Abstract
We explored global myocardial work index (GWI), a novel measure of myocardial function that integrates left ventricular (LV) hemodynamic load, in relation to sex and increased body mass index (BMI). We used data from 467 individuals (61% women, average age 47 ± 9 years and BMI 31.2 kg/m2) without known cardiac disease. Central arterial function was analysed by applanation tonometry. GWI was calculated from global longitudinal strain (GLS) and post-echocardiography supine blood pressure (BP). Covariables of GWI were identified in linear regression analyses. Women had higher BMI, aortic augmentation pressure (12 ± 7 vs. 8 ± 6 mmHg), LV GLS (20.0 ± 2.8 vs. 18.8 ± 2.8%), and GWI (2126 ± 385 vs. 2047 ± 389 mmHg%) than men (all p < 0.05). In univariable analyses, higher GWI was associated with female sex, higher age, systolic BP, LV wall stress, LV ejection fraction, left atrial size, LV ejection time, and with lower waist circumference (all p < 0.05). In multivariable analysis, adjusting for these correlates, female sex remained independently associated with higher GWI (β = 0.13, p = 0.007). After additional adjustment for aortic augmentation pressure or central pulse pressure, this association became non-significant. In conclusion, the higher GWI in women compared to men was mainly explained by increased LV workload due to higher aortic augmentation pressure in women.
1. Introduction
Obesity is a major risk factor for hypertension and strongly associated with development of organ damage like arterial stiffness, left ventricular (LV) hypertrophy, and left atrial dilatation, with higher prevalence rates among women [1,2,3]. Previous studies involving subjects with increased body mass index (BMI) have demonstrated that although LV systolic function measured by ejection fraction often is normal, LV myocardial function assessed by global longitudinal strain (GLS) is frequently reduced [4]. At the same time, women tend to have better GLS compared to men [5,6,7], consistent with higher LV ejection fraction and midwall shortening in women [8]. GLS is a robust marker of early LV systolic dysfunction [9], but it is negatively influenced by higher blood pressure (BP), central arterial stiffening, and backward wave reflections, reflecting its afterload dependency [10,11].
Recently, a novel method to quantify LV myocardial work by pressure-strain loops was introduced [12]. The method is based upon combining speckle tracking strain imaging and a non-invasive estimate of LV pressure. Myocardial work estimated by this method has been shown to be closely related to invasively estimated work and metabolism [12]. In the population-based Copenhagen City cohort study, LV myocardial work indices differed by sex and changed with age in a sex-dependent manner [13]. However, the sex differences were small, and abnormal myocardial work indices were particularly associated with cardiovascular risk factors, markers of increased afterload, and abnormal LV geometry [13]. In the Characteristics and Course of Heart Failure STAges A/B and Determinants of Progression cohort study, obesity was associated with lower and hypertension with higher global work index (GWI), and these associations were stronger in women [14]. However, none of these previous studies adjusted for the documented sex differences in arterial function [15,16], which may contribute significantly to LV load. Thus, the aim of the present study was to assess the impact of central aortic function on LV myocardial work indices in middle-aged women and men with increased BMI.
2. Materials and Methods
2.1. Study Population
The present analysis is a substudy of the cross-sectional FAT-associated CardiOvasculaR dysfunction (FATCOR) study that was conducted in Bergen, Norway, from 2009 to 2017 as a collaboration between the Department of Heart Disease, Haukeland University Hospital, and a general practitioner center that focuses on management of obesity. Details regarding the study protocol have been published [17]. Briefly, a total of 620 women and men between 30 and 65 years with a BMI greater than 27 kg/m2 were included. Exclusion criteria were previous cardiovascular disease, gastrointestinal disorders, severe psychiatric illness, or inability to understand Norwegian language. For the present study, we included 595 participants with echocardiograms taken using a GE Vivid E9 machine (GE Vingmed Ultrasound, Horten, Norway). Among these participants, 2 withdraw consent, 2 were excluded due to missing BP measurements, 51 due to incomplete echocardiographic data, 49 due to inadequate echocardiographic image quality for strain analysis, and 24 due to missing segmental strain values in ≥2 LV segments. This resulted in a total of 467 (78%) participants eligible for the present analysis.
