
Red Cell Distribution Width as a Prognostic Indicator in Acute Medical Admissions


Abstract

1. Introduction
2. Materials and Methods
2.1. Background
2.2. Data Collection
2.3. Risk Predictors
2.4. Match to Irish National Death Register
2.5. Statistical Methods
3. Results
3.1. Patient Demographics
3.2. Demographics Related to 30-Day In-Hospital Mortality
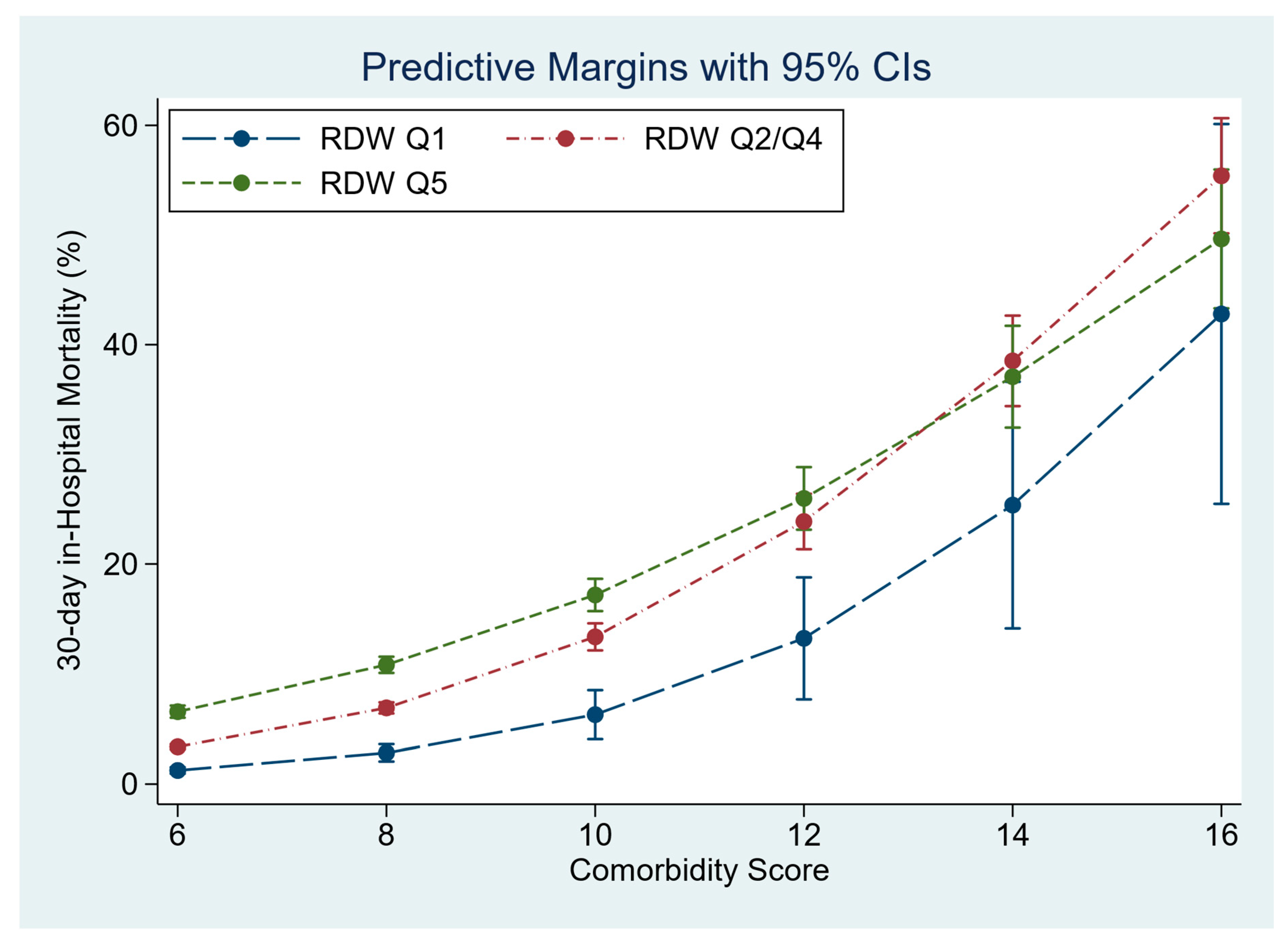
3.3. RDW as a Predictor of 30-Day In-Hospital Mortality
3.4. RDW as a Predictor of Long-Term Mortality
3.5. Survival Analysis of Long-Term Mortality
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Langlands, A.; Dowdle, R.; Elliott, A.; Gaddie, J.; Graham, A.; Johnson, G.; Lam, S.; McGowan, A.; McNamee, P.; Morrison, J.; et al. RCPE UK Consensus Statement on Acute Medicine, November 2008. Br. J. Hosp. Med. 2009, 70 (Suppl. S1), S6–S7. [Google Scholar]
- Conway, R.; Byrne, D.; Cournane, S.; O’Riordan, D.; Silke, B. Fifteen-year outcomes of an acute medical admission unit. Ir. J. Med. Sci. 2018, 187, 1097–1105. [Google Scholar] [CrossRef]
- Conway, R.; O’Riordan, D.; Silke, B. Long-term outcome of an AMAU—A decade’s experience. QJM 2014, 107, 43–49. [Google Scholar] [CrossRef]
- Coary, R.; Byrne, D.; O’Riordan, D.; Conway, R.; Cournane, S.; Silke, B. Does admission via an acute medical unit influence hospital mortality? 12 years’ experience in a large Dublin hospital. Acute Med. 2014, 13, 152–158. [Google Scholar] [CrossRef]
- Silke, B.; Kellett, J.; Rooney, T.; Bennett, K.; O’Riordan, D. An improved medical admissions risk system using multivariable fractional polynomial logistic regression modelling. Q. J. Med. 2010, 103, 23–32. [Google Scholar] [CrossRef]
- Arkew, M.; Gemechu, K.; Haile, K.; Asmerom, H. Red Blood Cell Distribution Width as Novel Biomarker in Cardiovascular Diseases: A Literature Review. J. Blood Med. 2022, 13, 413–424. [Google Scholar] [CrossRef]
- Uffen, J.W.; Oomen, P.; de Regt, M.; Oosterheert, J.J.; Kaasjager, K. The prognostic value of red blood cell distribution width in patients with suspected infection in the emergency department. BMC Emerg. Med. 2019, 19, 76. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Zhang, H.; Cao, X.; Deng, R.; Ye, Y.; Fu, Z.; Gou, L.; Shao, F.; Li, J.; Fu, W.; et al. Red cell distribution width (RDW): A prognostic indicator of severe COVID-19. Ann. Transl. Med. 2020, 8, 1230. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, B.; Sanaie, S.; Ghamari, A.A.; Soleimanpour, H.; Karimian, A.; Mahmoodpoor, A. Red Cell Distribution Width as a Novel Prognostic Marker in Multiple Clinical Studies. Indian J. Crit. Care Med. 2020, 24, 49–54. [Google Scholar]
