and Depression in Patients with Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2019, 50, 132–143. [Google Scholar] [CrossRef]
- Altomare, A.; Di Rosa, C.; Imperia, E.; Emerenziani, S.; Cicala, M.; Guarino, M.P.L. Diarrhea Predominant-Irritable Bowel Syndrome (IBS-D): Effects of Different Nutritional Patterns on Intestinal Dysbiosis and Symptoms. Nutrients 2021, 13, 1506. [Google Scholar] [CrossRef]
- Valentin, N.; Camilleri, M.; Altayar, O.; Vijayvargiya, P.; Acosta, A.; Nelson, A.D.; Murad, M.H. Biomarkers for Bile Acid Diarrhoea in Functional Bowel Disorder with Diarrhoea: A Systematic Review and Meta-Analysis. Gut 2015, 65, 1951–1959. [Google Scholar] [CrossRef]
- Camilleri, M. Bile Acid Diarrhea: Prevalence, Pathogenesis, and Therapy. Gut Liver 2015, 9, 332–339. [Google Scholar] [CrossRef]
- Miehlke, S.; Guagnozzi, D.; Zabana, Y.; Tontini, G.E.; Kanstrup Fiehn, A.-M.; Wildt, S.; Bohr, J.; Bonderup, O.; Bouma, G.; D’Amato, M.; et al. European Guidelines on Microscopic Colitis: United European Gastroenterology and European Microscopic Colitis Group Statements and Recommendations. United Eur. Gastroenterol. J. 2021, 9, 13–37. [Google Scholar] [CrossRef]
- Guagnozzi, D.; Arias, Á.; Lucendo, A.J. Systematic Review with Meta-Analysis: Diagnostic Overlap of Microscopic Colitis and Functional Bowel Disorders. Aliment. Pharm. 2016, 43, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, M.A.; Munck, L.K. Systematic Review: Are Lymphocytic Colitis and Collagenous Colitis Two Subtypes of the Same Disease—Microscopic Colitis? Aliment Pharm. 2012, 36, 79–90. [Google Scholar] [CrossRef]
- Brydon, W.G.; Nyhlin, H.; Eastwood, M.A.; Merrick, M.V. Serum 7α-Hydroxy-4-Cholesten-3-One and Selenohomocholyltaurine (SeHCAT) Whole Body Retention in the Assessment of Bile Acid Induced Diarrhoea. Eur. J. Gastroenterol. Hepatol. 1996, 8, 117. [Google Scholar] [CrossRef] [PubMed]
- Sauter, G.H.; Munzing, W.; Ritter, C.V.; Paumgartner, G. Bile Acid Malabsorption as a Cause of Chronic Diarrhea Diagnostic Value of 7α-Hydroxy-4-Cholesten-3-One in Serum. Dig. Dis. Sci. 1999, 44, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Vijayvargiya, P.; Camilleri, M.; Shin, A.; Saenger, A. Methods for Diagnosis of Bile Acid Malabsorption in Clinical Practice. Clin. Gastroenterol. Hepatol. 2013, 11, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Fani, B.; Bertani, L.; Paglianiti, I.; Fantechi, L.; de Bortoli, N.; Costa, F.; Volterrani, D.; Marchi, S.; Bellini, M. Pros and Cons of the SeHCAT Test in Bile Acid Diarrhea: A More Appropriate Use of an Old Nuclear Medicine Technique. Gastroenterol. Res. Pract. 2018, 2018, 2097359. [Google Scholar] [CrossRef]
- Fernández-Bañares, F.; Esteve, M.; Salas, A.; Forné, M.; Espinós, J.C.; Martín-Comín, J.; Viver, J.M. Bile Acid Malabsorption in Microscopic Colitis and in Previously Unexplained Functional Chronic Diarrhea. Dig. Dis. Sci. 2001, 46, 2231–2238. [Google Scholar] [CrossRef]
- Rampton, D.S.; Baithun, S.I. Is Microscopic Colitis Due to Bile-Salt Malabsorption? Dis. Colon. Rectum. 1987, 30, 950. [Google Scholar] [CrossRef]
