
Reference Values for Birth Weight in Relation to Gestational Age in Poland and Comparison with the Global Percentile Standards
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Newborn Parameters
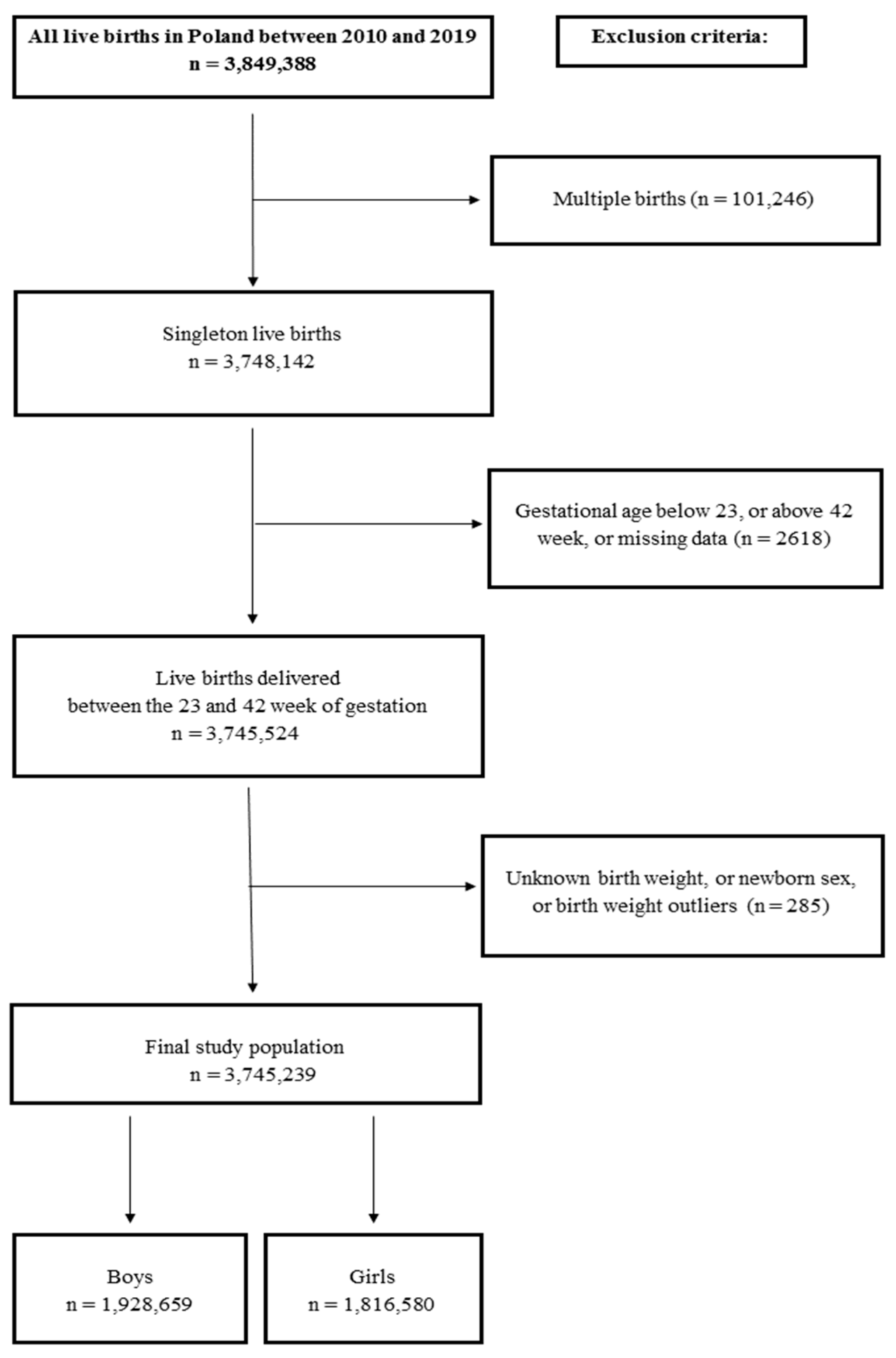
2.3. Exclusion Criteria and Study Population
2.4. Statistical Analysis
2.5. International Comparison
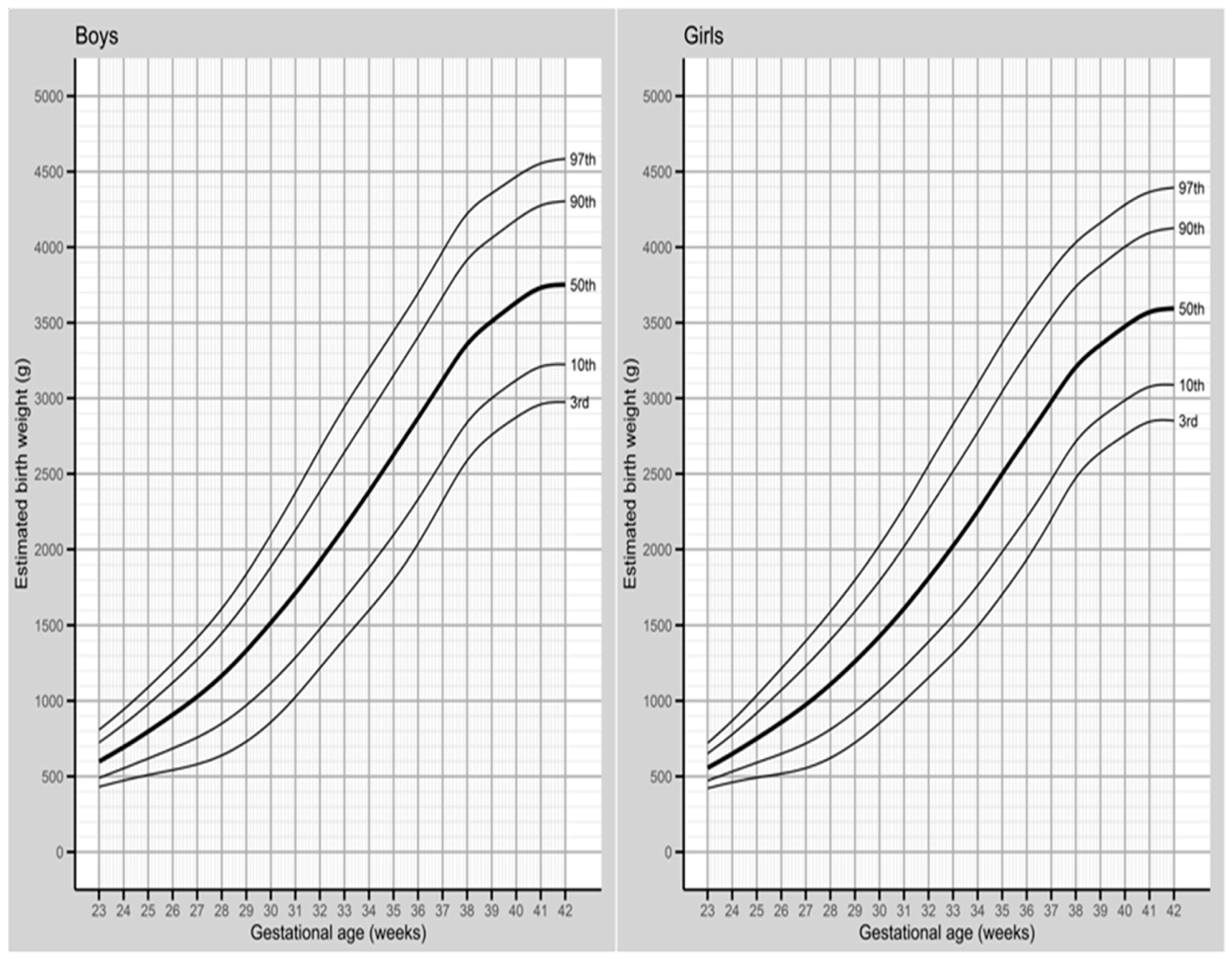
3. Results
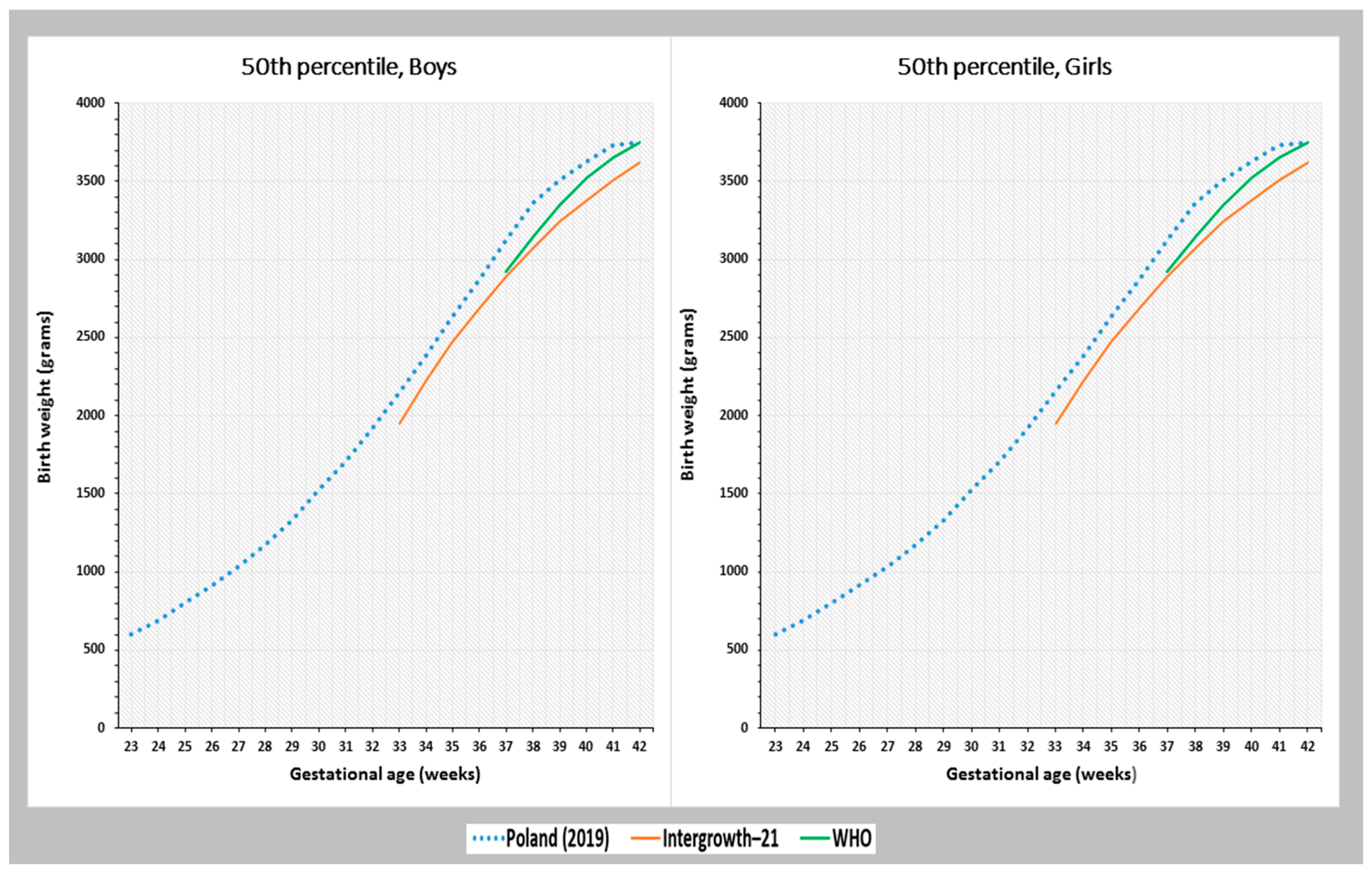
Comparison with the Global References
4. Discussion
4.1. Main Findings of the Study
4.2. Interpretation of Results
4.3. Strengths and Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Norris, T.; Seaton, S.E.; Manktelow, B.N.; Baker, P.N.; Kurinczuk, J.J.; Field, D.; Draper, E.S.; Smith, L.K. Updated birth weight centiles for England and Wales. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F577–F582. [Google Scholar]
- Hajihosseini, M.; Savu, A.; Moore, L.; Dinu, I.; Kaul, P. An updated reference for age-sex-specific birth weight percentiles stratified for ethnicity based on data from all live birth infants between 2005 and 2014 in Alberta, Canada. Can. J. Public Health 2022, 113, 272–281. [Google Scholar]
- Cunningham, F.G.; Leveno, K.J.; Bloom, S.L.; Hauth, J.C.; Rouse, D.J.; Spong, C.Y. Williams Obstetrics, 23rd ed.; McGraw–Hill: New York, NY, USA, 2010. [Google Scholar]
- Chiossi, G.; Pedroza, C.; Costantine, M.M.; Truong, V.T.T.; Gargano, G.; Saade, G.R. Customized vs population-based growth charts to identify neonates at risk of adverse outcome: Systematic review and Bayesian meta-analysis of observational studies. Ultrasound Obstet. Gynecol. 2017, 50, 156–166. [Google Scholar]
