
Characterization of Immunogenicity and Safety of COVID-19 mRNA-1273 in HIV-Positive Italian Patients with Hemophilia: A Prospective Single-Center Cohort Study

 ,
,  ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Laboratory Measurements
2.4. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chavda, V.P.; Vuppu, S.; Mishra, T.; Kamara, S.; Patel, A.B.; Sharma, N.; Chen, Z.S. Recent review of COVID-19 management: Diagnosis, treatment and vaccination. Pharmacol. Rep. 2022, 74, 1120–1148. [Google Scholar] [CrossRef] [PubMed]
- EMA, European Medicines Agency. Committee for Medicinal Products for Human Use (CHMP). Assessment Report—COVID-19 Vaccine Moderna. 11 March 2021 EMA/15689/2021. 2021. Available online: https://www.ema.europa.eu/en/documents/assessment-report/covid-19-vaccine-moderna-epar-public-assessment-report_en.pdf (accessed on 6 June 2023).
- Peck, R.C.; Clark, A.; Shapiro, S. Experience of COVID 19 vaccination in patients with bleeding disorders. Haemophilia 2022, 28, e9–e11. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarek, R.; El Ekiaby, M.; Hart, D.P.; Hermans, C.; Makris, M.; Noone, D.; O’Mahony, B.; Page, D.; Peyvandi, F.; Pipe, S.W.; et al. Vaccination against COVID-19: Rationale, modalities and precautions for patients with haemophilia and other inherited bleeding disorders. Haemophilia 2021, 27, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Pfrepper, C.; Holstein, K.; Königs, C.; Heller, C.; Krause, M.; Olivieri, M.; Bidlingmaier, C.; Sigl-Kraetzig, M.; Wendisch, J.; Halimeh, S.; et al. Consensus Recommendations for Intramuscular COVID-19 Vaccination in Patients with Hemophilia. Hamostaseologie 2021, 41, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Kocher, F.; Seeber, A.; Fauser, J.; Petzer, V.; Wolf, D.; Feistritzer, C. High SARS-CoV-2 vaccination coverage but still room for improvement in patients with haemophila: A single-centre analysis. Haemophilia 2022, 28, e71–e72. [Google Scholar] [CrossRef] [PubMed]
- Tiede, A.; Leise, H.; Horneff, S.; Oldenburg, J.; Halimeh, S.; Heller, C.; Königs, C.; Holstein, K.; Pfrepper, C. Safety of intramuscular COVID-19 vaccination in patients with haemophilia. Haemophilia 2022, 28, 687–693. [Google Scholar] [CrossRef]
- Tesoriero, J.M.; Swain, C.A.E.; Pierce, J.L.; Zamboni, L.; Wu, M.; Holtgrave, D.R.; Gonzalez, C.J.; Udo, T.; Morne, J.E.; Hart-Malloy, R.; et al. COVID-19 Outcomes Among persons living With or without diagnosed HIV infection in New York state. JAMA Netw. Open 2021, 4, e2037069. [Google Scholar] [CrossRef]
- Mirzaei, H.; McFarland, W.; Karamouzian, M.; Sharifi, H. COVID-19 among People living with HIV: A systematic review. AIDS Behav. 2021, 25, 85–92. [Google Scholar] [CrossRef]
