
Long-Term Surgical Outcomes and Pathological Analysis of Proctectomy Specimens after Subtotal Colectomy for Ulcerative Colitis: A Retrospective Cohort Study from a Tertiary Centre

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- To assess the long-term surgical outcomes of patients who had undergone a STC as treatment for UC through survival analysis from a tertiary centre;
- Pathological analysis of the proctectomy specimens of patients who had proctectomy by means of analysing the degree of inflammation of the rectal stump, whether there was any inflammation present at the distal margins, and whether the specimens had any dysplasia to determine if IRA would have potentially constituted a suitable alternative surgical treatment strategy.
2. Methods
- -
- Inclusion: patients undergoing a STC for UC;
- -
- Exclusion: patients who did not have an STC or patients who had a STC for a clinical indication other than UC.
3. Results
3.1. Demographics
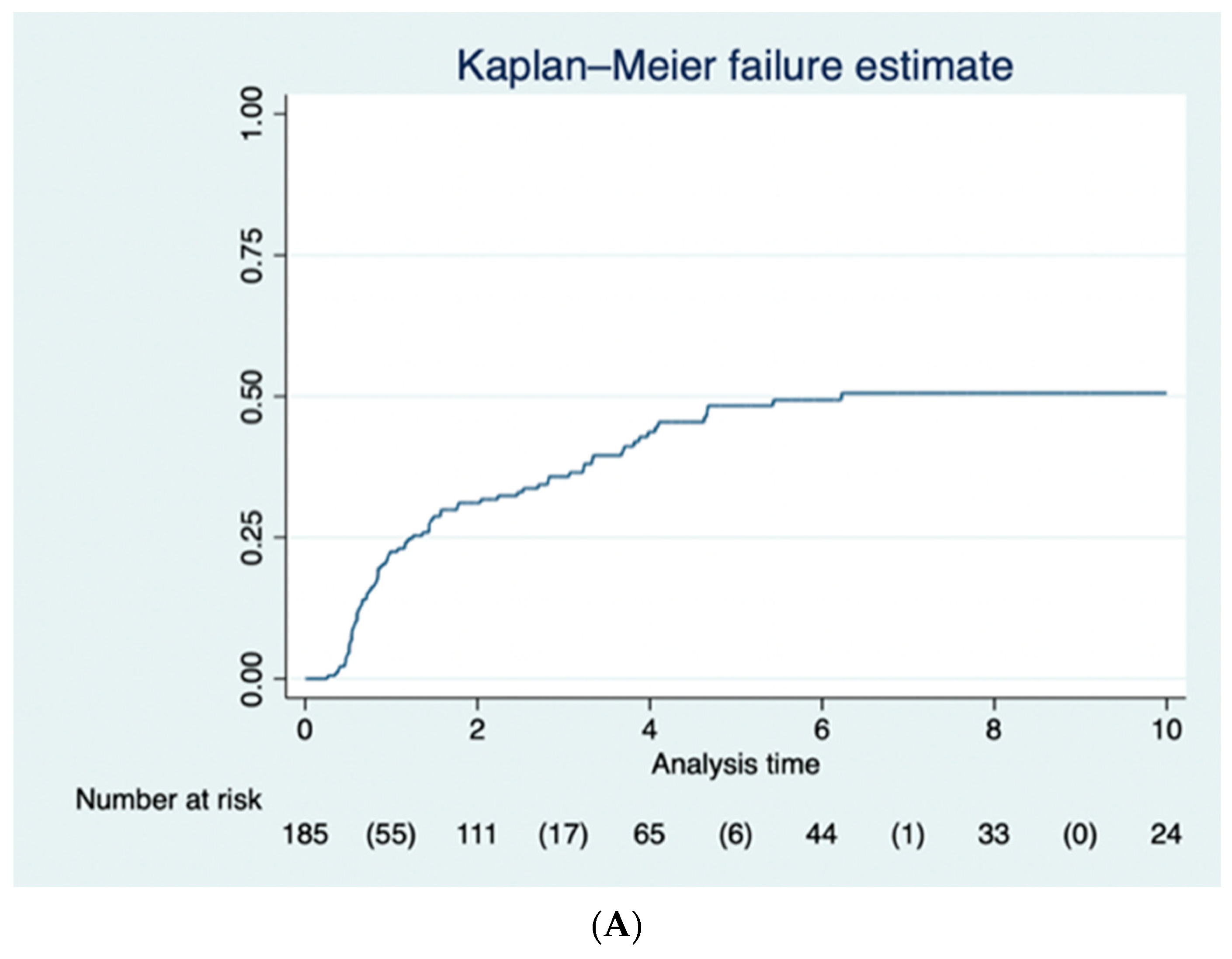
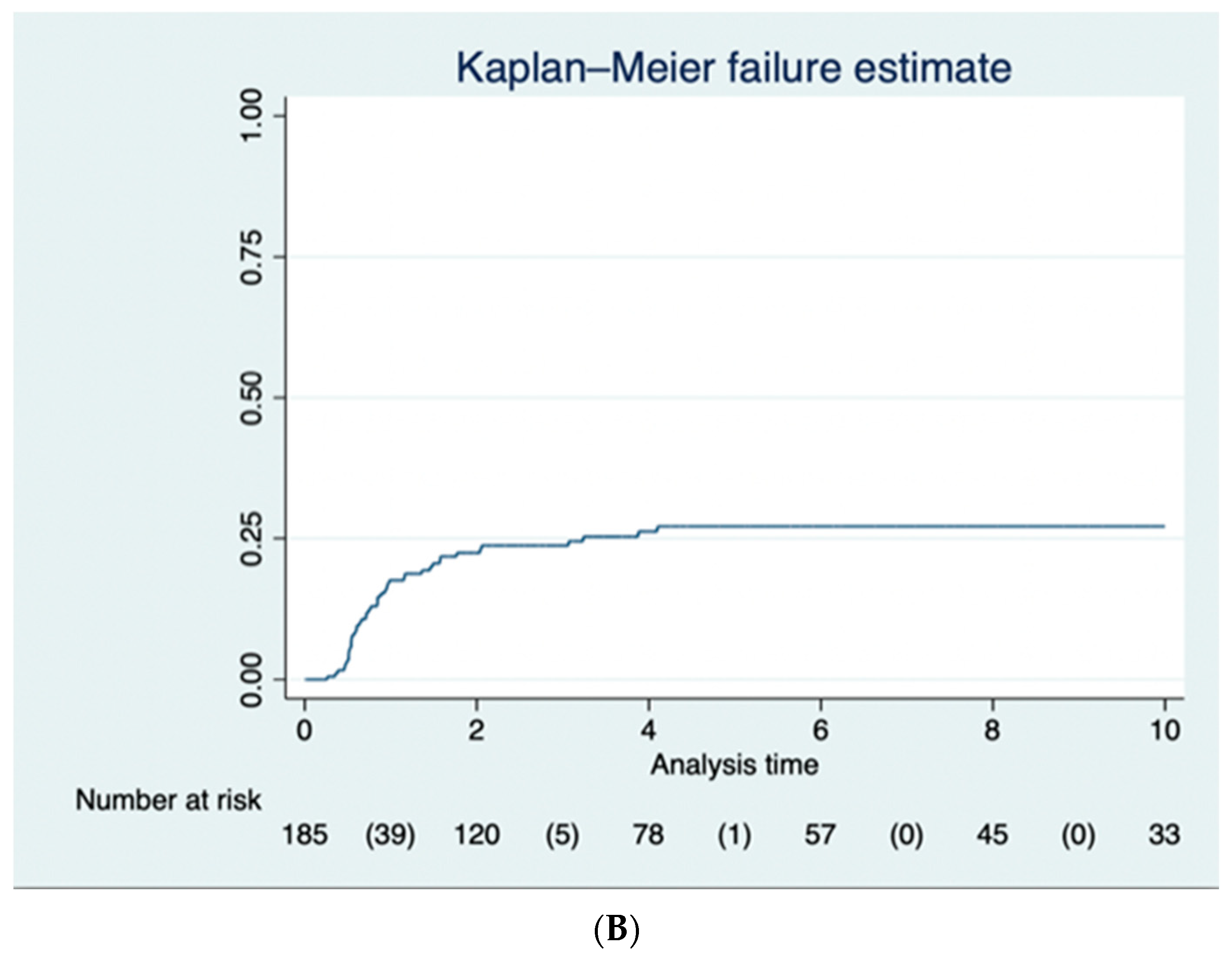
3.2. Long-Term Surgical Outcomes
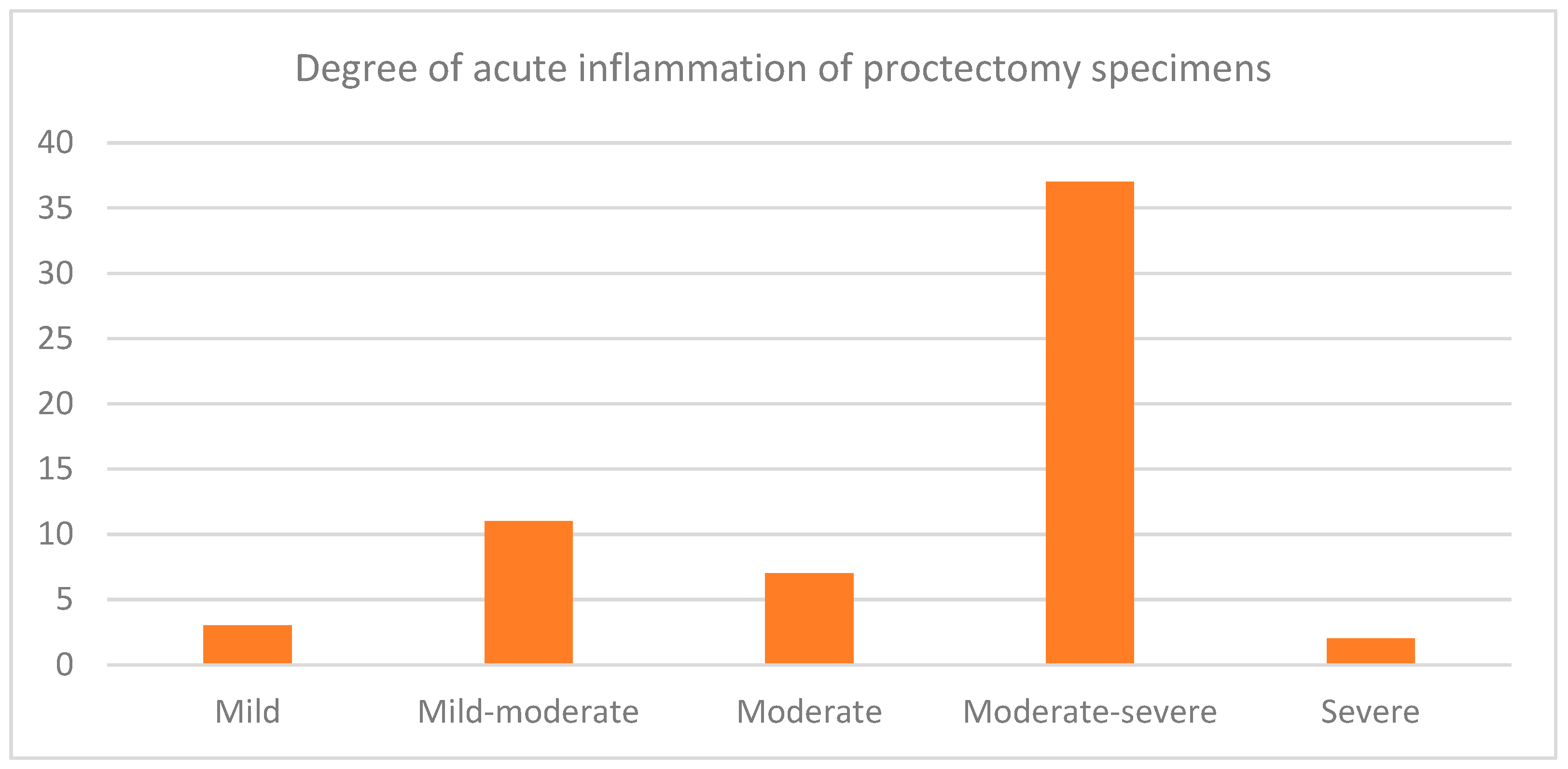
3.3. Evaluation of the Inflammation of the Residual Rectum
4. Discussion
- (1)
- A modest sample size caused by the monocentric design of the study and the low incidence of UC requiring STC. With the hospital’s electronic record only developing in 2014, it also made it difficult to obtain data before this period. The pathology data was also on a different system to the main hospital record, which limited the data that we could obtain from the database of histopathology specimens. This also made it difficult to interpret whether patients before 2014 had adhered to follow-up with endoscopic surveillance.
