
Are We Focused on the Wrong Early Postoperative Quality Metrics? Optimal Realignment Outweighs Perioperative Risk in Adult Spinal Deformity Surgery

 ,
,  , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Inclusion Criteria
2.2. Data Collection
2.3. Radiographic Data Collection
2.4. Clinical Outcomes
2.5. Complication Assessment
2.6. Definition of Optimal Radiographic Criteria
2.7. Propensity Score Matching
2.8. Cost Calculation
2.9. Utility Calculation
2.10. Statistical Analysis
3. Result
3.1. Patient Demographics
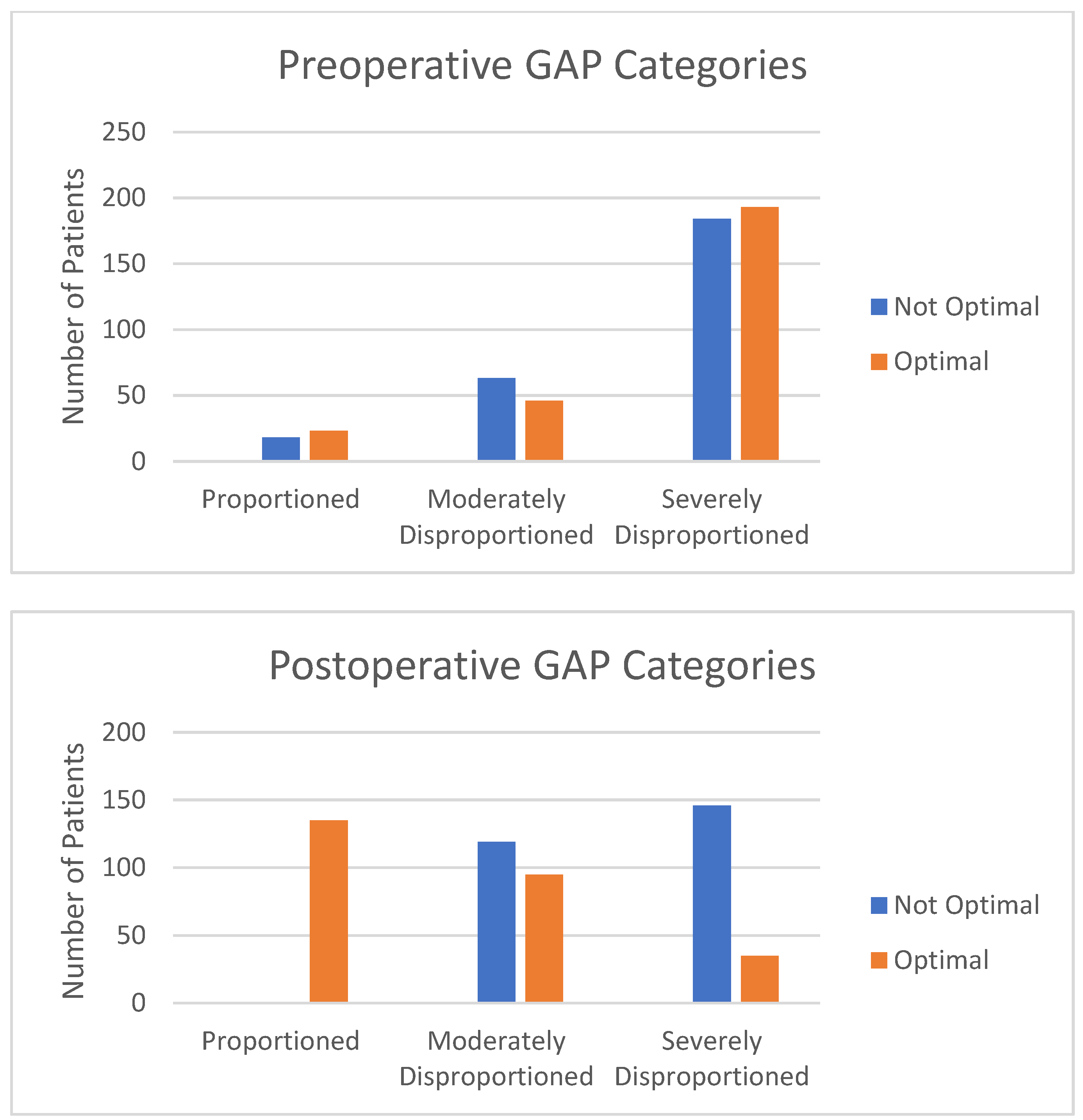
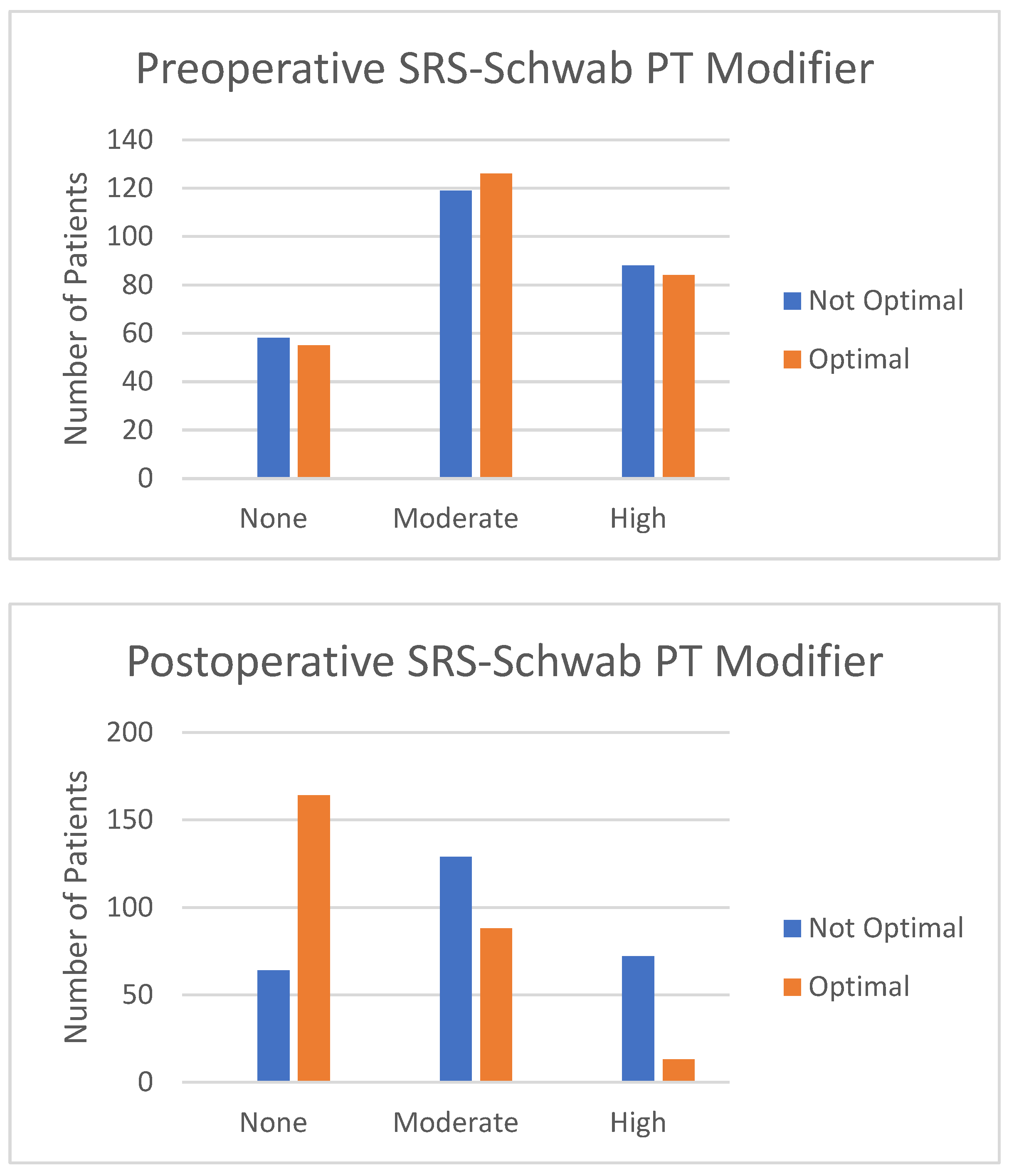
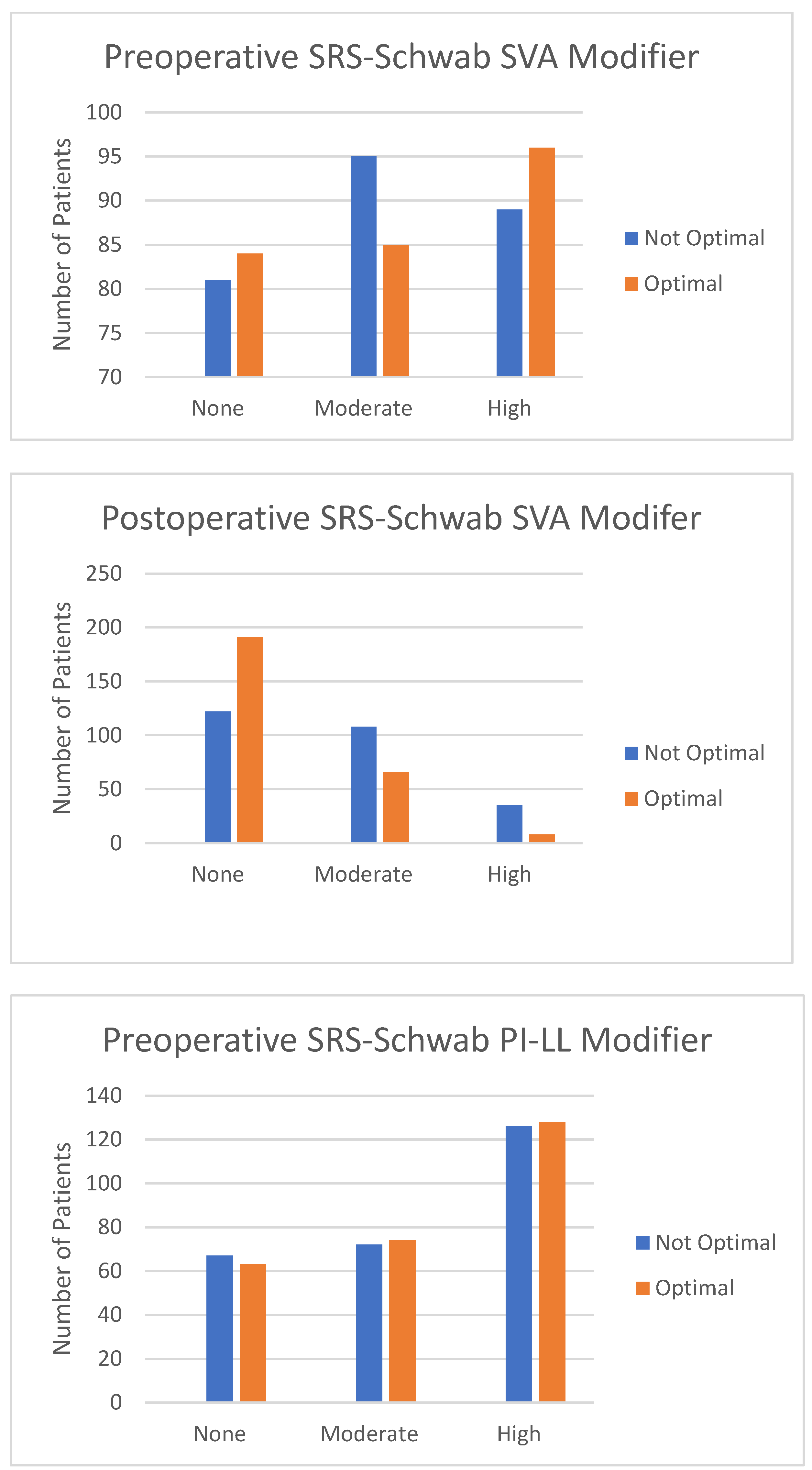
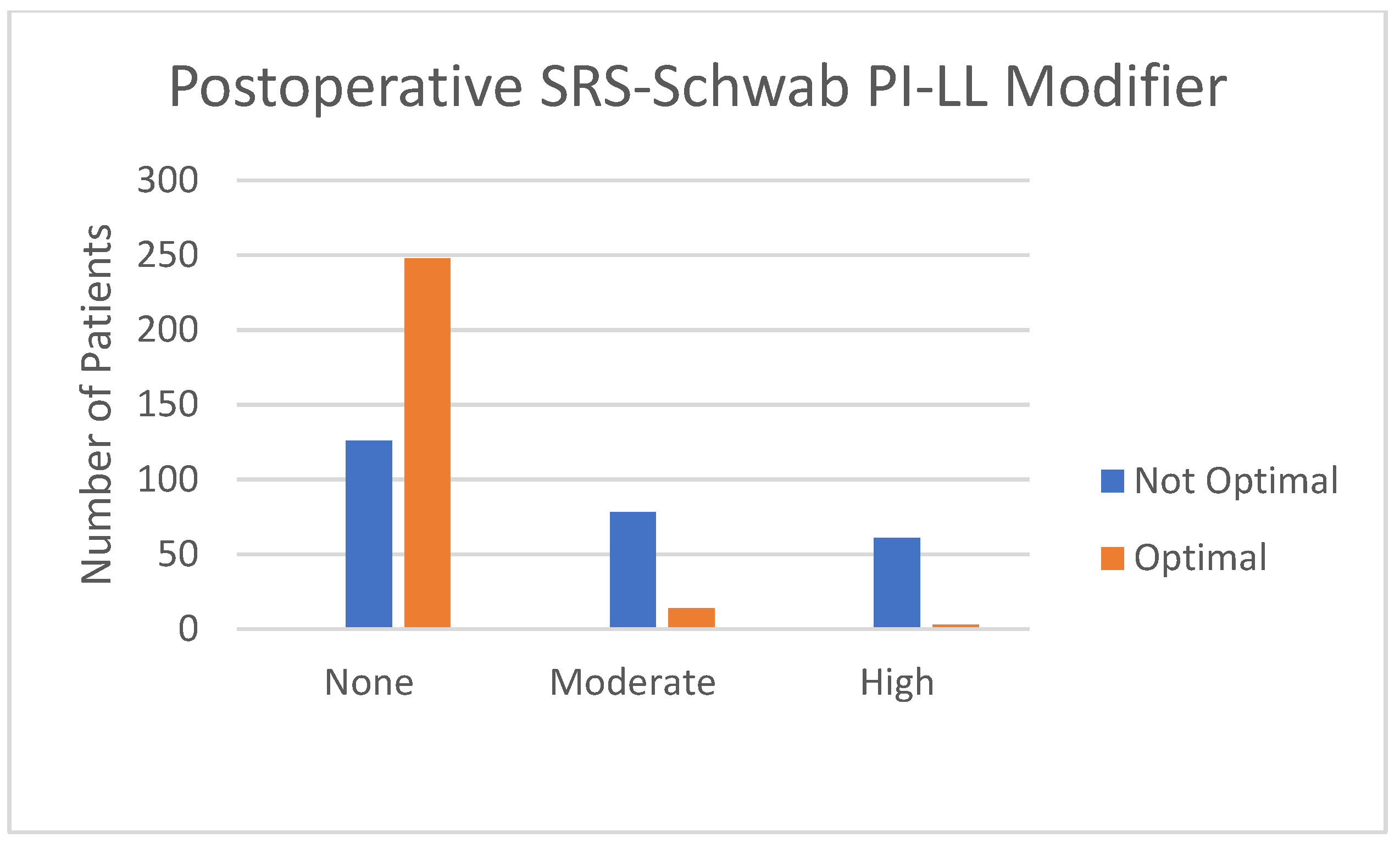
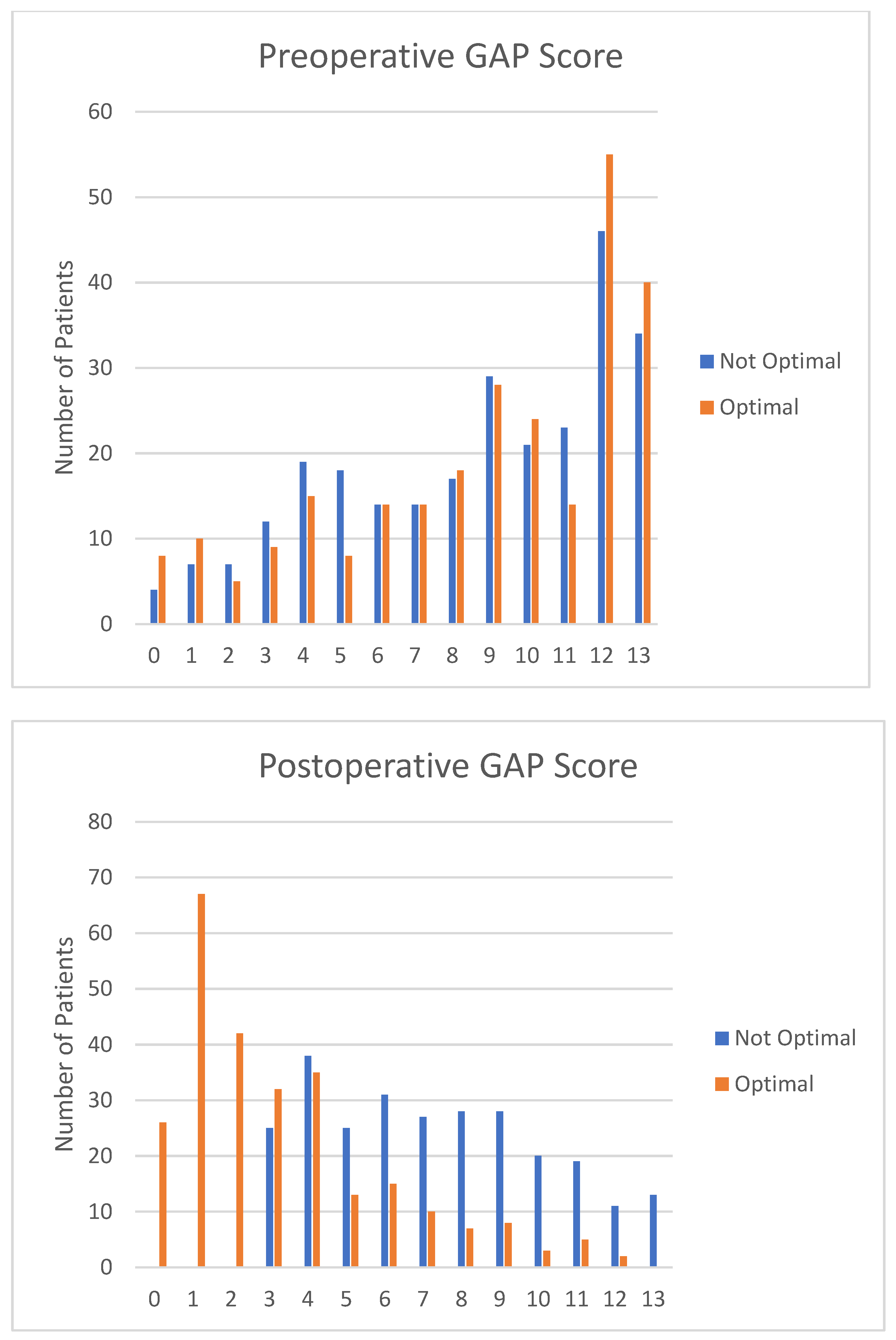
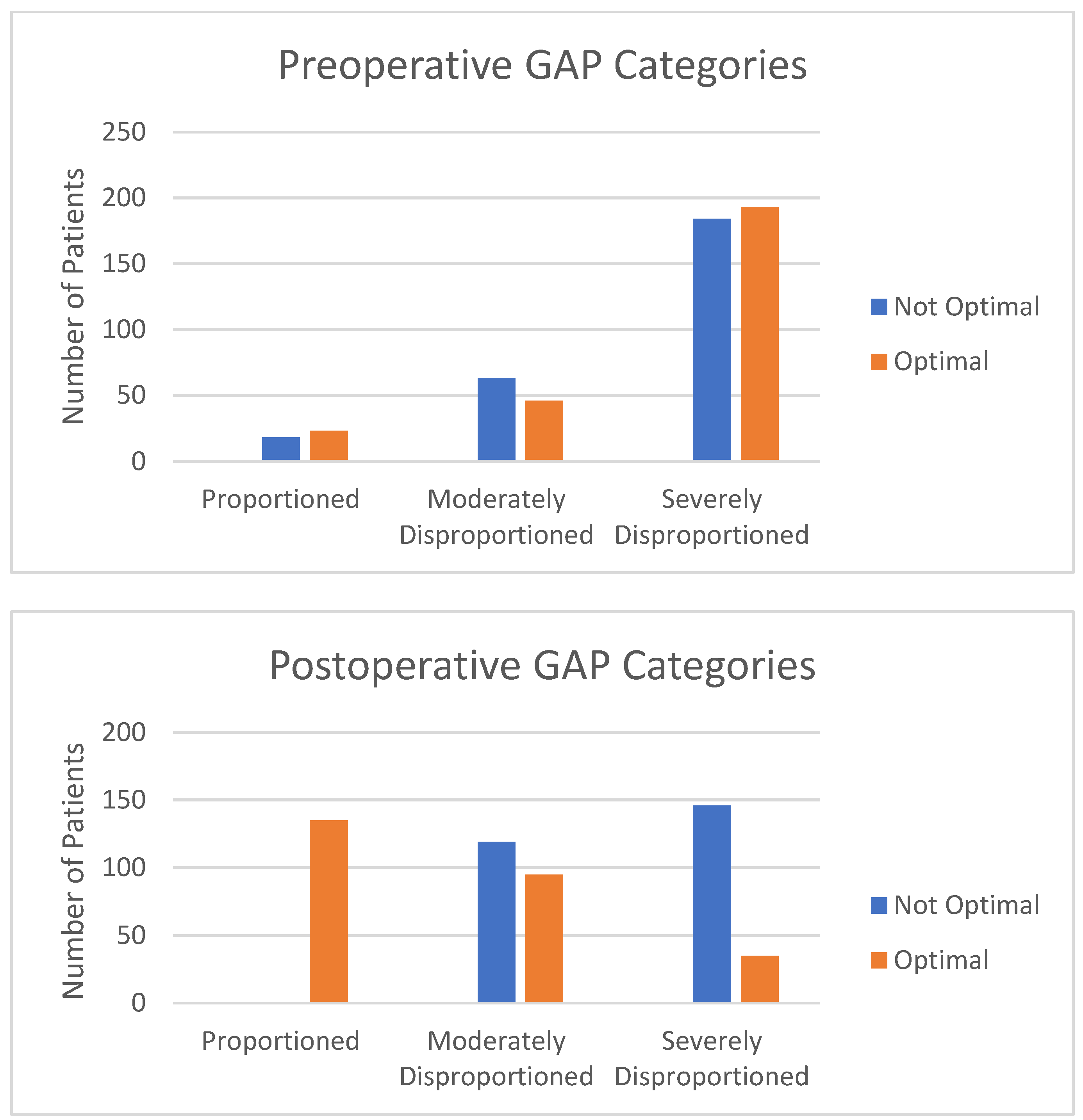
3.2. Categorization
3.3. Comparison of Surgical Details and Hospital Stay Based on Radiographic Outcomes
3.4. Comparison of Early Metrics during 90-Day Perioperative Course
3.5. Complication Rates by Two Years
3.6. Patient-Reported Outcomes by Two Years
3.7. Cost Analysis
3.8. Cost-Utility Trend Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Passias, P.G.; Segreto, F.A.; Lafage, R.; Lafage, V.; Smith, J.S.; Line, B.G.; Scheer, J.K.; Mundis, G.M.; Hamilton, D.K.; Kim, H.J.; et al. Recovery kinetics following spinal deformity correction: A comparison of isolated cervical, thoracolumbar, and combined deformity morphometries. Spine J. 2019, 19, 1422–1433. [Google Scholar] [CrossRef]
- Passias, P.G.; Jalai, C.M.; Lafage, V.; Poorman, G.W.; Vira, S.; Horn, S.R.; Scheer, J.K.; Hamilton, D.K.; Line, B.G.; Bess, S.; et al. Recovery Kinetics of Radiographic and Implant-Related Revision Patients Following Adult Spinal Deformity Surgery. Neurosurgery 2017, 83, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Bridwell, K.H.; Glassman, S.; Horton, W.; Shaffrey, C.; Schwab, F.; Zebala, L.P.; Lenke, L.G.; Hilton, J.F.; Shainline, M.; Baldus, C.; et