- Moir, S.; Ho, J.; Malaspina, A.; Wang, W.; DiPoto, A.C.; O’Shea, M.A.; Roby, G.; Kottilil, S.; Arthos, J.; Proschan, M.A.; et al. Evidence for HIV-associated B cell exhaustion in a dysfunctional memory B cell compartment in HIV-infected viremic individuals. J. Exp. Med. 2008, 205, 1797–1805. [Google Scholar] [CrossRef]
- Moir, S.; Malaspina, A.; Ogwaro, K.M.; Donoghue, E.T.; Hallahan, C.W.; Ehler, L.A.; Liu, S.; Adelsberger, J.; Lapointe, R.; Hwu, P.; et al. HIV-1 induces phenotypic and functional perturbations of B cells in chronically infected individuals. Proc. Natl. Acad. Sci. USA 2001, 98, 10362–10367. [Google Scholar] [CrossRef]
- Liechti, T.; Kadelka, C.; Braun, D.L.; Kuster, H.; Böni, J.; Robbiani, M.; Günthard, H.F.; Trkola, A. Widespread B cell perturbations in HIV-1 infection afflict naive and marginal zone B cells. J. Exp. Med. 2019, 216, 2071–2090. [Google Scholar] [CrossRef]
- Krause, R.; Snyman, J.; Shi-Hsia, H.; Muema, D.; Karim, F.; Ganga, Y.; Ngoepe, A.; Zungu, Y.; Gazy, I.; Bernstein, M.; et al. HIV skews the SARS-CoV-2 B cell response towards an extrafollicular maturation pathway. Elife 2022, 11, e79924. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Farhadian, N.; Sharifi, S.; Taghadosi, M.; Farhadian, M.; Vaziri, S. Humoral immune response to two doses of COVID-19 mRNA-based vaccines in people living with HIV: A systematic review and meta-analysis. Rev. Med. Virol. 2023, 33, e2451. [Google Scholar] [CrossRef]