- Montagnana, M.; Danese, E. Red cell distribution width and cancer. Ann. Transl. Med. 2016, 4, 399. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; Byrne, D.; O’Riordan, D.; Silke, B. Outcomes in acute medicine—Evidence from extended observations on readmissions, hospital length of stay and mortality outcomes. Eur. J. Intern. Med. 2019, 66, 69–74. [Google Scholar] [CrossRef]
- O’Callaghan, A.; Colgan, M.P.; McGuigan, C.; Smyth, F.; Haider, N.; O’Neill, S.; Moore, D.; Madhavan, P. A critical evaluation of HIPE data. Ir. Med. J. 2012, 105, 21–23. [Google Scholar]
- Cournane, S.; Conway, R.; Byrne, D.; O’Riordan, D.; Silke, B. Predicting Outcomes in Emergency Medical Admissions Using a Laboratory Only Nomogram. Comput Math Methods Med. 2017, 2017, 5267864. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; Byrne, D.; O’Riordan, D.; Silke, B. Comparative influence of Acute Illness Severity and comorbidity on mortality. Eur. J. Intern. Med. 2020, 72, 42–46. [Google Scholar] [CrossRef]
- Kopelman, P.G.; Sanderson, A.J. Application of database systems in diabetes care. Med. Inform. 1996, 21, 259–271. [Google Scholar] [CrossRef]
- Courtney, D.; Conway, R.; Kavanagh, J.; O’Riordan, D.; Silke, B. High-sensitivity troponin as an outcome predictor in acute medical admissions. Postgrad. Med. J. 2014, 90, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.L.; O’Dowd, S.; Adnan, W.A.; Bennett, K.; O’Riordan, D.; Mellotte, G.J.; Silke, B. Using the MDRD value as an outcome predictor in emergency medical admissions. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2011, 26, 3155–3159. [Google Scholar] [CrossRef]
- Conway, R.; O’Connell, B.; Byrne, D.; O’Riordan, D.; Silke, B. Prognostic Value of Blood Cultures as an Illness Severity Marker in Emergency Medical Admissions. Acute Med. 2020, 19, 83–89. [Google Scholar] [CrossRef]
- Kelly, A.; Teljeur, C. SAHRU National Deprivation Index Trinity College, Dublin 2007. Available online: http://www.sahru.tcd.ie/services/deprivation/DeprivationFiles/WebReport07.pdf (accessed on 15 February 2023).