al. Does treatment (nonoperative and operative) improve the two-year quality of life in patients with adult symptomatic lumbar scoliosis: A prospective multicenter evidence-based medicine study. Spine 2009, 34, 2171–2178. [Google Scholar] [CrossRef]
- Smith, J.S.; The Spinal Deformity Study Group; Shaffrey, C.I.; Glassman, S.D.; Carreon, L.Y.; Schwab, F.J.; Lafage, V.; Arlet, V.; Fu, K.-M.G.; Bridwell, K.H. Clinical and radiographic parameters that distinguish between the best and worst outcomes of scoliosis surgery for adults. Eur. Spine J. 2012, 22, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Bridwell, K.H.; Baldus, C.; Berven, S.; Edwards, C.; Glassman, S.; Hamill, C.; Horton, W.; Lenke, L.G.; Ondra, S.; Schwab, F.; et al. Changes in Radiographic and Clinical Outcomes with Primary Treatment Adult Spinal Deformity Surgeries From Two Years to Three- to Five-Years Follow-up. Spine 2010, 35, 1849–1854. [Google Scholar] [CrossRef]
- Smith, J.S.; Shaffrey, C.I.; Lafage, V.; Scheer, J.K.; Fu, K.-M.G.; Mundis, G.M.; Kim, H.J.; Deviren, V.; Soroceanu, A.; Hart, R.A.; et al. Comparison of best versus worst clinical outcomes for adult spinal deformity surgery: A retrospective review of a prospectively collected, multicenter database with 2-year follow-up. J. Neurosurg. Spine 2015, 23, 349–359. [Google Scholar] [CrossRef]
- Smith, J.S.; Shaffrey, C.I.; Lafage, R.; Mundis, G.M.; Errico, T.J.; Kim, H.J.; Protopsaltis, T.S.; Hamilton, D.K.; Scheer, J.K.; Soroceanu, A.; et al. Prospective multicenter assessment of perioperative and minimum 2-year postoperative complication rates associated with adult spinal deformity surgery. J. Neurosurg. Spine 2016, 25, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Marbacher, S.; Mannion, A.F.; Burkhardt, J.