- (2)
- A follow-up period limited to a maximum of 16 years. Perhaps if we had included earlier, we could have used a longer follow-up period. However, the incidence of metachronous surgery after STC plateaued quite early in our study, and thus, extending the follow-up period may not have necessarily added further useful data.
- (3)
- Our study was designed as a retrospective cohort study, resulting in a possible increased loss to follow-up if patients sought treatment in another centre. A prospective cohort study may have enabled us to keep track of patient adherence to follow-up.
- (4)
- Limited access to data made it very difficult to perform a full analysis on the risk factors for proctectomy. This was particularly the case with any data before the installation of the current electronic health record in 2014.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68 (Suppl. S3), s1–s106. [Google Scholar] [CrossRef] [PubMed]
- Pasvol, T.J.; Horsfall, L.; Bloom, S.; Segal, A.W.; Sabin, C.; Field, N.; Rait, G. Incidence and prevalence of inflammatory bowel disease in UK primary care: A population-based cohort study. BMJ Open 2020, 10, e036584. [Google Scholar] [CrossRef] [PubMed]
- Alatab, S.; Sepanlou, S.G.; Ikuta, K.; Vahedi, H.; Bisignano, C.; Safiri, S.; Sadeghi, A.; Nixon, M.R.; Abdoli, A.; Abolhassani, H.; et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Truelove, S.C.; Witts, L.J. Cortisone in Ulcerative Colitis. Br. Med. J. 1955, 2, 1041–1048. [Google Scholar] [CrossRef]
- Osei-Bimpong, A.; Meek, J.H.; Lewis, S.M. ESR or CRP? A comparison of their clinical utility. Hematology 2007, 12, 353–357. [Google Scholar] [CrossRef]
- Bewtra, M.; Newcomb, C.W.; Wu, Q.; Chen, L.; Xie, F.; Roy, J.A.; Aarons, C.B.; Osterman, M.T.; Forde, K.A.; Curtis, J.R.; et al. Mortality Associated With Medical Therapy Versus Elective Colectomy in Ulcerative Colitis. Ann. Intern. Med. 2015, 163, 262–270. [Google Scholar] [CrossRef]
- Øresland, T.; Bemelman, W.A.; Sampietro, G.M.; Spinelli, A.; Windsor, A.; Ferrante, M.; Marteau, P.; Zmora, O.; Kotze, P.G.; Espin-Basany, E.; et al. European evidence based consensus on surgery for ulcerative colitis. J. Crohn’s Colitis 2015, 9, 4–25. [Google Scholar] [CrossRef]
- Kotze, P.G.; Heuthorst, L.; Lightner, A.L.; Damião, A.O.M.C.; Bemelman, W.A. New insights on the surgical management of ulcerative colitis in the 21st century. Lancet Gastroenterol. Hepatol. 2022, 7, 679–688. [Google Scholar] [CrossRef]
- Böhm, G.; O’dwyer, S.T. The fate of the rectal stump after subtotal colectomy for ulcerative colitis. Int. J. Color. Dis. 2006, 22, 277–282. [Google Scholar] [CrossRef]
- Bellolio, R.F.; Zúñiga, A.J.M.; Wagner, H.P.; Pinedo, M.G.; Duarte, G.I.; Zúñiga, D.A. Ileorectal anastomosis in the surgical treatment of ulcerative colitis: Long-term results. Rev. Médica Chile 2008, 136, 1121–1126. [Google Scholar]
- Scoglio, D.; Ali, U.A.; Fichera, A. Surgical treatment of ulcerative colitis: Ileorectal vs ileal pouch-anal anastomosis. World J. Gastroenterol. 2014, 20, 13211–13218. [Google Scholar] [CrossRef] [PubMed]
- Statistical Software for Data Science|Stata [Internet]. Available online: https://www.stata.com/ (accessed on 14 August 2023).