- Bohr, J.; Tysk, C.; Eriksson, S.; Abrahamsson, H.; Järnerot, G. Collagenous Colitis: A Retrospective Study of Clinical Presentation and Treatment in 163 Patients. Gut 1996, 39, 846–851. [Google Scholar] [CrossRef]
- Ung, K.-A.; Gillberg, R.; Kilander, A.; Abrahamsson, H. Role of Bile Acids and Bile Acid Binding Agents in Patients with Collagenous Colitis. Gut 2000, 46, 170–175. [Google Scholar] [CrossRef]
- Gurbuz, Y.; Senturk, O.; Muezzinoğlu, B. Postcholecystectomy Microscopic Colitis: Is Bile Acid Malabsorption a Triggering Factor? Off. J. Am. Coll. Gastroenterol. ACG 2001, 96, 1655. [Google Scholar] [CrossRef]
- Ung, K.-A.; Kilander, A.; Willén, R.; Abrahamsson, H. Role of Bile Acids in Lymphocytic Colitis. Hepatogastroenterology 2002, 49, 432–437. [Google Scholar] [PubMed]
- Fernández-Bañares, F.; Salas, A.; Esteve, M.; Espinos, J.; Montserrat, F.; Viver, J.M. Collagenous and Lymphocytic Colitis: Evaluation of Clinical and Histological Features, Response to Treatment, and Long-Term Follow-Up. Am. J. Gastroenterol. 2003, 98, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Wildt, S.; Rasmussen, S.N.; Madsen, J.L.; Rumessen, J.J. Bile Acid Malabsorption in Patients with Chronic Diarrhoea: Clinical Value of SeHCAT Test. Scand. J. Gastroenterol. 2003, 38, 826–830. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Willén, R.; Stotzer, P.-O. Colonoscopy and SeHCAT for Investigation of Chronic Diarrhea. Digestion 2004, 69, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Bajor, A.; Kilander, A.; Gälman, C.; Rudling, M.; Ung, K.-A. Budesonide Treatment Is Associated with Increased Bile Acid Absorption in Collagenous Colitis. Aliment. Pharmacol. Ther. 2006, 24, 1643–1649. [Google Scholar] [CrossRef]
- Bjørnbak, C.; Engel, P.J.H.; Nielsen, P.L.; Munck, L.K. Microscopic Colitis: Clinical Findings, Topography and Persistence of Histopathological Subgroups. Aliment. Pharm. 2011, 34, 1225–1234. [Google Scholar] [CrossRef]
- Brydon, W.G.; Culbert, P.; Kingstone, K.; Jarvie, A.; Iacucci, M.; Tenhage, M.; Ghosh, S. An Evaluation of the Use of Serum 7-Alpha-Hydroxycholestenone as a Diagnostic Test of Bile Acid Malabsorption Causing Watery Diarrhea. Can. J. Gastroenterol. 2011, 25, 319–323. [Google Scholar] [CrossRef]
- Appleby, R.N.; Nolan, J.D.; Johnston, I.M.; Pattni, S.S.; Fox, J.; Walters, J.R. Novel Associations of Bile Acid Diarrhoea with Fatty Liver Disease and Gallstones: A Cohort Retrospective Analysis. BMJ Open Gastroenterol. 2017, 4, e000178. [Google Scholar] [CrossRef]
- Davie, M.; Trimble, R.; Robertson, A.R.; Koulaouzidis, A. Faecal Calprotectin and 7-α Cholestenone Levels in Microscopic Colitis: Experience from Edinburgh. Clin. Exp. Gastroenterol. 2020, 13, 115–121. [Google Scholar] [CrossRef]
- Vijayvargiya, P.; Gonzalez Izundegui, D.; Calderon, G.; Tawfic, S.; Batbold, S.; Saifuddin, H.; Duggan, P.; Melo, V.; Thomas, T.; Heeney, M.; et al. Increased Fecal Bile Acid Excretion in a Significant Subset of Patients with Other Inflammatory Diarrheal Diseases. Dig. Dis. Sci. 2022, 67, 2413–2419. [Google Scholar] [CrossRef]
- Mottacki, N.; Simrén, M.; Bajor, A. Review Article: Bile Acid Diarrhoea—Pathogenesis, Diagnosis and Management. Aliment. Pharmacol. Ther. 2016, 43, 884–898. [Google Scholar] [CrossRef] [PubMed]
