
Exploring Adaptive Cycling Interventions for Young People with Disability: An Online Survey of Providers in Australia
 ,
,  and
and
Abstract
:1. Introduction
- To describe adaptive cycling interventions delivered by allied health therapists, teachers and sports and recreation providers using the template for intervention description and replication (TIDieR) checklist [23].
- To explore providers’ perspectives for recommending an adaptive cycling intervention, and the barriers and facilitators for using an adapted cycle.
2. Materials and Methods
2.1. Study Design
2.2. Survey Development, Content and Pre-Testing
2.3. Participant Eligibility and Recruitment
- A recognized qualification and/or registration within their respective area of practice;
- Experience leading adaptive cycling interventions or training in Australia;
- Aged > 18 years; and
- Able to complete a survey in English.
2.4. Management of Responses
2.5. Data Analysis
3. Results
3.1. Respondent Demographics
3.2. Respondent Roles
3.3. Characteristics of Young Riders with Disability
3.4. Parameters for Beginner Adaptive Cycle Interventions
3.4.1. Providers’ Rationale and Goals
3.4.2. Essential Elements and Training Approaches
3.4.3. Equipment and Materials
3.4.4. Training Dose

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FITT Domain | Response | n | % |
|---|---|---|---|
| Frequency (a) | Over several weeks | 47 | 52.2 |
| On request | 32 | 35.6 | |
| Once-off | 22 | 24.2 | |
| 3–5 days | 12 | 13.3 | |
| Other | 10 | 11.1 | |
| Intensity (b) | Skills focus | 66 | 74.2 |
| Low intensity | 7 | 7.9 | |
| Moderate intensity | 13 | 14.6 | |
| Moderate to vigorous | 3 | 3.4 | |
