
Performance of Prognostic Scoring Systems in MINOCA: A Comparison among GRACE, TIMI, HEART, and ACEF Scores
 , ,
, ,  , , ,
, , ,  ,
,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
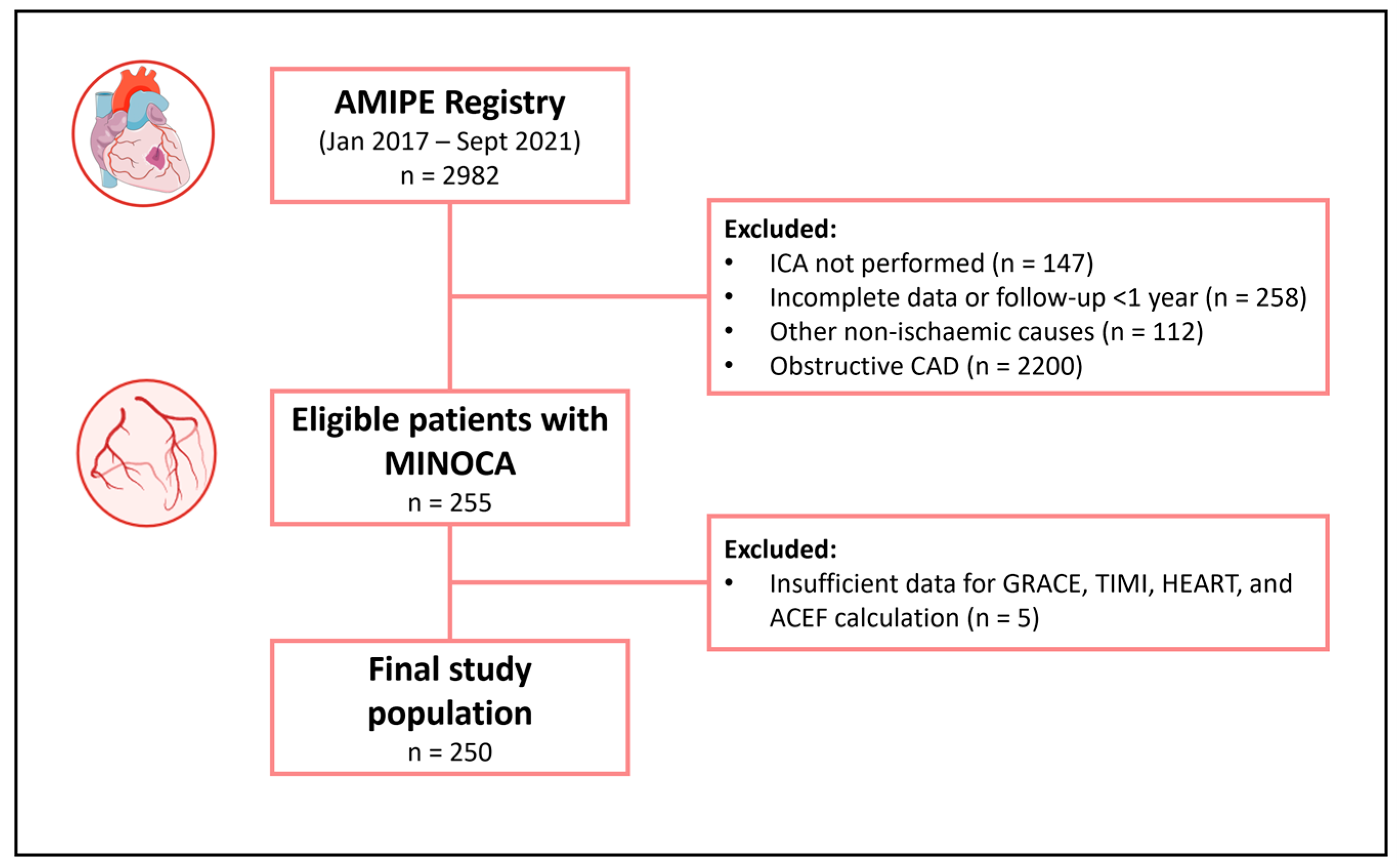
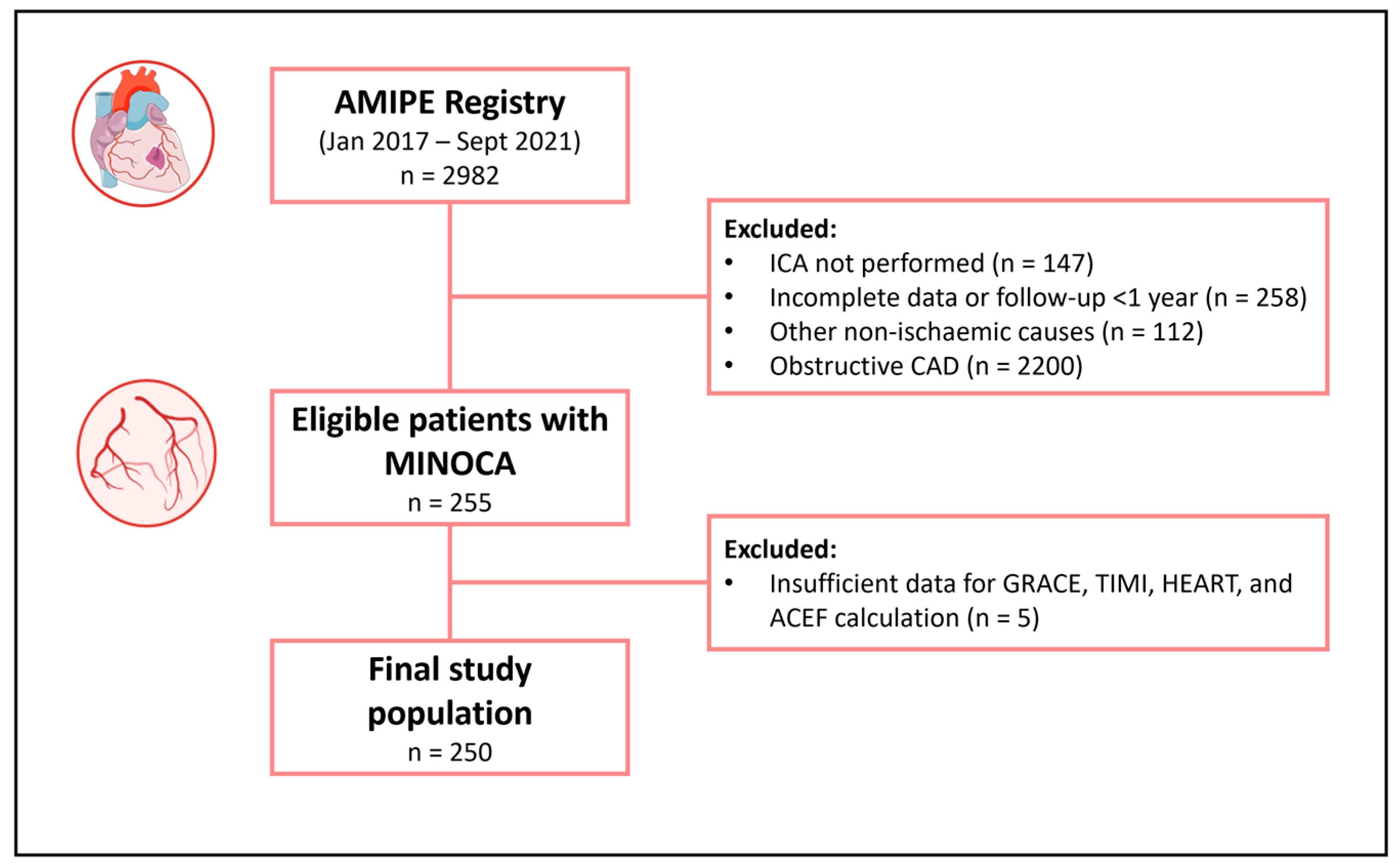
2.1. Study Population
2.2. Study Endpoints
2.3. Statistical Analysis
3. Results
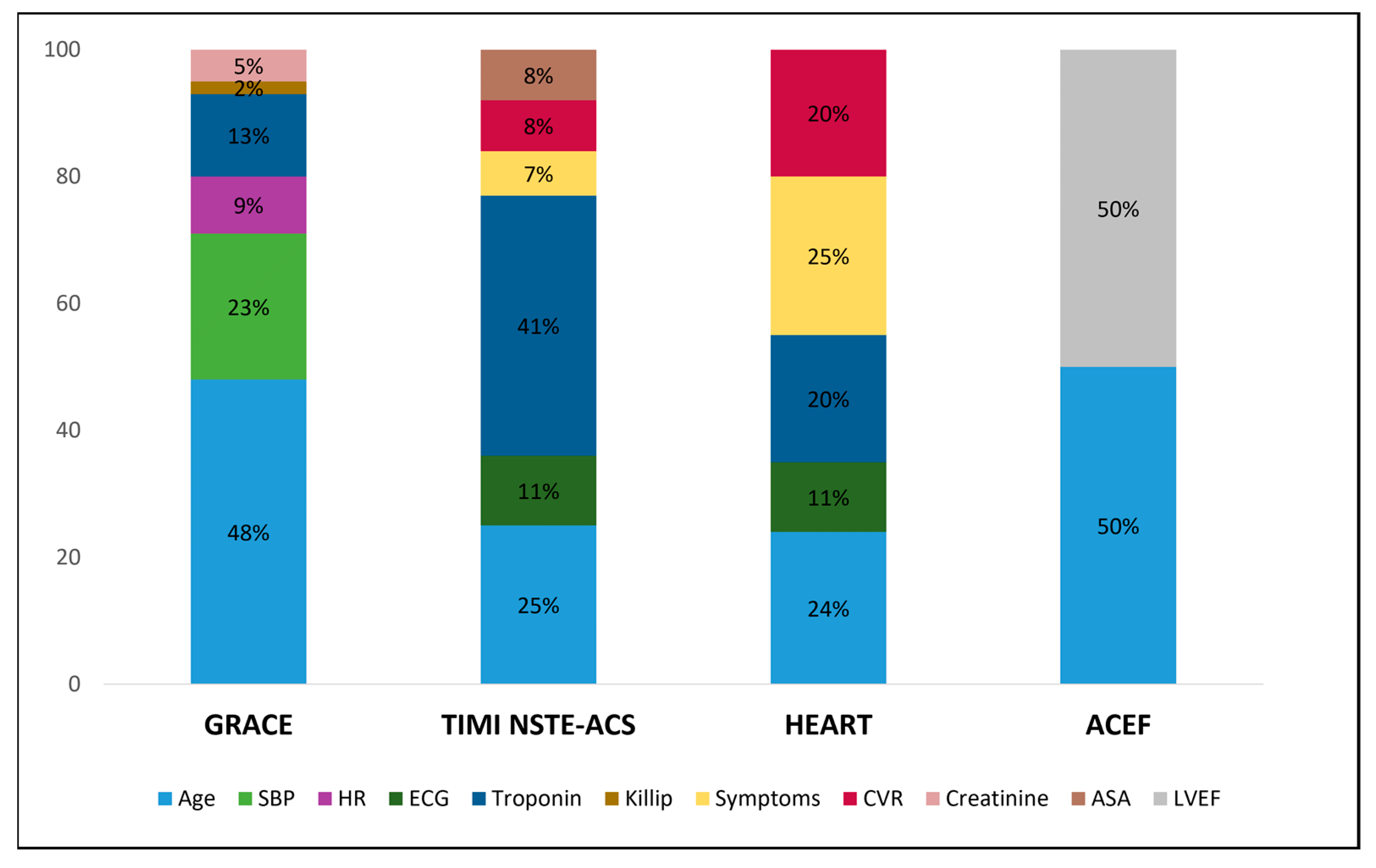
3.1. Admission Clinical Features Included in the Prognostic Scores
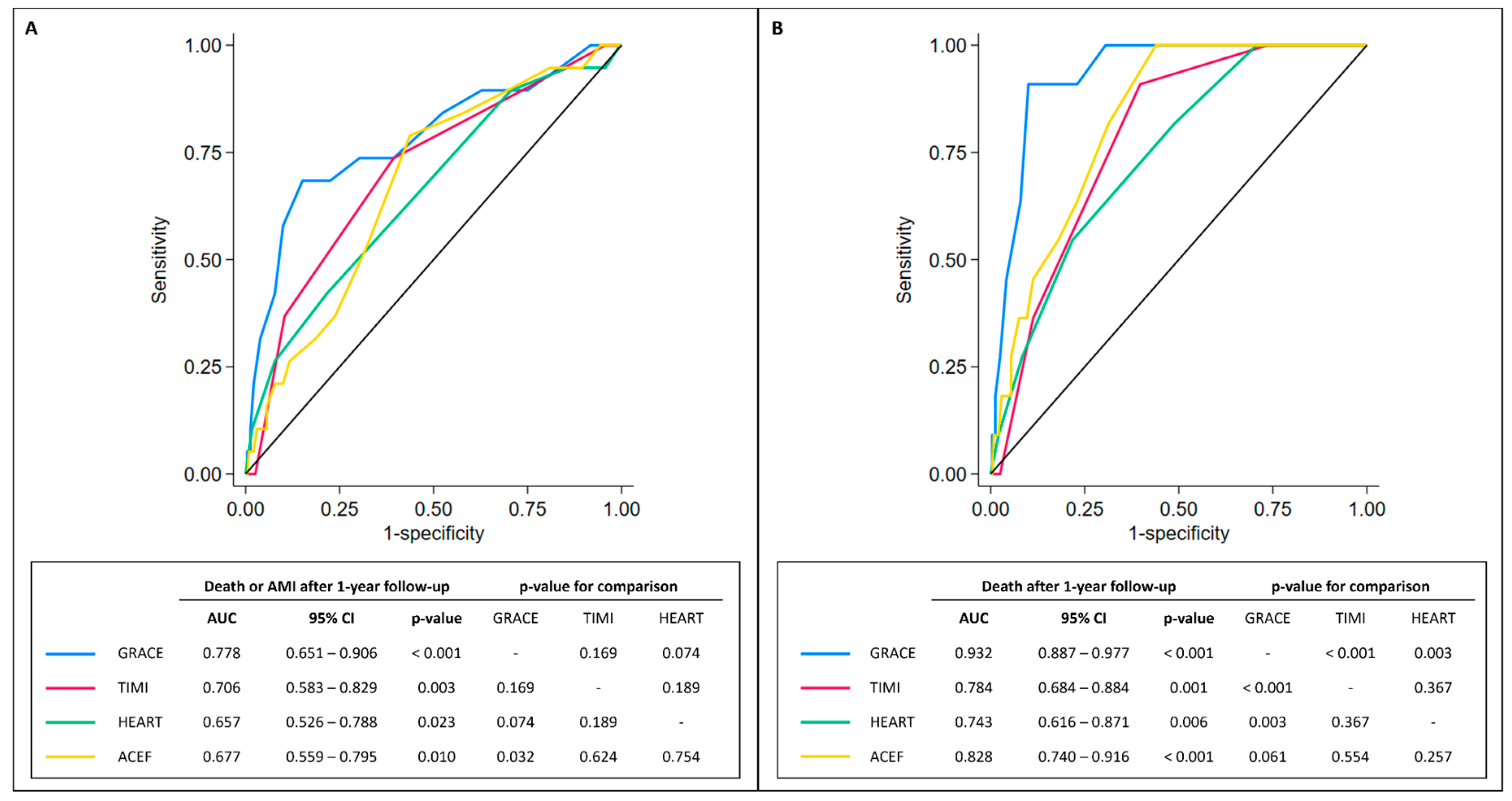
3.2. Prognostic Scoring Systems’ Performance
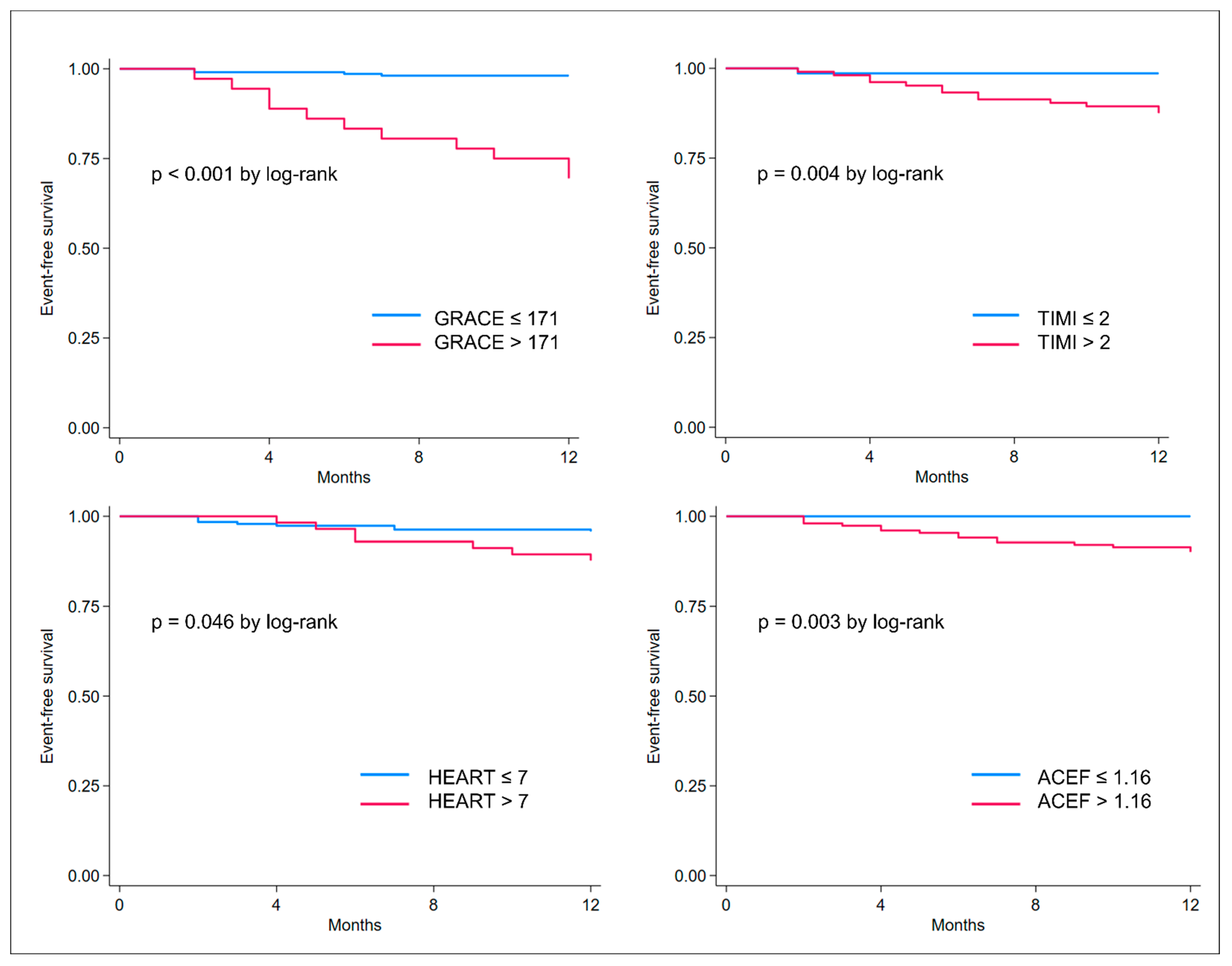
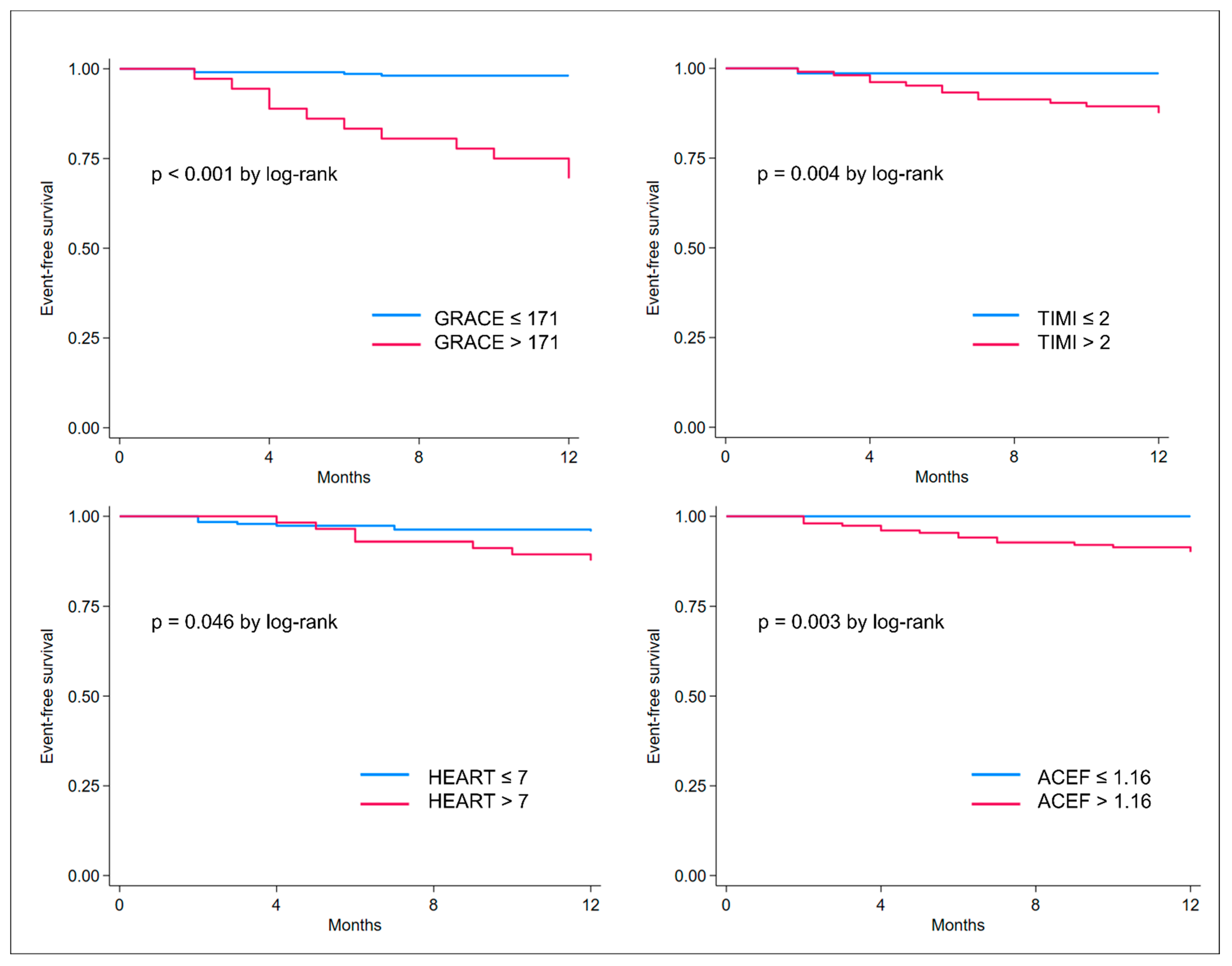
3.3. Best Cut-Offs and Survival Analyses
4. Discussion
4.1. Prognostic Scores in MINOCA
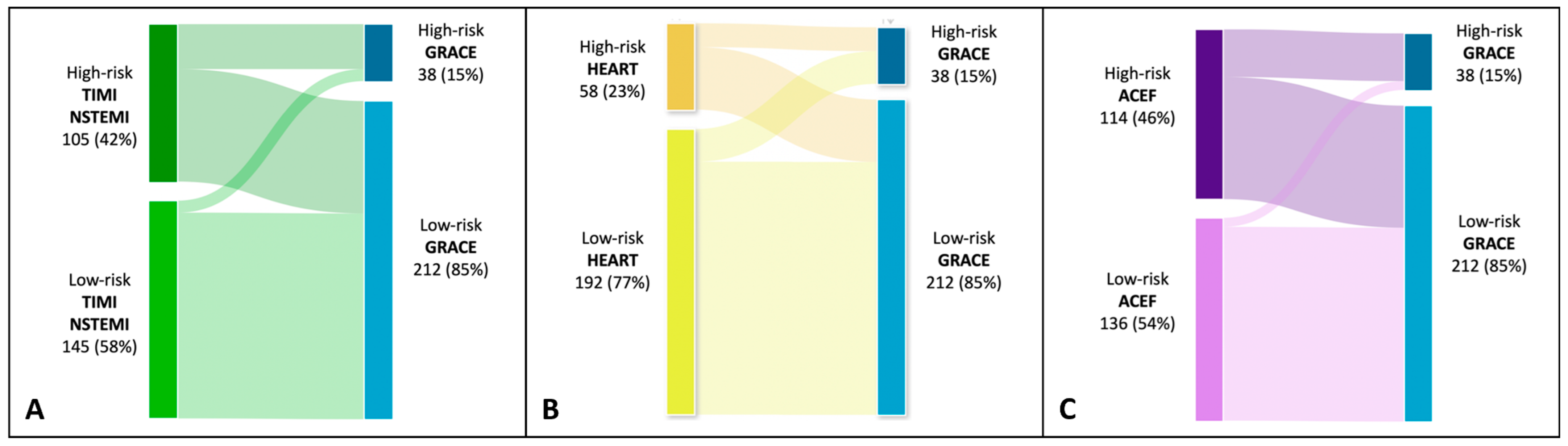
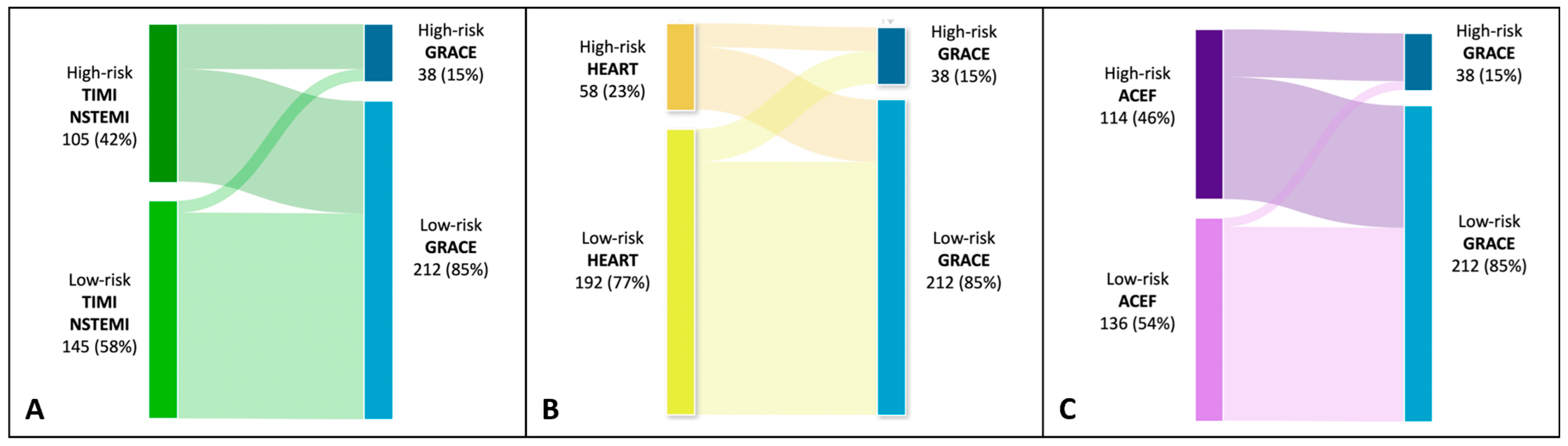
4.2. Risk Categories in MINOCA
4.3. Clinical Implications
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Pasupathy, S.; Air, T.; Dreyer, R.P.; Tavella, R.; Beltrame, J.F. Systematic Review of Patients Presenting with Suspected Myocardial Infarction and Nonobstructive Coronary Arteries. Circulation 2015, 131, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Pasupathy, S.; Lindahl, B.; Litwin, P.; Tavella, R.; Williams, M.J.A.; Air, T.; Zeitz, C.; Smilowitz, N.R.; Reynolds, H.R.; Eggers, K.M.; et al. Survival in Patients with Suspected Myocardial Infarction with Nonobstructive Coronary Arteries: A Comprehensive Systematic Review and Meta-Analysis from the MINOCA Global Collaboration. Circ. Cardiovasc. Qual. Outcomes 2021, 14, e007880. [Google Scholar] [CrossRef] [PubMed]
- Singh, T.; Chapman, A.R.; Dweck, M.R.; Mills, N.L.; Newby, D.E. MINOCA: A heterogenous group of conditions associated with myocardial damage. Heart. 2021, 107, 1458–1464. [Google Scholar] [CrossRef]
- Tamis-Holland, J.E.; Jneid, H.; Reynolds, H.R.; Agewall, S.; Brilakis, E.S.; Brown, T.M.; Lerman, A.; Cushman, M.; Kumbhani, D.J.; Arslanian-Engoren, C.; et al. Contemporary Diagnosis and Management of Patients with Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement from the American Heart Association. Circulation 2019, 139, e891–e908. [Google Scholar] [CrossRef]
- Bassand, J.-P.; Hamm, C.W.; Ardissino, D.; Boersma, E.; Budaj, A.; Fernandez-Aviles, F.; Fox, K.A.A.; Hasdai, D.; Ohman, E.M.; Wallentin, L.; et al. Guidelines for the Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes: The Task Force for the Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes of the European Society of Cardiology. Eur. Heart J. 2007, 28, 1598–1660. [Google Scholar] [CrossRef]
- Granger, C.B. Predictors of Hospital Mortality in the Global Registry of Acute Coronary Events. Arch. Intern. Med. 2003, 163, 2345–2353. [Google Scholar] [CrossRef]
- Eagle, K.A.; Lim, M.J.; Dabbous, O.H.; Pieper, K.S.; Goldberg, R.J.; Van de Werf, F.; Goodman, S.G.; Granger, C.B.; Steg, P.G.; Gore, J.M.; et al. A Validated Prediction Model for All Forms of Acute Coronary Syndrome. JAMA 2004, 291, 2727–2733. [Google Scholar] [CrossRef]