2.2. Cardiovascular Risk Factor Assessment
All participants underwent a standardized clinical examination at the general practitioner center. Additionally, participants completed a standardized questionnaire on self-reported health, including use of any medication. The provided information was quality assured by a study nurse. Waist circumference was measured using a nonflexible measuring tape as recommended by the World Health Organization. BMI was calculated from weight in kilograms divided by the square of body height in meters (kg/m2). Obesity was defined as a BMI ≥ 30.0 kg/m2.
BP was measured using an Omron M4 sphygmomanometer (Omron Healthcare Co. Ltd., Hoofddorp, The Netherlands) with an appropriately sized cuff. BP was measured in triplicates with 1 min intervals after 5 min of initial rest in the seated position [18]. Clinic BP was calculated as the average of the last two BP measurements. BP was also measured at completion of the echocardiographic examination, with the participant supine on the examination table with dimmed lights. Ambulatory 24-hour BP was recorded using a Diasys Integra II apparatus (Novacor, Cedex, France) on the non-dominant arm. Measurements were performed every 20 min during daytime and every 30 min at night. Hypertension was defined as use of antihypertensive medication or an elevated 24-hour ambulatory BP (≥130 mmHg systolic or ≥80 mmHg diastolic) in the individual participant.
A standardized 2-hour oral glucose tolerance test was performed in all participants without known diabetes mellitus (DM). DM was defined as a previous history of diabetes, glycated haemoglobin A1c (HbA1c) ≥ 6.5%, fasting plasma glucose ≥ 7 mmol/L, or a 2-hour plasma glucose ≥ 11.1 mmol/L during an oral glucose tolerance test.
2.3. Central Arterial Stiffness and Pulse Wave Analysis
Central arterial stiffness and aortic hemodynamic parameters were assessed by applanation tonometry using a SphygmoCor apparatus (AtCor Medical, Sydney, Australia). Carotid-femoral pulse wave velocity (PWV) was calculated as previously reported [17]. Central aortic parameters, including central pulse pressure (cPP), augmentation pressure (AP), and augmentation index (AIx), were derived from pulse wave analysis of the right carotid artery pressure waveform. AP was defined as the difference between the second and first systolic pressure peaks of the central pressure waveform. AIx was calculated as AP/cPP and expressed as a percentage.
2.4. Conventional Echocardiography
Transthoracic two-dimensional echocardiography was performed following a standardized protocol in all participants. Echocardiographic images were analysed off-line in the Echocardiography Core Laboratory at the University of Bergen, Norway, using Tomtec Image Arena Software version 4.6 (Tomtec Imaging Systems GmbH, Unterschleissheim, Germany).
Quantitative echocardiography was assessed following joint guidelines from the American Society of Echocardiography and the European Association of Cardiovascular Imaging [8]. LV hypertrophy was defined as LV mass index > 47.0 g/m2.7 in women and >50.0 g/m2.7 in men, respectively [18,19]. Left atrial volumes and left ventricular ejection fraction were assessed by the biplane Simpson’s method. Stroke volume was calculated by the Doppler method. Left atrial volume was indexed for height2 and stroke volume was indexed to height at the allometric power of 2.04 [20]. Meridional LV wall stress was estimated using a validated equation [21]. Systolic ejection time was measured as the time interval in milliseconds from aortic valve opening to closure [22].
2.5. Myocardial Work Analysis
Two-dimensional speckle tracking analysis was performed offline on a dedicated workstation equipped with EchoPac BT 202 (GE Vingmed Ultrasound, Horten, Norway). Apical two-, three-, and four-chamber views with an optimized frame rate were analysed using the Automated Function Imaging application. GLS was calculated as the average peak systolic negative longitudinal shortening of the 18 LV segments. Since GLS is expressed as a negative percentage, we report the absolute values |x| for a simpler interpretation. Timing of mitral and aortic valve opening and closure were determined using pulsed-wave Doppler signals. The supine brachial BP measured at the end of the echocardiographic examination was used in the calculation of LV myocardial work. By synchronizing longitudinal strain, BP, and timing of valvular events, non-invasive pressure-strain loops (PSL) were provided (Figure 1). The area within the PSL corresponds to a global myocardial work index (GWI), calculated from mitral valve closure to mitral valve opening. In addition, other indices of myocardial work such as global constructive work (GCW, the work performed during LV shortening in systole and LV lengthening during isovolumic relaxation), global wasted work (GWW, myocardial work not contributing to LV ejection due to lengthening in systole and LV shortening during isovolumic relaxation), and global work efficiency (GWE, constructive work divided by the sum of constructive and wasted work) were calculated [23].