- Yin, J.; Chen, Y.; Li, Y.; Wang, C.; Zhang, X. Immunogenicity and efficacy of COVID-19 vaccines in people living with HIV: A systematic review and meta-analysis. Int. J. Infect. Dis. 2022, 124, 212–223. [Google Scholar] [CrossRef]
- Chun, H.M.; Milligan, K.; Agyemang, E.; Ford, N.; Rangaraj, A.; Desai, S.; Wilder-Smith, A.; Vitoria, M.; Zulu, I. A Systematic Review of COVID-19 Vaccine Antibody Responses in People with HIV. Open Forum Infect. Dis. 2022, 9, ofac579. [Google Scholar] [CrossRef]
- Kang, L.; Shang, W.; Gao, P.; Wang, Y.; Liu, J.; Liu, M. Immunogenicity and Safety of COVID-19 Vaccines among People Living with HIV: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1569. [Google Scholar] [CrossRef]
- Zhou, Q.; Liu, Y.; Zeng, F.; Meng, Y.; Liu, H.; Deng, G. Correlation between CD4 T-Cell Counts and Seroconversion among COVID-19 Vaccinated Patients with HIV: A Meta-Analysis. Vaccines 2023, 11, 789. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Heidari, S.; Babor, T.F.; De Castro, P.; Tort, S.; Curno, M. Sex and Gender Equity in Research: Rationale for the SAGER guidelines and recommended use. Res. Integr. Peer Rev. 2016, 1, 2. [Google Scholar] [CrossRef] [PubMed]
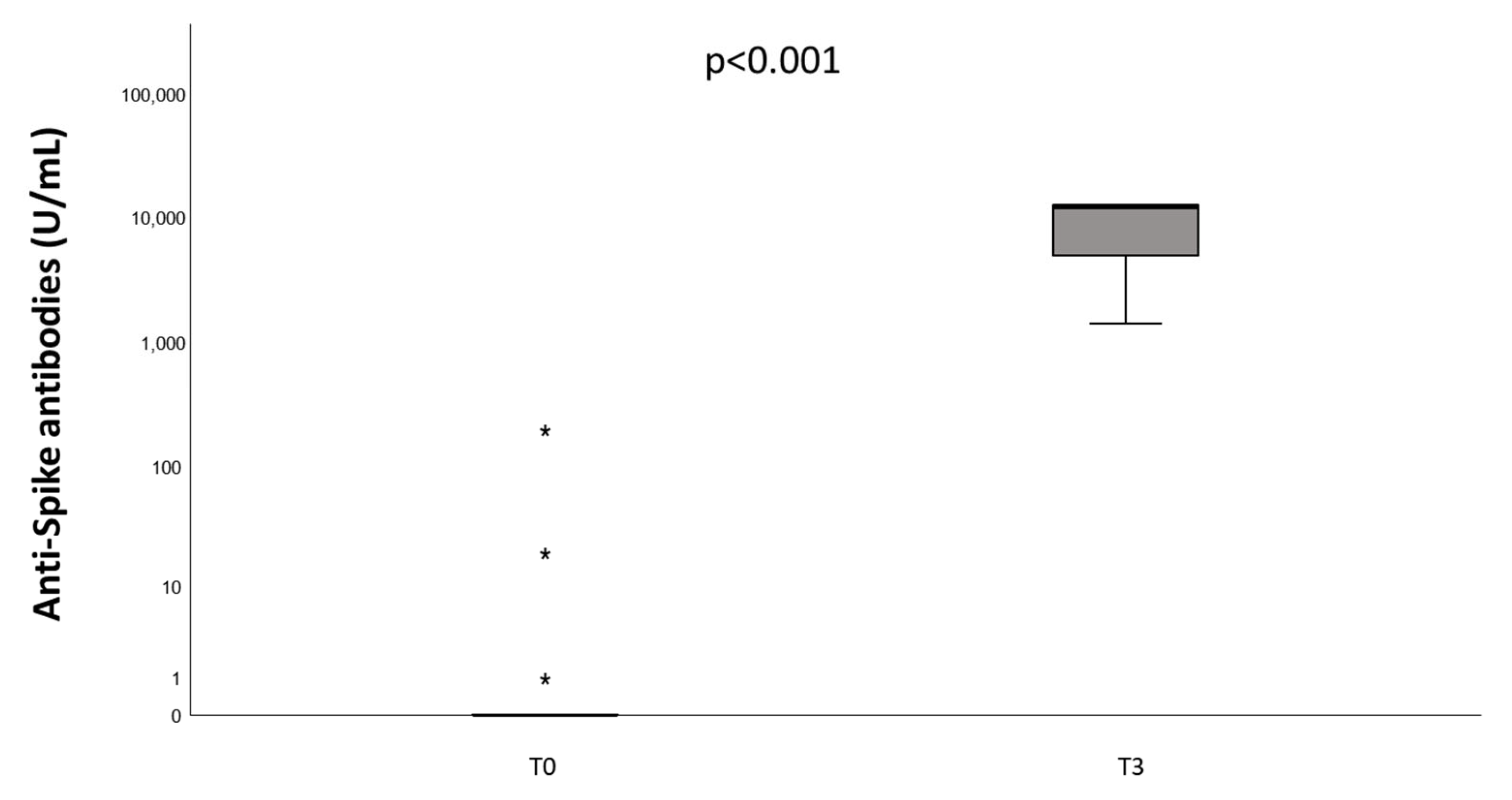
