

SARS-CoV-2 Vaccination Response in Japanese Patients with Autoimmune Hepatitis: Results of Propensity Score-Matched Case–Control Study

Abstract
:1. Introduction
2. Research Design and Methods
2.1. Study Population and Data Collection
2.2. Laboratory Assessments
2.3. Statistical Analyses
2.4. Ethical Issues
3. Results
3.1. Clinical Characteristics of the Study Population
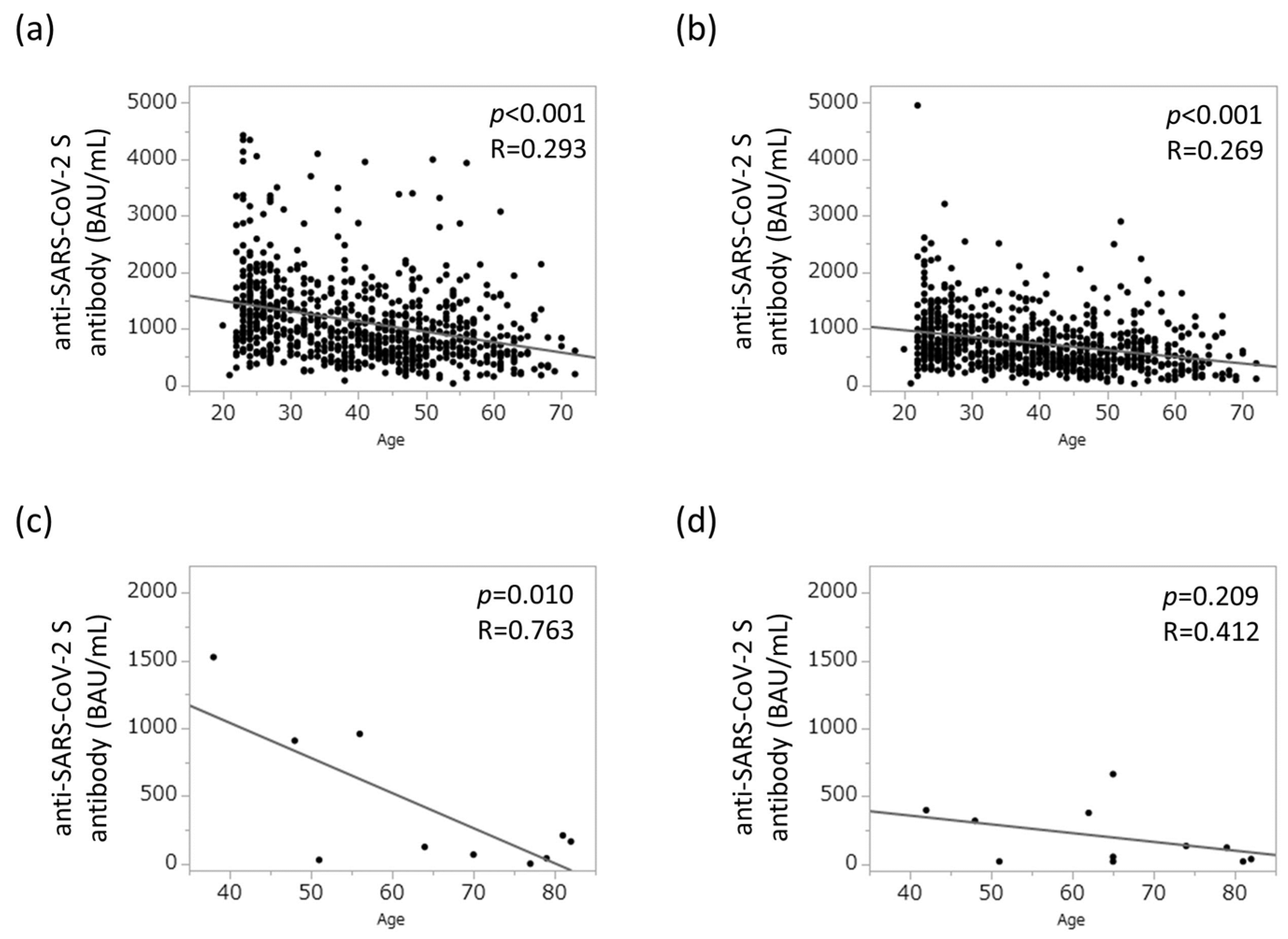
3.2. Risk Factors for Attenuated Humoral Vaccination Response in the Study Population
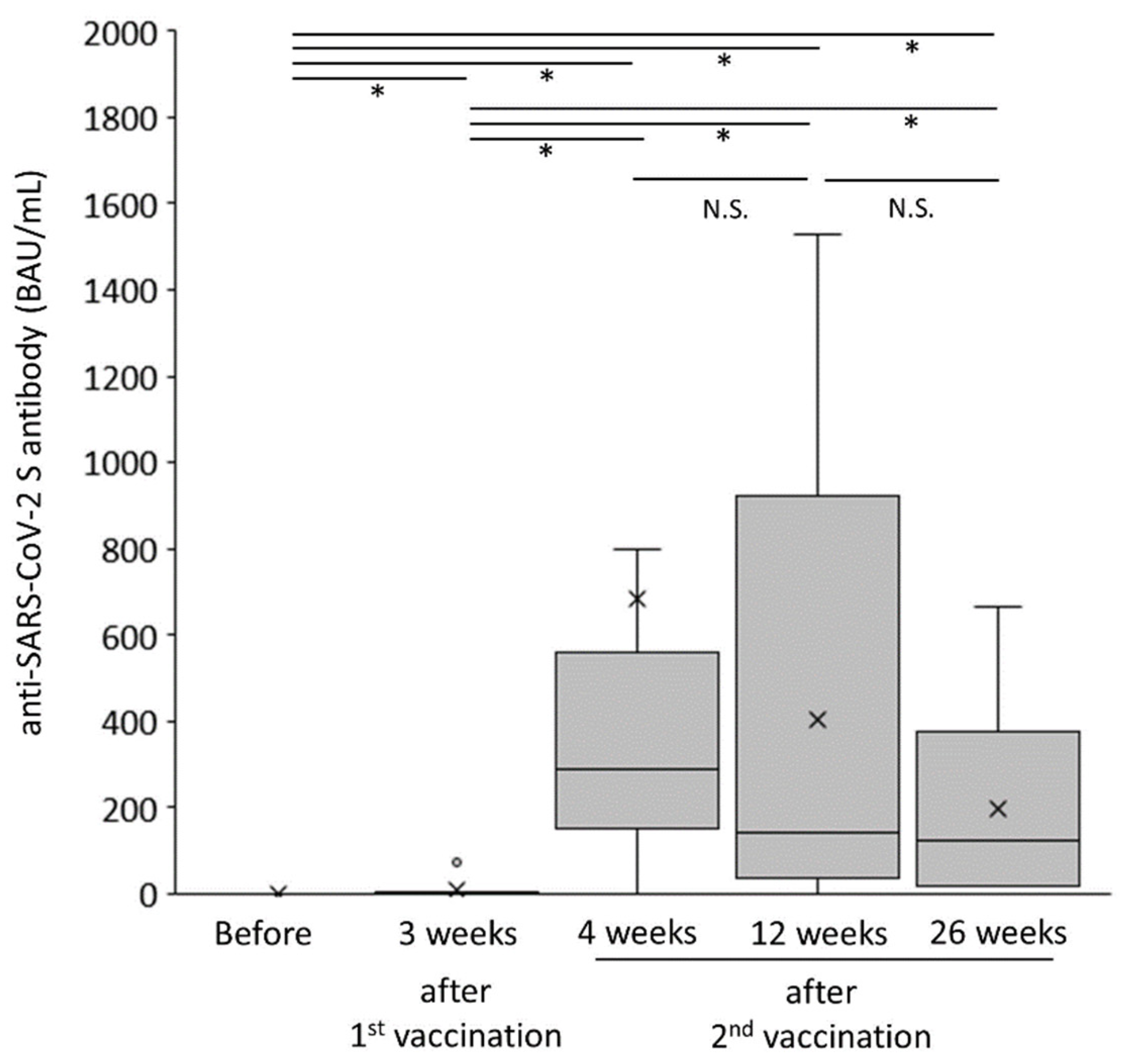
3.3. Attenuated Humoral Immune Response in the AIH Group
