
Is Serum 25-Hydroxyvitamin D Level Associated with Severity of COVID-19? A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Outcomes
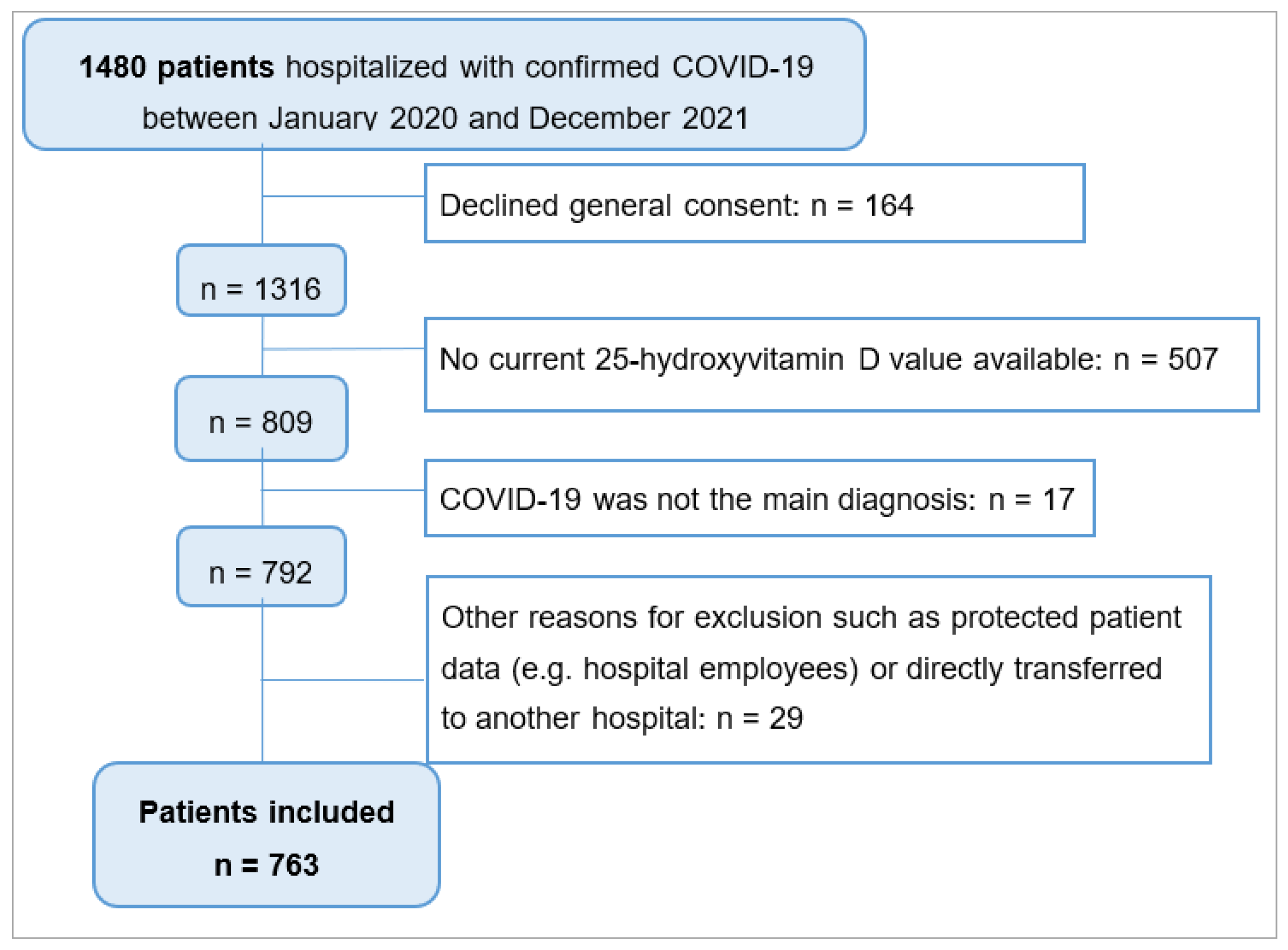
2.3. Patient Population: Inclusion and Exclusion Criteria
2.4. Data Collection Process
2.5. Defining Vitamin D Deficiency
2.6. Statistical Analysis
2.7. Ethical Approval
3. Results
3.1. Patient-Based Baseline Characteristics
3.2. Primary Study Outcome: COVID-19 Severity According to Vitamin D Status
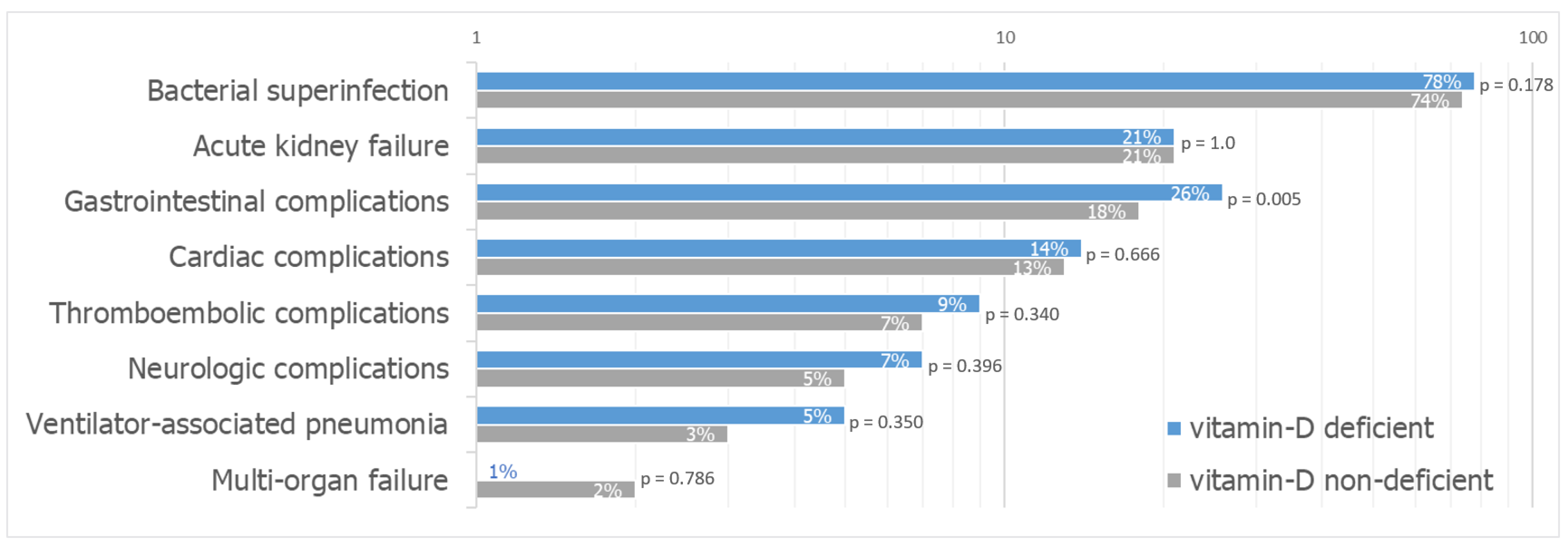
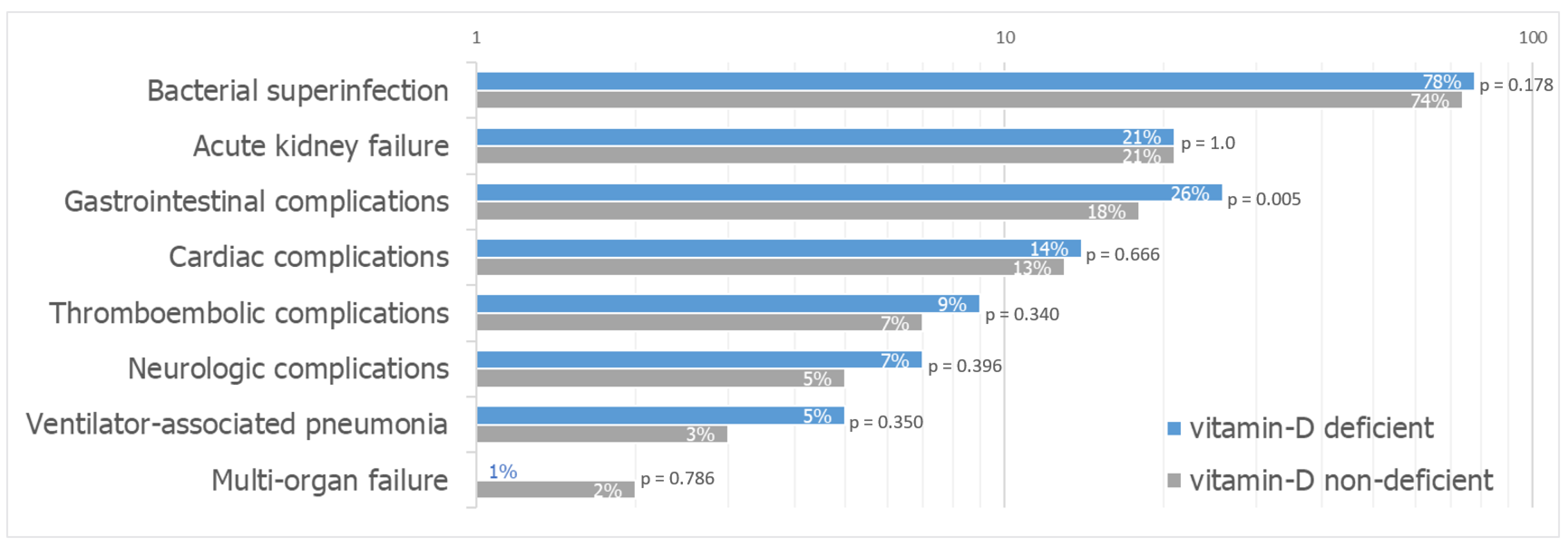
3.3. Secondary Study Outcomes: COVID-19 Clinical Outcome According to Vitamin D Status
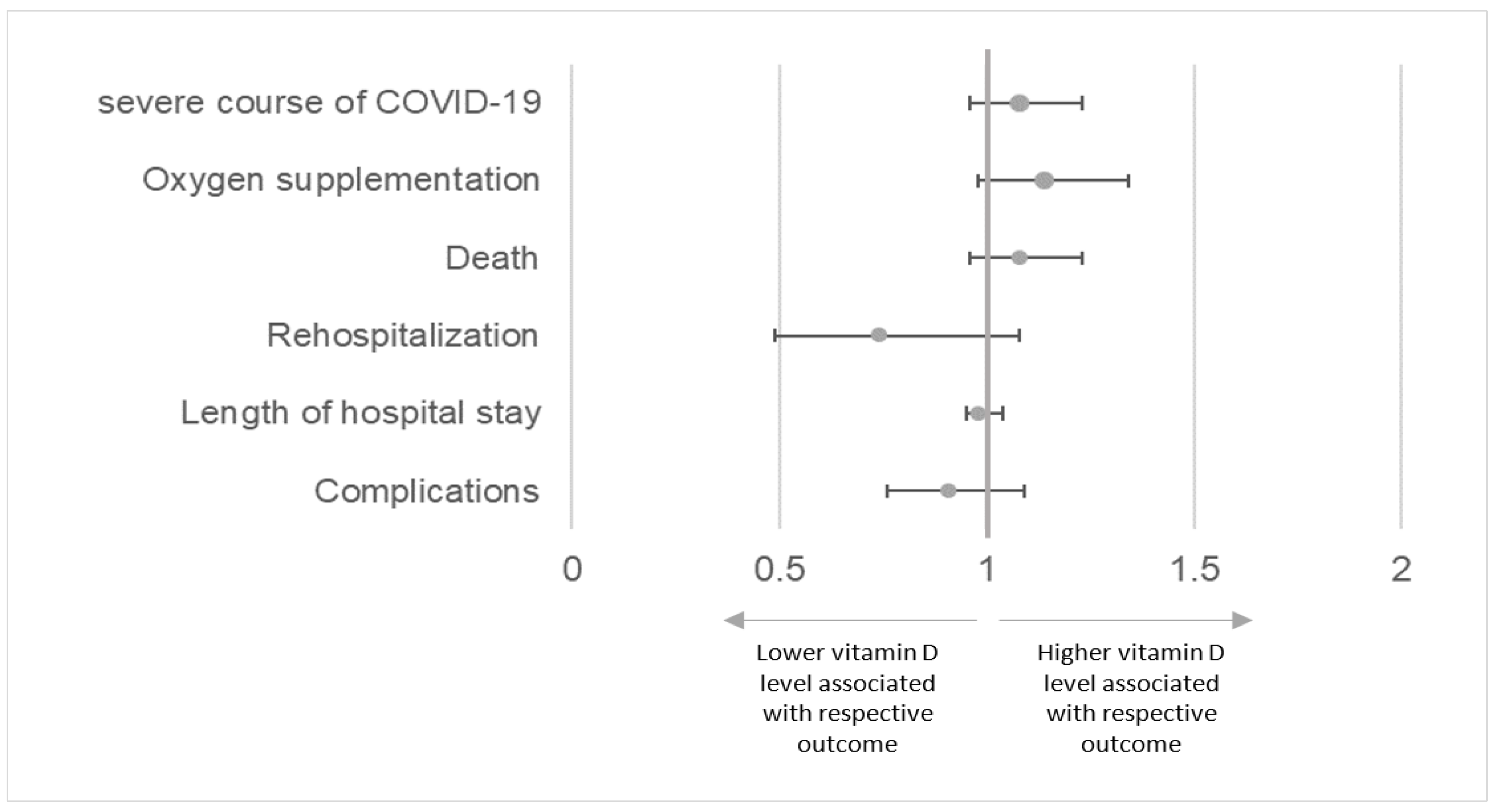
3.4. Multivariable Analysis of Primary and Secondary Study Outcome Measures