-K.; Schär, R.T.; Porchet, F.; Kleinstück, F.; Jeszenszky, D.; Fekete, T.F.; Haschtmann, D. Patient-Rated Outcomes of Lumbar Fusion in Patients With Degenerative Disease of the Lumbar Spine. Spine 2016, 41, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Reid, D.B.; Daniels, A.H.; Ailon, T.; Miller, E.; Sciubba, D.M.; Smith, J.S.; Shaffrey, C.I.; Schwab, F.; Burton, D.; Hart, R.A.; et al. Frailty and Health-Related Quality of Life Improvement Following Adult Spinal Deformity Surgery. World Neurosurg. 2018, 112, e548–e554. [Google Scholar] [CrossRef]
- Scheer, J.K.; Smith, J.S.; Lafage, V.; Shaffrey, C.I.; Bess, S.; Daniels, A.H.; Hart, R.A.; Protopsaltis, T.S.; Mundis, G.M.; Sciubba, D.M.; et al. Development of a preoperative predictive model for major complications following adult spinal deformity surgery. J. Neurosurg. Spine 2017, 26, 736–743. [Google Scholar] [CrossRef]
- Cho, K.-J.; Suk, S.-I.; Park, S.-R.; Kim, J.-H.; Kim, S.-S.; Choi, W.-K.; Lee, K.-Y.; Lee, S.-R. Complications in Posterior Fusion and Instrumentation for Degenerative Lumbar Scoliosis. Spine 2007, 32, 2232–2237. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, J.D.; Lenke, L.G.; Bridwell, K.H.; Sehn, J.K.; Milby, A.H.; Bumpass, D.; Crawford, C.H.; Oʼshaughnessy, B.A.; Buchowski, J.M.; Chang, M.S.; et al. Major Complications and Comparison between 3-Column Osteotomy Techniques in 105 Consecutive Spinal Deformity Procedures. Spine 2012, 37, 1198–1210. [Google Scholar] [CrossRef]
- Lafage, R.; Schwab, F.; Glassman, S.; Bess, S.; Harris, B.; Sheer, J.; Hart, R.; Line, B.; Henry, J.; Burton, D.; et al. Age-Adjusted Alignment Goals Have the Potential to Reduce PJK. Spine 2017, 42, 1275–1282. [Google Scholar] [CrossRef]
- Yilgor, C.; Sogunmez, N.; Boissiere, L.; Yavuz, Y.; Obeid, I.; Kleinstück, F.; Pérez-Grueso, F.J.S.; Acaroglu, E.; Haddad, S.; Mannion, A.F.; et al. Global Alignment and Proportion (GAP) Score: Development and Validation of a New Method of Analyzing Spinopelvic Alignment to Predict Mechanical Complications After Adult Spinal Deformity Surgery. J. Bone Jt. Surg. 2017, 99, 1661–1672. [Google Scholar] [CrossRef]