| Time/duration (b) | <20 min | 6 | 6.7 |
| 30 min | 29 | 32.6 | |
| 45 min | 28 | 31.5 | |
| 60 min | 25 | 28.1 | |
| 75 min | 1 | 1.1 | |
| Type of setting (c) | School | 46 | 50.5 |
| Car traffic-free environment | 44 | 48.4 | |
| Home | 40 | 44.0 | |
| Clinic | 30 | 33.0 | |
| Bike path | 22 | 24.2 | |
| Velodrome | 2 | 2.2 | |
| Trail (e.g., mountain bike track) | 2 | 2.2 |
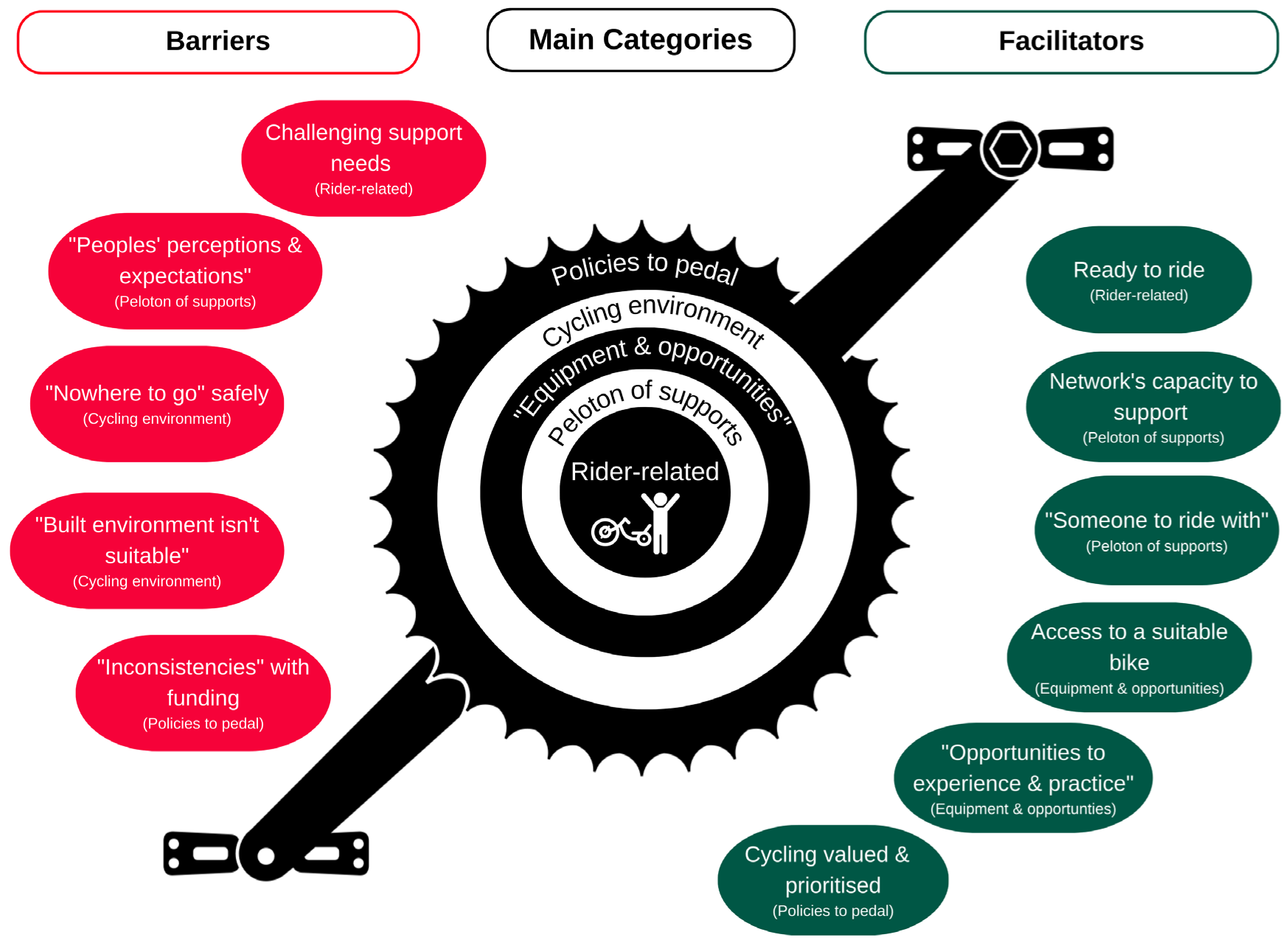
3.5. Barriers and Facilitators to Adaptive Cycling
3.5.1. Rider-Related Factors
3.5.2. Peloton of Supports
3.5.3. Equipment and Opportunities
3.5.4. Cycling Environment
3.5.5. Policies to Pedal
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Munro, C. National Walking and Cycling Participation Survey 2021. Cycling and Walking Australia and New Zealand (CWANZ). 2022. Available online: https://www.cwanz.com.au/wp-content/uploads/2021/08/NWCPS_2021_report_v2.0.pdf (accessed on 23 July 2023).
- Toovey, R.; Reid, S.M.; Rawicki, B.; Harvey, A.R.; Watt, K. Ability of independently ambulant children with cerebral palsy to ride a two-wheel bicycle: A case–control study. Dev. Med. Child Neurol. 2017, 59, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Hawks, Z.; Constantino, J.N.; Weichselbaum, C.; Marrus, N. Accelerating Motor Skill Acquisition for Bicycle Riding in Children with ASD: A Pilot Study. J. Autism Dev. Disord. 2020, 50, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Witter, A. The Determinants of Successful Cycling in Children with Special Needs. Master’s Thesis, University of Victoria, Victoria, BC, Canada, 19 August 2013. Available online: http://hdl.handle.net/1828/4760 (accessed on 23 July 2023).