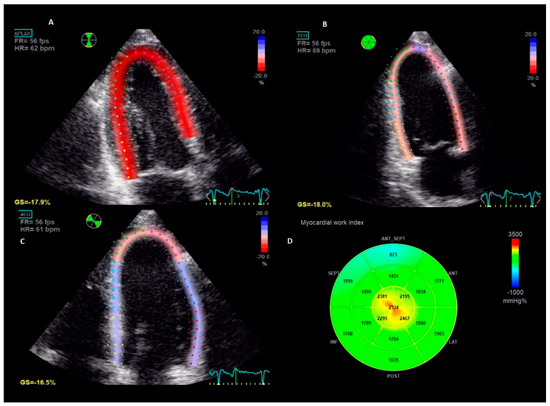
Figure 1.
Measurement of myocardial work in an individual patient. The figure represents the longitudinal strain imaging from the standard apical-three-chamber (Panel (A)), two-chamber (Panel (B)) and four-chamber (Panel (C)) views and the corresponding bull`s eye of global work index calculated from the area within the pressure-strain loop (Panel (D)).
2.6. Statistical Analysis
Data management and statistical analyses were performed using IBM SPSS version 26 (IBM Corporation, Armonk, NY, USA) and R version 1.2.5042 (R Foundation for Statistical Computing, Vienna, Austria) with the package “cocor”. The study population was grouped by sex. Data are presented as mean ± standard deviation for normally distributed variables, median with interquartile range (25–75 percentile) for non-normally distributed variables, and as percentages for categorical variables. Group comparisons were performed using Student’s t-test for continuous variables, Mann–Whitney U test for non-normally distributed variables, and Pearson’s chi-square test for categorial variables. For continuous variables, normality was checked by Q-Q plots and visual assessment of histograms prior to analyses. Homogeneity of variance was assessed using Levene’s test. The Spearman’s rank-order correlation (ρ) was used to assess univariable associations between GWI and covariables. The Spearman correlation coefficients between GWI and clinic systolic and central systolic BP, respectively, were normalized by Fisher’s z-transformation and compared by z-statistics. Multivariable linear regression analyses with collinearity tools were used to identify independent covariables of GWI. The multivariable models were constructed as follows: In Model 1, we included all correlates among clinic and echocardiographic variables with a p value < 0.1 in univariable analyses using a stepwise procedure. In Model 2, we added AP, the central aortic variable that had the highest correlation coefficient with GWI and was statistically different between sexes. In a subsequent model, AP was replaced by cPP. The AP is known to be significantly influenced by body height, sex, and heart rate. The relative importance of these covariables to GWI was determined with analysis of variance (ANOVA) using the F statistics and the Akaike information criterion (AIC). In sex specific analyses, significant univariable correlations by sex were added to a primary multivariable model by a similar procedure as mentioned above. Secondary multivariable models for each central aortic parameter, adjusted for otherwise significant correlates of GWI by sex, were constructed using an enter procedure. Results are presented as standardized β coefficients and p values. Interobserver reproducibility for GLS was calculated by intraclass correlation coefficient after reanalysis of 26 randomly selected participants. A two tailed p value < 0.05 was considered statistically significant in all analyses.
3. Results
3.1. Patient Characteristics
The present analysis included a total of 467 participants from the FATCOR study (61% women). The average age was 47 ± 9 years, and the median BMI was 31.2 (28.9–33.8) kg/m2. Women had higher BMI, AP, and AIx, but lower waist circumference, clinic and 24-hour systolic BP and PWV, and lower prevalence of hypertension (all p < 0.05) (Table 1). cPP and the prevalence of obesity and diabetes did not differ between sexes (Table 1).

Table 1.
Characteristics of the total study population and groups of women and men.