- Yusufali, A.; Zubaid, M.; Al-Zakwani, I.; Alsheikh-Ali, A.A.; Al-Mallah, M.H.; Al Suwaidi, J.; AlMahmeed, W.; Rashed, W.; Sulaiman, K.; Amin, H. Validation of the GRACE Risk Score for Hospital Mortality in Patients with Acute Coronary Syndrome in the Arab Middle East. Angiology 2011, 62, 390–396. [Google Scholar] [CrossRef]
- Elbarouni, B.; Goodman, S.G.; Yan, R.T.; Welsh, R.C.; Kornder, J.M.; DeYoung, J.P.; Wong, G.C.; Rose, B.; Grondin, F.R.; Gallo, R.; et al. Validation of the Global Registry of Acute Coronary Event (GRACE) Risk Score for in-Hospital Mortality in Patients with Acute Coronary Syndrome in Canada. Am. Heart. J. 2009, 158, 392–399. [Google Scholar] [CrossRef]
- Yan, A.T.; Yan, R.T.; Tan, M.; Eagle, K.A.; Granger, C.B.; Dabbous, O.H.; Fitchett, D.; Grima, E.; Langer, A.; Goodman, S.G. In-Hospital Revascularization and One-Year Outcome of Acute Coronary Syndrome Patients Stratified by the GRACE Risk Score. Am. J. Cardiol. 2005, 96, 913–916. [Google Scholar] [CrossRef]
- Tang, E.W.; Wong, C.-K.; Herbison, P. Global Registry of Acute Coronary Events (GRACE) Hospital Discharge Risk Score Accurately Predicts Long-Term Mortality Post Acute Coronary Syndrome. Am. Heart J. 2007, 153, 29–35. [Google Scholar] [CrossRef]
- Reaney, P.D.W.; Elliott, H.I.; Noman, A.; Cooper, J.G. Risk Stratifying Chest Pain Patients in the Emergency Department Using HEART, GRACE and TIMI Scores, with a Single Contemporary Troponin Result, to Predict Major Adverse Cardiac Events. Emerg. Med. J. 2018, 35, 420–427. [Google Scholar] [CrossRef]
- Antman, E.M.; Cohen, M.; Bernink, P.J.L.M.; McCabe, C.H.; Horacek, T.; Papuchis, G.; Mautner, B.; Corbalan, R.; Radley, D.; Braunwald, E. The TIMI Risk Score for Unstable Angina/Non–ST Elevation MI. JAMA 2000, 284, 835–842. [Google Scholar] [CrossRef]
- Yang, B.; Bai, L.; Zhang, Y.; Cheng, Y.; Zhao, C.; Huang, B.; Chen, M. The Value of Different Short-Term Risk Scoring Models in Predicting Long-Term Death of Acute Myocardial Infarction. J. Clin. Med. 2022, 11, 5054. [Google Scholar] [CrossRef] [PubMed]
- Backus, B.E.; Six, A.J.; Kelder, J.C.; Bosschaert, M.A.R.; Mast, E.G.; Mosterd, A.; Veldkamp, R.F.; Wardeh, A.J.; Tio, R.; Braam, R.; et al. A Prospective Validation of the HEART Score for Chest Pain Patients at the Emergency Department. Int. J. Cardiol. 2013, 168, 2153–2158. [Google Scholar] [CrossRef] [PubMed]
- Fiore, G.; Pinto, G.; Preda, A.; Rampa, L.; Gaspardone, C.; Oppizzi, M.; Slavich, M.; Di Napoli, D.; Bianchi, G.; Etteri, M.; et al. Performances of HEART Score to Predict 6-Month Prognostic of Emergency Department Patients with Chest Pain: A Retrospective Cohort Analysis. Eur. J. Emerg. Med. 2023, 30, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Ola, O.; Akula, A.; De Michieli, L.; Knott, J.D.; Lobo, R.; Mehta, R.A.; Hodge, D.O.; Gulati, R.; Sandoval, Y.; Jaffe, A.S. Use of the HEAR Score for 30-Day Risk-Stratification in Emergency Department Patients. Am. J. Med. 2023, 136, 918–926.e5. [Google Scholar] [CrossRef] [PubMed]
