

Outcomes of the Next In Vitro Fertilization Cycle in Women with Polycystic Ovary Syndrome after a Failed In Vitro Maturation Attempt

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Dissemination and Ethics
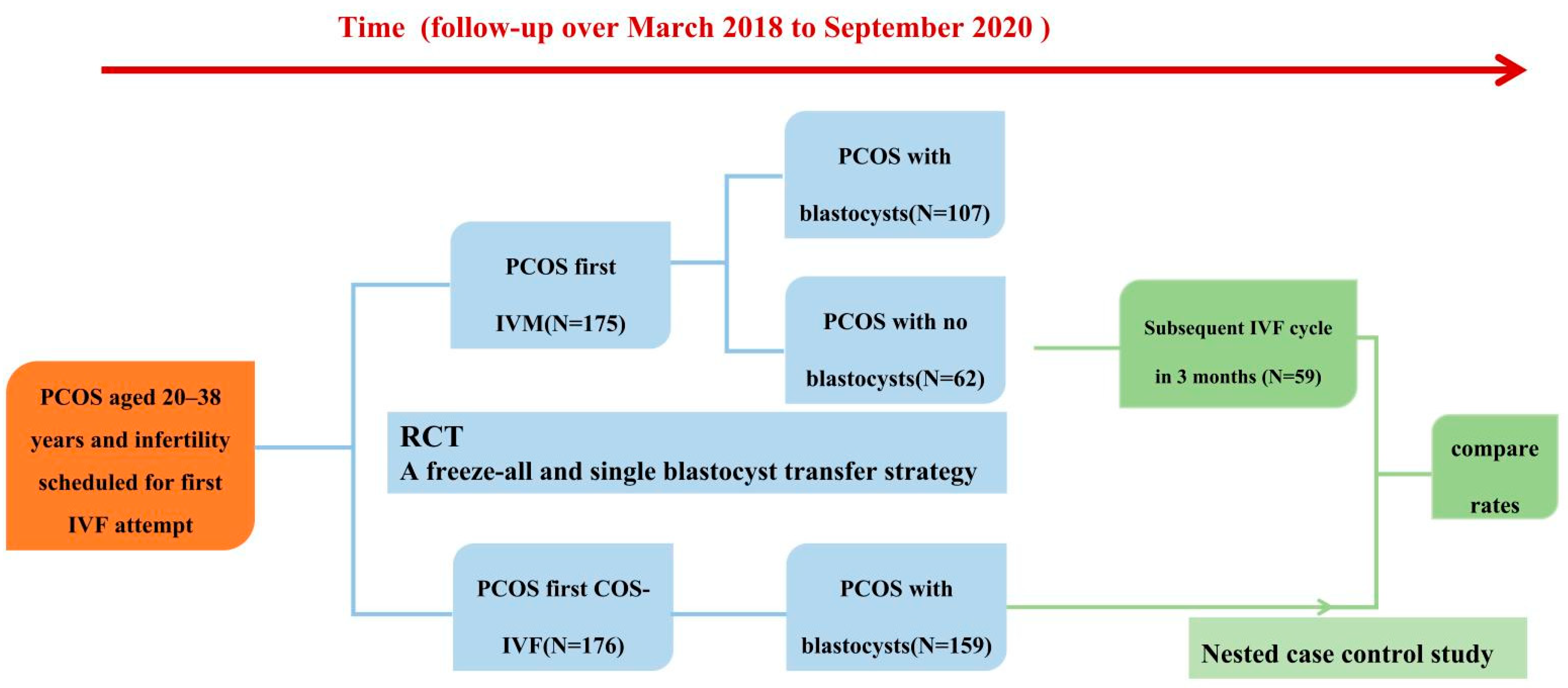
2.2. Study Design (Figure 1)

2.2.1. The Protocol of a Preliminary Study
2.2.2. The Protocol of the Prospective Nested Case–Control Study
2.3. Natural IVM Plus Subsequent IVF Cycle (the Study Group)
2.4. Controlled Ovarian Stimulation (COS) First IVF Cycle (the Control Group)
2.5. Step-by-Step Descriptions of the IVF Procedures: Oocyte Retrieval, In Vitro Fertilization, and Embryo Culture
2.6. Luteal Phase Supplementation
2.7. Variables and Outcome Assessments
2.8. Statistical Analysis
3. Results
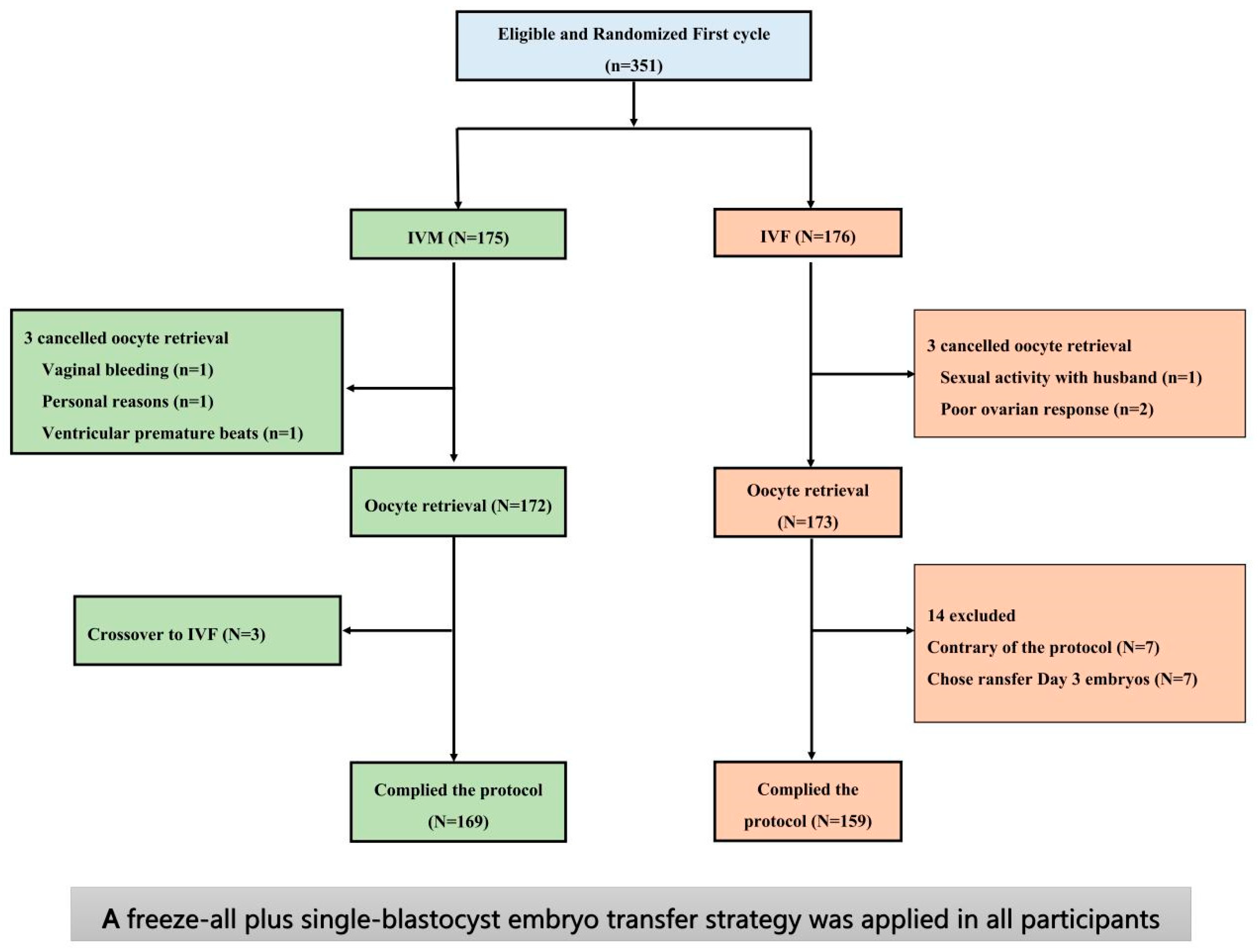
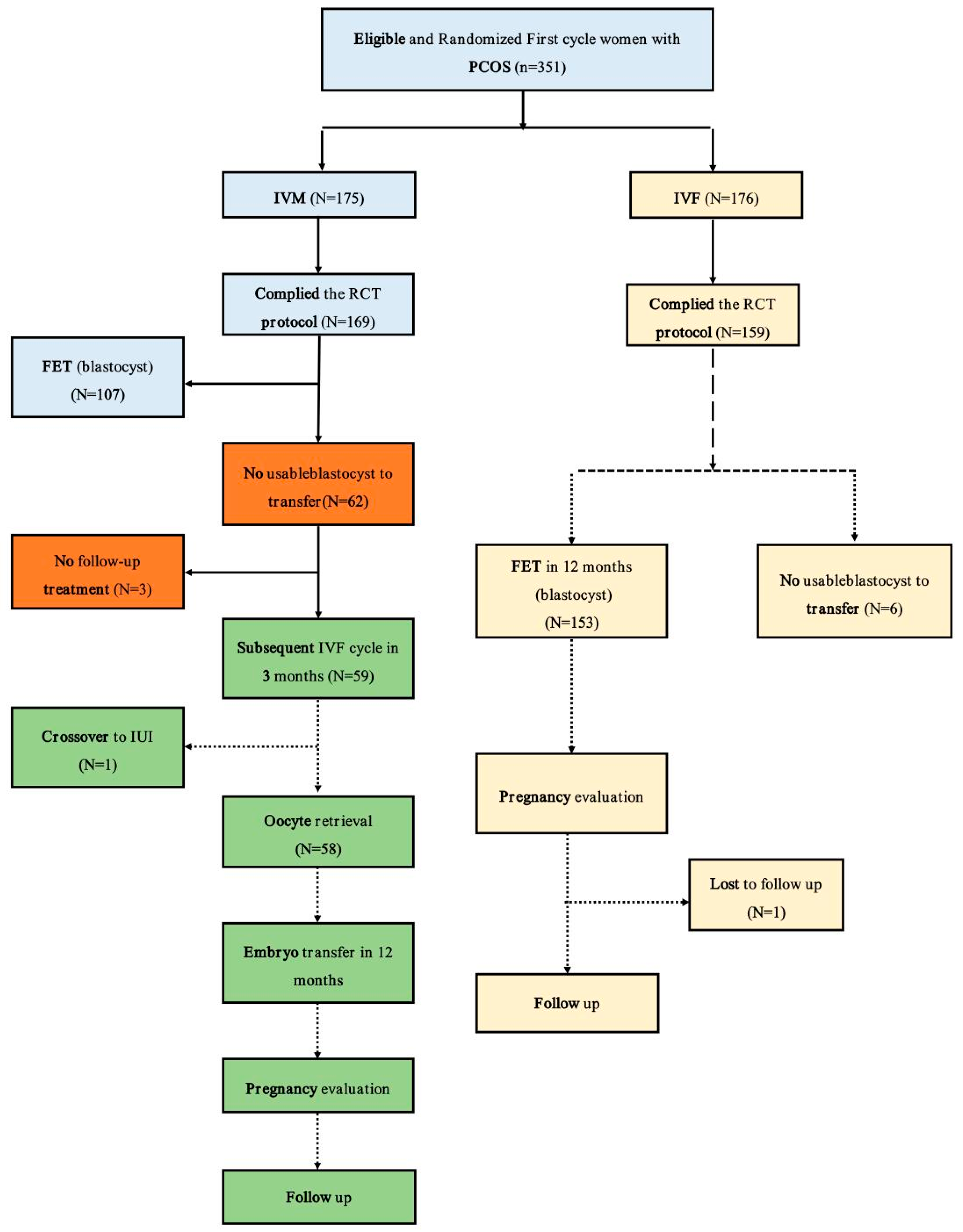
3.1. Participants
3.2. Demographic and Clinical Characteristics
3.3. Primary and Pregnancy Outcomes
3.4. Treatment and Laboratory Measures
3.5. Effect of the Time Interval between IVM and the Subsequent IVF and Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, R.; Zhang, Q.; Yang, D.; Li, S.; Lu, S.; Wu, X.; Wei, Z.; Song, X.; Wang, X.; Fu, S.; et al. Prevalence of polycystic ovary syndrome in women in China: A large community-based study. Hum. Reprod. 2013, 28, 2562–2569. [Google Scholar] [CrossRef]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.; International, P.N. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [PubMed]
- Mourad, S.; Brown, J.; Farquhar, C. Interventions for the prevention of OHSS in ART cycles: An overview of Cochrane reviews. Cochrane Database Syst. Rev. 2017, 1, CD012103. [Google Scholar] [CrossRef] [PubMed]
- Vuong, L.N.; Ho, V.N.A.; Ho, T.M.; Dang, V.Q.; Phung, T.H.; Giang, N.H.; Le, A.H.; Pham, T.D.; Wang, R.; Smitz, J.; et al. In-vitro maturation of oocytes versus conventional IVF in women with infertility and a high antral follicle count: A randomized non-inferiority controlled trial. Hum. Reprod. 2020, 35, 2537–2547. [Google Scholar] [CrossRef] [PubMed]