- Ulrich, D.A.; Burghardt, A.R.; Lloyd, M.; Tiernan, C.; Hornyak, J.E. Physical Activity Benefits of Learning to Ride a Two-Wheel Bicycle for Children with Down Syndrome: A Randomized Trial. Phys. Ther. 2011, 91, 1463–1477. [Google Scholar] [CrossRef]
- Buckley, T.; Bird, S.; Sacks, G.; Archer, B. The achievements of teenagers with Down syndrome. Down Syndr. News Update 2002, 2, 90–96. [Google Scholar]
- Toovey, R.A.M.; Harvey, A.R.; McGinley, J.L.; Lee, K.J.; Shih, S.T.; Spittle, A.J. Task-specific training for bicycle-riding goals in ambulant children with cerebral palsy: A randomized controlled trial. Dev. Med. Child Neurol. 2022, 64, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.E.; McHugh, E.; Harrington, S.L.; Davis, T.; Lieberman, L.J. Adapted Bicycles for Teaching Riding Skills. Teach. Except. Child. 2005, 37, 50–56. [Google Scholar] [CrossRef]
- Halayko, J.; Magill-Evans, J.; Smith, V.; Polatajko, H. Enabling 2-wheeled cycling for youth with Down syndrome. Pediatr. Phys. Ther. 2016, 28, 224–230. [Google Scholar] [CrossRef]
- Pickering, D.M.; Horrocks, L.; Visser, K.; Todd, G. Adapted bikes—What children and young people with cerebral palsy told us about their participation in adapted dynamic cycling. Disabil. Rehabil. Assist. Technol. 2013, 8, 30–37. [Google Scholar] [CrossRef]
- Clayton, W.; Parkin, J.; Billington, C. Cycling and disability: A call for further research. J. Transp. Health 2017, 6, 452–462. [Google Scholar] [CrossRef]
- Thevarajah, A.; Wallen, M.; Imms, C.; Lonsdale, C.; Carey, J.J.; Froude, E.H. Impact of adapted bicycle riding on outcomes for children and adolescents with disabilities: A systematic review. Dev. Med. Child Neurol. 2023, 65, 456–468. [Google Scholar] [CrossRef]
- Toovey, R.; Spittle, A.J.; Nicolaou, A.; McGinley, J.L.; Harvey, A.R. Training Two-Wheel Bike Skills in Children with Cerebral Palsy: A Practice Survey of Therapists in Australia. Phys. Occup. Ther. Pediatr. 2019, 39, 580–597. [Google Scholar] [CrossRef] [PubMed]
- Goodlin, G.T.; Steinbeck, L.; Bergfeld, D.; Haselhorst, A. Adaptive Cycling: Classification, Adaptations, and Biomechanics. Phys. Med. Rehabil. Clin. N. Am. 2022, 33, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Pickering, D.; Horrocks, L.M.; Visser, K.S.; Todd, G. ‘Every picture tells a story’: Interviews and diaries with children with cerebral palsy about adapted cycling. J. Paediatr. Child Health 2013, 49, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, E.L.; Boyd, R.N.; Carty, C.P.; Kentish, M.J.; Goodlich, B.I.; Horan, S.A. A qualitative analysis of the experiences of children with cerebral palsy and their caregivers in a goal-directed cycling programme. Disabil. Rehabil. 2022, 44, 2715–2722. [Google Scholar] [CrossRef] [PubMed]
- Jackman, M.; Sakzewski, L.; Morgan, C.; Boyd, R.N.; Brennan, S.E.; Langdon, K.; Toovey, R.; Greaves, S.; Thorley, M.; Novak, I. Interventions to improve physical function for children and young people with cerebral palsy: International clinical practice guideline. Dev. Med. Child Neurol. 2022, 64, 536–549. [Google Scholar] [CrossRef]
- Pearson, L.; Berkovic, D.; Reeder, S.; Gabbe, B.; Beck, B. Adults’ self-reported barriers and enablers to riding a bike for transport: A systematic review. Transp. Rev. 2022, 43, 356–384. [Google Scholar] [CrossRef]
- Mercê, C.; Branco, M.; Catela, D.; Lopes, F.; Cordovil, R. Learning to Cycle: From Training Wheels to Balance Bike. Int. J. Environ. Res. Public Health 2022, 19, 1814. [Google Scholar] [CrossRef]
- Daly, C.; Moore, C.L.; Johannes, S.; Middleton, J.; Kenyon, L.K. Pilot Evaluation of a School-Based Programme Focused on Activity, Fitness, and Function among Children with Cerebral Palsy at GMFCS Level IV: Single-Subject Research Design. Physiother. Can. 2020, 72, 195–204. [Google Scholar] [CrossRef]
- Todd, T.; Reid, G.; Butler-Kisber, L. Cycling for students with ASD: Self-regulation promotes sustained physical activity. Adapt. Phys. Act. Q. 2010, 27, 226–241. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; Petticrew, M.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Barbour, V.; Macdonald, H. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Improving the quality of web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Sharma, A.; Duc, N.T.M.; Thang, T.L.L.; Nam, N.H.; Ng, S.J.; Abbas, K.S.; Huy, N.T.; Marušić, A.; Paul, C.L.; Kwok, J.; et al. A Consensus-Based Checklist for Reporting of Survey Studies (CROSS). J. Gen. Intern. Med. 2021, 36, 3179–3187. [Google Scholar] [CrossRef]
- IAP2 Spectrum of Public Participation. Available online: https://iap2.org.au/resources/iap2-tools/ (accessed on 23 July 2023).