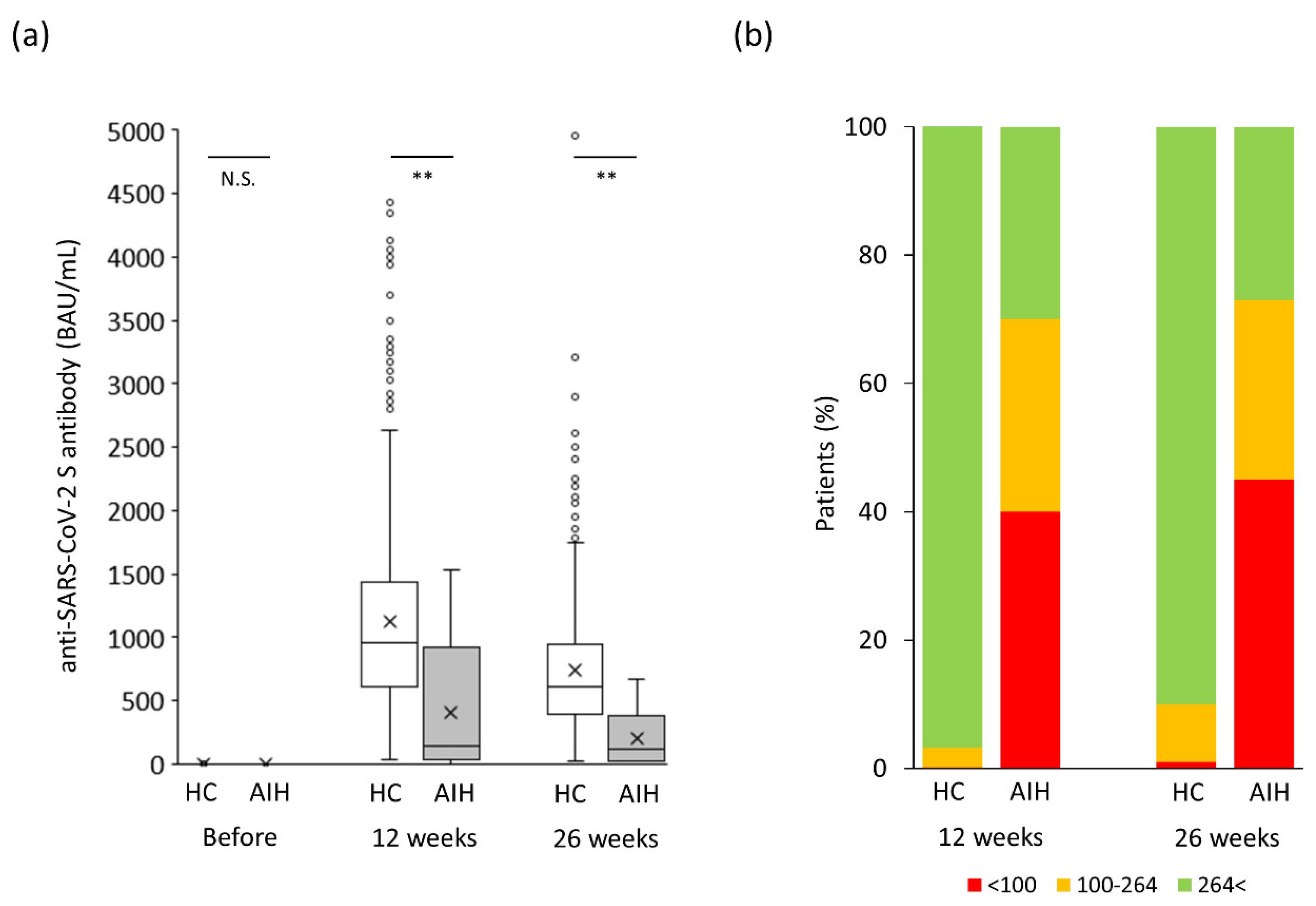
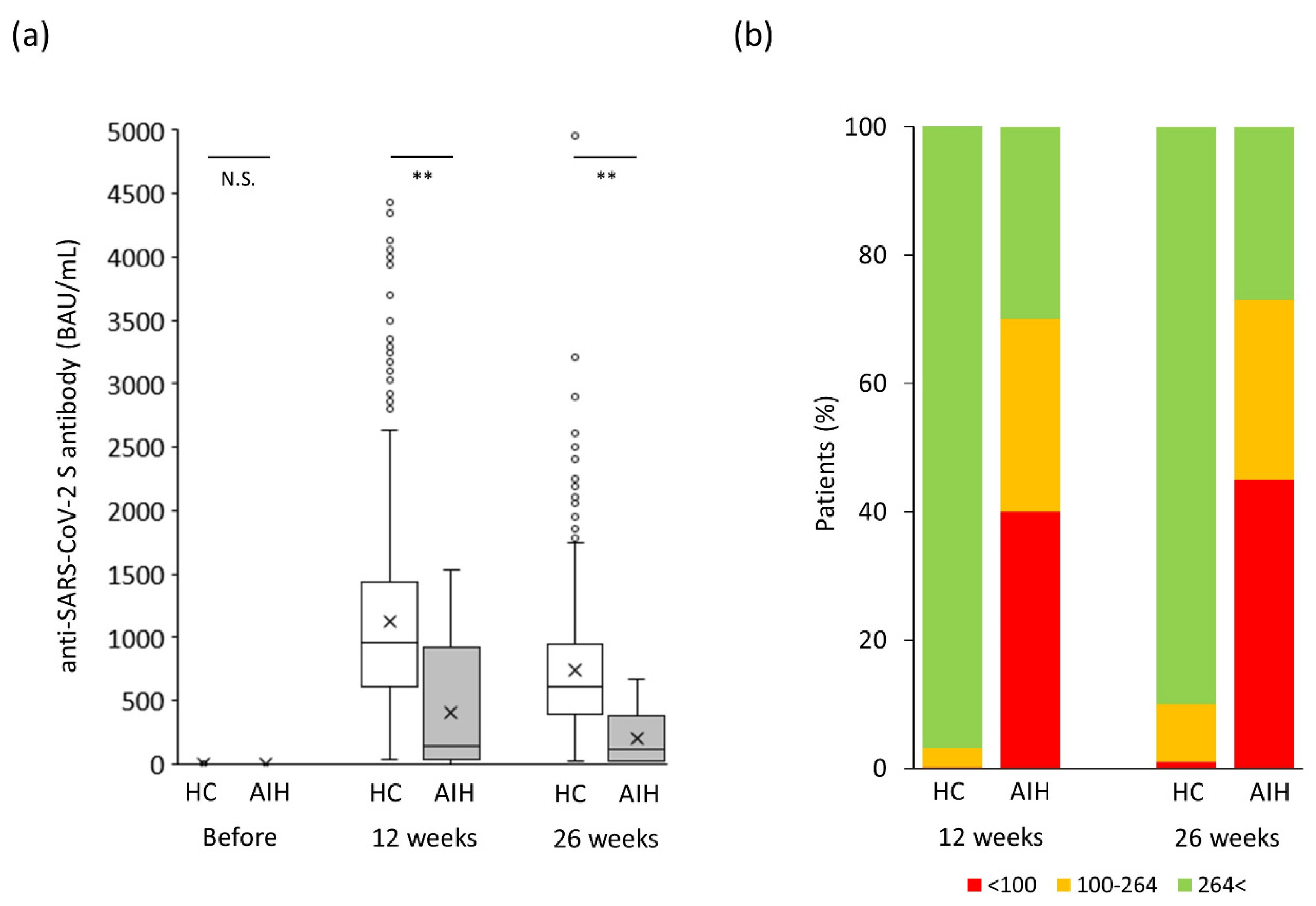
3.4. Propensity Score-Matched Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
References
- Takahashi, A.; Moriya, K.; Ohira, H.; Arinaga-Hino, T.; Zeniya, M.; Torimura, T.; Abe, M.; Takaki, A.; Kang, J.-H.; Inui, A.; et al. Health-related quality of life in patients with autoimmune hepatitis: A questionnaire survey. PLoS ONE 2018, 13, e0204772. [Google Scholar] [CrossRef] [PubMed]
- Lamba, M.; Ngu, J.H.; Stedman, C.A.M. Trends in incidence of autoimmune liver diseases and increasing incidence of autoimmune hepatitis. Clin. Gastroenterol. Hepatol. 2021, 19, 573–579.e1. [Google Scholar]