- Lombardi, A.; Butta, G.M.; Donnici, L.; Bozzi, G.; Oggioni, M.; Bono, P.; Matera, M.; Consonni, D.; Ludovisi, S.; Muscatello, A.; et al. Anti-spike antibodies and neutralising antibody activity in people living with HIV vaccinated with COVID-19 mRNA-1273vaccine: A prospective single-centre cohort study. Lancet Reg. Health 2022, 13, 100287. [Google Scholar] [CrossRef]
- Antinori, A.; Cicalini, S.; Meschi, S.; Bordoni, V.; Lorenzini, P.; Vergori, A.; Lanini, S.; De Pascale, L.; Matusali, G.; Mariotti, D.; et al. Humoral and cellular immune response elicited by mRNA vaccination against SARS-CoV-2 in people living with HIV (PLWH) receiving antiretroviral therapy (ART) based on current CD4 T-lymphocyte count. Clin. Infect. Dis. 2022, 75, e552–e563. [Google Scholar] [CrossRef] [PubMed]
- Benet, S.; Blanch-Lombarte, O.; Ainsua-Enrich, E.; Pedreño-Lopez, N.; Muñoz-Basagoiti, J.; Raïch-Regué, D.; Perez-Zsolt, D.; Peña, R.; Jiménez, E.; de la Concepción, M.L.R.; et al. Limited humoral and specific T-cell responses after SARS-CoV-2 vaccination in PLWH with poor immune reconstitution. J. Infect. Dis. 2022, 226, 1913–1923. [Google Scholar] [CrossRef]
- Briggs, C. Quality counts: New parameters in blood cell counting. Int. J. Lab. Hematol. 2009, 31, 277–297. [Google Scholar] [CrossRef]
- Sing, C.W.; Tang, C.T.L.; Chui, C.S.L.; Fan, M.; Lai, F.T.T.; Li, X.; Wan, E.Y.F.; Wong, C.K.H.; Chan, E.W.Y.; Hung, I.F.N.; et al. COVID-19 vaccines and risks of hematological abnormalities: Nested case-control and self-controlled case series study. Am. J. Hematol. 2022, 97, 470–480. [Google Scholar] [CrossRef]