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report—51; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. Severe acute respiratory syndrome-related coronavirus: The species and its viruses—A statement of the Coronavirus Study Group. bioRxiv 2020. [Google Scholar] [CrossRef]
- Notz, Q.; Herrmann, J.; Schlesinger, T.; Kranke, P.; Sitter, M.; Helmer, P.; Stumpner, J.; Roeder, D.; Amrein, K.; Stoppe, C.; et al. Vitamin D deficiency in critically ill COVID-19 ARDS patients. Clin. Nutr. 2021, 41, 3089–3095. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Abbas, M.; Robalo Nunes, T.; Martischang, R.; Zingg, W.; Iten, A.; Pittet, D.; Harbarth, S. Nosocomial transmission and outbreaks of coronavirus disease 2019: The need to protect both patients and healthcare workers. Antimicrob. Resist. Infect. Control 2021, 10, 7. [Google Scholar] [CrossRef]
- John Hopkins University & Medicine. Mortality Analysis. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 16 December 2021).
- Diebold, M.; Martinez, A.E.; Adam, K.M.; Bassetti, S.; Osthoff, M.; Kassi, E.; Steiger, J.; Pargger, H.; Siegemund, M.; Battegay, M.; et al. Temporal trends of COVID-19 related in-hospital mortality and demographics in Switzerland—A retrospective single centre cohort study. Swiss Med. Wkly. 2021, 151, w20572. [Google Scholar] [CrossRef]
- Federal Office of Public Health FOPH. COVID-19 Switzerland, Information on the Current Situation, as of 4 June 2021. Available online: https://www.covid19.admin.ch/de/epidemiologic/case?demoView=graph (accessed on 17 December 2021).