- Cartwright, R.D.; Anderson, N.H.; Sadler, L.C.; Harding, J.E.; McCowan, L.M.E.; McKinlay, C.J.D. Neonatal morbidity and small and large size for gestation: A comparison of birthweight centiles. J. Perinatol. 2020, 40, 732–742. [Google Scholar]
- Wołejszo, S.; Genowska, A.; Motkowski, R.; Strukcinskiene, B.; Klukowski, M.; Konstantynowicz, J. Insights into Prevention of Health Complications in Small for Gestational Age (SGA) Births in Relation to Maternal Characteristics: A Narrative Review. J. Clin. Med. 2023, 12, 531. [Google Scholar] [PubMed]
- Salmeri, N.; Carbone, I.F.; Cavoretto, P.I.; Farina, A.; Morano, D. Epigenetics Beyond Fetal Growth Restriction: A Comprehensive Overview. Mol. Diagn. Ther. 2022, 26, 607–626. [Google Scholar] [PubMed]
- Kofman, R.; Farkash, R.; Rottenstreich, M.; Samueloff, A.; Wasserteil, N.; Kasirer, Y.; Grisaru Granovsky, S. Parity-Adjusted Term Neonatal Growth Chart Modifies Neonatal Morbidity and Mortality Risk Stratification. J. Clin. Med. 2022, 11, 3097. [Google Scholar] [PubMed]
- Xia, Q.; Cai, H.; Xiang, Y.B.; Zhou, P.; Li, H.; Yang, G.; Jiang, Y.; Shu, X.O.; Zheng, W.; Xu, W.H. Prospective cohort studies of birth weight and risk of obesity, diabetes, and hypertension in adulthood among the Chinese population. J. Diabetes 2019, 11, 55–64. [Google Scholar] [PubMed]
- Genowska, A.; Motkowski, R.; Strukcinskaite, V.; Abramowicz, P.; Konstantynowicz, J. Inequalities in Birth Weight in Relation to Maternal Factors: A Population-Based Study of 3,813,757 Live Births. Int. J. Environ. Res. Public Health 2022, 19, 1384. [Google Scholar]