- Cummins, D.; Wilson, M.E.; Foulger, K.J.; Dawson, D.; Hogarth, A.M. Haematological changes associated with influenza vaccination in people aged over 65: Case report and prospective study. Clin. Lab. Haematol. 1998, 20, 285–287. [Google Scholar] [CrossRef]
- Griffin, M.; Makris, M. Vaccination induced neutropenia. Int. J. Lab. Hematol. 2013, 35, e33. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Understanding the Biology of Sex and Gender Differences. Exploring the Biological Contributions to Human Health: Does Sex Matter? Wizemann, T.M., Pardue, M.L., Eds.; National Academies Press: Washington, DC, USA, 2001. Available online: https://www.ncbi.nlm.nih.gov/books/NBK222288/ (accessed on 30 May 2023). [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antiretroviral Treatment Regimen | Number of Patients (%) |
|---|---|
| darunavir + cobicistat + dolutegravir | 5 (21.7) |
| dolutegravir + rilpivirine | 3 (13.0) |
| bictegravir + emtricitabine + tenofovir | 3 (13.0) |
| darunavir + cobicistat + emtricitabine + tenofovir | 2 (8.7) |
| emtricitabine + tenofovir + raltegravir | 2 (8.7) |
| dolutegravir + abacavir + lamivudine | 1 (4.3) |
| darunavir + cobicistat | 1 (4.3) |
| ritonavir + darunavir + emtricitabine + tenofovir | 1 (4.3) |
| dolutegravir + ritonavir + darunavir | 1 (4.3) |
| abacavir + lamivudine + nevirapine | 1 (4.3) |