- Holick, M.F. Resurrection of vitamin D deficiency and rickets. J. Clin. Investig. 2006, 116, 2062–2072. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Hribar, C.A.; Cobbold, P.H.; Church, F.C. Potential Role of Vitamin D in the Elderly to Resist COVID-19 and to Slow Progression of Parkinson’s Disease. Brain. Sci. 2020, 10, 284. [Google Scholar] [CrossRef]
- Teymoori-Rad, M.; Shokri, F.; Salimi, V.; Marashi, S.M. The interplay between vitamin D and viral infections. Rev. Med. Virol. 2019, 29, e2032. [Google Scholar] [CrossRef]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Mei, K.; Xie, L.; Yuan, P.; Ma, J.; Yu, P.; Zhu, W.; Zheng, C.; Liu, X. Low vitamin D levels do not aggravate COVID-19 risk or death, and vitamin D supplementation does not improve outcomes in hospitalized patients with COVID-19: A meta-analysis and GRADE assessment of cohort studies and RCTs. Nutr. J. 2021, 20, 89. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.; Solway, J. Association of Vitamin D Status and Other Clinical Characteristics with COVID-19 Test Results. JAMA Netw. Open 2020, 3, e2019722. [Google Scholar] [CrossRef]
- Mendy, A.; Apewokin, S.; Wells, A.A.; Morrow, A.L. Factors Associated with Hospitalization and Disease Severity in a Racially and Ethnically Diverse Population of COVID-19 Patients. medRxiv 2020. [Google Scholar] [CrossRef]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. [Google Scholar] [CrossRef]
- Hastie, C.E.; Pell, J.P.; Sattar, N. Vitamin D and COVID-19 infection and mortality in UK Biobank. Eur. J. Nutr. 2021, 60, 545–548. [Google Scholar] [CrossRef]
- Angelidi, A.M.; Belanger, M.J.; Lorinsky, M.K.; Karamanis, D.; Chamorro-Pareja, N.; Ognibene, J.; Palaiodimos, L.; Mantzoros, C.S. Vitamin D Status Is Associated with In-Hospital Mortality and Mechanical Ventilation: A Cohort of COVID-19 Hospitalized Patients. Mayo Clin. Proc. 2021, 96, 875–886. [Google Scholar] [CrossRef]
- Karahan, S.; Katkat, F. Impact of Serum 25(OH) Vitamin D Level on Mortality in Patients with COVID-19 in Turkey. J. Nutr. Health Aging 2021, 25, 189–196. [Google Scholar] [CrossRef]
- Charoenngam, N.; Shirvani, A.; Reddy, N.; Vodopivec, D.M.; Apovian, C.M.; Holick, M.F. Association of Vitamin D Status with Hospital Morbidity and Mortality in Adult Hospitalized Patients with COVID-19. Endocr. Pract. 2021, 27, 271–278. [Google Scholar] [CrossRef]
- AlSafar, H.; Grant, W.B.; Hijazi, R.; Uddin, M.; Alkaabi, N.; Tay, G.; Mahboub, B.; Al Anouti, F. COVID-19 Disease Severity and Death in Relation to Vitamin D Status among SARS-CoV-2-Positive UAE Residents. Nutrients 2021, 13, 1714. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Di Lecce, V.; Quaranta, V.N.; Zito, A.; Buonamico, E.; Capozza, E.; Palumbo, A.; Di Gioia, G.; Valerio, V.N.; Resta, O. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J. Endocrinol. Investig. 2021, 44, 765–771. [Google Scholar] [CrossRef] [PubMed]
- De Smet, D.; De Smet, K.; Herroelen, P.; Gryspeerdt, S.; Martens, G.A. Serum 25(OH)D Level on Hospital Admission Associated with COVID-19 Stage and Mortality. Am. J. Clin. Pathol. 2021, 155, 381–388. [Google Scholar] [CrossRef]
- Hastie, C.E.; Mackay, D.F.; Ho, F.; Celis-Morales, C.A.; Katikireddi, S.V.; Niedzwiedz, C.L.; Jani, B.D.; Welsh, P.; Mair, F.S.; Gray, S.R.; et al. Corrigendum to “Vitamin D concentrations and COVID-19 infection in UK Biobank” [Diabetes Metabol Syndr: Clin Res Rev 2020 14 (4) 561–5]. Diabetes Metab. Syndr. 2020, 14, 1315–1316. [Google Scholar] [CrossRef] [PubMed]