- Cheng, Y.; Leung, T.Y.; Lao, T.; Chan, Y.M.; Sahota, D.S. Impact of replacing Chinese ethnicity-specific fetal biometry charts with the INTERGROWTH-21(st) standard. BJOG Int. J. Obstet. Gynaecol. 2016, 123 (Suppl. S3), 48–55. [Google Scholar]
- Stirnemann, J.J.; Fries, N.; Bessis, R.; Fontanges, M.; Mangione, R.; Salomon, L.J. Implementing the INTERGROWTH-21st fetal growth standards in France: A ‘flash study’ of the College Français d’Echographie Foetale (CFEF). Ultrasound Obstet. Gynecol. 2017, 49, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Cavoretto, P.I.; Salmeri, N.; Candiani, M.; Farina, A. Reference ranges of uterine artery pulsatility index from first to third trimester based on serial Doppler measurements: Longitudinal cohort study. Ultrasound Obstet. Gynecol. 2023, 61, 474–480. [Google Scholar] [CrossRef]
- Mozas-Moreno, J.; Sánchez-Fernández, M.; González-Mesa, E.; Olmedo-Requena, R.; Amezcua-Prieto, C.; Jiménez-Moleón, J.J. Perinatal and Maternal Outcomes According to the Accurate Term Antepartum Ultrasound Estimation of Extreme Fetal Weights. J. Clin. Med. 2023, 12, 2995. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Altman, D.G.; Purwar, M.; Noble, J.A.; Knight, H.E.; Ruyan, P.; Cheikh Ismail, L.; Barros, F.C.; Lambert, A.; Papageorghiou, A.T.; et al. The objectives, design and implementation of the INTERGROWTH-21st Project. BJOG Int. J. Obstet. Gynaecol. 2013, 120 (Suppl. S2), 9–26. [Google Scholar] [CrossRef] [PubMed]