- Almand, J.; Pickering, T.; Parsell, D.; Stronach, B.; Carlisle, R.; McIntyre, L. The successful migration of total joint arthroplasty from the hospital inpatient to outpatient ASC setting. Knee 2021, 34, 17–23. [Google Scholar] [CrossRef]
- Smith, J.S.; Klineberg, E.; Schwab, F.; Shaffrey, C.I.; Moal, B.; Ames, C.P.; Hostin, R.; Fu, K.-M.G.; Burton, D.; Akbarnia, B.; et al. Change in classification grade by the srs-schwab adult spinal deformity classification predicts impact on health-related quality of life measures: Prospective analysis of operative and nonoperative treatment. Spine 2013, 38, 1663–1671. [Google Scholar] [CrossRef]
- Copay, A.G.; Glassman, S.D.; Subach, B.R.; Berven, S.; Schuler, T.C.; Carreon, L.Y. Minimum clinically important difference in lumbar spine surgery patients: A choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and Pain Scales. Spine J. 2008, 8, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Courtney, M.P.; Ashley, B.S.; Hume, E.L.; Kamath, A.F. Are Bundled Payments a Viable Reimbursement Model for Revision Total Joint Arthroplasty? Clin. Orthop. Relat. Res. 2016, 474, 2714–2721. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.T.; D’Oro, A.; Buser, Z.; Youssef, J.A.; Park, J.-B.; Meisel, H.-J.; Brodke, D.S.; Wang, J.C.; Yoon, S.T. Trends and Costs of Anterior Cervical Discectomy and Fusion: A Comparison of Inpatient And Outpatient Procedures. Iowa Orthop. J. 2018, 38, 167–176. [Google Scholar]
- Malik, A.T.; Phillips, F.M.; Yu, E.; Khan, S.N. Are current DRG-based bundled payment models for lumbar fusions risk-adjusting adequately? An analysis of Medicare beneficiaries. Spine J. 2019, 20, 32–40. [Google Scholar] [CrossRef]