- Raisi-Estabragh, Z.; McCracken, C.; Bethell, M.S.; Cooper, J.; Cooper, C.; Caulfield, M.J.; Munroe, P.B.; Harvey, N.C.; Petersen, S.E. Greater risk of severe COVID-19 in Black, Asian and Minority Ethnic populations is not explained by cardiometabolic, socioeconomic or behavioural factors, or by 25(OH)-vitamin D status: Study of 1326 cases from the UK Biobank. J. Public Health 2020, 42, 451–460. [Google Scholar] [CrossRef]
- Dancer, R.C.; Parekh, D.; Lax, S.; D’Souza, V.; Zheng, S.; Bassford, C.R.; Park, D.; Bartis, D.G.; Mahida, R.; Turner, A.M.; et al. Vitamin D deficiency contributes directly to the acute respiratory distress syndrome (ARDS). Thorax 2015, 70, 617–624. [Google Scholar] [CrossRef]
- Jaun, F.; Boesing, M.; Luthi-Corridori, G.; Abig, K.; Makhdoomi, A.; Bloch, N.; Lins, C.; Raess, A.; Grillmayr, V.; Haas, P.; et al. High-dose vitamin D substitution in patients with COVID-19: Study protocol for a randomized, double-blind, placebo-controlled, multi-center study-VitCov Trial. Trials 2022, 23, 114. [Google Scholar] [CrossRef]
- Bergman, P.; Lindh, A.U.; Bjorkhem-Bergman, L.; Lindh, J.D. Vitamin D and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2013, 8, e65835. [Google Scholar] [CrossRef]
- Sabico, S.; Enani, M.A.; Sheshah, E.; Aljohani, N.J.; Aldisi, D.A.; Alotaibi, N.H.; Alshingetti, N.; Alomar, S.Y.; Alnaami, A.M.; Amer, O.E.; et al. Effects of a 2-Week 5000 IU versus 1000 IU Vitamin D3 Supplementation on Recovery of Symptoms in Patients with Mild to Moderate Covid-19: A Randomized Clinical Trial. Nutrients 2021, 13, 2170. [Google Scholar] [CrossRef]
- Amrein, K.; Schnedl, C.; Holl, A.; Riedl, R.; Christopher, K.B.; Pachler, C.; Urbanic Purkart, T.; Waltensdorfer, A.; Munch, A.; Warnkross, H.; et al. Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vitamin D deficiency: The VITdAL-ICU randomized clinical trial. JAMA 2014, 312, 1520–1530. [Google Scholar] [CrossRef]
- Marshall, J.C.; Murthy, S.; Diaz, J.; Adhikari, N.K.; Angus, D.C.; Arabi, Y.M.; Baillie, K.; Bauer, M.; Berry, S.; Blackwood, B.; et al. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Mineva, E.M.; Schleicher, R.L.; Chaudhary-Webb, M.; Maw, K.L.; Botelho, J.C.; Vesper, H.W.; Pfeiffer, C.M. A candidate reference measurement procedure for quantifying serum concentrations of 25-hydroxyvitamin D(3) and 25-hydroxyvitamin D(2) using isotope-dilution liquid chromatography-tandem mass spectrometry. Anal. Bioanal. Chem. 2015, 407, 5615–5624. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D status: Measurement, interpretation, and clinical application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Bess Dawson-Hughes, M. Patient Education: Vitamin D Deficiency (Beyond the Basics). Available online: https://www.uptodate.com/contents/vitamin-d-deficiency-beyond-the-basics (accessed on 16 August 2023).
- Brigham and Women’s Hospital. COVID Protocols—Treatments. Available online: https://covidprotocols.org/en/chapters/treatments/ (accessed on 15 June 2022).
- National Institutes of Health. COVID-19 Treatment Guidelines—Therapies. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/ (accessed on 15 June 2022).
- Hernandez, J.L.; Nan, D.; Fernandez-Ayala, M.; Garcia-Unzueta, M.; Hernandez-Hernandez, M.A.; Lopez-Hoyos, M.; Munoz-Cacho, P.; Olmos, J.M.; Gutierrez-Cuadra, M.; Ruiz-Cubillan, J.J.; et al. Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection. J. Clin. Endocrinol. Metab. 2021, 106, e1343–e1353. [Google Scholar] [CrossRef]
- Im, J.H.; Je, Y.S.; Baek, J.; Chung, M.H.; Kwon, H.Y.; Lee, J.S. Nutritional status of patients with COVID-19. Int. J. Infect. Dis. 2020, 100, 390–393. [Google Scholar] [CrossRef]