- Six, A.J.; Backus, B.E.; Kelder, J.C. Chest Pain in the Emergency Room: Value of the HEART Score. Neth. Heart J. 2008, 16, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Castelvecchio, S.; Menicanti, L.; Frigiola, A.; Pelissero, G. Risk of Assessing Mortality Risk in Elective Cardiac Operations. Circulation 2009, 119, 3053–3061. [Google Scholar] [CrossRef]
- Lee, J.H.; Bae, M.H.; Yang, D.H.; Park, H.S.; Cho, Y.; Jeong, M.H.; Kim, Y.J.; Kim, K.-S.; Hur, S.H.; Seong, I.W.; et al. Prognostic Value of the Age, Creatinine, and Ejection Fraction Score for 1-Year Mortality in 30-Day Survivors Who Underwent Percutaneous Coronary Intervention After Acute Myocardial Infarction. Am. J. Cardiol. 2015, 115, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Stähli, B.E.; Wischnewsky, M.B.; Jakob, P.; Klingenberg, R.; Obeid, S.; Heg, D.; Räber, L.; Windecker, S.; Roffi, M.; Mach, F.; et al. Predictive Value of the Age, Creatinine, and Ejection Fraction (ACEF) Score in Patients with Acute Coronary Syndromes. Int. J. Cardiol. 2018, 270, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef] [PubMed]
- Agewall, S.; Beltrame, J.F.; Reynolds, H.R.; Niessner, A.; Rosano, G.; Caforio, A.L.P.; De Caterina, R.; Zimarino, M.; Roffi, M.; Kjeldsen, K.; et al. ESC Working Group Position Paper on Myocardial Infarction with Non-Obstructive Coronary Arteries. Eur. Heart J. 2017, 38, 143–153. [Google Scholar] [CrossRef]
- Meune, C.; Drexler, B.; Haaf, P.; Reichlin, T.; Reiter, M.; Meissner, J.; Twerenbold, R.; Stelzig, C.; Freese, M.; Winkler, K.; et al. The GRACE Score’s Performance in Predicting in-Hospital and 1-Year Outcome in the Era of High-Sensitivity Cardiac Troponin Assays and B-Type Natriuretic Peptide. Heart 2011, 97, 1479–1483. [Google Scholar] [CrossRef]
- Khand, A.U.; Backus, B.; Campbell, M.; Frost, F.; Mullen, L.; Fisher, M.; Theodoropoulos, K.C.; Obeidat, M.; Batouskaya, K.; Carlton, E.W.; et al. HEART Score Recalibration Using Higher Sensitivity Troponin T. Ann. Emerg. Med. 2023, in press. [Google Scholar] [CrossRef]
- Ma, C.-P.; Wang, X.; Wang, Q.-S.; Liu, X.-L.; He, X.-N.; Nie, S.-P. A Modified HEART Risk Score in Chest Pain Patients with Suspected Non-ST-Segment Elevation Acute Coronary Syndrome. J. Geriatr. Cardiol. 2016, 13, 64–69. [Google Scholar]
- Eggers, K.M.; Baron, T.; Hjort, M.; Nordenskjöld, A.M.; Tornvall, P.; Lindahl, B. GRACE 2.0 Score for Risk Prediction in Myocardial Infarction with Nonobstructive Coronary Arteries. J. Am. Heart Assoc. 2021, 10, e021374. [Google Scholar] [CrossRef]
- Gao, S.; Ma, W.; Huang, S.; Lin, X.; Yu, M. Predictive Value of the Age, Creatinine, and Ejection Fraction Score in Patients with Myocardial Infarction with Nonobstructive Coronary Arteries. Clin. Cardiol. 2021, 44, 1011–1018. [Google Scholar] [CrossRef]