- Sadowski, D.C.; Camilleri, M.; Chey, W.D.; Leontiadis, G.I.; Marshall, J.K.; Shaffer, E.A.; Tse, F.; Walters, J.R.F. Canadian Association of Gastroenterology Clinical Practice Guideline on the Management of Bile Acid Diarrhea. Clin. Gastroenterol. Hepatol. 2020, 18, 24–41.e1. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Nurko, S. Bile Acid Diarrhea in Adults and Adolescents. Neurogastroenterol. Motil. 2022, 34, e14287. [Google Scholar] [CrossRef] [PubMed]
- Berti, G.; Rettura, F.; Lambiase, C.; Bellini, M. Empirical Trial or Diagnostic Tests for Bile Acid Diarrhea? That Is the Question! J. Dig. Dis. 2021, 22, 557–558. [Google Scholar] [CrossRef] [PubMed]
- Walters, J.R.F.; Tasleem, A.M.; Omer, O.S.; Brydon, W.G.; Dew, T.; Roux, C.W. le A New Mechanism for Bile Acid Diarrhea: Defective Feedback Inhibition of Bile Acid Biosynthesis. Clin. Gastroenterol. Hepatol. 2009, 7, 1189–1194. [Google Scholar] [CrossRef]
- Pouw, R.E.; Bisschops, R.; Gecse, K.B.; De Hertogh, G.; Iacucci, M.; Rutter, M.; Barret, M.; Biermann, K.; Czakó, L.; Hucl, T.; et al. Endoscopic Tissue Sampling—Part 2: Lower Gastrointestinal Tract. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021, 53, 1261–1273. [Google Scholar] [CrossRef]
- Ung, K.-A.; Kilander, A.; Nilsson, O.; Abrahamsson, H. Long-Term Course in Collagenous Colitis and the Impact of Bile Acid Malabsorption and Bile Acid Sequestrants on Histopathology and Clinical Features. Scand. J. Gastroenterol. 2001, 36, 601–609. [Google Scholar] [CrossRef]
- Kamp, E.J.C.A.; Kane, J.S.; Ford, A.C. Irritable Bowel Syndrome and Microscopic Colitis: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 659–668.e1. [Google Scholar] [CrossRef]
- Gadaleta, R.M.; van Mil, S.W.C.; Oldenburg, B.; Siersema, P.D.; Klomp, L.W.J.; van Erpecum, K.J. Bile Acids and Their Nuclear Receptor FXR: Relevance for Hepatobiliary and Gastrointestinal Disease. Biochim. Biophys. Acta 2010, 1801, 683–692. [Google Scholar] [CrossRef]
- Torres, J.; Palmela, C.; de Sena, P.G.; Costa Santos, M.P.; Gouveia, C.; Oliveira, M.H.; Henriques, A.R.; Rodrigues, C.; Cravo, M.; Borralho, P. Farnesoid X Receptor Expression in Microscopic Colitis: A Potential Role in Disease Etiopathogenesis. GE Port. J. Gastroenterol. 2017, 25, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Sayin, S.I.; Wahlström, A.; Felin, J.; Jäntti, S.; Marschall, H.-U.; Bamberg, K.; Angelin, B.; Hyötyläinen, T.; Orešič, M.; Bäckhed, F. Gut Microbiota Regulates Bile Acid Metabolism by Reducing the Levels of Tauro-Beta-Muricholic Acid, a Naturally Occurring FXR Antagonist. Cell Metab. 2013, 17, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Carlson, P.; BouSaba, J.; McKinzie, S.; Vijayvargiya, P.; Magnus, Y.; Sannaa, W.; Wang, X.J.; Chedid, V.; Zheng, T.; et al. Comparison of Biochemical, Microbial and Mucosal MRNA Expression in Bile Acid Diarrhoea and Irritable Bowel Syndrome with Diarrhoea. Gut 2022, 72, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Yang, W.; Chen, Y.; Huang, F.; Lu, L.; Lin, C.; Huang, T.; Ning, Z.; Zhai, L.; Zhong, L.L.; et al. A Clostridia-Rich Microbiota Enhances Bile Acid Excretion in Diarrhea-Predominant Irritable Bowel Syndrome. J. Clin. Investig. 2020, 130, 438–450. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.M.; Cao, Y.; Miller, K.; McGoldrick, J.; Bellavance, D.; Chin, S.M.; Halvorsen, S.; Maxner, B.; Richter, J.M.; Sassi, S.; et al. Microscopic Colitis Is Characterized by Intestinal Dysbiosis. Clin. Gastroenterol. Hepatol. 2020, 18, 984–986. [Google Scholar] [CrossRef]