- Staniszewska, S.; Brett, J.; Simera, I.; Seers, K.; Mockford, C.; Goodlad, S.; Altman, D.G.; Moher, D.; Barber, R.; Denegri, S.; et al. GRIPP2 reporting checklists: Tools to improve reporting of patient and public involvement in research. BMJ 2017, 358, j3453. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Dreyfus, S.E. The five-stage model of adult skill acquisition. Bull. Sci. Technol. Soc. 2004, 24, 177–181. [Google Scholar] [CrossRef]
- Law, M.; Baptiste, B.; Mccoll, M.; Opzoomer, A.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: An Outcome Measure for Occupational Therapy. Can. J. Occup. Ther. 1990, 57, 82–87. [Google Scholar] [CrossRef]
- Turner-Stokes, L. Goal attainment scaling (GAS) in rehabilitation: A practical guide. Clin. Rehabil. 2009, 23, 362–370. [Google Scholar] [CrossRef]
- Jansen, M.; De Jong, M.; Coes, H.M.; Eggermont, F.; Van Alfen, N.; De Groot, I.J.M. The assisted 6-minute cycling test to assess endurance in children with a neuromuscular disorder. Muscle Nerve 2012, 46, 520–530. [Google Scholar] [CrossRef]
- Halayko, J. You Can Ride Too! An Exploration of the Guided Discovery of Two-wheeled Cycling Skills by Youth with Intellectual Disabilities. Master’s Thesis, University of Alberta, Edmonton, AB, Canada, 2014; pp. 63–65. Available online: https://era.library.ualberta.ca/items/9e277c60-e496-456c-a4ca-08332078d563 (accessed on 23 July 2023).
- Polatajko, H.J.; Mandich, A. Enabling Occupation in Children: The Cognitive Orientation to Daily Occupational Performance (CO-OP) Approach; CAOT Publications ACE: Ottawa, ON, Canada, 2004. [Google Scholar]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Behav. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Burt, T.; Porretta, D.; Klein, R. Use of Adapted Bicycles on the Learning of Conventional Cycling by Children with Mental Retardation. Educ. Train. Dev. Disabil. Publ. Div. Autism Dev. Disabil. 2007, 42, 364–379. [Google Scholar]
- Field, D.A.; Livingstone, R.W. Power mobility skill progression for children and adolescents: A systematic review of measures and their clinical application. Dev. Med. Child Neurol. 2018, 60, 997–1011. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, L.K.; Schmitt, J.; Otieno, S.; Cohen, L. Providing paediatric power wheelchairs in the USA then and now: A survey of providers. Disabil. Rehabil. Assist. Technol. 2020, 15, 708–717. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, L.; Kenyon, L. Assessment and Intervention for Tool-Use in Learning Powered Mobility Intervention: A Focus on Tyro Learners. Disabilities 2022, 2, 304–316. [Google Scholar] [CrossRef]
- Fragala-Pinkham, M.A.; Ball, A.L.; Jeffries, L.M. Efficacy of Lower Extremity Cycling Interventions for Youth with Intellectual Disabilities: A Systematic Review. Phys. Occup. Ther. Pediatr. 2021, 41, 410–428. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Gorter, J. The ‘F-words’ in childhood disability: I swear this is how we should think! Child Care Health Dev. 2012, 38, 457–463. [Google Scholar] [CrossRef]
- Goodlin, G.T.; Steinbeck, L.; Bergfeld, D.; Haselhorst, A. Adaptive Cycling: Injuries and Health Concerns. Phys. Med. Rehabil. Clin. N. Am. 2022, 33, 45–60. [Google Scholar] [CrossRef]