3.2. Echocardiographic Findings
LV hypertrophy and LV ejection fraction did not differ between sexes, while GLS was higher in women (p < 0.001) (Table 2) (Figure 2). Among measures of myocardial work, GWI was higher in women (p = 0.031), while GCW, GWW, and GWE did not differ between sexes. Interobserver reproducibility for GLS was excellent, with an intraclass correlation coefficient of 0.96 (95% CI, 0.95–0.98).
Table 2.
Echocardiographic findings in the total study population and in groups of women and men.
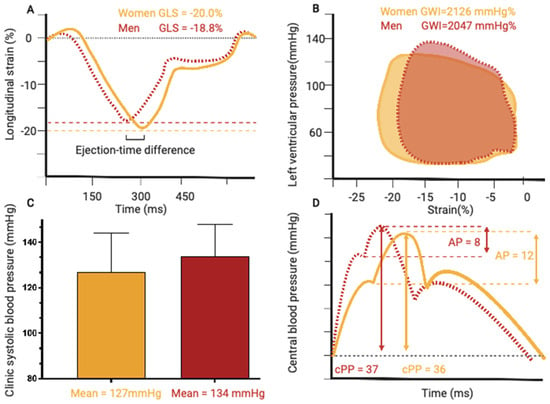
Figure 2.
Graphical representation of mean differences between women and men in; (A) global longitudinal strain, (B) clinic systolic blood pressure, (C) pressure-strain loops and global work index, (D) central arterial waveforms.
3.3. Covariables of Global Work Index
The univariable correlates with GWI are listed in Table 3. In univariable analysis, GWI showed a strong correlation with clinic systolic BP (ρ = 0.29, p-value < 0.001), post-echocardiography systolic BP (ρ = 0.51, p-value < 0.001), and central systolic BP (ρ = 0.37, p-value < 0.001). In Z-statistics, central systolic BP had a borderline stronger correlation with GWI than clinic systolic BP (z = −1.98, p value = 0.047). Due to collinearity between the supine post-echocardiography systolic BP and GWI, and between clinic and central systolic BP, only clinic systolic BP was included in the multivariable regression models to avoid collinearity and overfitting of the regression model. In multivariable analysis, including all significant univariable variables, except central aortic parameters, female sex was independently associated with higher GWI (Table 3, Model 1). When adding AP to the model, higher AP was significantly associated with higher GWI (β = 0.12, p = 0.024) while the association between GWI and female sex became non-significant (Table 3, Model 2). Due to collinearity, AP and cPP were not included in the same model. When AP was replaced by cPP, higher cPP was associated with higher GWI (β = 0.19, p < 0.001), and female sex remained non-significant. The relative contributions to GWI of known clinical correlates of AP are presented in Supplemental Material Figure S1. This analysis revealed that GWI was predominantly determined by AP, while variables known to influence AP, such as height, sex, and heart rate, had little impact. Substituting AP with cPP in the model gave similar results.
Table 3.
Univariable Spearman correlations and multivariable linear regression analyses of covariables of GWI.
3.4. Sex-Specific Analyses
Higher GWI was associated with increased arterial stiffness in both sexes in univariable analyses (Table 4). The correlation between GWI and LV ejection time was significant only in women (ρ = 0.28, p < 0.01 vs. ρ = 0.13, p = 0.08 in men). In the primary multivariable analysis, GWI correlated with higher systolic BP, wall stress, LV ejection fraction, left atrial volume index, and LV systolic ejection time in women (all p < 0.01). Among men, higher GWI correlated with lower waist circumference, higher systolic BP, wall stress, ejection fraction, and left atrial volume index (all p < 0.011). In a series of secondary sex-specific models, each including one central aortic parameter and adjusting for the covariables identified in the primary model, cPP remained the most important covariable of increased GWI in both sexes (Table 4). AP remained significantly associated with higher GWI in women, but not in men (Table 4). There were no significant associations between higher GWI and AIx or PWV in either sex.
Table 4.
Sex-specific univariable Spearman correlations and multivariable linear regression analyses of the association of individual measures of arterial wave reflection and stiffness with GWI.