- Tonelli, F.; Di Martino, C.; Giudici, F. Could Total Colectomy with Ileorectal Anastomosis Be an Alternative to Total Proctocolectomy with Ileal Pouch-Anal Anastomosis in Selected Ulcerative Colitis Patients? Gastroenterol. Res. Pract. 2016, 2016, e5832743. [Google Scholar] [CrossRef] [PubMed]
- Buchs, N.C.; Bloemendaal, A.L.A.; Wood, C.P.J.; Travis, S.; Mortensen, N.J.; Guy, R.J.; George, B.D. Subtotal colectomy for ulcerative colitis: Lessons learned from a tertiary centre. Color. Dis. 2017, 19, O153–O161. [Google Scholar] [CrossRef]
- Hocevar, L.A.; Fitzgerald, B.M. American Society of Anesthesiologists Staging. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: http://www.ncbi.nlm.nih.gov/books/NBK549785/ (accessed on 3 June 2023).
- Al-Rashedy, M.; Mukherjee, T.; Askari, A.; Gurjar, S. A systematic review of outcomes and quality of life after ileorectal anastomosis for ulcerative colitis. Arab. J. Gastroenterol. 2023, 24, 79–84. Available online: https://www.sciencedirect.com/science/article/pii/S1687197923000084 (accessed on 3 June 2023). [CrossRef] [PubMed]
- Elton, C.; Makin, G.; Hitos, K.; Cohen, C.R.G. Mortality, morbidity and functional outcome after ileorectal anastomosis. Br. J. Surg. 2002, 90, 59–65. [Google Scholar] [CrossRef]
- Munie, S.; Hyman, N.; Osler, T. Fate of the Rectal Stump After Subtotal Colectomy for Ulcerative Colitis in the Era of Ileal Pouch–Anal Anastomosis. JAMA Surg. 2013, 148, 408–411. [Google Scholar] [CrossRef]
- Wasmann, K.A.; van der Does de Willebois, E.M.; Koens, L.; Duijvestein, M.; Bemelman, W.A.; Buskens, C.J. The Impact of Rectal Stump Inflammation After Subtotal Colectomy on Pouch Outcomes in Ulcerative Colitis Patients. J. Crohn’s Colitis 2020, 15, 299–306. [Google Scholar] [CrossRef]
- Landerholm, K.; Wood, C.; Bloemendaal, A.; Buchs, N.; George, B.; Guy, R. The rectal remnant after total colectomy for colitis –intra-operative, post-operative and longer-term considerations. Scand. J. Gastroenterol. 2018, 53, 1443–1452. [Google Scholar] [CrossRef]
- Parks, A.G.; Nicholls, R.J. Proctocolectomy without ileostomy for ulcerative colitis. Br. Med. J. 1978, 2, 85–88. [Google Scholar] [CrossRef]
- Berghog, J.; Hermanson, M.; de la Croix, H.; Bengtson, J.; Block, M. Ileo-rectal anastomosis in ulcerative colitis—Long-term outcome, failure and risk of cancer at a tertiary centre. Color. Dis. 2022, 24, 1535–1542. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/codi.16237 (accessed on 24 September 2022). [CrossRef]
- Orkin, B.A.; Telander, R.L.; Wolff, B.G.; Perrault, J.; Ilstrup, D.M. The surgical management of children with ulcerative colitis. The old vs. the new. Dis. Colon Rectum 1990, 33, 947–955. [Google Scholar] [CrossRef]
- Soravia, C.; O’Connor, B.I.; Berk, T.; McLeod, R.S.; Cohen, Z. Functional outcome of conversion of ileorectal anastomosis to ileal pouch-anal anastomosis in patients with familial adenomatous polyposis and ulcerative colitis. Dis. Colon Rectum 1999, 42, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Brar, M.S.; de Buck van Overstraeten, A.; Baxter, N.N. Rectal Cancer Incidence is Low Following Rectal Diversion or Subtotal Colectomy for IBD: Results of a Population-based Study. J. Crohn’s Colitis 2021, 15, 1787–1798. [Google Scholar] [CrossRef]