- Papageorghiou, A.T.; Kennedy, S.H.; Salomon, L.J.; Altman, D.G.; Ohuma, E.O.; Stones, W.; Gravett, M.G.; Barros, F.C.; Victora, C.; Purwar, M.; et al. The INTERGROWTH-21st fetal growth standards: Toward the global integration of pregnancy and pediatric care. Am. J. Obstet. Gynecol. 2018, 218, S630–S640. [Google Scholar] [CrossRef]
- Kiserud, T.; Benachi, A.; Hecher, K.; Perez, R.G.; Carvalho, J.; Piaggio, G.; Platt, L.D. The World Health Organization fetal growth charts: Concept, findings, interpretation, and application. Am. J. Obstet. Gynecol. 2018, 218, S619–S629. [Google Scholar] [CrossRef]
- Poon, L.C.; Tan, M.Y.; Yerlikaya, G.; Syngelaki, A.; Nicolaides, K.H. Birth weight in live births and stillbirths. Ultrasound Obstet. Gynecol. 2016, 48, 602–606. [Google Scholar] [CrossRef]
- Liu, S.; Metcalfe, A.; León, J.A.; Sauve, R.; Kramer, M.S.; Joseph, K.S. Evaluation of the INTERGROWTH-21st project newborn standard for use in Canada. PLoS ONE 2017, 12, e0172910. [Google Scholar] [CrossRef]
- Pritchard, N.; Lindquist, A.; Siqueira, I.D.A.; Walker, S.P.; Permezel, M. INTERGROWTH-21st compared with GROW customized centiles in the detection of adverse perinatal outcomes at term. J. Matern. Fetal Neonatal Med. 2020, 33, 961–966. [Google Scholar] [CrossRef]
- Stampalija, T.; Ghi, T.; Rosolen, V.; Rizzo, G.; Ferrazzi, E.M.; Prefumo, F.; Dall’Asta, A.; Quadrifoglio, M.; Todros, T.; Frusca, T. Current use and performance of the different fetal growth charts in the Italian population. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 252, 323–329. [Google Scholar] [CrossRef]
- Central Statistical Office. Demographic Yearbook 2021; CSO: Warsaw, Poland, 2021.