4. Discussion
The present study provides new insight into the interaction of central aortic function with LV myocardial work in women and men with increased BMI. Our findings suggest that higher GWI among women with increased BMI may reflect a higher arterial load. Importantly, the association between AP and GWI was independent of heart rate and body height, factors which are known to differ between sexes and to significantly influence AP [24]. Despite a lower PWV in women, AP was higher and cPP comparable between sexes. This is in concordance with a previous study showing that cPP is mainly determined by wave reflections in the proximal aorta [25]. Among individuals younger than 50 years, as in the present study cohort, AIx, similar to AP, is a more sensitive marker of arterial aging and risk [16].
It should be noted that cPP is also influenced by LV ejection time [26]. A longer ejection time implies a lower volume ejected at the time of the first peak of the pressure waveform, which is a major component of the cPP [26]. We observed that women had a significantly longer LV ejection time compared to men, in line with previous reports [27,28]. Longer ejection time also correlated with a higher GWI, and more strongly in women compared to men. Arterial stiffness may contribute to a prolonged ejection because early wave reflections may independently increase the duration of systole [29]. The Framingham Heart Study reported that the longer ejection time in women compared to men could partly account for the observed sex differences in AP [30]. However, in the present study, the associations between LV ejection time, AP, and GWI were relatively independent of each other.
Previous results from the FATCOR study showed that women have higher prevalence of LV atrial dilation, which was associated with higher brachial PP [1]. In the Framingham Heart Study, the more pronounced increase in PP with aging in women was strongly associated with proximal aortic stiffening [31]. The interplay between higher PP, higher LV systolic function, and more subclinical cardiac disease in women could be reflected by a higher GWI, as a measure of increased LV metabolic demand [12]. Peterson et al. showed in a study combining echocardiography and positron emission tomography that women with obesity had significantly higher cardiac work, better LV systolic function, and increased myocardial oxygen consumption compared to men with obesity [32]. As demonstrated by the present study, sex differences in central arterial function may contribute to the higher GWI in women, adding to previous studies assessing clinic BP and obesity [13,14]. Furthermore, wave reflections during mid-to-late systole, as represented by AP, increase peak myocardial wall stress which is a primary determinant of myocardial oxygen consumption [11], and also an independent covariate of higher GWI in the present study.
In line with previous findings, GWI was strongly associated with higher systolic BP [14,33]. However, the correlation between GWI and clinic systolic BP in the present study was weaker compared to findings from the NORRE Study [33]. The differential findings may be related to that NORRE used clinic BP for calculation of GWI, while the supine post-echocardiography BP was used in the present study, in line with the original concept [23]. Even so, with higher systolic BP, the LV shifts to a higher energy level by an increase in inotropy to counteract the higher afterload during contraction [34].
Study Limitations
The present study has some limitations. Firstly, due to the cross-sectional study design, cause–effect relationships could not be explored. Use of antihypertensive treatment was not associated with higher GWI in multivariable analysis, probably reflecting that a large proportion of the patients were diagnosed with de-novo hypertension during the study based on 24 h BP recording. The cross-sectional study design precludes analysis of antihypertensive drug treatment effects on GWI. Furthermore, the impact of sex differences in longitudinal changes BP and arterial stiffness over the life course on LV myocardial work could not be assessed [35,36]. The trajectory of arterial stiffness progression during midlife is accentuated by menopause transition among women. However, our data collection did not include measurement of follicle-stimulating hormone levels or information regarding the time since last menstruation. We were therefore unable to assess the influence of menopause and subsequent accelerated arterial aging on our findings. However, patients’ age was included in the multivariable models. It should be noted that our cohort was middle-aged individuals with increased BMI, but without known cardiac disease. Since we did not include normal weight individuals, it remains to be demonstrated whether our results are valid also when BMI is normal. Lastly, echocardiographic evaluations of GLS and GWI could be affected by suboptimal image quality and orientation, although we carefully excluded participants with insufficient image quality.
5. Conclusions
Women with increased BMI have higher GWI compared to men. In the present cohort, the sex difference in GWI was mainly explained by higher AP in women.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm12175676/s1, Figure S1: The relative importance of AP, body height, heart rate and sex for GWI by the Akaike information criterion.