- Practice Committees of the American Society for Reproductive Medicine; The Society of Reproductive Biologists and Technologists; The Society for Assisted Reproductive Technology. In vitro maturation: A committee opinion. Fertil. Steril. 2021, 115, 298–304. [Google Scholar] [CrossRef]
- Zheng, X.; Guo, W.; Zeng, L.; Zheng, D.; Yang, S.; Wang, L.; Wang, R.; Mol, B.W.; Li, R.; Qiao, J. Live birth after in vitro maturation versus standard in vitro fertilisation for women with polycystic ovary syndrome: Protocol for a non-inferiority randomised clinical trial. BMJ Open 2020, 10, e035334. [Google Scholar] [CrossRef]
- Zheng, X.; Guo, W.; Zeng, L.; Zheng, D.; Yang, S.; Xu, Y.; Wang, L.; Wang, R.; Mol, B.W.; Li, R.; et al. In vitro maturation without gonadotropins versus in vitro fertilization with hyperstimulation in women with polycystic ovary syndrome: A non-inferiority randomized controlled trial. Hum. Reprod. 2022, 37, 242–253. [Google Scholar] [CrossRef]
- Vuong, L.N.; Le, A.H.; Ho, V.N.A.; Pham, T.D.; Sanchez, F.; Romero, S.; De Vos, M.; Ho, T.M.; Gilchrist, R.B.; Smitz, J. Live births after oocyte in vitro maturation with a prematuration step in women with polycystic ovary syndrome. J. Assist. Reprod. Genet. 2020, 37, 347–357. [Google Scholar] [CrossRef]
- Walls, M.L.; Hunter, T.; Ryan, J.P.; Keelan, J.A.; Nathan, E.; Hart, R.J. In vitro maturation as an alternative to standard in vitro fertilization for patients diagnosed with polycystic ovaries: A comparative analysis of fresh, frozen and cumulative cycle outcomes. Hum. Reprod. 2015, 30, 88–96. [Google Scholar] [CrossRef]
- Agdi, M.; Zarei, A.; Al-Sannan, B.; Tulandi, T.; Tan, S.L. Effects of ovarian puncture for in vitro maturation on subsequent in vitro fertilization cycle in women with polycystic ovaries. Fertil. Steril. 2010, 94, 381–383. [Google Scholar] [CrossRef]