- Dera-Szymanowska, A.; Horst, N.; Sobkowski, M.; Szymanowski, K. Outcome dependent growth curves for singleton pregnancies based on birth weight of babies for Polish population. Ginekol. Pol. 2020, 91, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Kajdy, A.; Modzelewski, J.; Filipecka-Tyczka, D.; Pokropek, A.; Rabijewski, M. Development of birth weight for gestational age charts and comparison with currently used charts: Defining growth in the Polish population. J. Matern. Fetal Neonatal Med. 2021, 34, 2977–2984. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Cheikh Ismail, L.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef] [PubMed]
- Kiserud, T.; Piaggio, G.; Carroli, G.; Widmer, M.; Carvalho, J.; Neerup Jensen, L.; Giordano, D.; Cecatti, J.G.; Abdel Aleem, H.; Talegawkar, S.A.; et al. The World Health Organization Fetal Growth Charts: A Multinational Longitudinal Study of Ultrasound Biometric Measurements and Estimated Fetal Weight. PLoS Med. 2017, 14, e1002220. [Google Scholar]
- Hoaglin, D.C.; John, W. Tukey and Data Analysis. Statist. Sci. 2003, 18, 311–318. [Google Scholar] [CrossRef]
- Cole, T.J.; Green, P.J. Smoothing reference centile curves: The LMS method and penalized likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef]
- Rigby, R.A.; Stasinopoulos, D.M. Using the Box-Cox t distribution in GAMLSS to model skewness and kurtosis. Stat. Model. 2006, 6, 209–229. [Google Scholar] [CrossRef]
- Rigby, R.A.; Stasinopoulos, D.M. Generalized Additive Models for Location, Scale and Shape. J. R. Stat. Soc. 2005, 54, 507–554. [Google Scholar] [CrossRef]
- Francis, A.; Hugh, O.; Gardosi, J. Customized vs INTERGROWTH-21st standards for the assessment of birthweight and stillbirth risk at term. Am. J. Obstet. Gynecol. 2018, 218, S692–S699. [Google Scholar] [CrossRef]
- Odibo, A.O.; Nwabuobi, C.; Odibo, L.; Leavitt, K.; Obican, S.; Tuuli, M.G. Customized fetal growth standard compared with the INTERGROWTH-21st century standard at predicting small-for-gestational-age neonates. Acta Obstet. Gynecol. Scand. 2018, 97, 1381–1387. [Google Scholar] [CrossRef]
- Choi, S.K.Y.; Gordon, A.; Hilder, L.; Henry, A.; Hyett, J.A.; Brew, B.K.; Joseph, F.; Jorm, L.; Chambers, G.M. Performance of six birth-weight and estimated-fetal-weight standards for predicting adverse perinatal outcome: A 10-year nationwide population-based study. Ultrasound Obstet. Gynecol. 2021, 58, 264–277. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.S. Determinants of low birth weight: Methodological assessment and meta-analysis. Bull. World Health Organ. 1987, 65, 663–737. [Google Scholar] [PubMed]
- Waage, C.W.; Mdala, I.; Stigum, H.; Jenum, A.K.; Birkeland, K.I.; Shakeel, N.; Michelsen, T.M.; Richardsen, K.R.; Sletner, L. Lipid and lipoprotein concentrations during pregnancy and associations with ethnicity. BMC Pregnancy Childbirth 2022, 22, 246. [Google Scholar] [CrossRef] [PubMed]
- Fragoso-Bargas, N.; Opsahl, J.O.; Kiryushchenko, N.; Böttcher, Y.; Lee-Ødegård, S.; Qvigstad, E.; Richardsen, K.R.; Waage, C.W.; Sletner, L.; Jenum, A.K.; et al. Cohort profile: Epigenetics in Pregnancy (EPIPREG)—Population-based sample of European and South Asian pregnant women with epigenome-wide DNA methylation (850k) in peripheral blood leukocytes. PLoS ONE 2021, 16, e0256158. [Google Scholar] [CrossRef]