- Sutton, J.C.; Antoniou, J.; Epure, L.M.; Huk, O.L.; Zukor, D.J.; Bergeron, S.G. Hospital Discharge within 2 Days Following Total Hip or Knee Arthroplasty Does not Increase Major-Complication and Readmission Rates. J. Bone Jt. Surg. 2016, 98, 1419–1428. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.E.; Lebovic, J.; Alas, H.; Pierce, K.E.; Bortz, C.A.; Ahmad, W.; Naessig, S.; Hassanzadeh, H.; Labaran, L.A.; Puvanesarajah, V.; et al. A cost utility analysis of treating different adult spinal deformity frailty states. J. Clin. Neurosci. 2020, 80, 223–228. [Google Scholar] [CrossRef]
- Passias, P.G.; Bortz, C.A.; Pierce, K.E.; Alas, H.; Brown, A.; Vasquez-Montes, D.; Naessig, S.; Ahmad, W.; Diebo, B.G.; Raman, T.; et al. A Simpler, Modified Frailty Index Weighted by Complication Occurrence Correlates to Pain and Disability for Adult Spinal Deformity Patients. Int. J. Spine Surg. 2020, 14, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Champain, S.; Benchikh, K.; Nogier, A.; Mazel, C.; Guise, J.D.; Skalli, W. Validation of new clinical quantitative analysis software applicable in spine orthopaedic studies. Eur. Spine J. 2005, 15, 982–991. [Google Scholar] [CrossRef]
- Rillardon, L.; Levassor, N.; Guigui, P.; Wodecki, P.; Cardinne, L.; Templier, A.; Skalli, W. Validation of a tool to measure pelvic and spinal parameters of sagittal balance. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2003, 89, 218–227. [Google Scholar]
- O’Brien, M.F.; Kuklo, T.R.T.R.; Blanke, K.M.; Lenke, L.G. Spinal Deformity Study Group Radiographic Measurement Manual. Medtronic Sofamor Danek. 2005. Available online: http://www.oref.org/docs/default-source/default-document-library/sdsg-radiographic-measuremnt-manual.pdf?sfvrsn=2 (accessed on 26 May 2022).
- Copay, A.G.; Subach, B.R.; Glassman, S.D.; Polly, D.W., Jr.; Schuler, T.C. Understanding the minimum clinically important difference: A review of concepts and methods. Spine J. 2007, 7, 541–546. [Google Scholar] [CrossRef]