- Balakrishnan, A.; Polli, J.E. Apical Sodium Dependent Bile Acid Transporter (ASBT, SLC10A2): A Potential Prodrug Target. Mol. Pharm. 2006, 3, 223–230. [Google Scholar] [CrossRef]
- Qie, D.; Zhang, Y.; Gong, X.; He, Y.; Qiao, L.; Lu, G.; Li, Y. SLC10A2 Deficiency-Induced Congenital Chronic Bile Acid Diarrhea and Stunting. Mol. Genet. Genom. Med. 2021, 9, e1740. [Google Scholar] [CrossRef]
- Al-Dury, S.; Marschall, H.-U. Ileal Bile Acid Transporter Inhibition for the Treatment of Chronic Constipation, Cholestatic Pruritus, and NASH. Front. Pharmacol. 2018, 9, 931. [Google Scholar] [CrossRef]
- Fitzpatrick, L.R.; Jenabzadeh, P. IBD and Bile Acid Absorption: Focus on Pre-Clinical and Clinical Observations. Front. Pharmacol. 2020, 11, 564. [Google Scholar] [CrossRef]
- Jung, D. Human Ileal Bile Acid Transporter Gene ASBT (SLC10A2) Is Transactivated by the Glucocorticoid Receptor. Gut 2004, 53, 78–84. [Google Scholar] [CrossRef]
- Ferrell, J.M.; Chiang, J.Y.L. Bile Acid Receptors and Signaling Crosstalk in the Liver, Gut and Brain. Liver Res. 2021, 5, 105–118. [Google Scholar] [CrossRef]
- Walters, J.R.F. The Role of Bile Acids and Their TGR5 Receptor in Irritable Bowel Syndrome and Diarrhoea. Dig. Liver Dis. 2021, 53, 1118–1119. [Google Scholar] [CrossRef] [PubMed]
- Alemi, F.; Poole, D.P.; Chiu, J.; Schoonjans, K.; Cattaruzza, F.; Grider, J.R.; Bunnett, N.W.; Corvera, C.U. The Receptor TGR5 Mediates the Prokinetic Actions of Intestinal Bile Acids and Is Required for Normal Defecation in Mice. Gastroenterology 2013, 144, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Bellini, M.; Gambaccini, D.; Stasi, C.; Urbano, M.T.; Marchi, S.; Usai-Satta, P. Irritable Bowel Syndrome: A Disease Still Searching for Pathogenesis, Diagnosis and Therapy. World J. Gastroenterol. 2014, 20, 8807–8820. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Type of Study | Age and Gender | Symptoms | Criteria to Define BAM | Type of MC | Prevalence of BAM in MC | Associated Treatments | Response to Therapy | Histology after Therapy | |
|---|---|---|---|---|---|---|---|---|---|
| Rampton (UK, 1987) [18] | Case report | 32 years old; F | 10 daily bowel movements, occasionally night evacuation, predefecatory lower abdominal pain. | Response to a trial with cholestyramine. After a week off cholestyramine SeHCAT test showed an increased fractional turnover rate over the gallbladder but a normal daily absorptive efficiency. | NA | 1/1 | Loperamide | No response to oral sulfasalazine, mebeverine, and metronidazole, or topical corticosteroids. Response to cholestyramine (4 g, 3 bowel movements/day of normal feces). | Rectal biopsies taken after cholestyramine intake for three months were normal. |