- Sletner, L.; Nakstad, B.; Yajnik, C.S.; Mørkrid, K.; Vangen, S.; Vårdal, M.H.; Holme, I.M.; Birkeland, K.I.; Jenum, A.K. Ethnic differences in neonatal body composition in a multi-ethnic population and the impact of parental factors: A population-based cohort study. PLoS ONE 2013, 8, e73058. [Google Scholar] [CrossRef]
- Voigt, M.; Rochow, N.; Schneider, K.T.; Hagenah, H.P.; Scholz, R.; Hesse, V.; Wittwer-Backofen, U.; Straube, S.; Olbertz, D. New percentile values for the anthropometric dimensions of singleton neonates: Analysis of perinatal survey data of 2007–2011 from all 16 states of Germany. Z. Geburtshilfe Neonatol. 2014, 218, 210–217. [Google Scholar]
- Ananth, C.V.; Wen, S.W. Trends in fetal growth among singleton gestations in the United States and Canada, 1985 through 1998. Semin. Perinatol. 2002, 26, 260–267. [Google Scholar] [CrossRef]
- Hadfield, R.M.; Lain, S.J.; Simpson, J.M.; Ford, J.B.; Raynes-Greenow, C.H.; Morris, J.M.; Roberts, C.L. Are babies getting bigger? An analysis of birthweight trends in New South Wales, 1990–2005. Med. J. Aust. 2009, 190, 312–315. [Google Scholar] [CrossRef]
- Ghosh, R.E.; Berild, J.D.; Sterrantino, A.F.; Toledano, M.B.; Hansell, A.L. Birth weight trends in England and Wales (1986–2012): Babies are getting heavier. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F264–F270. [Google Scholar] [CrossRef]
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.J.; Bergström, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; Chrousos, G.P.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American and Australian cohorts. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 984–995. [Google Scholar] [CrossRef]
- Marchi, J.; Berg, M.; Dencker, A.; Olander, E.K.; Begley, C. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obes. Rev. 2015, 16, 621–638. [Google Scholar] [CrossRef]
- Lawlor, D.A. The Society for Social Medicine John Pemberton Lecture 2011. Developmental overnutrition-an old hypothesis with new importance? Int. J. Epidemiol. 2013, 42, 7–29. [Google Scholar] [CrossRef] [PubMed]
- Ewington, L.J.; Gardosi, J.; Lall, R.; Underwood, M.; Fisher, J.D.; Wood, S.; Griffin, R.; Harris, K.; Bick, D.; Booth, K.; et al. Induction of labour for predicted macrosomia: Study protocol for the ‘Big Baby’ randomised controlled trial. BMJ Open 2022, 12, e058176. [Google Scholar] [CrossRef] [PubMed]
- Vaiserman, A.M. Birth weight predicts aging trajectory: A hypothesis. Mech. Ageing Dev. 2018, 173, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Reitan, T.; Callinan, S. Changes in smoking rates among pregnant women and the general female population in Australia, Finland, Norway, and Sweden. Nicotine Tob. Res. 2017, 19, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Hiersch, L.; Lipworthm, H.; Kingdomm, J.; Barrettm, J.; Melamedm, N. Identification of the optimal growth chart and threshold for the prediction of antepartum stillbirth. Arch. Gynecol. Obstet. 2021, 303, 381–390. [Google Scholar] [CrossRef]
- Duryea, E.L.; Hawkins, J.S.; McIntire, D.D.; Casey, B.M.; Leveno, K.J. A revised birth weight reference for the United States. Obstet Gynecol. 2014, 124, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Teshome, A.A.; Li, Q.; Garoma, W.; Chen, X.; Wu, M.; Zhang, Y.; Zhang, X.; Lin, L.; Wang, H.; Yang, X.; et al. Gestational diabetes mellitus, pre-pregnancy body mass index and gestational weight gain predicts fetal growth and neonatal outcomes. Clin. Nutr. ESPEN 2021, 42, 307–312. [Google Scholar] [CrossRef]