- Berven, S.; Deviren; Demir-Deviren, S.; Hu, S.; Bradford, D. Minimal clinically important difference in adult spinal deformity: How much change is significant? In Proceedings of the 12th International Meeting for Advanced Spine Techniques (IMAST), Banff, Canada, 7–9 July 2005; 2005. [Google Scholar]
- Blondel, B.; Schwab, F.; Ungar, B.B.; Smith, J.; Bridwell, K.; Glassman, S.; Shaffrey, C.; Farcy, J.-P.; Lafage, V. Impact of Magnitude and Percentage of Global Sagittal Plane Correction on Health-Related Quality of Life at 2-Years Follow-Up. Neurosurgery 2012, 71, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Schwab, F.; Smith, J.S.; Klineberg, E.; Ames, C.P.; Mundis, G.; Hostin, R.; Kebaish, K.; Deviren, V.; Gupta, M.; et al. Likelihood of reaching minimal clinically important difference in adult spi-nal deformity: A comparison of operative and nonoperative treatment. Ochsner J. 2014, 14, 67–77. [Google Scholar]
- Pierce, K.E.; Kapadia, B.H.; Bortz, C.; Alas, H.; Brown, A.E.; Diebo, B.G.; Raman, T.; Jain, D.; Lebovic, J.; Passias, P.G. Frailty Severity Impacts Development of Hospital-acquired Conditions in Patients Undergoing Corrective Surgery for Adult Spinal Deformity. Clin. Spine Surg. Spine Publ. 2021, 34, E377–E381. [Google Scholar] [CrossRef]
- Terran, J.; Schwab, F.; Shaffrey, C.I.; Smith, J.S.; Devos, P.; Ames, C.P.; Fu, K.-M.G.; Burton, D.; Hostin, R.; Klineberg, E.; et al. The SRS-Schwab adult spinal deformity classification: Assessment and clinical correlations based on a prospective operative and nonoperative cohort. Neurosurgery 2013, 73, 559–568. [Google Scholar] [CrossRef]
- Draft ICD-10-CM/PCS MS-DRGv28 Definitions Manual n.d. Available online: https://www.cms.gov/icd10manual/fullcode_cms/p0370.html (accessed on 9 March 2019).