| Bohr (Sweden, 1996) [19] | Retrospective observational study | Median age 55 (18–87) years old; 142/163 (87%) F, 21/163 (13%) M | Chronic diarrhea | SeHCAT test with a retention <10% on day 7 was considered abnormal. | 163 CC | 10/26 CC that responded to cholestyramine had abnormal SeHCAT test | Sulphasalazine (108/163); mesalazine (16/163); olsalazine (15/163); prednisolone (39/163); budesonide (2/163); metronidazole (44/163); erythromycin (15/163); penicillin (8/163); mepacrine (19/163); loperamide (69/163) | NA | NA |
| Ung (Sweden, 2000) [20] | Uncontrolled clinical study | NA, 22/27 (81%) F, 5/28 (19%) M | Chronic diarrhea | SeHCAT test with a retention <10% on day 7 was considered abnormal. | 27 CC | Abnormal SeHCAT test (<10%) in 12/27 (44%) of CC patients. | 4/27 (15%) non responders to bile acids sequestrants were prescribed sulphasalazine 1 g 2 daily was prescribed for 2 months. 1/27 (4%) non responder to sulphasalazine too, was prescribed metronidazole 0.4 g 3 times daily for 2 weeks followed by 0.4 g 2 daily for 6 months |
| NA |
| Fernández-Bañares (Spain, 2001) [17] | Uncontrolled clinical study | Median age 60.7 ± 2.2, 41/51 (80%) F, 10/51 (20%) M for MC. Median age 55.6 ± 3.2, 3/26 (12%) F, 23/26 (88%) M for CC. Median age 65.1 ± 2.7, 18/25 (72%) F, 7/25 (28%) M for LC |
|
| 26/51 (51%) CC 25/51 (49%) LC |
| Before prescription of cholestyramine:
|
|
|
| Gurbuz (Turkey, 2001) [21] | Case report | 44-yr-old; M | Cholecystectomy for cholelithiasis. On the third postoperative day he had high volume watery diarrhea with loss of approximately 500 mL/24 h and a frequency of three times per day | Response to cholestyramine 12 g/die | LC | 1/1 | NA | Stool volume and frequency progressively decreased; consistency improved. Symptoms relapsed after drug withdrawal. | NA |
| Ung (Sweden, 2002) [22] | Abstract of uncontrolled clinical study | NA | Chronic diarrhea | SeHCAT <\=10% | 23 LC | 2/23 (9%) with LC had abnormal SeHCAT (≤10%). No correlation between the SeHCAT values and the degree of colonic inflammation | NA | 6/13 (46%) responded to bile acid sequestrants | NA |
| Fernández-Bañares (Spain, 2003) [23] | Uncontrolled clinical study | Median age 57.0 ± 2.3 in CC, 65.5 ± 2.3 in LC Gender 5/37 (14%) M and 32/37 (86%) F in CC; 11/44 (25%) M and 33/44 (75%) F | Chronic or recurrent watery diarrhea of at least 1-month duration. | SeHCAT test <11% on day 7 | 37/81 (46%) with CC 44/81 (54%) with LC | In 8/26 (31%) of patients with CC and in 16/26 (62%) of patients with LC BAM was diagnosed | 13/37 (35%) patients with CC and 8/44 (18%) with LC were taking NSAIDs at diagnosis. 16% and 20% of patients with CC and LC, respectively, were on antidepressants.Patients with MC and BAM who failed cholestyramine were treated with mesalazine. Those failing mesalazine were treated with prednisone, and in the last years, with budesonide with controlled ileal release. |
|
|