- Martin Ginis, K.A.; Ma, J.K.; Latimer-Cheung, A.E.; Rimmer, J.H. A systematic review of review articles addressing factors related to physical activity participation among children and adults with physical disabilities. Health Psychol. Rev. 2016, 10, 478–494. [Google Scholar] [CrossRef]
| Demographic | Response | n | % |
|---|---|---|---|
| Discipline | Physiotherapist | 61 | 57.0 |
| Occupational therapist | 20 | 18.7 | |
| Teacher | 12 | 11.2 | |
| Leisure or recreational therapist | 5 | 4.7 | |
| Teacher aide | 3 | 2.8 | |
| Exercise physiologist | 2 | 1.9 | |
| Other * provider | 4 | 3.7 | |
| Practice setting | Community allied health (not-for-profit/charity) | 38 | 35.5 |
| Allied health private practice | 29 | 27.1 | |
| Special education | 28 | 26.2 | |
| Tertiary health service | 6 | 5.6 | |
| Sport and recreation | 3 | 2.8 | |
| Other # | 3 | 2.8 | |
| Australian state or territory | Victoria | 53 | 49.5 |
| New South Wales | 16 | 15.0 | |
| Queensland | 14 | 13.1 | |
| South Australia | 11 | 10.3 | |
| Western Australia | 8 | 7.5 | |
| Tasmania | 3 | 2.8 | |
| Northern Territory | 1 | 0.9 | |
| Australian Capital Territory | 1 | 0.9 | |
| Geographic setting (ASGS∧) | Metropolitan | 72 | 67.3 |
| Inner regional | 20 | 18.7 | |
| Outer regional | 14 | 13.1 | |
| Remote | 1 | 0.9 | |
| Experience in adaptive cycling (years worked) | <1 year | 8 | 7.5 |
| 1–5 years | 32 | 29.9 | |
| 6–10 years | 28 | 26.2 | |
| 11–15 years | 26 | 24.3 | |
| >16 years | 13 | 12.1 | |
| Caseload age range (a) | Early intervention (aged 0–6 years) | 54 | 50.5 |
| Primary school (aged 5–12 years) | 84 | 79.2 | |
| Secondary school (aged 12–18 years) | 72 | 67.9 | |
| Young adults (aged 18–30 years) | 37 | 34.9 | |
| Adults (aged >18 years) | 6 | 5.7 | |
| Lifespan service (all ages) | 6 | 5.7 |
| Demographic | Response | n | % |
|---|---|---|---|
| Health condition or disability (a) | Cerebral palsy | 78 | 72.9 |
| Developmental delay | 72 | 67.3 | |
| Multiple disability | 56 | 52.3 | |
| Autism spectrum disorder | 51 | 47.7 | |
| Intellectual disability | 50 | 46.7 | |
| Acquired brain injury or stroke | 39 | 36.4 | |
| Down syndrome | 36 | 33.6 | |
| Sensory impairment | 19 | 17.7 | |
| Spinal cord injury | 9 | 9.3 | |
| Other * | 14 | 13.1 | |
| Rider skill level [30] (b) | Novice | 95 | 89.6 |
| Advanced beginner | 69 | 65.1 | |
| Competent | 20 | 18.7 | |
| Proficient | 6 | 5.7 | |
| Expert | 4 | 3.8 | |
| Riders’ access to an adapted cycle (c) | Purchase/provision via NDIS∧ | 85 | 85.0 |
| School/rehabilitation loan pool | 46 | 46.0 | |
| Self-funded purchase | 23 | 23.0 | |
| Short-term loan or hire | 11 | 11.0 | |
| Purchase/provision via other fundings | 7 | 7.0 | |
| Long-term loan or hire | 1 | 1.0 | |
| Riders’ perceived support needs for using an adapted cycle (d) | Balance and stability | 96 | 94.1 |
| Rider’s physical support needs | 91 | 89.2 | |
| Confidence | 88 | 86.3 | |
| Safety features | 46 | 45.1 | |
| Further possible modifications | 45 | 44.1 | |
| Other # | 12 | 11.8 | |
| None | 2 | 2.0 |
| TIDieR Domain | No. | TIDieR Item | Finding |
|---|---|---|---|
| WHY | 1. | Intervention | Training adaptive cycling skills for novice or beginner riders in car-free traffic environments. |
| 2. | Rationale | A means for young people with disabilities to work towards cycling goals whilst developing fitness, learning new skills and participating with others. Early skills training was expected to lead to local active leisure participation with immediate caregivers (i.e., family or a support worker). | |