- Nakashima, Y.; Mori, Y.; Sugiura, H.; Hirose, E.; Toyoshima, K.; Masutani, S.; Tanaka, Y.; Yoda, H. Very low birth weight infants with congenital heart disease: A multicenter cohort study in Japan. J. Cardiol. 2022, 80, 344–350. [Google Scholar] [CrossRef]
- Philips, E.M.; Santos, S.; Trasande, L.; Aurrekoetxea, J.J.; Barros, H.; von Berg, A.; Bergström, A.; Bird, P.K.; Brescianini, S.; Ní Chaoimh, C.; et al. Changes in parental smoking during pregnancy and risks of adverse birth outcomes and childhood overweight in Europe and North America: An individual participant data meta-analysis of 229,000 singleton births. PLoS Med. 2020, 17, e1003182. [Google Scholar] [CrossRef]
- He, J.R.; Xia, H.M.; Liu, Y.; Xia, X.Y.; Mo, W.J.; Wang, P.; Cheng, K.K.; Leung, G.M.; Feng, Q.; Schooling, C.M.; et al. A new birthweight reference in Guangzhou, southern China, and its comparison with the global reference. Arch. Dis. Child. 2014, 99, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.M.; George, K.; Muliyil, J.; Bose, A.; Prasad, J.H. Birthweight centile charts from rural community-based data from southern India. Indian Pediatr. 2013, 50, 1020–1024. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| GA at Delivery [Weeks] | Boys | Girls | Mean of Sex Differences [Grams] | p | ||||
|---|---|---|---|---|---|---|---|---|
| n = 1,928,659 | Mean [Grams] | SD [Grams] | n = 1,816,580 | Mean [Grams] | SD [Grams] | |||
| 23 | 615 | 603 | 85 | 529 | 581 | 82 | 22 | <0.001 |
| 24 | 918 | 700 | 122 | 707 | 650 | 105 | 50 | <0.001 |
| 25 | 1013 | 788 | 153 | 868 | 749 | 144 | 39 | <0.001 |
| 26 | 1185 | 894 | 177 | 1054 | 853 | 198 | 41 | <0.001 |
| 27 | 1496 | 1015 | 235 | 1233 | 960 | 238 | 55 | <0.001 |
| 28 | 1860 | 1155 | 257 | 1500 | 1103 | 266 | 52 | <0.001 |
| 29 | 2100 | 1310 | 286 | 1707 | 1230 | 292 | 80 | <0.001 |
| 30 | 2871 | 1506 | 341 | 2439 | 1420 | 357 | 87 | <0.001 |
| 31 | 3682 | 1687 | 367 | 2878 | 1601 | 370 | 86 | <0.001 |
| 32 | 5602 | 1919 | 418 | 4391 | 1837 | 442 | 82 | <0.001 |
| 33 | 7662 | 2137 | 409 | 6060 | 2037 | 430 | 100 | <0.001 |
| 34 | 13,364 | 2378 | 427 | 10,649 | 2267 | 433 | 111 | <0.001 |
| 35 | 23,633 | 2621 | 440 | 18,872 | 2508 | 438 | 113 | <0.001 |
| 36 | 49,885 | 2867 | 441 | 41,149 | 2744 | 439 | 123 | <0.001 |
| 37 | 119,346 | 3124 | 442 | 101,131 | 2987 | 433 | 137 | <0.001 |
| 38 | 329,249 | 3348 | 432 | 296,488 | 3201 | 414 | 147 | <0.001 |
| 39 | 540,203 | 3501 | 427 | 510,517 | 3348 | 408 | 153 | <0.001 |
| 40 | 566,588 | 3622 | 432 | 558,599 | 3465 | 414 | 157 | <0.001 |
| 41 | 231,119 | 3714 | 433 | 230,026 | 3552 | 414 | 162 | <0.001 |
| 42 | 26,268 | 3751 | 450 | 25,783 | 3589 | 431 | 162 | <0.001 |
| Mean for 23–42 weeks | 3453 | 540 | 3317 | 509 | 136 | <0.001 | ||
| n * | Smoothed Percentiles [Kilograms] | |||||||
|---|---|---|---|---|---|---|---|---|
| 3 | 5 | 10 | 50 | 90 | 95 | 97 | ||
| Boys | ||||||||
| INTERGROWTH–21 (years 2009–2014) | n = 2568 | 2.63 | 2.88 | 3.38 | 3.94 | 4.22 | ||
| WHO (years 2009–2015) | n = 691 | 2.880 | 3.519 | 4.067 | 4.251 | |||
| Poland | ||||||||
| 2010 | n = 208,768 | 2.793 | 2.898 | 3.055 | 3.595 | 4.165 | 4.344 | 4.467 |