- Ferraretti, A.P.; Gianaroli, L.; Magli, M.C.; Iammarrone, E.; Feliciani, E.; Fortini, D. Transvaginal ovarian drilling: A new surgical treatment for improving the clinical outcome of assisted reproductive technologies in patients with polycystic ovary syndrome. Fertil. Steril. 2001, 76, 812–816. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Hrepich, C.; Polyzos, N.P.; Anckaert, E.; Guzman, L.; Tournaye, H.; Smitz, J.; De Vos, M. The effect of ovarian puncture on the endocrine profile of PCOS patients who undergo IVM. Reprod. Biol. Endocrinol. 2014, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Wang, P.; Zhao, J.; Xiao, S.; Yu, R.; Jin, C.; Zhu, R. Outcomes of in vitro fertilization cycles among patients with polycystic ovary syndrome following ovarian puncture for in vitro maturation. Int. J. Gynaecol. Obs. Obstet. 2016, 135, 319–323. [Google Scholar] [CrossRef]
- Braam, S.C.; Consten, D.; Smeenk, J.M.J.; Cohlen, B.J.; Curfs, M.; Hamilton, C.; Repping, S.; Mol, B.W.J.; de Bruin, J.P. In Vitro Maturation of Oocytes in Women at Risk of Ovarian Hyperstimulation Syndrome-A Prospective Multicenter Cohort Study. Int. J. Fertil. Steril. 2019, 13, 38–44. [Google Scholar] [CrossRef]
- Xu, B.; Zhou, M.; Cheng, M.; Zhang, D.; Wu, X.; Si, C.; Xia, L.; Xu, H.; Li, J.; Chang, H.M.; et al. Transvaginal ovarian drilling followed by controlled ovarian stimulation from the next day improves ovarian response for the poor responders with polycystic ovary syndrome during IVF treatment: A pilot study. Reprod. Biol. Endocrinol. 2020, 18, 7. [Google Scholar] [CrossRef]
- Chau, P.; Keltz, M. Transvaginal ovarian drilling for severe polycystic ovary syndrome (PCOS) prior to in vitro fertilization (IVF) improves outcomes. Fertil. Steril. 2010, 94, S196. [Google Scholar] [CrossRef]
- Nada, A.M.; Abdelwahab, H.; Nabil, H.; Mohsen, R.A. Impact of laparoscopic ovarian drilling on the pregnancy rate in clomiphene-resistant polycystic ovarian syndrome patients undergoing in vitro fertilization: Randomized controlled trial. Middle East. Fertil. Soc. J. 2020, 25, 15. [Google Scholar] [CrossRef]