- Gum, J.L.; Hostin, R.; Robinson, C.; Kelly, M.P.; Carreon, L.Y.; Polly, D.W.; Bess, R.S.; Burton, D.C.; Shaffrey, C.I.; Smith, J.S.; et al. Impact of cost valuation on cost-effectiveness in adult spine deformity surgery. Spine J. 2016, 17, 96–101. [Google Scholar] [CrossRef]
- Murray, C.J. Quantifying the burden of disease: The technical basis for disability-adjusted life years. Bull. World Health Organ. 1994, 72, 429–445. [Google Scholar] [PubMed]
- WHO-CHOICE. Making Choices in Health: WHO Guide to Cost-Effectiveness Analysis. Glob Program Evidence for Health Policy; World Health Organization: Geneva, Switzerland, 2003; p. 71. Available online: https://www.who.int/choice/publications/p_2003_generalised_cea.pdf (accessed on 25 June 2023).
- Hutubessy, R.; Chisholm, D.; Edejer, T.T.-T. Generalized cost-effectiveness analysis for national-level priority-setting in the health sector. Cost Eff. Resour. Alloc. 2003, 1, 8. [Google Scholar] [CrossRef]
- Grosse, S.D.; Teutsch, S.M.; Haddix, A.C. Lessons from Cost-Effectiveness Research for United States Public Health Policy. Annu. Rev. Public Health 2007, 28, 365–391. [Google Scholar] [CrossRef] [PubMed]
- International Monetary Fund. Report for Selected Countries and Subjects. World Economic Outlook Database. February 2022. Available online: https://www.imf.org/en/Publications/SPROLLs/world-economic-outlook-databases#sort=%40imfdate%20descending (accessed on 25 June 2023).
- Carreon, L.Y.; Anderson, P.A.; McDonough, C.M.; Djurasovic, M.; Glassman, S.D. Predicting SF-6D Utility Scores From the Neck Disability Index and Numeric Rating Scales for Neck and Arm Pain. Spine 2011, 36, 490–494. [Google Scholar] [CrossRef]
- Ames, C.P.; Scheer, J.K.; Lafage, V.; Smith, J.S.; Bess, S.; Berven, S.H.; Mundis, G.M.; Sethi, R.K.; Deinlein, D.A.; Coe, J.D.; et al. Adult Spinal Deformity: Epidemiology, Health Impact, Evaluation, and Management. Spine Deform. 2016, 4, 310–322. [Google Scholar] [CrossRef]
- Sciubba, D.M.; Scheer, J.K.; Yurter, A.; Smith, J.S.; Lafage, V.; Klineberg, E.; Gupta, M.; Eastlack, R.; Mundis, G.M.; Protopsaltis, T.S.; et al. Patients with spinal deformity over the age of 75: A retrospective analysis of operative versus non-operative management. Eur. Spine J. 2015, 25, 2433–2441. [Google Scholar] [CrossRef]
- Alvarado, A.M.; Schatmeyer, B.A.; Arnold, P.M. Cost-Effectiveness of Adult Spinal Deformity Surgery. Glob. Spine J. 2020, 11, 73S–78S. [Google Scholar] [CrossRef] [PubMed]
- Scheer, J.K.; Hostin, R.; Robinson, C.; Schwab, F.; Lafage, V.; Burton, D.C.; Hart, R.A.; Kelly, M.P.; Keefe, M.; Polly, D.; et al. Operative Management of Adult Spinal Deformity Results in Significant Increases in QALYs Gained Compared to Nonoperative Management: Analysis of 479 Patients with Minimum 2-Year Follow-Up. Spine 2018, 43, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Yeramaneni, S.; Robinson, C.; Hostin, R. Impact of spine surgery complications on costs associated with management of adult spinal deformity. Curr. Rev. Musculoskelet. Med. 2016, 9, 327–332. [Google Scholar] [CrossRef]
- Arutyunyan, G.G.; Angevine, P.D.; Berven, S. Cost-Effectiveness in Adult Spinal Deformity Surgery. Neurosurgery 2018, 83, 597–601, Erratum in Neurosurgery 2019, 84, 815. [Google Scholar] [CrossRef] [PubMed]
- Terran, J.; McHugh, B.J.; Fischer, C.R.; Lonner, B.; Warren, D.; Glassman, S.; Bridwell, K.; Schwab, F.; Lafage, V. Surgical treatment for adult spinal deformity: Projected cost effectiveness at 5-year follow-up. Ochsner J. 2014, 14, 14–22. [Google Scholar]
- Passias, P.G.; Brown, A.E.; Bortz, C.; Alas, H.; Pierce, K.; Ahmad, W.; Naessig, S.; Lafage, R.; Lafage, V.; Hassanzadeh, H.; et al. Increasing Cost Efficiency in Adult Spinal Deformity Surgery. Spine 2021, 47, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.R.; Terran, J.; Lonner, B.; McHugh, B.; Warren, D.; Glassman, S.; Bridwell, K.; Schwab, F.; Lafage, V. Factors Predicting Cost-effectiveness of Adult Spinal Deformity Surgery at 2 Years. Spine Deform. 2014, 2, 415–422. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Not Optimal | Optimal | p-Value | |
|---|---|---|---|
| Surgical/Admission Characteristic | |||