| WHAT | 3. | Materials | Adapted cycle and accessories chosen for the rider’s personalized function and learning needs. Physical and instructional materials are listed in Supplementary File S5 (Figures S1 and S2). |
| 4. | Procedures | Six phases were found: (I) goal setting, (II) assessment, (III) bike exploration, (IV) bike selection, (V) skills training and (VI) community participation. Intervention types varied and included:
| |
| WHO | 5. | Provided | Allied health professionals (i.e., physiotherapists and occupational therapists) often led the assessment phase. Therapists, teachers and other providers contributed to adaptive cycling skills training. Family members and support workers led local practice. |
| HOW | 6. | Delivery mode | Face-to-face training delivered one-to-one or as part of a group. |
| WHERE | 7. | Setting | “Safe” protected spaces largely away from car-traffic situations. Many providers never experienced riders cycling in traffic situations (51.6%) or participating in active travel (55.9%) or cycling sports (road-cycling: 78.5% and mountain-biking: 84.9%) as per Supplementary File S5. |
| WHEN AND HOW MUCH | 8. | Frequency, intensity, time/duration, type | Providers offered training over several weeks, focusing on skills development rather than aerobic gains. Skills practice took 30–60 min (see Table 4 for further information). |
| 9. | Tailoring and modifications | Tailoring and modifications centred on changes relating to the task, adapted cycle, environment and rider. | |
| 10. | Task modification varied the level of assistance offered or the demand (physical or cognitive) required of the rider. The adapted cycle was modified based on physical support needs and rider confidence. The practice environment was altered based on the providers’ perception of safety, rider goals and local opportunities. | ||
| EVALUATION | 11. | Measuring change | Performance of the cycling activity and goal attainment [31,32] were the primary evaluative foci (see Supplementary File S5, Figure S3) [33]. This included cycle skills checklists [34], spatiotemporal parameters and levels of independence riding. |
| 12. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carey, J.J.; Toovey, R.; Spittle, A.J.; Imms, C.; Shields, N. Exploring Adaptive Cycling Interventions for Young People with Disability: An Online Survey of Providers in Australia. J. Clin. Med. 2023, 12, 5523. https://doi.org/10.3390/jcm12175523
Carey JJ, Toovey R, Spittle AJ, Imms C, Shields N. Exploring Adaptive Cycling Interventions for Young People with Disability: An Online Survey of Providers in Australia. Journal of Clinical Medicine. 2023; 12(17):5523. https://doi.org/10.3390/jcm12175523
Chicago/Turabian StyleCarey, John J., Rachel Toovey, Alicia J. Spittle, Christine Imms, and Nora Shields. 2023. "Exploring Adaptive Cycling Interventions for Young People with Disability: An Online Survey of Providers in Australia" Journal of Clinical Medicine 12, no. 17: 5523. https://doi.org/10.3390/jcm12175523
APA StyleCarey, J. J., Toovey, R., Spittle, A. J., Imms, C., & Shields, N. (2023). Exploring Adaptive Cycling Interventions for Young People with Disability: An Online Survey of Providers in Australia. Journal of Clinical Medicine, 12(17), 5523. https://doi.org/10.3390/jcm12175523