| lamivudine + zidovudine + dolutegravir | 1 (4.3) |
| abacavir + lamivudine + efavirenz | 1 (4.3) |
| emtricitabine + rilpivirine + tenofovir | 1 (4.3) |
| T0 (N = 22) | Female Patient T0 | T3 (N = 22) | Female Patient T3 | |
|---|---|---|---|---|
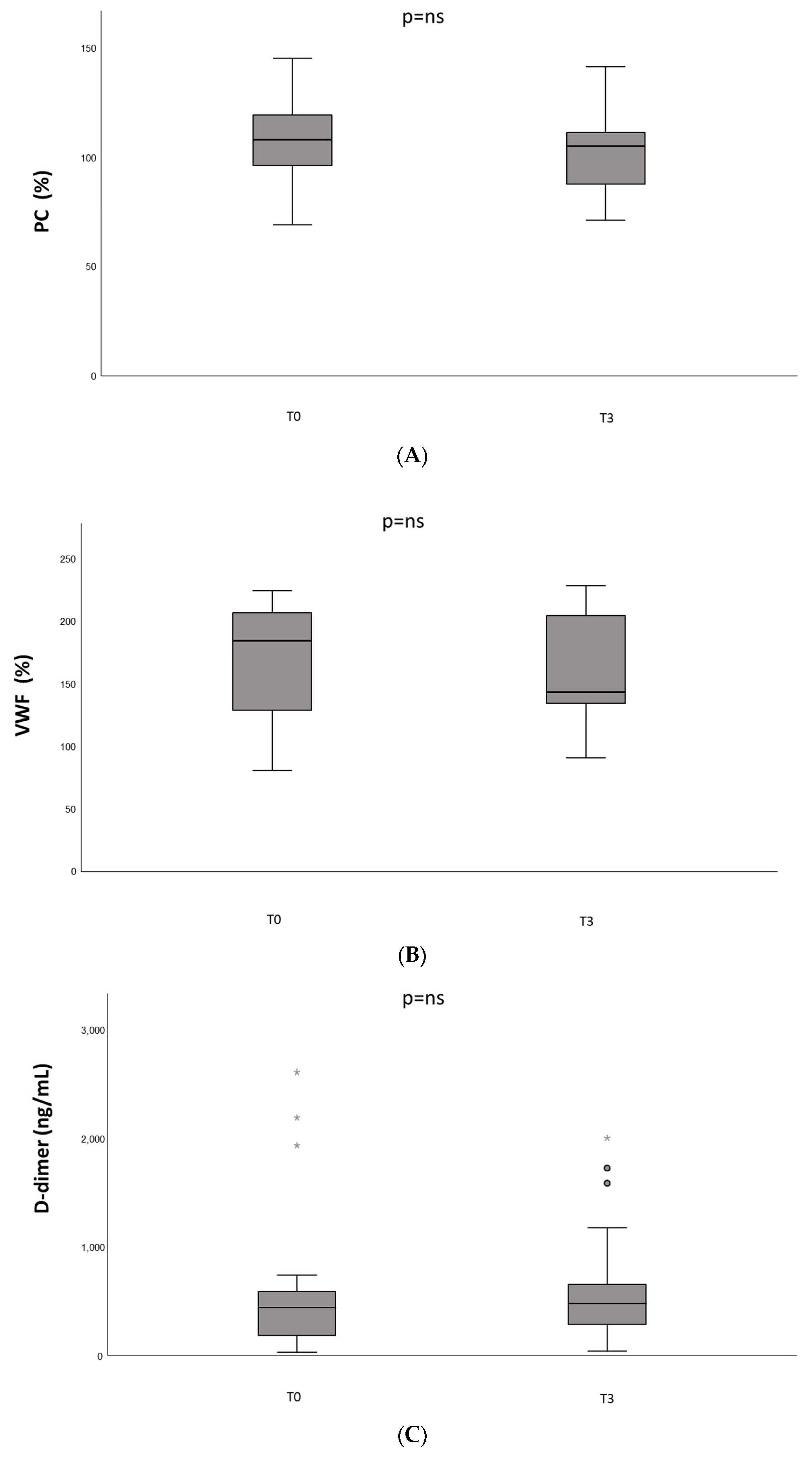
| Protein C (%) | 107 ± 21 | 83 | 103 ± 20 | 79 |
| VWF (%) | 171 ± 46 | 183 | 164 ± 44 | 139 |
| D-dimer (ng/mL) | 460 (625–203) | 28 | 490 (693–299) | 40 |
| Platelets (109/L) | 223 ± 71 | 283 | 231 ± 74 | 274 |
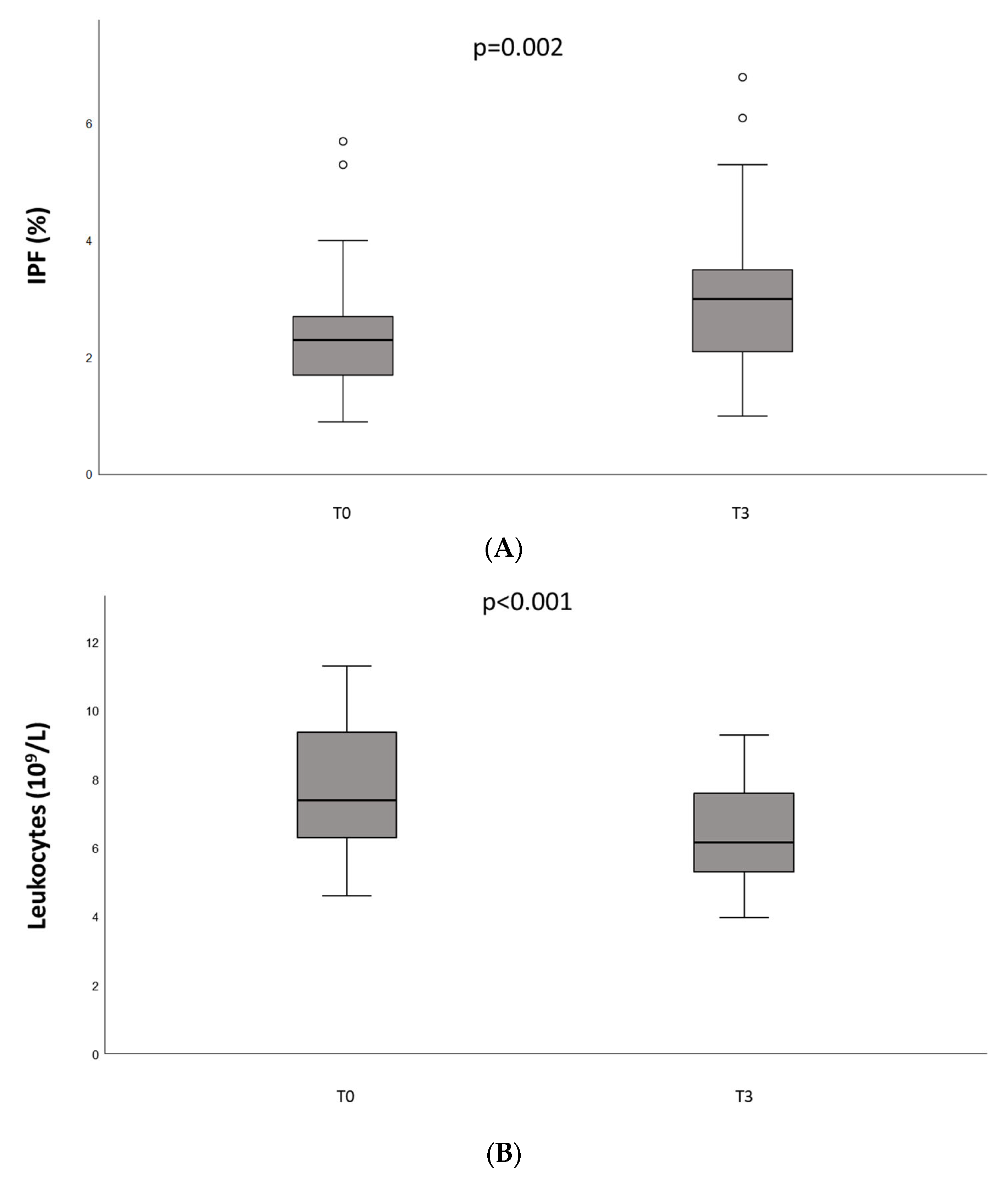
| IPF (%) | 2.6 ± 1.3 | 3.1 | 3.1 ± 1.5 | 5.0 |
| Leukocytes (109/L) | 7.64 ± 1.94 | 10.24 | 6.31 ± 1.55 | 7.08 |
| Lymphocytes (103/µL) | 2.22 ± 0.89 | 3.39 | 2.10 ± 0.92 | 3.40 |
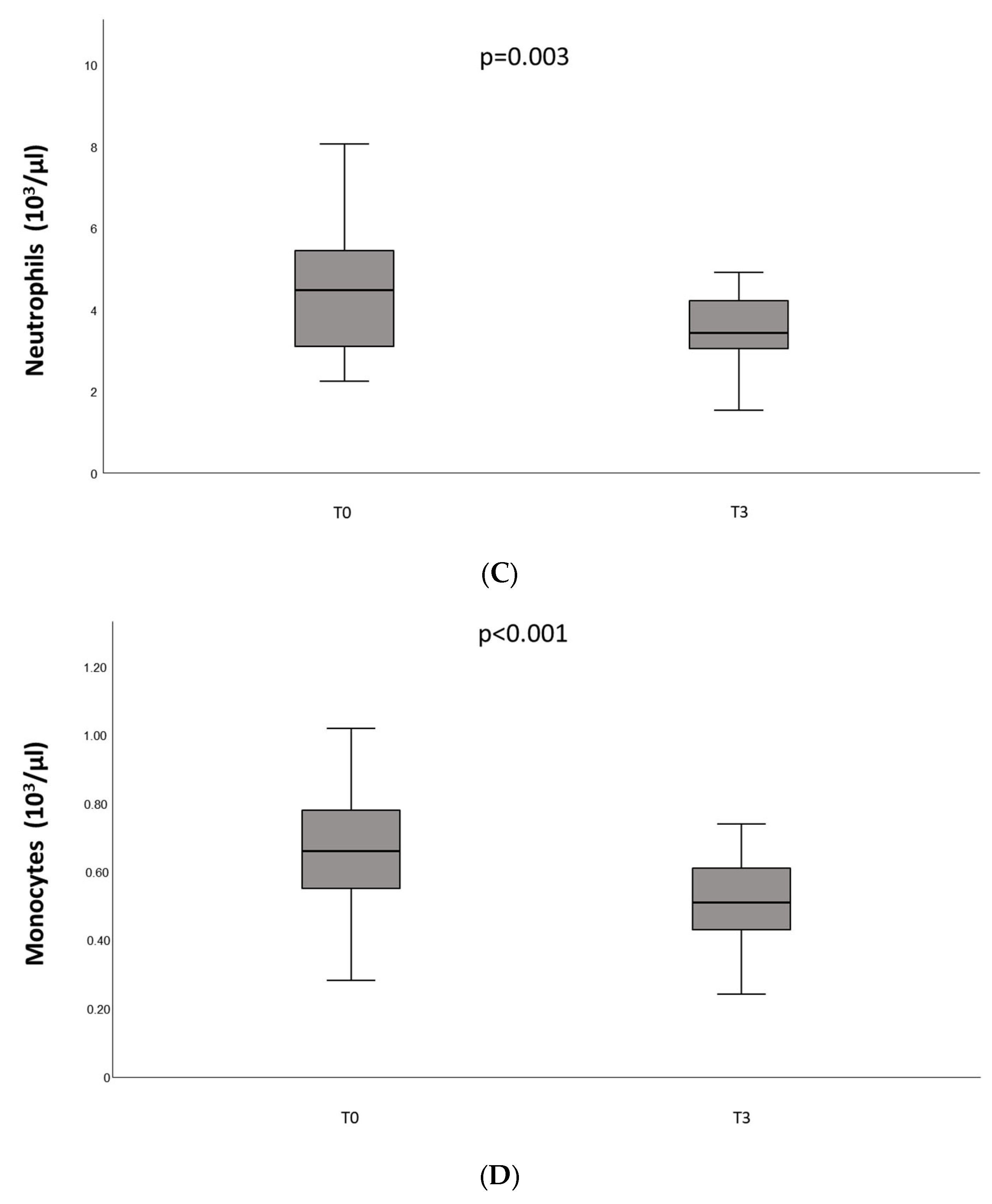
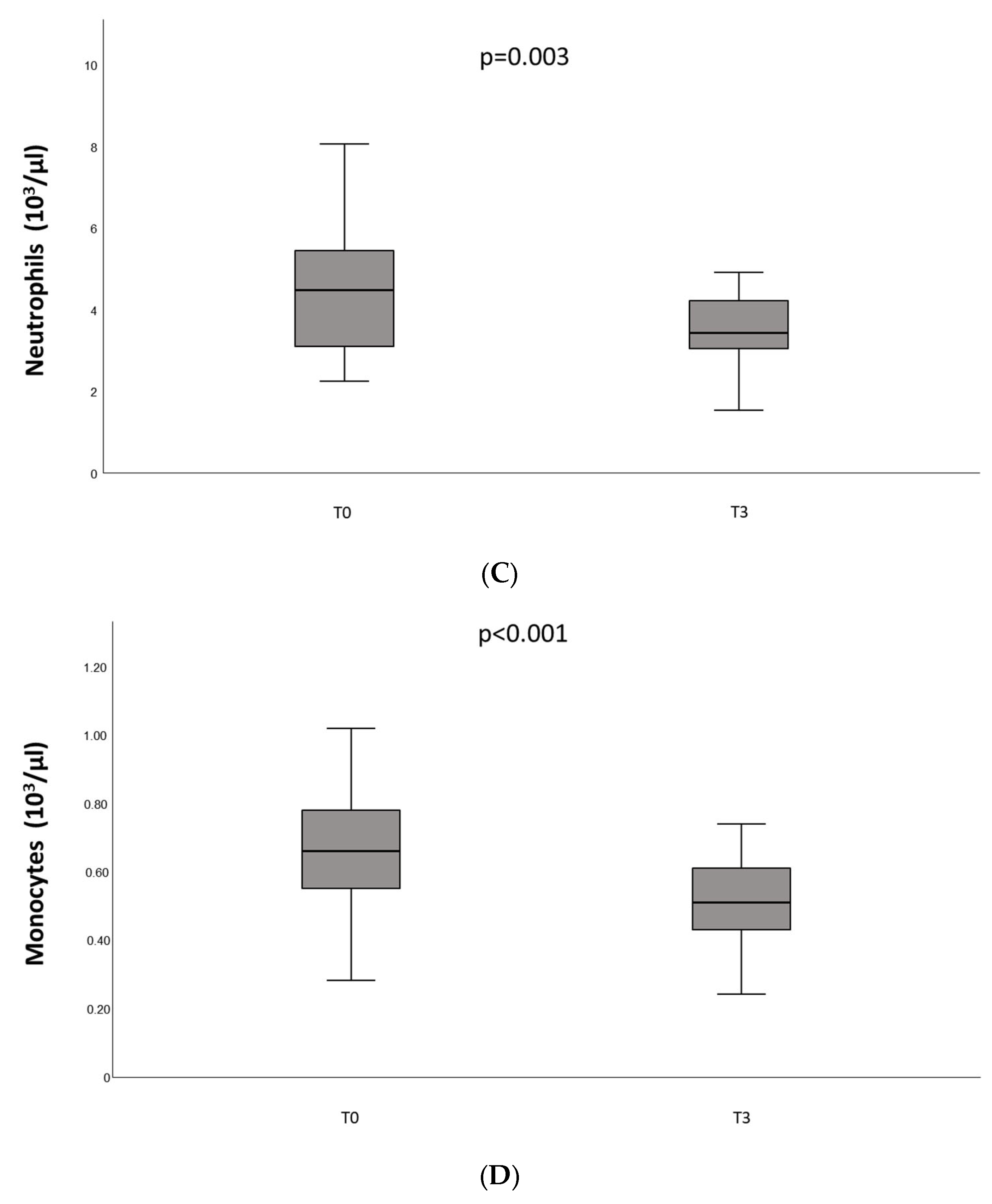
| Neutrophils (103/µL) | 4.58 ± 1.70 | 5.85 | 3.52 ± 0.82 | 2.93 |
| Monocytes (103/µL) | 0.65 ± 0.21 | 0.86 | 0.51 ± 0.14 | 0.64 |
| Eosinophils (103/µL) | 0.14 ± 0.10 | 0.09 | 0.14 ± 0.08 | 0.07 |
| Basophils (103/µL) | 0.04 ± 0.02 | 0.05 | 0.04 ± 0.02 | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suffritti, C.; Gualtierotti, R.; Arcudi, S.; Ciavarella, A.; Novembrino, C.; Lecchi, A.; La Marca, S.; Padovan, L.; Scalambrino, E.; Clerici, M.; et al. Characterization of Immunogenicity and Safety of COVID-19 mRNA-1273 in HIV-Positive Italian Patients with Hemophilia: A Prospective Single-Center Cohort Study. J. Clin. Med. 2023, 12, 5475. https://doi.org/10.3390/jcm12175475