Author Contributions
Conceptualization, E.E. and E.G.; data curation, K.T.L. and E.E.; formal analysis, K.T.L., E.E. and E.G.; methodology, K.T.L., E.E., N.P. and E.G.; project administration, E.G.; supervision, E.E., H.M. and E.G.; visualization, E.E.; writing—original draft, K.T.L.; writing—review and editing, K.T.L., E.G., H.M., N.P., D.C. and E.E. All authors have read and agreed to the published version of the manuscript.
Funding
The FATCOR study was funded by a grant from the Western Norwegian Regional Health Authorities (Grant number 911402).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Regional Ethics Committee of Western Norway (REK Vest), approval number 17173, initial approval date 13 November 2008.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are not available due to ethical restrictions.
Acknowledgments
The authors thank Liv Himle, Hilde Jacobsen, Marina V. Kokorina, Britt Gjellefall, and Synnøve Ygre Hauge for technical assistance with data collection, registration, and participant management.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Halland, H.; Lonnebakken, M.T.; Pristaj, N.; Saeed, S.; Midtbo, H.; Einarsen, E.; Gerdts, E. Sex differences in subclinical cardiac disease in overweight and obesity (the FATCOR study). Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1054–1060. [Google Scholar] [CrossRef]
- Herfindal, B.; Gerdts, E.; Kringeland, E.A.; Saeed, S.; Midtbo, H.; Halland, H. Concomitant hypertension is associated with abnormal left ventricular geometry and lower systolic myocardial function in overweight participants: The FAT associated CardiOvasculaR dysfunction study. J. Hypertens. 2020, 38, 1158–1164. [Google Scholar] [CrossRef]
- Lu, Y.; Pechlaner, R.; Cai, J.; Yuan, H.; Huang, Z.; Yang, G.; Wang, J.; Chen, Z.; Kiechl, S.; Xu, Q. Trajectories of Age-Related Arterial Stiffness in Chinese Men and Women. J. Am. Coll. Cardiol. 2020, 75, 870–880. [Google Scholar] [CrossRef]
- Tadic, M.; Cuspidi, C.; Majstorovic, A.; Pencic, B.; Backovic, S.; Ivanovic, B.; Scepanovic, R.; Martinov, J.; Kocijancic, V.; Celic, V. Does the metabolic syndrome impact left-ventricular mechanics? A two-dimensional speckle tracking study. J. Hypertens. 2014, 32, 1870–1878. [Google Scholar] [CrossRef]
- Pristaj, N.; Saeed, S.; Midtbo, H.; Halland, H.; Matre, K.; Gerdts, E. Covariables of Myocardial Function in Women and Men with Increased Body Mass Index. High. Blood Press. Cardiovasc. Prev. 2020, 27, 579–586. [Google Scholar] [CrossRef]
- Dalen, H.; Thorstensen, A.; Aase, S.A.; Ingul, C.B.; Torp, H.; Vatten, L.J.; Stoylen, A. Segmental and global longitudinal strain and strain rate based on echocardiography of 1266 healthy individuals: The HUNT study in Norway. Eur. J. Echocardiogr. 2010, 11, 176–183. [Google Scholar] [CrossRef]
- Sugimoto, T.; Dulgheru, R.; Bernard, A.; Ilardi, F.; Contu, L.; Addetia, K.; Caballero, L.; Akhaladze, N.; Athanassopoulos, G.D.; Barone, D.; et al. Echocardiographic reference ranges for normal left ventricular 2D strain: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 833–840. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Biering-Sorensen, T.; Biering-Sorensen, S.R.; Olsen, F.J.; Sengelov, M.; Jorgensen, P.G.; Mogelvang, R.; Shah, A.M.; Jensen, J.S. Global Longitudinal Strain by Echocardiography Predicts Long-Term Risk of Cardiovascular Morbidity and Mortality in a Low-Risk General Population: The Copenhagen City Heart Study. Circ. Cardiovasc. Imaging 2017, 10, e005521. [Google Scholar] [CrossRef]