- Patel, A.S.; Leong, J.Y.; Ramasamy, R. Prediction of male infertility by the World Health Organization laboratory manual for assessment of semen analysis: A systematic review. Arab. J. Urol. 2018, 16, 96–102. [Google Scholar] [CrossRef]
- Capkova, J.; Kubatova, A.; Ded, L.; Tepla, O.; Peknicova, J. Evaluation of the expression of sperm proteins in normozoospermic and asthenozoospermic men using monoclonal antibodies. Asian J. Androl. 2016, 18, 108–113. [Google Scholar] [CrossRef]
- Zhu, X.; Tian, T.; Jiesisibieke, D.; Fang, S.; Zhang, N.; Ma, J.; Xia, Y.; Liu, P.; Li, R.; Qiao, J.; et al. Clinical outcome of different embryo transfer strategies after late rescue ICSI procedure: A 10-year total fertilisation failure cohort study. BMC Pregnancy Childbirth 2023, 23, 549. [Google Scholar] [CrossRef]
- Kedem, A.; Yerushalmi, G.M.; Maman, E.; Hemi, R.; Hanochi, M.; Hourvitz, A. What is the optimal threshold of serum Anti-Mullerian hormone (AMH) necessary for IVM treatments? J. Assist. Reprod. Genet. 2013, 30, 745–751. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Seok, H.H.; Song, H.; Lyu, S.W.; Kim, Y.S.; Lee, D.R.; Lee, W.S.; Yoon, T.K. Application of serum anti-Mullerian hormone levels in selecting patients with polycystic ovary syndrome for in vitro maturation treatment. Clin. Exp. Reprod. Med. 2016, 43, 126–132. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dahan, M.H.; Tan, S.L.; Chung, J.; Son, W.Y. Clinical definition paper on in vitro maturation of human oocytes. Hum. Reprod. 2016, 31, 1383–1386. [Google Scholar] [CrossRef] [PubMed]
- Vuong, L.N.; Dang, V.Q.; Ho, T.M.; Huynh, B.G.; Ha, D.T.; Pham, T.D.; Nguyen, L.K.; Norman, R.J.; Mol, B.W. IVF Transfer of Fresh or Frozen Embryos in Women without Polycystic Ovaries. N. Engl. J. Med. 2018, 378, 137–147. [Google Scholar] [CrossRef]
- Ahmad, M.F.; Elias, M.H.; Mat Jin, N.; Abu, M.A.; Syafruddin, S.E.; Zainuddin, A.A.; Suzuki, N.; Abdul Karim, A.K. The spectrum of in vitro maturation in clinical practice: The current insight. Front. Endocrinol. 2023, 14, 1192180. [Google Scholar] [CrossRef]