- Canton, L.; Fedele, D.; Bergamaschi, L.; Foà, A.; Di Iuorio, O.; Tattilo, F.P.; Rinaldi, A.; Angeli, F.; Armillotta, M.; Sansonetti, A.; et al. Sex- and Age-Related Differences in Outcomes of Patients with Acute Myocardial Infarction: MINOCA vs. MIOCA. Eur. Heart J. Acute Cardiovasc. Care 2023, zuad059, in press. [Google Scholar] [CrossRef] [PubMed]
- Paolisso, P.; Foà, A.; Bergamaschi, L.; Angeli, F.; Fabrizio, M.; Donati, F.; Toniolo, S.; Chiti, C.; Rinaldi, A.; Stefanizzi, A.; et al. Impact of Admission Hyperglycemia on Short and Long-Term Prognosis in Acute Myocardial Infarction: MINOCA versus MIOCA. Cardiovasc. Diabetol. 2021, 20, 192. [Google Scholar] [CrossRef] [PubMed]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e18–e114. [Google Scholar] [CrossRef] [PubMed]
- Yin, G.; Abdu, F.A.; Liu, L.; Xu, S.; Xu, B.; Luo, Y.; Lv, X.; Fan, R.; Che, W. Prognostic Value of GRACE Risk Scores in Patients with Non-ST-Elevation Myocardial Infarction with Non-Obstructive Coronary Arteries. Front. Cardiovasc. Med. 2021, 8, 582246. [Google Scholar] [CrossRef]
- Eggers, K.M.; Hjort, M.; Baron, T.; Jernberg, T.; Nordenskjöld, A.M.; Tornvall, P.; Lindahl, B. Morbidity and Cause-specific Mortality in First-time Myocardial Infarction with Nonobstructive Coronary Arteries. J. Intern. Med. 2019, 285, 419–428. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Mahajan, A.M.; Roe, M.T.; Hellkamp, A.S.; Chiswell, K.; Gulati, M.; Reynolds, H.R. Mortality of Myocardial Infarction by Sex, Age, and Obstructive Coronary Artery Disease Status in the ACTION Registry–GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry–Get with the Guidelines). Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003443. [Google Scholar] [CrossRef]
- Abdu, F.A.; Liu, L.; Mohammed, A.-Q.; Luo, Y.; Xu, S.; Auckle, R.; Xu, Y.; Che, W. Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA) in Chinese Patients: Clinical Features, Treatment and 1 year Follow-Up. Int. J. Cardiol. 2019, 287, 27–31. [Google Scholar] [CrossRef]
- Rao, K.; De Silva, K.; Sood, A.; Denniss, A.R.; Hsu, C.-J. Predicting Patients with Troponin Positive Chest Pain and Unobstructed Coronary Arteries with Electrocardiogram, Troponin Kinetics and GRACE Score. Heart Lung Circ. 2022, 31, 1219–1227. [Google Scholar] [CrossRef]
- Jobs, A.; Mehta, S.R.; Montalescot, G.; Vicaut, E.; van’t Hof, A.W.J.; Badings, E.A.; Neumann, F.-J.; Kastrati, A.; Sciahbasi, A.; Reuter, P.-G.; et al. Optimal Timing of an Invasive Strategy in Patients with Non-ST-Elevation Acute Coronary Syndrome: A Meta-Analysis of Randomised Trials. Lancet 2017, 390, 737–746. [Google Scholar] [CrossRef]
- Fox, K.A.A.; Clayton, T.C.; Damman, P.; Pocock, S.J.; de Winter, R.J.; Tijssen, J.G.P.; Lagerqvist, B.; Wallentin, L. Long-Term Outcome of a Routine Versus Selective Invasive Strategy in Patients with Non–ST-Segment Elevation Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2010, 55, 2435–2445. [Google Scholar] [CrossRef]