- Georgoulis, M.; Kontogianni, M.D.; Kechribari, I.; Tenta, R.; Fragopoulou, E.; Lamprou, K.; Perraki, E.; Vagiakis, E.; Yiannakouris, N. Associations between serum vitamin D status and the cardiometabolic profile of patients with obstructive sleep apnea. Hormones 2023. [Google Scholar] [CrossRef]
- Drame, M.; Cofais, C.; Hentzien, M.; Proye, E.; Coulibaly, P.S.; Demoustier-Tampere, D.; Destailleur, M.H.; Lotin, M.; Cantagrit, E.; Cebille, A.; et al. Relation between Vitamin D and COVID-19 in Aged People: A Systematic Review. Nutrients 2021, 13, 1339. [Google Scholar] [CrossRef]
- Kazemi, A.; Mohammadi, V.; Aghababaee, S.K.; Golzarand, M.; Clark, C.C.T.; Babajafari, S. Association of Vitamin D Status with SARS-CoV-2 Infection or COVID-19 Severity: A Systematic Review and Meta-analysis. Adv. Nutr. 2021, 12, 1636–1658. [Google Scholar] [CrossRef]
- Reis, B.Z.; Fernandes, A.L.; Sales, L.P.; Santos, M.D.; Dos Santos, C.C.; Pinto, A.J.; Goessler, K.F.; Franco, A.S.; Duran, C.S.C.; Silva, C.B.R.; et al. Influence of vitamin D status on hospital length of stay and prognosis in hospitalized patients with moderate to severe COVID-19: A multicenter prospective cohort study. Am. J. Clin. Nutr. 2021, 114, 598–604. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Kostenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.M.; Grandoff, P.G.; Schneider, S.T. Vitamin D Intake and Factors Associated with Self-Reported Vitamin D Deficiency Among US Adults: A 2021 Cross-Sectional Study. Front. Nutr. 2022, 9, 899300. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.C.; Jindal, P.S.; Smith, L.M. Vitamin D supplementation in young White and African American women. J. Bone Miner. Res. 2014, 29, 173–181. [Google Scholar] [CrossRef]
- Bahar-Shany, K.; Ravid, A.; Koren, R. Upregulation of MMP-9 production by TNFalpha in keratinocytes and its attenuation by vitamin D. J. Cell Physiol. 2010, 222, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Barlow, P.G.; Beaumont, P.E.; Cosseau, C.; Mackellar, A.; Wilkinson, T.S.; Hancock, R.E.; Haslett, C.; Govan, J.R.; Simpson, A.J.; Davidson, D.J. The human cathelicidin LL-37 preferentially promotes apoptosis of infected airway epithelium. Am. J. Respir. Cell Mol. Biol. 2010, 43, 692–702. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Chen, Q.; Schmidt, A.P.; Anderson, G.M.; Wang, J.M.; Wooters, J.; Oppenheim, J.J.; Chertov, O. Ll-37, the Neutrophil Granule–And Epithelial Cell–Derived Cathelicidin, Utilizes Formyl Peptide Receptor–Like 1 (Fprl1) as a Receptor to Chemoattract Human Peripheral Blood Neutrophils, Monocytes, and T Cells. J. Exp. Med. 2000, 192, 1069–1074. [Google Scholar] [CrossRef]
- Syed Mohd, S.S.; Mishra, A.; Ashraf, M.Z. Vitamin D and Its Relationship with the Pathways Related to Thrombosis and Various Diseases. In Vitamin D; IntechOpen: London, UK, 2021. [Google Scholar]
- Wu, Z.; Liu, D.; Deng, F. The Role of Vitamin D in Immune System and Inflammatory Bowel Disease. J. Inflamm. Res. 2022, 15, 3167–3185. [Google Scholar] [CrossRef]
- Ko, K.H.; Kim, Y.S.; Lee, B.K.; Choi, J.H.; Woo, Y.M.; Kim, J.Y.; Moon, J.S. Vitamin D deficiency is associated with disease activity in patients with Crohn’s disease. Intest. Res. 2019, 17, 70–77. [Google Scholar] [CrossRef]
- Ulitsky, A.; Ananthakrishnan, A.N.; Naik, A.; Skaros, S.; Zadvornova, Y.; Binion, D.G.; Issa, M. Vitamin D deficiency in patients with inflammatory bowel disease: Association with disease activity and quality of life. J. Parenter. Enteral. Nutr. 2011, 35, 308–316. [Google Scholar] [CrossRef]
- Calabrese, E.; Zorzi, F.; Monteleone, G.; Del Vecchio Blanco, G. Onset of ulcerative colitis during SARS-CoV-2 infection. Dig. Liver Dis. 2020, 52, 1228–1229. [Google Scholar] [CrossRef]