- Chambers, W.M.; Warren, B.F.; Jewell, D.P.; Mortensen, N.J.M. Cancer surveillance in ulcerative colitis. Br. J. Surg. 2005, 92, 928–936. [Google Scholar] [CrossRef] [PubMed]
- Peyrin-Biroulet, L.; Germain, A.; Patel, A.S.; Lindsay, J.O. Systematic review: Outcomes and post-operative complications following colectomy for ulcerative colitis. Aliment. Pharmacol. Ther. 2016, 44, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, O.; Egan, L.; Joyce, M. Subtotal colectomy in ulcerative colitis—Long term considerations for the rectal stump. World J. Gastrointest. Surg. 2021, 13, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhao, T.; Wu, D.; Li, J.; Wang, M.; Sun, Y.; Hou, S. Colorectal Cancer in Ulcerative Colitis: Mechanisms, Surveillance and Chemoprevention. Curr. Oncol. 2022, 29, 6091–6114. [Google Scholar] [CrossRef]
- Ballester, M.P.; Mesonero, F.; Flórez-Diez, P.; Gómez, C.; Fuentes-Valenzuela, E.; Martín, N.; Senosiain, C.; Vela, M.; Fernández-Clotet, A.; Pérez, P.; et al. Adherence to endoscopic surveillance for advanced lesions and colorectal cancer in inflammatory bowel disease: An AEG and GETECCU collaborative cohort study. Aliment. Pharmacol. Ther. 2022, 55, 1402–1413. [Google Scholar] [CrossRef]
- Anderson, M.; Grucela, A. Robotic Surgery for Ulcerative Colitis. Clin. Colon Rectal Surg. 2021, 34, 292–296. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prathivadi Bhayankaram, K.; Meyer, J.; Sebastian, B.; Davies, J.; Wheeler, J. Long-Term Surgical Outcomes and Pathological Analysis of Proctectomy Specimens after Subtotal Colectomy for Ulcerative Colitis: A Retrospective Cohort Study from a Tertiary Centre. J. Clin. Med. 2023, 12, 5729. https://doi.org/10.3390/jcm12175729
Prathivadi Bhayankaram K, Meyer J, Sebastian B, Davies J, Wheeler J. Long-Term Surgical Outcomes and Pathological Analysis of Proctectomy Specimens after Subtotal Colectomy for Ulcerative Colitis: A Retrospective Cohort Study from a Tertiary Centre. Journal of Clinical Medicine. 2023; 12(17):5729. https://doi.org/10.3390/jcm12175729
Chicago/Turabian StylePrathivadi Bhayankaram, Kethaki, Jeremy Meyer, Boby Sebastian, Justin Davies, and James Wheeler. 2023. "Long-Term Surgical Outcomes and Pathological Analysis of Proctectomy Specimens after Subtotal Colectomy for Ulcerative Colitis: A Retrospective Cohort Study from a Tertiary Centre" Journal of Clinical Medicine 12, no. 17: 5729. https://doi.org/10.3390/jcm12175729
APA StylePrathivadi Bhayankaram, K., Meyer, J., Sebastian, B., Davies, J., & Wheeler, J. (2023). Long-Term Surgical Outcomes and Pathological Analysis of Proctectomy Specimens after Subtotal Colectomy for Ulcerative Colitis: A Retrospective Cohort Study from a Tertiary Centre. Journal of Clinical Medicine, 12(17), 5729. https://doi.org/10.3390/jcm12175729