- Mehta, S.R.; Granger, C.B.; Boden, W.E.; Steg, P.G.; Bassand, J.-P.; Faxon, D.P.; Afzal, R.; Chrolavicius, S.; Jolly, S.S.; Widimsky, P.; et al. Early versus Delayed Invasive Intervention in Acute Coronary Syndromes. N. Engl. J. Med. 2009, 360, 2165–2175. [Google Scholar] [CrossRef] [PubMed]
- Kofoed, K.F.; Kelbæk, H.; Hansen, P.R.; Torp-Pedersen, C.; Høfsten, D.; Kløvgaard, L.; Holmvang, L.; Helqvist, S.; Jørgensen, E.; Galatius, S.; et al. Early Versus Standard Care Invasive Examination and Treatment of Patients with Non-ST-Segment Elevation Acute Coronary Syndrome. Circulation 2018, 138, 2741–2750. [Google Scholar] [CrossRef] [PubMed]
- Ciliberti, G.; Verdoia, M.; Merlo, M.; Zilio, F.; Vatrano, M.; Bianco, F.; Mancone, M.; Zaffalon, D.; Bonci, A.; Boscutti, A.; et al. Pharmacological Therapy for the Prevention of Cardiovascular Events in Patients with Myocardial Infarction with Non-Obstructed Coronary Arteries (MINOCA): Insights from a Multicentre National Registry. Int. J. Cardiol. 2021, 327, 9–14. [Google Scholar] [CrossRef]
- Bossard, M.; Gao, P.; Boden, W.; Steg, G.; Tanguay, J.-F.; Joyner, C.; Granger, C.B.; Kastrati, A.; Faxon, D.; Budaj, A.; et al. Antiplatelet Therapy in Patients with Myocardial Infarction without Obstructive Coronary Artery Disease. Heart 2021, 107, 1739–1747. [Google Scholar] [CrossRef]
- Lindahl, B.; Baron, T.; Erlinge, D.; Hadziosmanovic, N.; Nordenskjöld, A.; Gard, A.; Jernberg, T. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients with Myocardial Infarction With Nonobstructive Coronary Artery Disease. Circulation 2017, 135, 1481–1489. [Google Scholar] [CrossRef]
- De Filippo, O.; Russo, C.; Manai, R.; Borzillo, I.; Savoca, F.; Gallone, G.; Bruno, F.; Ahmad, M.; De Ferrari, G.M.; D’Ascenzo, F. Impact of secondary prevention medical therapies on outcomes of patients suffering from Myocardial Infarction with NonObstructive Coronary Artery disease (MINOCA): A meta-analysis. Int J Cardiol. 2022, 368, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, R.; Bashline, M.; Novelli, E.M.; Bliden, K.P.; Tantry, U.S.; Olafiranye, O.; Rahman, A.; Gurbel, P.A.; Pacella, J.J. Sex-related differences in clinical outcomes among patients with myocardial infarction with nonobstructive coronary artery disease: A systematic review and meta-analysis. Int J Cardiol. 2022, 369, 1–4. [Google Scholar] [CrossRef]
- Armillotta, M.; Amicone, S.; Bergamaschi, L.; Angeli, F.; Rinaldi, A.; Paolisso, P.; Stefanizzi, A.; Sansonetti, A.; Impellizzeri, A.; Bodega, F.; et al. Predictive Value of Killip Classification in MINOCA Patients. Eur. J. Intern. Med. 2023, in press. [Google Scholar] [CrossRef]