- Guo, W.; Zheng, X.; Zheng, D.; Yang, Z.; Yang, S.; Yang, R.; Li, R.; Qiao, J. Effectiveness, Flexibility and Safety of Switching IVF to IVM as a Rescue Strategy in Unexpected Poor Ovarian Response for PCOS Infertility Patients. J. Clin. Med. 2023, 12, 1978. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| IVM-IVF Group (N = 58) | IVF Group (N = 158) | p Value | |
|---|---|---|---|
| Age (Median [IQR]) | 29 (27–31) | 29 (27–31.25) | 0.574 |
| Distribution-no. (%) | 0.439 | ||
| <35 years | 53 (91.40%) | 149 (94.30%) | |
| ≥35 years | 5 (8.60%) | 9 (5.70%) | |
| Body-mass index †—kg/m2 (Median [IQR]) | 24.75 (21.58–27.5) | 24 (21.25–27.15) | 0.554 |
| Fertility history | |||
| Duration of the attempt to conceive—years (Median [IQR]) | 3.0 (2.0–5.0) | 3.0 (2.0–4.0) | 0.377 |
| Previous conception—no. (%) | 0.157 | ||
| 0 | 40 (69.00%) | 119 (75.30%) | |
| 1 | 16 (27.60%) | 27 (17.10%) | |
| ≥2 | 2 (3.40%) | 12 (7.60%) | |
| Indications for IVF—no. (%) | 0.185 | ||
| Anovulation only | 14 (24.10%) | 22 (17.70%) | |
| Anovulation combined with other factors | |||
| Female factors | 18 (31.00%) | 51 (32.30%) | |
| Male factors | 20 (34.50%) | 70 (44.30%) | |
| Both factors | 6 (10.30%) | 9 (5.70%) | |
| Ultrasonographic findings | |||
| Antral follicle count in each ovary—no. (%) | 0.99 | ||
| 12~20 | 43 (74.10%) | 117 (74.10%) | |
| >20 | 15 (25.90%) | 41 (25.90%) | |
| Endometrial thickness—mm (Median [IQR]) | 5 (5–6.10) | 5 (5–6) | 0.978 |
| Laboratory tests | |||
| FSH—IU/L (Median [IQR]) | 6.06 (4.63–7.28) | 6.12 (4.69–7.26) | 0.997 |
| LH—IU/L ‡ (Median [IQR]) | 7.62 (4.80–12.25) | 7.08 (4.40–11.10) | 0.364 |
| Estradiol—pmol/L (Median [IQR]) | 184.00 (127–252.5) | 189 (148.95–232.5) | 0.53 |
| Hyperandrogenism § (Distribution-no. (%)) | 28 (48.30%) | 64 (40.50%) | 0.306 |
| AMH—IU/L ** (Median [IQR]) | 9.16 (5.91–15.30) | 9.42 (6.26–13.89) | 0.778 |
| Number of ovulation induction cycles before randomization (Median [IQR]) | 2 (0–4) | 1 (0–3) | |
| PCOS phenotype # | 0.174 | ||