| Number of Levels Fused | 10.1 ± 4.6 levels | 11.8 ± 3.9 levels | <0.001 |
| Estimated Blood Loss | 1684 ± 1588 mL | 1829 ± 1386 mL | 0.264 |
| Operative Time | 448 ± 188 min | 465 ± 190 min | 0.299 |
| Osteotomy | 65% | 83% | <0.001 |
| 3CO | 15% | 25% | 0.006 |
| Decompression | 61% | 68% | 0.065 |
| Invasiveness Index | 83.3 | 104.3 | <0.001 |
| Length of Stay | 7.8 ± 4.3 days | 8.3 ± 6.2 days | 0.231 |
| SICU Admission | 67% | 71% | 0.303 |
| Not Optimal | Optimal | p-Value | |
|---|---|---|---|
| Complications within 90 Days | |||
| Adverse Event | 12.1% | 16.6% | 0.137 |
| Hospital-Acquired Condition | 9.8% | 9.4% | 0.883 |
| Any Perioperative Complication | 49.4% | 50.2% | 0.862 |
| Medical | 7.9% | 10.6% | 0.295 |
| Neurological | 3.4% | 1.1% | 0.080 |
| Pulmonary | 4.2% | 4.5% | 0.832 |
| Renal | 1.1% | 0.4% | 0.316 |
| Musculoskeletal | 3.4% | 3.8% | 0.816 |
| Cardiac | 0.8% | 1.5% | 0.413 |
| Gastrointestinal | 5.3% | 5.3% | 0.999 |
| Infection | 5.7% | 4.2% | 0.422 |
| Two-Year Complications | |||
| Any Complication | 72.1% | 70.6% | 0.702 |
| Major Complication | 51.9% | 38.4% | 0.021 |
| Minor Complication | 40.0% | 36.6% | 0.422 |
| Mechanical Complication | 44.2% | 31.7% | 0.003 |
| Major Mechanical Complications | 22.4% | 12.1% | 0.002 |
| Mechanical Complications Requiring Reoperation | 18.2% | 8.0% | 0.001 |
| Reoperation | 32.5% | 22.6% | 0.008 |
| Outcome | Not Optimal | Optimal | p-Value |
|---|---|---|---|
| MCID in ODI | 47% | 53% | 0.218 |
| MCID in SRS-22 Pain | 60% | 71% | 0.042 |
| MCID in SRS-22 Appearance | 57% | 74% | 0.001 |
| MCID in SRS-22 Activity | 56% | 60% | 0.531 |
| MCID in SF-36 PCS | 45% | 64% | 0.001 |
| Best Clinical Outcome | 8.8% | 15.1% | 0.025 |
| Did Not Meet Optimal Radiographic Outcome | Met Optimal Radiographic Outcome | p-Value | |
|---|---|---|---|
| 6 Weeks | |||
| Utility Gained | 0.552 | 0.548 | 0.837 |
| Week 6 QALYs | 0.063 | 0.063 | 0.837 |
| Upfront Cost | $63,623.07 | $62,406.37 | 0.399 |
| Week 6 Cost per QALY | $1,138,113.98 | $1,081,398.68 | 0.261 |
| 1 Year | |||
| Utility Gained | 0.468 | 0.485 | 0.184 |
| Year 1 QALYs | 0.461 | 0.477 | 0.184 |
| Year 1 Cost per QALY | $234,966.79 | $196,186.90 | <0.001 |
| 2 Year | |||
| Utility Gained | 0.475 | 0.495 | 0.108 |
| Year 2 QALYs | 0.922 | 0.961 | 0.108 |
| Year 2 Overall Cost | $108,320.30 | $93,727.98 | 0.002 |
| Year 2 Cost per QALY | $117,488.03 | $97,553.18 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Passias, P.G.; Williamson, T.K.; Mir, J.M.; Smith, J.S.; Lafage, V.; Lafage, R.; Line, B.; Daniels, A.H.; Gum, J.L.; Schoenfeld, A.J.; et al. Are We Focused on the Wrong Early Postoperative Quality Metrics? Optimal Realignment Outweighs Perioperative Risk in Adult Spinal Deformity Surgery. J. Clin. Med. 2023, 12, 5565. https://doi.org/10.3390/jcm12175565
Passias PG, Williamson TK, Mir JM, Smith JS, Lafage V, Lafage R, Line B, Daniels AH, Gum JL, Schoenfeld AJ, et al. Are We Focused on the Wrong Early Postoperative Quality Metrics? Optimal Realignment Outweighs Perioperative Risk in Adult Spinal Deformity Surgery. Journal of Clinical Medicine. 2023; 12(17):5565. https://doi.org/10.3390/jcm12175565
Chicago/Turabian StylePassias, Peter G., Tyler K. Williamson, Jamshaid M. Mir, Justin S. Smith, Virginie Lafage, Renaud Lafage, Breton Line, Alan H. Daniels, Jeffrey L. Gum, Andrew J. Schoenfeld, and et al. 2023. "Are We Focused on the Wrong Early Postoperative Quality Metrics? Optimal Realignment Outweighs Perioperative Risk in Adult Spinal Deformity Surgery" Journal of Clinical Medicine 12, no. 17: 5565. https://doi.org/10.3390/jcm12175565
APA StylePassias, P. G., Williamson, T. K., Mir, J. M., Smith, J. S., Lafage, V., Lafage, R., Line, B., Daniels, A. H., Gum, J. L., Schoenfeld, A. J., Hamilton, D. K., Soroceanu, A., Scheer, J. K., Eastlack, R., Mundis, G. M., Diebo, B., Kebaish, K. M., Hostin, R. A., Jr., Gupta, M. C., ... on behalf of the International Spine Study Group. (2023). Are We Focused on the Wrong Early Postoperative Quality Metrics? Optimal Realignment Outweighs Perioperative Risk in Adult Spinal Deformity Surgery. Journal of Clinical Medicine, 12(17), 5565. https://doi.org/10.3390/jcm12175565