- Conway, R.; Galvin, S.; Coveney, S.; O’Riordan, D.; Silke, B. Deprivation as an outcome determinant in emergency medical admissions. QJM 2013, 106, 245–251. [Google Scholar] [CrossRef]
- Patel, K.V.; Ferrucci, L.; Ershler, W.B.; Longo, D.L.; Guralnik, J.M. Red blood cell distribution width and the risk of death in middle-aged and older adults. Arch. Intern. Med. 2009, 169, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; Byrne, D.; O’Riordan, D.; Silke, B. Emergency readmissions are substantially determined by acute illness severity and chronic debilitating illness: A single centre cohort study. Eur. J. Intern. Med. 2015, 26, 12–17. [Google Scholar] [CrossRef]
- Conway, R.; Byrne, D.; O’Riordan, D.; Silke, B. Blood Culture and Troponin Testing in Suspected Bacteraemic Admissions—Example of Risk Stratification Based on Clinical Testing. Acute Med. 2022, 21, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Mattiuzzi, C.; Cervellin, G. Learning more and spending less with neglected laboratory parameters: The paradigmatic case of red blood cell distribution width. Acta Biomed. 2016, 87, 323–328. [Google Scholar] [PubMed]
- Conway, R.; Byrne, D.; O’Riordan, D.; Cournane, S.; Coveney, S.; Silke, B. Deprivation index and dependency ratio are key determinants of emergency medical admission rates. Eur. J. Intern. Med. 2015, 26, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; Byrne, D.; O’Riordan, D.; Cournane, S.; Coveney, S.; Silke, B. Influence of social deprivation, overcrowding and family structure on emergency medical admission rates. QJM 2016, 109, 675–680. [Google Scholar] [CrossRef][Green Version]
- Quinn, K.L.; Stall, N.M.; Yao, Z.; Stukel, T.A.; Cram, P.; Detsky, A.S.; Bell, C.M. The risk of death within 5 years of first hospital admission in older adults. CMAJ 2019, 191, E1369–E1377. [Google Scholar] [CrossRef]
- Fløjstrup, M.; Henriksen, D.P.; Brabrand, M. An acute hospital admission greatly increases one year mortality—Getting sick and ending up in hospital is bad for you: A multicentre retrospective cohort study. Eur. J. Intern. Med. 2017, 45, 5–7. [Google Scholar] [CrossRef]
- Clark, D.; Armstrong, M.; Allan, A.; Graham, F.; Carnon, A.; Isles, C. Imminence of death among hospital inpatients: Prevalent cohort study. Palliat. Med. 2014, 28, 474–479. [Google Scholar] [CrossRef]
- Moore, E.; Munoz-Arroyo, R.; Schofield, L.; Radley, A.; Clark, D.; Isles, C. Death within 1 year among emergency medical admissions to Scottish hospitals: Incident cohort study. BMJ Open 2018, 8, e021432. [Google Scholar] [CrossRef]
- Conway, R.; Creagh, D.; Byrne, D.G.; O’Riordan, D.; Silke, B. Serum potassium levels as an outcome determinant in acute medical admissions. Clin. Med. 2015, 15, 239–243. [Google Scholar] [CrossRef]
- Conway, R.; Byrne, D.; O’Riordan, D.; Silke, B. Hyponatraemia in Emergency Medical Admissions-Outcomes and Costs. J. Clin. Med. 2014, 3, 1220–1233. [Google Scholar] [CrossRef]