| A—no. (%) | 17 (29.30%) | 45 (28.40%) | |
| C—no. (%) | 13 (22.40%) | 20 (12.70%) | |
| D—no. (%) | 28 (48.30%) | 93 (58.90%) |
| Baseline Characteristics in the Study Group before and after IVM Cycles | |||
|---|---|---|---|
| Before IVM (N = 58) | After IVM (N = 58) | p Value | |
| FSH—IU/L (Median [IQR]) | 5.91 (5.00–7.01) | 6.05 (5.07–6.99) | 0.821 |
| LH—IU/L (Median [IQR]) | 5.59 (3.95–10.75) | 6.70 (4.47–10.18) | 0.639 |
| Estradiol—pmol/L (Median [IQR]) | 159.0 (126.50–222.00) | 167.50 (115.75–213.50) | 0.634 |
| Progesterone—nmol/L (Median [IQR]) | 0.86 (0.64–1.05) | 0.93 (0.64–1.29) | 0.318 |
| IVM-IVF (N = 58) | IVF (N = 158) | Rate Difference (95% CI) | Rate Ratio in the IVM-IVF Group (95% CI) | p Value | |
|---|---|---|---|---|---|
| Total transfer cycles no./total no. (%) | |||||
| Cleavage embryos cycle | 112 (85.50) | ||||
| Blastocyst cycle | 19 (14.50) | 244 (100) | |||
| Primary outcome | |||||
| Live birth—no. (%) ‖ | 33 (56.90) | 93 (58.86) | −0.0196 (−0.1228–0.1672) | 0.923 (0.502–1.696) | 0.795 |
| Secondary pregnancy outcomes | |||||
| Conception—no. (%) † | 51 (87.93) | 128 (81.01) | −0.0692 (−0.0514–0.1607) | 1.708 (0.705–4.135) | 0.232 |
| Clinical pregnancy—no. (%) ‡ | 49 (84.48) | 120 (75.95) | −0.8448 (−0.0436–0.1869) | 1.724 (0.775–3.833) | 0.178 |
| Singleton | 43 | 120 | |||
| Twins * | 6 | 0 | |||
| (Intrauterine with ectopic pregnancy) | 1 | 0 | |||
| Implantation (per embryo)—no./total no. (%) § | |||||
| D3 cleavage embryo | 50/221 (22.62) | 0 | |||
| D5 blastocyst embryo | 7/20 (35.00) | 120/244 (49.18) | −0.1339 (−0.0918–0.3137) | 0.574 (0.222–1.488) | 0.249 |
| Ongoing pregnancy—no. (%) ¶ | 34/58 (58.62) | 96/158 (60.76) | −0.0214 (−0.1196–0.1688) | 0.915 (0.496–1.688) | 0.776 |
| Pregnancy complication | |||||
| Pregnancy loss—no./total no. (%) | 16/49 (32.65) | 30/120 (25.0) | 0.0765 (−0.0657–0.2323) | 1.455 (0.704–3.007) | 0.310 |
| First trimester | 14/49 (28.57) | 24/120 (20.0) | |||
| Second trimester | 2/49 (4.08) | 6/120 (5) |