| Wildt (Denmark, 2003) [24] | Uncontrolled clinical study | SeHCAT <15% was found in 74/133 (56%) patients with chronic diarrhea; 46/74 (62%) F, 28/74 (38%) M. No data for MC group | Chronic diarrhea defined as change in stool frequency and/or consistency for more than 3 weeks | SeHCAT test <15% on day 7 | NA | Of 74 patients with SeHCAT <15%: 12/74 (16%) type 1 BAM, 24/74 (33%) type 2 BAM, 38/74 (51%) type 3 BAM 9/23 (39%) of patients with MC showed SeHCAT <15% | NA | Criteria for remission: reduction of 25% of frequency, or file data reporting excellent or moderate response to treatment
| NA |
| Müller (Sweden, 2004) [25] | Prospective observational study | In 158 patients with non-bloody diarrhea mean age was 46 (range 16–84); 103/158 (65%) F, 55/158 (35%) M | Three or more loose stools daily and/or a substantial increase in stool frequency and/or fluidity for more than 4 weeks | SeHCAT test <10% on day 7 | 34 patients: 8 LC, 12 CC. In the study 14 eosinophilic colitis were also included | 8/34 (26%) | NA | NA | NA |
| Bajor (Sweden, 2006) [26] | Uncontrolled clinical study |
The median age in the collagenous group was 59 years (53 and 70 years) and the gender distribution was 22/25 (88%) F, 3/25 (12%) M. The median age in the control group was 45 years (25 and 47.5) and the gender distribution was 21/29 (72%) F and 8/29 (28%) M | Chronic diarrhea | SeHCAT test <11% on day 7, C4 plasma concentrations over 20 ng/mL were also evaluated | 25 CC | 6/25 (24%) | Before initiation of the treatment with budesonide there was a wash out period of at least 2 weeks of antidiarrheals and drugs with a potential effect on BA metabolism, including corticosteroids. These drugs were not allowed during the study period | After treatment with budesonide 9 mg daily for 8 weeks median 75SeHCAT retention increased from 18% to 35% (p < 0.001) (6 patients (24%) had an abnormal value initially). The C4 values decreased significantly (from 36 to 23 ng/mL, p = 0.04). The 29 healthy controls 75SeHCAT values were 38% (29% and 48%). The difference between the collagenous colitis group and healthy controls (p < 0.0001) disappeared during the treatment (p = 0.26) | NA |
| Bjørnbak (Denmark, 2011) [27] | Retrospective observational study | The median age was (years) 65 CC, 63 LC, 62 MCi. The gender distribution was 200/270 (74%) F and 79/270 (26%) M in CC, 108/168 (64%) F and 60/168 (36%) M in LC, 83/101(82%) F and 18/101 (18%) in MCi | Watery diarrhea with often associated nightly evacuations, urgency, abdominal pain and sometimes loss of weight | SeHCAT test <10% on day 7 | 539 (168 with LC, 270 with CC, 101 MCi) | 70/270 CC (26%), 30/168 LC (18%), 64/101 MCi (63%) | Concomitant therapies at diagnosis:NSAID use was 54/270 (20%) in CC, 20/168 (12%) in LC, 26/101 (26%) in MCi. Salicylic acid use was 81/270 (30%) in CC, 44/168 (26%) in LC, 27/101 (27%) in MCi Proton pump inhibitor use was 89/270 (33%) in CC, 37/168 (22%) in LC, 35/101 (35%) in MCi | Efficacy of different therapies: Psyllium 36⁄86 (42%) CC, 14⁄40 (35%) LC, 7⁄15 (47%) MCi. Psyllium + Calcium 20⁄50 (40%) CC, 5⁄13 (38%) LC, 7⁄15 (47%) MCi Cholestyramine 39⁄95 (41%) CC, 23⁄43 (52%) LC, 22⁄29 (76%) MCi Loperamide 30⁄49 (61%) CC, 11⁄22 (50%) LC, 5⁄6 (83%) MCi Antibiotics 1⁄13 (6%) CC, 2⁄10 (20%) LC, 3⁄10 (30%) MCi 5-ASA 4⁄28 (14%) CC, 1⁄9 (11%) LC, 1⁄6 (17%) MCi Budesonide 135⁄161 (84%) CC, 86⁄98 (88%) LC, 26⁄31 (84%) Azathioprine 7⁄22 (32%) CC, 1⁄10 (10%) LC, 0⁄3 (0%) MCi | NA |