- de-Madaria, E.; Capurso, G. COVID-19 and acute pancreatitis: Examining the causality. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 3–4. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mild | Hospitalised without oxygen therapy |
| Moderate | Hospitalised with oxygen by a nasal prong or mask |
| Severe | Hospitalised with oxygen by non-invasive ventilation (NIV) or high-flow nasal oxygen (HFNO) |
| Critical | Hospitalised and intubated, incl. patients with additional organ support (dialysis, extracorporeal membrane oxygenation (ECMO), vasoactive drugs) |
| Dead |
| First wave | 27 February 2020 to 30 June 2020 |
| Second wave | 1 July 2020 to 28 February 2021 |
| Third wave | 1 March 2021 to 30 June 2021 |
| Fourth wave | 1 July 2021 to 15 October 2022 |
| Fifth wave | 16 October 2021 to 31 December 2021 |
| Total Study Population | Vitamin D Deficient (<50 nmol/L) | Vitamin D Non-Deficient (≥50 nmol/L) | p-Value | |
|---|---|---|---|---|
| n (%) | 763 (100) | 343 (47) | 420 (53) | |
| Age (years), mean ± SD | 65.28 ± 16.36 | 64.09 ± 17.27 | 66.26 ± 15.53 | 0.068 |
| Sex female, n (%) | 329 (43.1) | 121 (35.3) | 208 (49.5) | <0.001 *** |
| BMI (kg/m2) mean ± SD | 28.18 ± 5.45 | 28.95 ± 5.72 | 27.56 ± 5.14 | 0.002 ** |
| Smoking status | 0.409 | |||
| Non-smoker, n (%) | 107 (14.0) | 50 (14.6) | 57 (13.6) | |
| Smoker, n (%) | 28 (3.7) | 11 (3.2) | 17 (4.0) | |
| Former smoker, n (%) | 98 (12.8) | 51 (14.9) | 47 (11.2) | |
| Unknown, n (%) | 530 (69.5) | 231 (67.3) | 299 (71.2) | |
| Pack years, median (IQR) | 40 (23.5–52.3) | 40 (25–52.5) | 37.5 (20.8–52.3) | 0.504 ‡ |
| Patients with comorbidity, n (%) | 642 (84.1) | 295 (86) | 347 (82.6) | 0.240 |
| Number of comorbidities, median (IQR) | 3 (2–4) | 3 (2–4) | 3 (2–4) | 0.212 ‡ |
| Arterial hypertension, n (%) | 360 (47.2) | 160 (46.6) | 200 (47.6) | 0.846 |
| Cardiac diseases, n (%) | 231 (30.3) | 112 (32.7) | 119 (28.3) | 0.225 |
| Obesity, n (%) | 225 (29.7) | 116 (34.2) | 109 (26.1) | 0.018 * |
| Diabetes, n (%) | 166 (21.8) | 83 (24.2) | 83 (19.8) | 0.165 |
| Chronic respiratory diseases, n (%) | 172 (22.5) | 83 (24.2) | 89 (21.2) | 0.367 |
| Immunosuppression, n (%) | 60 (7.9) | 18 (5.2) | 42 (10) | 0.022 * |
| Chronic kidney diseases, n (%) | 161 (21.1) | 74 (21.6) | 87 (20.7) | 0.825 |
| Thyroid diseases, n (%) | 93 (12.2) | 33 (9.6) | 60 (14.3) | 0.065 |
| Malignant diseases, n (%) | 100 (13.1) | 40 (11.7) | 60 (14.3) | 0.337 |
| Active Cancer, n (%) | 32 (4.2) | 11 (3.2) | 21 (5) | 0.295 |
| Chronic liver diseases, n (%) | 58 (7.6) | 27 (7.9) | 31 (7.4) | 0.907 |
| Neurological disorders, n (%) | 196 (25.7) | 73 (21.3) | 123 (29.3) | 0.015 * |
| Electrolyte imbalance, n (%) | 181 (23.7) | 75 (21.9) | 106 (25.2) | 0.315 |
| COVID-19 vaccination status | 661 (87) | 0.156 | ||
| Negative (unvaccinated), n (%) | 616 (81) | 262 (76) | 354 (84) | |
| Positive (vaccinated), n (%) | 45 (6.8) | 23 (8.1) | 22 (5.9) | |
| Time between vaccination and admission (days), median (IQR) | 63 (12.5–200.5) | 95.5 (10–214.5) | 46 (13–183) | 0.978 ‡ |
| 25-hydroxy vitamin D measured 5 days before admission or during admission, n (%), mean | 751 (98.4) | 339 (98.8) | 412 (98.1) | 0.601 |
| Total | Vitamin D Deficient (<50 nmol/L) | Vitamin D Non-Deficient (≥50 nmol/L) | p-Value | |
|---|---|---|---|---|
| n (%) | 763 (100) | 343 (45) | 420 (55) | |
| COVID-19 severity category | 763 (100) | 0.561 a | ||
| Mild, n (%) | 255 (33.4) | 112 (32.7) | 143 (34) | |
| Moderate, n (%) | 374 (49) | 166 (48.4) | 208 (49.5) | |
| Severe, n (%) | 27 (3.5) | 11 (3.2) | 16 (3.8) | |
| Critical, n (%) | 38 (5) | 22 (6.4) | 16 (3.8) | |