| IVM-IVF (N = 58) | IVF (N = 158) | Between Group Difference (95% CI) | p Value | |
|---|---|---|---|---|
| Baseline characteristics | ||||
| FSH—IU/L (Median [IQR]) | 6.05 (5.07–6.99) | 6.02 (4.84–7.12) | 0.796 | |
| LH—IU/L (Median [IQR]) | 6.70 (4.47–10.18) | 5.43 (3.95–7.86) | 0.057 | |
| Estradiol—pmol/L (Median [IQR]) | 167.50 (115.75–213.50) | 167.50 (125.25–218) | 0.569 | |
| Progesterone—nmol/L (Median [IQR]) | 0.93 (0.64–1.29) | 0.89 (0.64–1.23) | 0.768 | |
| Oocyte retrieval characteristics | ||||
| Duration of stimulation—days | 10.0 (9.0–11.0) | 10.0 (9.0–12.0) | 0.206 (0.194–0.210) | 0.206 |
| GN starting dose (IU) | 150.0 (150.0–150.0) | 150.0 (125.0–150.0) | 0.00 (0.00–0.00) | 0 |
| GN total dose—IU | 1500.00 (1275.00–2034.38) | 1500 (1275.00–2296.88) | 0.721 (0.713–0.730) | 0.722 |
| Estradiol level on hCG trigger day | 14,428.5 (7246.25–22,516.00) | 12,441 (6920.5–19,503.25) | 0.204 (0.196–0.212) | 0.202 |
| LH level on hCG trigger day | 3.43 (1.11–6.50) | 2.08 (1.34–3.58) | 0.028 (0.024–0.031) | 0.023 |
| p level on hCG trigger day | 2.22 (1.64–3.20) | 1.96 (1.37–2.82) | 0.028 (0.024–0.031) | 0.027 |
| Trigger day LH/basal LH (hLH/bLH) | 0.51 (3.43/6.70) | 0.38 (2.08/5.43) | ||
| Safety endpoints—no. total no. (%) | ||||
| Moderate–severe OHSS | 4/58 (6.9%) | 9/158 (5.7%) | 1.226 (0.363–4.147) | 0.742 |
| Embryology outcomes | ||||
| Fertilization method ‡ | 0.233 | |||
| With IVF | 41 (70.7%) | 121 (76.6%) | ||
| With ICSI | 15 (25.9%) | 36 (22.8%) | ||
| With mixed IVF and ICSI | 2 (3.4%) | 1 (0.6%) | ||
| No. of oocytes retrieved | ||||
| Total | 1315 | 3109 | ||
| Per patient (median (IQR)) | 22 (13–29.25) | 18 (11.00–25.00) | 0.959 | |
| No. of mature oocytes | ||||
| Total (%) | 251/321 (78.19%) | 535/727 (73.59%) | ||
| Per patient (median (IQR)) | 13 (9–23) | 13 (8.25, 20) | 0.702 | |
| No. of 2PN (pronuclear) | ||||
| Total (%) | 757/1315 (57.57) | 1857/3109 (59.7) | ||
| Per patient (median (IQR)) | 11 (6.75–20) | 10 (6, 15) | 0.551 (0.541–0.561) | 0.663 |
| No. of good—quality embryo | ||||