Suffritti C, Gualtierotti R, Arcudi S, Ciavarella A, Novembrino C, Lecchi A, La Marca S, Padovan L, Scalambrino E, Clerici M, et al. Characterization of Immunogenicity and Safety of COVID-19 mRNA-1273 in HIV-Positive Italian Patients with Hemophilia: A Prospective Single-Center Cohort Study. Journal of Clinical Medicine. 2023; 12(17):5475. https://doi.org/10.3390/jcm12175475
Chicago/Turabian StyleSuffritti, Chiara, Roberta Gualtierotti, Sara Arcudi, Alessandro Ciavarella, Cristina Novembrino, Anna Lecchi, Silvia La Marca, Lidia Padovan, Erica Scalambrino, Marigrazia Clerici, and et al. 2023. "Characterization of Immunogenicity and Safety of COVID-19 mRNA-1273 in HIV-Positive Italian Patients with Hemophilia: A Prospective Single-Center Cohort Study" Journal of Clinical Medicine 12, no. 17: 5475. https://doi.org/10.3390/jcm12175475
APA StyleSuffritti, C., Gualtierotti, R., Arcudi, S., Ciavarella, A., Novembrino, C., Lecchi, A., La Marca, S., Padovan, L., Scalambrino, E., Clerici, M., Bono, P., Ceriotti, F., Muscatello, A., Siboni, S. M., & Peyvandi, F. (2023). Characterization of Immunogenicity and Safety of COVID-19 mRNA-1273 in HIV-Positive Italian Patients with Hemophilia: A Prospective Single-Center Cohort Study. Journal of Clinical Medicine, 12(17), 5475. https://doi.org/10.3390/jcm12175475