| Death, n (%) | 69 (9) | 32 (9.3) | 37 (8.8) | |
| Oxygen supplementation, n (%) | 508 (66.6) | 231 (67.3) | 277 (66) | 0.742 a |
| Death, n (%) | 69 (9) | 32 (9.3) | 37 (8.8) | 0.903 a |
| COVID-19-related complications | 647 (84.8) | 306 (89.2) | 341 (81.2) | 0.003 a |
| Length of hospital stay alive (LOS) (days), median (IQR) | 7 (4–11) | 7 (4–11) | 7 (4–11) | 0.865 b |
| Rehospitalised at KSBL within 30 days, n (%) | 32 (4.2) | 17 (5) | 15 (3.6) | 0.443 a |
| Serum Vitamin D (nmol/L), Median (IQR) | p-Value | |
|---|---|---|
| COVID-19 severity | ||
| Mild | 55 (36–76) | |
| Moderate | 54 (36–76) | |
| Severe | 55 (36–73) | 0.649 ₤ |
| Critical | 45 (34–71) | |
| Dead | 51 (29–82) | |
| Oxygen supplementation | ||
| Yes | 53 (36–76) | 0.837 ‡ |
| No | 55 (35–76) | |
| Death | ||
| Yes | 51 (29–82) | 0.836 ‡ |
| No | 54 (35–74) | |
| Rehospitalisation at KSBL within 30 days | ||
| Yes | 45 (32–73) | 0.402 ‡ |
| No | 54 (36–76) | |
| Length of hospital stay | ||
| 1–3 days | 52 (38–79) | 0.942 ₤ |
| 4–7 days | 56 (37–74) | |
| 8–13 days | 52 (34–71) | |
| 14–21 days | 55 (36–78) | |
| 22–28 days | 52 (36–86) | |
| >28 days | 50 (38–70) | |
| COVID-19-related complications | ||
| Yes | 52 (43–82) | 0.016 ‡* |
| No | 64 (35–74) | |
| Total | Vitamin D Deficient (<50 nmol/L) | Vitamin D Non-Deficient (≥50 nmol/L) | |
|---|---|---|---|
| n (%) | 763 (100) | 343 (45) | 420 (55) |
| Antibiotics, n (%) | 592 (78) | 264 (77) | 328 (78) |
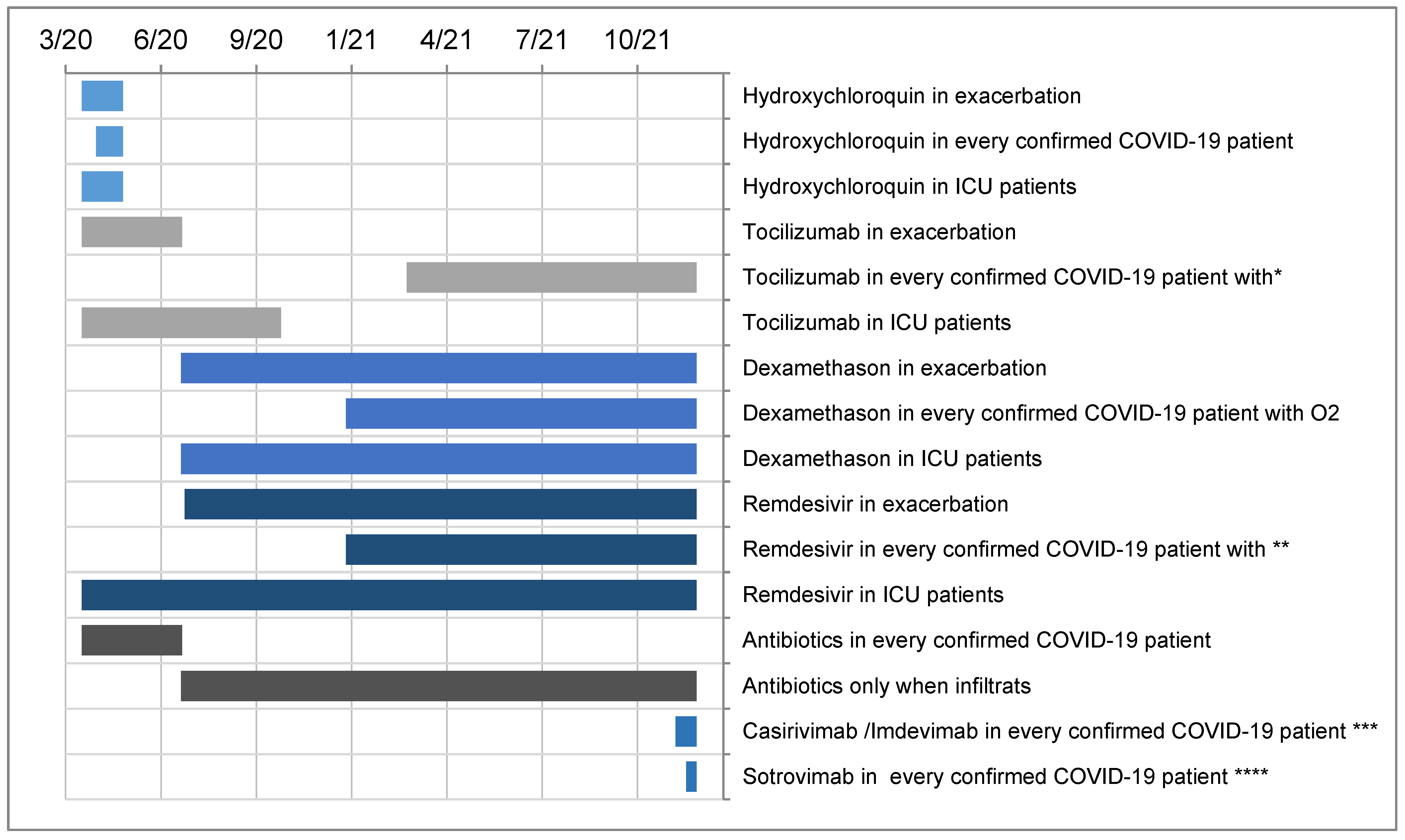
| Specific COVID-19 therapy, n (%) | 513 (67) | 236 (69) | 277 (66) |
| Anticoagulants and platelet aggregation inhibitors, n (%) | 750 (98) | 336 (98) | 414 (98) |
| Antihypertensive therapy, n (%) | 407 (53) | 167 (49) | 240 (57) |
| Inhalation therapy, n (%) | 239 (31) | 102 (30) | 137 (33) |
| Vitamin D supplementation, n (%) | 279 (37) | 150 (44) | 129 (31) |
| Only before hospitalization, n (%) | 111 (15) | 21 (14) | 90 (70) |
| Only during hospitalization, n (%) | 168 (22) | 129 (86) | 39 (30) |
| No vitamin D supplementation, n (%) | 484 (63) | 193 (56) | 291 (69) |
| Additional Organ Support | 59 (8) | 27 (8) | 32 (8) |
| Dialysis, n (%) | 5 (1) | 1 (4) | 4 (1) |
| Vasoactive drugs, n (%) | 45 (6) | 21 (6) | 24 (6) |
| ECMO, n (%) | 9 (1) | 5 (19) | 4 (1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mbata, M.K.; Hunziker, M.; Makhdoomi, A.; Lüthi-Corridori, G.; Boesing, M.; Giezendanner, S.; Muser, J.; Leuppi-Taegtmeyer, A.B.; Leuppi, J.D. Is Serum 25-Hydroxyvitamin D Level Associated with Severity of COVID-19? A Retrospective Study. J. Clin. Med. 2023, 12, 5520. https://doi.org/10.3390/jcm12175520
Mbata MK, Hunziker M, Makhdoomi A, Lüthi-Corridori G, Boesing M, Giezendanner S, Muser J, Leuppi-Taegtmeyer AB, Leuppi JD. Is Serum 25-Hydroxyvitamin D Level Associated with Severity of COVID-19? A Retrospective Study. Journal of Clinical Medicine. 2023; 12(17):5520. https://doi.org/10.3390/jcm12175520
Chicago/Turabian StyleMbata, Munachimso Kizito, Mireille Hunziker, Anja Makhdoomi, Giorgia Lüthi-Corridori, Maria Boesing, Stéphanie Giezendanner, Jürgen Muser, Anne B. Leuppi-Taegtmeyer, and Jörg D. Leuppi. 2023. "Is Serum 25-Hydroxyvitamin D Level Associated with Severity of COVID-19? A Retrospective Study" Journal of Clinical Medicine 12, no. 17: 5520. https://doi.org/10.3390/jcm12175520
APA StyleMbata, M. K., Hunziker, M., Makhdoomi, A., Lüthi-Corridori, G., Boesing, M., Giezendanner, S., Muser, J., Leuppi-Taegtmeyer, A. B., & Leuppi, J. D. (2023). Is Serum 25-Hydroxyvitamin D Level Associated with Severity of COVID-19? A Retrospective Study. Journal of Clinical Medicine, 12(17), 5520. https://doi.org/10.3390/jcm12175520