- Szolc, P.; Niewiara, Ł.; Kleczyński, P.; Bryniarski, K.; Ostrowska-Kaim, E.; Szkodoń, K.; Brzychczy, P.; Żmudka, K.; Legutko, J.; Guzik, B. Clinical Characteristics Predicting Worse Long-Term Outcomes in Patients with Myocardial Infarction and Non-Obstructive Coronary Arteries (MINOCA). J. Cardiovasc. Dev. Dis. 2022, 9, 286. [Google Scholar] [CrossRef]
- Paolisso, P.; Bergamaschi, L.; Rambaldi, P.; Gatta, G.; Foà, A.; Angeli, F.; Fabrizio, M.; Casella, G.; Barbieri, M.; Galiè, N.; et al. Impact of Admission Hyperglycemia on Heart Failure Events and Mortality in Patients with Takotsubo Syndrome at Long-Term Follow-up: Data From HIGH-GLUCOTAKO Investigators. Diabetes Care 2021, 44, 2158–2161. [Google Scholar] [CrossRef]
- Mileva, N.; Paolisso, P.; Gallinoro, E.; Fabbricatore, D.; Munhoz, D.; Bergamaschi, L.; Belmonte, M.; Panayotov, P.; Pizzi, C.; Barbato, E.; et al. Diagnostic and Prognostic Role of Cardiac Magnetic Resonance in MINOCA. JACC Cardiovasc. Imaging 2023, 16, 376–389. [Google Scholar] [CrossRef] [PubMed]
- Taruya, A.; Tanaka, A.; Nishiguchi, T.; Ozaki, Y.; Kashiwagi, M.; Yamano, T.; Matsuo, Y.; Ino, Y.; Kitabata, H.; Takemoto, K.; et al. Lesion Characteristics and Prognosis of Acute Coronary Syndrome without Angiographically Significant Coronary Artery Stenosis. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Zhao, C.; Bao, X.; Liu, M.; He, L.; Xu, Y.; Meng, W.; Qin, Y.; Weng, Z.; Yi, B.; et al. Clinical Characteristics and Prognosis of MINOCA Caused by Atherosclerotic and Nonatherosclerotic Mechanisms Assessed by OCT. JACC Cardiovasc. Imaging 2023, 16, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Abdu, F.A.; Liu, L.; Mohammed, A.-Q.; Yin, G.; Xu, B.; Zhang, W.; Xu, S.; Lv, X.; Fan, R.; Feng, C.; et al. Prognostic Impact of Coronary Microvascular Dysfunction in Patients with Myocardial Infarction with Non-Obstructive Coronary Arteries. Eur. J. Intern. Med. 2021, 92, 79–85. [Google Scholar] [CrossRef]
- Bergamaschi, L.; Foà, A.; Paolisso, P.; Renzulli, M.; Angeli, F.; Fabrizio, M.; Bartoli, L.; Armillotta, M.; Sansonetti, A.; Amicone, S.; et al. Prognostic Role of Early Cardiac Magnetic Resonance in Myocardial Infarction with Nonobstructive Coronary Arteries. JACC Cardiovasc. Imaging 2023, in press. [Google Scholar] [CrossRef]
- Reynolds, H.R.; Maehara, A.; Kwong, R.Y.; Sedlak, T.; Saw, J.; Smilowitz, N.R.; Mahmud, E.; Wei, J.; Marzo, K.; Matsumura, M.; et al. Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction With Nonobstructive Coronary Arteries in Women. Circulation 2021, 143, 624–640, Epub 2020. Erratum in: Circulation. 2023, 147, e624. [Google Scholar] [CrossRef]
- Usui, E.; Matsumura, M.; Smilowitz, N.R.; Mintz, G.S.; Saw, J.; Kwong, R.Y.; Hada, M.; Mahmud, E.; Giesler, C.; Shah, B.; et al. Coronary morphological features in women with non-ST-segment elevation MINOCA and MI-CAD as assessed by optical coherence tomography. Eur. Heart J. Open. 2022, 2, oeac058. [Google Scholar] [CrossRef]