| Total (% per 2PN) | 456/757 (60.24) | 1390/1857 (74.9) | ||
| Per patient (median (IQR)) | 7 (3–11.25) | 8 (5, 12) | 0.066 |
| GN Starting Dose | Duration of Stimulation | GN Total Dose | No. of Oocytes Retrieved | No. of Fertilization | No. of 2PN (Pronuclear) Zygotes | No. of Cleavage | No. of Good—Quality Embryo | No. of Embryos Transferable | No. of Vitrified Blastocysts | Clinical Pregnancy Rate | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time interval of oocyte retrieval in IVM-subsequent IVF (days) | Correlation coefficient | 0.072 | 0.321 * | 0.411 ** | −0.136 | −0.028 | −0.017 | −0.023 | −0.011 | −0.045 | 0.258 | 0.111 |
| Significance | 0.591 | 0.014 | 0.001 | 0.309 | 0.836 | 0.896 | 0.865 | 0.934 | 0.740 | 0.050 | 0.409 | |
| N | 58 | 58 | 58 | 58 | 58 | 58 | 58 | 58 | 58 | 58 | 58 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, W.; Xu, Y.; Tian, T.; Yang, S.; Li, R.; Qiao, J.; Zheng, X. Outcomes of the Next In Vitro Fertilization Cycle in Women with Polycystic Ovary Syndrome after a Failed In Vitro Maturation Attempt. J. Clin. Med. 2023, 12, 5761. https://doi.org/10.3390/jcm12175761
Guo W, Xu Y, Tian T, Yang S, Li R, Qiao J, Zheng X. Outcomes of the Next In Vitro Fertilization Cycle in Women with Polycystic Ovary Syndrome after a Failed In Vitro Maturation Attempt. Journal of Clinical Medicine. 2023; 12(17):5761. https://doi.org/10.3390/jcm12175761
Chicago/Turabian StyleGuo, Wei, Yalan Xu, Tian Tian, Shuo Yang, Rong Li, Jie Qiao, and Xiaoying Zheng. 2023. "Outcomes of the Next In Vitro Fertilization Cycle in Women with Polycystic Ovary Syndrome after a Failed In Vitro Maturation Attempt" Journal of Clinical Medicine 12, no. 17: 5761. https://doi.org/10.3390/jcm12175761
APA StyleGuo, W., Xu, Y., Tian, T., Yang, S., Li, R., Qiao, J., & Zheng, X. (2023). Outcomes of the Next In Vitro Fertilization Cycle in Women with Polycystic Ovary Syndrome after a Failed In Vitro Maturation Attempt. Journal of Clinical Medicine, 12(17), 5761. https://doi.org/10.3390/jcm12175761