| 2011 | n = 194,830 | 2.806 | 2.909 | 3.063 | 3.596 | 4.162 | 4.339 | 4.461 |
| 2012 | n = 193,474 | 2.817 | 2.918 | 3.072 | 3.604 | 4.170 | 4.347 | 4.469 |
| 2013 | n = 184,995 | 2.814 | 2.915 | 3.068 | 3.600 | 4.165 | 4.341 | 4.461 |
| 2014 | n = 188,082 | 2.828 | 2.929 | 3.082 | 3.606 | 4.162 | 4.337 | 4.457 |
| 2015 | n = 184,009 | 2.837 | 2.938 | 3.089 | 3.612 | 4.169 | 4.343 | 4.462 |
| 2016 | n = 191,066 | 2.857 | 2.956 | 3.106 | 3.625 | 4.179 | 4.351 | 4.469 |
| 2017 | n = 200,957 | 2.864 | 2.963 | 3.112 | 3.629 | 4.180 | 4.352 | 4.469 |
| 2018 | n = 194,786 | 2.870 | 2.966 | 3.111 | 3.625 | 4.178 | 4.351 | 4.468 |
| 2019 | n = 187,692 | 2.874 | 2.972 | 3.120 | 3.634 | 4.181 | 4.351 | 4.467 |
| Change between 2010 and 2019 [grams] | +81 | +74 | +65 | +39 | +16 | +7 | 0 | |
| Girls | ||||||||
| INTERGROWTH–21 (years 2009–2014) | n = 2523 | 2.55 | 2.78 | 3.26 | 3.80 | 4.08 | ||
| WHO (years 2009–2015) | n = 608 | 2.748 | 3.336 | 3.871 | 4.060 | |||
| Poland | ||||||||
| 2010 | n = 193,294 | 2.672 | 2.771 | 2.920 | 3.431 | 3.976 | 4.150 | 4.269 |
| 2011 | n = 183,307 | 2.681 | 2.780 | 2.928 | 3.438 | 3.980 | 4.152 | 4.270 |
| 2012 | n = 182,545 | 2.694 | 2.791 | 2.937 | 3.446 | 3.990 | 4.160 | 4.277 |
| 2013 | n = 174,647 | 2.696 | 2.792 | 2.937 | 3.441 | 3.982 | 4.152 | 4.268 |
| 2014 | n = 177,248 | 2.709 | 2.803 | 2.945 | 3.446 | 3.984 | 4.152 | 4.267 |
| 2015 | n = 174,136 | 2.721 | 2.815 | 2.957 | 3.454 | 3.986 | 4.153 | 4.267 |
| 2016 | n = 180,833 | 2.734 | 2.828 | 2.971 | 3.469 | 4.002 | 4.168 | 4.282 |
| 2017 | n = 190,079 | 2.745 | 2.837 | 2.977 | 3.472 | 4.007 | 4.176 | 4.292 |
| 2018 | n = 183,180 | 2.752 | 2.843 | 2.983 | 3.473 | 4.004 | 4.171 | 4.286 |
| 2019 | n = 177,311 | 2.757 | 2.848 | 2.987 | 3.476 | 4.003 | 4.168 | 4.280 |
| Change between 2010 and 2019 [grams] | +85 | +77 | +67 | +45 | +27 | +18 | +11 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genowska, A.; Strukcinskiene, B.; Bochenko-Łuczyńska, J.; Motkowski, R.; Jamiołkowski, J.; Abramowicz, P.; Konstantynowicz, J. Reference Values for Birth Weight in Relation to Gestational Age in Poland and Comparison with the Global Percentile Standards. J. Clin. Med. 2023, 12, 5736. https://doi.org/10.3390/jcm12175736
Genowska A, Strukcinskiene B, Bochenko-Łuczyńska J, Motkowski R, Jamiołkowski J, Abramowicz P, Konstantynowicz J. Reference Values for Birth Weight in Relation to Gestational Age in Poland and Comparison with the Global Percentile Standards. Journal of Clinical Medicine. 2023; 12(17):5736. https://doi.org/10.3390/jcm12175736
Chicago/Turabian StyleGenowska, Agnieszka, Birute Strukcinskiene, Joanna Bochenko-Łuczyńska, Radosław Motkowski, Jacek Jamiołkowski, Paweł Abramowicz, and Jerzy Konstantynowicz. 2023. "Reference Values for Birth Weight in Relation to Gestational Age in Poland and Comparison with the Global Percentile Standards" Journal of Clinical Medicine 12, no. 17: 5736. https://doi.org/10.3390/jcm12175736
APA StyleGenowska, A., Strukcinskiene, B., Bochenko-Łuczyńska, J., Motkowski, R., Jamiołkowski, J., Abramowicz, P., & Konstantynowicz, J. (2023). Reference Values for Birth Weight in Relation to Gestational Age in Poland and Comparison with the Global Percentile Standards. Journal of Clinical Medicine, 12(17), 5736. https://doi.org/10.3390/jcm12175736