- Pasupathy, S.; Beltrame, J.F. Refining the Role of CMR Imaging in MINOCA. JACC Cardiovasc Imaging. 2021, 14, 1784–1786. [Google Scholar] [CrossRef]
- Borzillo, I.; De Filippo, O.; Manai, R.; Bruno, F.; Ravetti, E.; Galanti, A.A.; Vergallo, R.; Porto, I.; De Ferrari, G.M.; D’Ascenzo, F. Role of Intracoronary Imaging in Myocardial Infarction with Non-Obstructive Coronary Disease (MINOCA): A Review. J. Clin. Med. 2023, 12, 2129. [Google Scholar] [CrossRef]
- Fluder-Wlodarczyk, J.; Milewski, M.; Roleder-Dylewska, M.; Haberka, M.; Ochala, A.; Wojakowski, W.; Gasior, P. Underlying Causes of Myocardial Infarction with Nonobstructive Coronary Arteries: Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging Pilot Study. J. Clin. Med. 2022, 11, 7495. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SCORE | GRACE | TIMI NSTE-ACS | HEART | ACEF |
|---|---|---|---|---|
| Original tested outcome | In-hospital mortality [7] | 14-day mortality, recurrent AMI, or urgent revascularization [14] | Long-term mortality, AMI, PCI/CABG [19] | Peri-operative mortality in elective cardiac surgery [20] |
| Further tested outcomes | ||||
| ITEMS (in brackets the minimum and maximum scoring, or score if present) | ||||
| Age |
|
|
| Age/LVEF (+1 if creatinine >2 mg/dL) |
| Past medical history | - |
|
| |
| Vital signs |
| - | - | |
| Clinical presentation |
|
|
| |
| ECG |
|
|
| |
| Laboratory test |
|
|
| |
| RISK CLASS | ||||
| Low risk | <109 in NSTE-ACS <126 in STEMI | 0–2 | 0–3 | <1.0 in PCI in AMI [21] ≤1.45 in ACS [22] |
| Intermediate risk | 109–140 in NSTE-ACS 126–154 in STEMI | 3–4 | 4–6 | 1–1.39 in PCI in AMI [21] 1.451–2.0 in ACS [22] |
| High risk | >140 in NSTE-ACS >154 in STEMI | 5–7 | 7–10 | ≥1.4 in PCI in AMI [21] >2.0 in ACS [22] |
| Total N = 250 | MAE N = 19 | No MAE N = 231 | p-Value | |
|---|---|---|---|---|
| Age, years | 68 [53–78] | 78 [69–87] | 67 [53–77] | <0.001 |
| Female, n (%) | 163 (65.2) | 17 (89.5) | 146 (63.2) | 0.021 |
| BMI, kg/m2 | 25.7 [22.8–28.8] | 25.9 [23.7–28.1] | 25.6 [22.7–28.8] | 0.694 |
| Cardiovascular risk factors | ||||
| Current smoking, n (%) | 46 (18.4) | 1 (5.3) | 45 (19.5) | 0.214 |
| Hypertension, n (%) | 167 (66.8) | 17 (89.5) | 150 (64.9) | 0.029 |
| Dyslipidemia, n (%) | 162 (64.8) | 11 (57.9) | 151 (65.4) | 0.618 |
| Type-2 diabetes, n (%) | 26 (10.4) | 5 (26.3) | 21 (9.1) | 0.034 |
| Family history of CVD, n (%) | 45 (18.0) | 2 (10.5) | 43 (18.6) | 0.540 |
| Comorbidities | ||||
| Previous stroke, n (%) | 16 (6.4) | 3 (15.8) | 13 (5.6) | 0.111 |
| COPD, n (%) | 27 (10.8) | 5 (26.3) | 22 (9.5) | 0.040 |
| PAD, n (%) | 6 (2.4) | 0 (0) | 6 (2.6) | 0.477 |
| Clinical presentation | ||||
| Typical chest pain a, n (%) | 138 (55.2) | 7 (36.8) | 131 (56.7) | 0.148 |
| Killip ≥2, n (%) | 25 (10.0) | 5 (26.3) | 20 (8.7) | 0.029 |
| SBP, mmHg | 138 ± 27.3 | 122 ± 31.8 | 139 ± 26.4 | 0.008 |
| HR, bpm | 80 [69–98] | 90 [74–120] | 80 [68–96] | 0.089 |