- Conway, R.; Byrne, D.; O’Riordan, D.; Silke, B. Prognostic value and clinical utility of NT-proBNP in acute emergency medical admissions. Ir. J. Med. Sci. 2022, 192, 1939–1946. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; Byrne, D.; O’Riordan, D.; Silke, B. Short and Long-Term Mortality Following Acute Medical Admission. QJM 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; O’Riordan, D.; Silke, B. Targets and the emergency medical system--intended and unintended consequences. Eur. J. Emerg. Med. Off. J. Eur. Soc. Emerg. Med. 2015, 22, 235–240. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | RDW Q1 | RDW Q2–Q4 | RDW Q5 | p-Value | |
|---|---|---|---|---|---|
| N | 12,240 | 38,673 | 11,271 | ||
| Age (years) | 49.5 (31.2, 69.4) | 66.6 (46.4, 79.1) | 67.5 (48.4, 79.5) | <0.001 | |
| LOS (days) | 4.3 (1.8, 8.9) | 5.9 (2.3, 12.9) | 8.2 (3.9, 17.5) | <0.001 | |
| Gender | Male | 6233 (50.9%) | 18,368 (48.5%) | 5392 (47.8%) | <0.001 |
| Female | 6007 (49.1%) | 19,469 (51.5%) | 5879 (52.2%) | ||
| Acute Illness | 1–3 | 6933 (56.6%) | 8948 (23.1%) | 350 (3.1%) | <0.001 |
| Severity Groups | 4 | 2486 (20.3%) | 6308 (16.3%) | 1146 (10.2%) | |
| 5 | 1777 (14.5%) | 8524 (22.0%) | 1940 (17.2%) | ||
| 6 | 1044 (8.5%) | 14,893 (38.5%) | 7835 (69.5%) | ||
| Charlson Index | 0 | 6969 (57.0%) | 15,581 (41.3%) | 3357 (29.9%) | <0.001 |
| 1 | 2954 (24.2%) | 10,023 (26.6%) | 2808 (25.0%) | ||
| 2 | 2293 (18.8%) | 12,081 (32.1%) | 5062 (45.1%) | ||
| Comorbidity | <6 | 8609 (70.3%) | 19,905 (51.5%) | 4396 (39.0%) | <0.001 |
| Score | 6 < 10 | 3146 (25.7%) | 15,100 (39.0%) | 5150 (45.7%) | |
| ≥10 | 485 (4.0%) | 3668 (9.5%) | 1725 (15.3%) | ||
| Blood Culture | 0 | 9243 (75.5%) | 27,738 (73.3%) | 7635 (67.7%) | <0.001 |
| Groups | 1 | 2584 (21.1%) | 8312 (22.0%) | 2822 (25.0%) | |
| 2 | 413 (3.4%) | 1787 (4.7%) | 814 (7.2%) |
| Variable | OR | Std. Err. | z | p > |z| | [95% Conf. Interval] | |
|---|---|---|---|---|---|---|
| RDW | 1.04 | 0.01 | 5.3 | 0.00 | 1.02 | 1.05 |
| Comorbidity Score | 1.11 | 0.01 | 21.4 | 0.00 | 1.10 | 1.12 |
| Charlson Index | 1.20 | 0.02 | 9.9 | 0.00 | 1.15 | 1.24 |
| Readmission No. | 1.03 | 0.01 | 4.5 | 0.00 | 1.02 | 1.05 |
| Respiratory | 0.92 | 0.03 | −2.4 | 0.02 | 0.86 | 0.98 |
| Cardiovascular | 1.17 | 0.04 | 4.2 | 0.00 | 1.09 | 1.26 |
| Neurology | 0.90 | 0.03 | −2.8 | 0.01 | 0.83 | 0.97 |
| Readmission/Older | 1.21 | 0.01 | 16.4 | 0.00 | 1.18 | 1.24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conway, R.; Byrne, D.; O’Riordan, D.; Silke, B. Red Cell Distribution Width as a Prognostic Indicator in Acute Medical Admissions. J. Clin. Med. 2023, 12, 5424. https://doi.org/10.3390/jcm12165424
Conway R, Byrne D, O’Riordan D, Silke B. Red Cell Distribution Width as a Prognostic Indicator in Acute Medical Admissions. Journal of Clinical Medicine. 2023; 12(16):5424. https://doi.org/10.3390/jcm12165424
Chicago/Turabian StyleConway, Richard, Declan Byrne, Deirdre O’Riordan, and Bernard Silke. 2023. "Red Cell Distribution Width as a Prognostic Indicator in Acute Medical Admissions" Journal of Clinical Medicine 12, no. 16: 5424. https://doi.org/10.3390/jcm12165424
APA StyleConway, R., Byrne, D., O’Riordan, D., & Silke, B. (2023). Red Cell Distribution Width as a Prognostic Indicator in Acute Medical Admissions. Journal of Clinical Medicine, 12(16), 5424. https://doi.org/10.3390/jcm12165424