| Brydon (UK, 2011) [28] | Prospective observational study | NA | Chronic diarrhoea | 7-alpha-hydroxy-4-cholesten-3-one serum levels were used to diagnose BAM | 6 CC | 1/6 CC (17%) | NA | NA | NA |
| Appleby (UK, 2017) [29] | Retrospective observational study | SeHCAT >15%: 275 patients, mean age (years) 48.7, gender distribution 176/275 (64%) F, 99/275 (36%) M SeHCAT <15%: 303 patients, mean age (years) 52.1, gender distribution 184/303 (61%) F, 119/303 (39%) M | Chronic diarrhea | SeHCAT test <15% on day 7 | NA |
328 had a completed colonoscopy, of which 172 had a SeHCAT <15% and 156 had a SeHCAT >15%. Two hundred patients had colonic biopsies, of them:
| NA | NA | NA |
| Davie (UK, 2020) [30] | Retrospective observational study | NA | Chronic diarrhea | Values of 7-alpha-hydroxy-4-cholesten-3-one measured >22 ng/mL were diagnostic for BAM | 140/646 CC had 7αC test 20/204 LC had 7αC test |
| NA | NA | NA |
| Vijayvargiya (USA, 2022) [31] | Uncontrolled clinical study | Mean age (years) 66 for CC, 58 for LC. Gender distribution: 27/34 (79%) F and 7/34 (21%) M in CC; 29/32 (91%) F and 3/32 (9%) M in LC. | Chronic diarrhea | BAM was defined as elevated total fecal bile acids (>2337 μmol total bile acids/48 h) or elevated primary faecal bile acids (>10% primary bile acids or >4% primary bile acids + >1000 μmol total bile acids/48 h). | 66 MC (34 CC, 32 LC) | BAM was found in approximately 50% of patients with MC | NA | All patients with MC (with or without BAM) were treated with budesonide. 17/45 (38%) of MC did not improve, 6/17 (35%) had bile acid diarrhea, and 2/6 (33%) improved with BAs. | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sciumè, G.D.; Berti, G.; Lambiase, C.; Paglianiti, I.; Villanacci, V.; Rettura, F.; Grosso, A.; Ricchiuti, A.; Bortoli, N.d.; Usai Satta, P.; et al. Misinterpreting Diarrhea-Predominant Irritable Bowel Syndrome and Functional Diarrhea: Pathophysiological Highlights. J. Clin. Med. 2023, 12, 5787. https://doi.org/10.3390/jcm12185787
Sciumè GD, Berti G, Lambiase C, Paglianiti I, Villanacci V, Rettura F, Grosso A, Ricchiuti A, Bortoli Nd, Usai Satta P, et al. Misinterpreting Diarrhea-Predominant Irritable Bowel Syndrome and Functional Diarrhea: Pathophysiological Highlights. Journal of Clinical Medicine. 2023; 12(18):5787. https://doi.org/10.3390/jcm12185787
Chicago/Turabian StyleSciumè, Giusi Desirè, Ginevra Berti, Christian Lambiase, Italia Paglianiti, Vincenzo Villanacci, Francesco Rettura, Antonio Grosso, Angelo Ricchiuti, Nicola de Bortoli, Paolo Usai Satta, and et al. 2023. "Misinterpreting Diarrhea-Predominant Irritable Bowel Syndrome and Functional Diarrhea: Pathophysiological Highlights" Journal of Clinical Medicine 12, no. 18: 5787. https://doi.org/10.3390/jcm12185787
APA StyleSciumè, G. D., Berti, G., Lambiase, C., Paglianiti, I., Villanacci, V., Rettura, F., Grosso, A., Ricchiuti, A., Bortoli, N. d., Usai Satta, P., Bassotti, G., & Bellini, M. (2023). Misinterpreting Diarrhea-Predominant Irritable Bowel Syndrome and Functional Diarrhea: Pathophysiological Highlights. Journal of Clinical Medicine, 12(18), 5787. https://doi.org/10.3390/jcm12185787