- Donal, E.; Bergerot, C.; Thibault, H.; Ernande, L.; Loufoua, J.; Augeul, L.; Ovize, M.; Derumeaux, G. Influence of afterload on left ventricular radial and longitudinal systolic functions: A two-dimensional strain imaging study. Eur. J. Echocardiogr. 2009, 10, 914–921. [Google Scholar] [CrossRef]
- Chirinos, J.A.; Segers, P.; Hughes, T.; Townsend, R. Large-Artery Stiffness in Health and Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 1237–1263. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: A non-invasive index of myocardial work. Eur. Heart J. 2012, 33, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Olsen, F.J.; Skaarup, K.G.; Lassen, M.C.H.; Johansen, N.D.; Sengelov, M.; Jensen, G.B.; Schnohr, P.; Marott, J.L.; Sogaard, P.; Gislason, G.; et al. Normal Values for Myocardial Work Indices Derived From Pressure-Strain Loop Analyses: From the CCHS. Circ. Cardiovasc. Imaging 2022, 15, e013712. [Google Scholar] [CrossRef]
- Sahiti, F.; Morbach, C.; Cejka, V.; Tiffe, T.; Wagner, M.; Eichner, F.A.; Gelbrich, G.; Heuschmann, P.U.; Stork, S. Impact of cardiovascular risk factors on myocardial work-insights from the STAAB cohort study. J. Hum. Hypertens. 2022, 36, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Zuo, J.; Chao, H.; Tang, B.; Avolio, A.P.; Schlaich, M.P.; Nolde, J.M.; Adji, A.; Carnagarin, R. Female Gender Is Associated with Higher Susceptibility of Weight Induced Arterial Stiffening and Rise in Blood Pressure. J. Clin. Med. 2021, 10, 3479. [Google Scholar] [CrossRef] [PubMed]
- McEniery, C.M.; Yasmin; Hall, I.R.; Qasem, A.; Wilkinson, I.B.; Cockcroft, J.R.; ACCT Investigators. Normal vascular aging: Differential effects on wave reflection and aortic pulse wave velocity: The Anglo-Cardiff Collaborative Trial (ACCT). J. Am. Coll. Cardiol. 2005, 46, 1753–1760. [Google Scholar] [CrossRef]
- Halland, H.; Lonnebakken, M.T.; Saeed, S.; Midtbo, H.; Cramariuc, D.; Gerdts, E. Does fitness improve the cardiovascular risk profile in obese subjects? Nutr. Metab. Cardiovasc. Dis. 2017, 27, 518–524. [Google Scholar] [CrossRef][Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Gerdts, E.; Izzo, R.; Mancusi, C.; Losi, M.A.; Manzi, M.V.; Canciello, G.; De Luca, N.; Trimarco, B.; de Simone, G. Left ventricular hypertrophy offsets the sex difference in cardiovascular risk (the Campania Salute Network). Int. J. Cardiol. 2018, 258, 257–261. [Google Scholar] [CrossRef]
- de Simone, G.; Devereux, R.B.; Daniels, S.R.; Mureddu, G.; Roman, M.J.; Kimball, T.R.; Greco, R.; Witt, S.; Contaldo, F. Stroke volume and cardiac output in normotensive children and adults. Assessment of relations with body size and impact of overweight. Circulation 1997, 95, 1837–1843. [Google Scholar] [CrossRef]
- de Simone, G.; Devereux, R.B.; Roman, M.J.; Ganau, A.; Saba, P.S.; Alderman, M.H.; Laragh, J.H. Assessment of left ventricular function by the midwall fractional shortening/end-systolic stress relation in human hypertension. J. Am. Coll. Cardiol. 1994, 23, 1444–1451. [Google Scholar] [CrossRef] [PubMed]
- Einarsen, E.; Cramariuc, D.; Bahlmann, E.; Midtbo, H.; Chambers, J.B.; Gerdts, E. Higher Acceleration/Ejection Time Ratio Predicts Impaired Outcome in Aortic Valve Stenosis. Circ. Cardiovasc. Imaging 2021, 14, e011467. [Google Scholar] [CrossRef]
- Smiseth, O.A.; Donal, E.; Penicka, M.; Sletten, O.J. How to measure left ventricular myocardial work by pressure-strain loops. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 259–261. [Google Scholar] [CrossRef]