| STEMI, n (%) | 28 (11.2) | 3 (15.8) | 25 (10.8) | 0.455 |
| AF, n (%) | 26 (10.4) | 6 (31.6) | 20 (8.7) | 0.008 |
| WBC, cell/nL | 8.6 [6.9–11.1] | 9.9 [7.4–13.1] | 8.5 [6.9–11.0] | 0.040 |
| Hb, g/dL | 13.4 ± 1.87 | 12.5 ± 1.84 | 13.5 ± 1.90 | 0.034 |
| Glucose, mg/dL | 107 [96–129] | 111 [100–158] | 107 [95–129] | 0.127 |
| Creatinine, mg/dL | 0.8 [0.7–1.0] | 0.9 [0.7–1.0] | 0.8 [0.7–1.0] | 0.750 |
| LDL cholesterol, mg/dL | 119 ± 37.4 | 104 ± 25.3 | 120 ± 37.3 | 0.093 |
| Troponin (1st sample), ng/L | 78 [40–330] | 132 [52–804] | 77 [40–327] | 0.149 |
| LVEF, % | 58 ± 8.9 | 58 ± 8.6 | 57 ± 11.7 | 0.999 |
| Risk scores | ||||
| GRACE | 128 [105–157] | 179 [132–204] | 126 [104–151] | <0.001 |
| TIMI NSTE-ACS | 2 [1–3] | 3 [2–4] | 2 [1–3] | 0.002 |
| HEART | 7 [5–7] | 7 [6–9] | 6 [5–7] | 0.020 |
| ACEF | 1.11 [0.90–1.34] | 1.26 [1.17–1.64] | 1.10 [0.90–1.33] | 0.010 |
| GRACE | TIMI NSTE-ACS | HEART | |
|---|---|---|---|
| GRACE | - | - | - |
| TIMI NSTE-ACS | 0.49 * | - | - |
| HEART | 0.42 * | 0.68 * | - |
| ACEF | 0.67 * | 0.46 * | 0.36 * |
| Sensitivity | Specificity | PPV | NPV | Accuracy | |
|---|---|---|---|---|---|
| GRACE > 171 | 68% | 89% | 34% | 97% | 88% |
| TIMI NSTE-ACS > 2 | 74% | 61% | 13% | 97% | 62% |
| HEART > 7 | 42% | 78% | 14% | 94% | 76% |
| ACEF > 1.16 | 79% | 57% | 13% | 97% | 58% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fedele, D.; Canton, L.; Bodega, F.; Suma, N.; Tattilo, F.P.; Impellizzeri, A.; Amicone, S.; Di Iuorio, O.; Ryabenko, K.; Armillotta, M.; et al. Performance of Prognostic Scoring Systems in MINOCA: A Comparison among GRACE, TIMI, HEART, and ACEF Scores. J. Clin. Med. 2023, 12, 5687. https://doi.org/10.3390/jcm12175687
Fedele D, Canton L, Bodega F, Suma N, Tattilo FP, Impellizzeri A, Amicone S, Di Iuorio O, Ryabenko K, Armillotta M, et al. Performance of Prognostic Scoring Systems in MINOCA: A Comparison among GRACE, TIMI, HEART, and ACEF Scores. Journal of Clinical Medicine. 2023; 12(17):5687. https://doi.org/10.3390/jcm12175687
Chicago/Turabian StyleFedele, Damiano, Lisa Canton, Francesca Bodega, Nicole Suma, Francesco Pio Tattilo, Andrea Impellizzeri, Sara Amicone, Ornella Di Iuorio, Khrystyna Ryabenko, Matteo Armillotta, and et al. 2023. "Performance of Prognostic Scoring Systems in MINOCA: A Comparison among GRACE, TIMI, HEART, and ACEF Scores" Journal of Clinical Medicine 12, no. 17: 5687. https://doi.org/10.3390/jcm12175687
APA StyleFedele, D., Canton, L., Bodega, F., Suma, N., Tattilo, F. P., Impellizzeri, A., Amicone, S., Di Iuorio, O., Ryabenko, K., Armillotta, M., Sansonetti, A., Stefanizzi, A., Cavallo, D., Casuso, M., Bertolini, D., Lovato, L., Gallinoro, E., Belmonte, M., Rinaldi, A., ... Pizzi, C. (2023). Performance of Prognostic Scoring Systems in MINOCA: A Comparison among GRACE, TIMI, HEART, and ACEF Scores. Journal of Clinical Medicine, 12(17), 5687. https://doi.org/10.3390/jcm12175687