- Janner, J.H.; Godtfredsen, N.S.; Ladelund, S.; Vestbo, J.; Prescott, E. Aortic augmentation index: Reference values in a large unselected population by means of the SphygmoCor device. Am. J. Hypertens. 2010, 23, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Cecelja, M.; Jiang, B.; McNeill, K.; Kato, B.; Ritter, J.; Spector, T.; Chowienczyk, P. Increased wave reflection rather than central arterial stiffness is the main determinant of raised pulse pressure in women and relates to mismatch in arterial dimensions: A twin study. J. Am. Coll. Cardiol. 2009, 54, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jiang, B.; Keehn, L.; Gu, H.; Boguslavskyi, A.; Cecelja, M.; Vennin, S.; Spector, T.; Alastruey, J.; Chowienczyk, P. Hemodynamic Mechanism of the Age-Related Increase in Pulse Pressure in Women. Hypertension 2019, 73, 1018–1024. [Google Scholar] [CrossRef]
- Wang, K.L.; Cheng, H.M.; Sung, S.H.; Chuang, S.Y.; Li, C.H.; Spurgeon, H.A.; Ting, C.T.; Najjar, S.S.; Lakatta, E.G.; Yin, F.C.; et al. Wave reflection and arterial stiffness in the prediction of 15-year all-cause and cardiovascular mortalities: A community-based study. Hypertension 2010, 55, 799–805. [Google Scholar] [CrossRef]
- Gatzka, C.D.; Kingwell, B.A.; Cameron, J.D.; Berry, K.L.; Liang, Y.L.; Dewar, E.M.; Reid, C.M.; Jennings, G.L.; Dart, A.M.; ANBO2 Investigators. Gender differences in the timing of arterial wave reflection beyond differences in body height. J. Hypertens. 2001, 19, 2197–2203. [Google Scholar] [CrossRef]
- Weber, T.; Auer, J.; O’Rourke, M.F.; Punzengruber, C.; Kvas, E.; Eber, B. Prolonged mechanical systole and increased arterial wave reflections in diastolic dysfunction. Heart 2006, 92, 1616–1622. [Google Scholar] [CrossRef]
- Torjesen, A.A.; Wang, N.; Larson, M.G.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J.; Vasan, R.S.; Mitchell, G.F. Forward and backward wave morphology and central pressure augmentation in men and women in the Framingham Heart Study. Hypertension 2014, 64, 259–265. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Rong, J.; Larson, M.G.; Cooper, L.L.; Xanthakis, V.; Benjamin, E.J.; Hamburg, N.M.; Vasan, R.S. Longitudinal Hemodynamic Correlates of and Sex Differences in the Evolution of Blood Pressure Across the Adult Lifespan: The Framingham Heart Study. J. Am. Heart Assoc. 2023, 12, e027329. [Google Scholar] [CrossRef] [PubMed]
- Peterson, L.R.; Soto, P.F.; Herrero, P.; Mohammed, B.S.; Avidan, M.S.; Schechtman, K.B.; Dence, C.; Gropler, R.J. Impact of gender on the myocardial metabolic response to obesity. JACC Cardiovasc. Imaging 2008, 1, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Manganaro, R.; Marchetta, S.; Dulgheru, R.; Ilardi, F.; Sugimoto, T.; Robinet, S.; Cimino, S.; Go, Y.Y.; Bernard, A.; Kacharava, G.; et al. Echocardiographic reference ranges for normal non-invasive myocardial work indices: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Kuznetsova, T.; D’Hooge, J.; Kloch-Badelek, M.; Sakiewicz, W.; Thijs, L.; Staessen, J.A. Impact of hypertension on ventricular-arterial coupling and regional myocardial work at rest and during isometric exercise. J. Am. Soc. Echocardiogr. 2012, 25, 882–890. [Google Scholar] [CrossRef]
- Ji, H.; Kim, A.; Ebinger, J.E.; Niiranen, T.J.; Claggett, B.L.; Bairey Merz, C.N.; Cheng, S. Sex Differences in Blood Pressure Trajectories Over the Life Course. JAMA Cardiol. 2020, 5, 19–26. [Google Scholar] [CrossRef]
- Campos-Arias, D.; De Buyzere, M.L.; Chirinos, J.A.; Rietzschel, E.R.; Segers, P. Longitudinal Changes of Input Impedance, Pulse Wave Velocity, and Wave Reflection in a Middle-Aged Population: The Asklepios Study. Hypertension 2021, 77, 1154–1165. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).