- Takahashi, A.; Ohira, H.; Abe, K.; Zeniya, M.; Abe, M.; Arinaga-Hino, T.; Torimura, T.; Yoshizawa, K.; Takaki, A.; Kang, J.-H.; et al. Increasing incidence of acute autoimmune hepatitis: A nationwide survey in Japan. Sci. Rep. 2020, 10, 14250. [Google Scholar] [CrossRef] [PubMed]
- Danielsson Borssén, Å.; Marschall, H.U.; Bergquist, A.; Rorsman, F.; Weiland, O.; Kechagias, S.; Nyhlin, N.; Verbaan, H.; Nilsson, E.; Werner, M. Epidemiology and causes of death in a Swedish cohort of patients with autoimmune hepatitis. Scand. J. Gastroenterol. 2017, 52, 1022–1028. [Google Scholar] [CrossRef]
- Yoshizawa, K.; Matsumoto, A.; Ichijo, T.; Umemura, T.; Joshita, S.; Komatsu, M.; Tanaka, N.; Tanaka, E.; Ota, M.; Katsuyama, Y. Long-term outcome of Japanese patients with type 1 autoimmune hepatitis. Hepatology 2012, 56, 668–676. [Google Scholar]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 30 June 2023).
- World Health Organization. Press Conferences on COVID-19 and Other Global Health Issues. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 30 June 2023).
- Nakase, H.; Hayashi, Y.; Hirayama, D.; Matsumoto, T.; Matsuura, M.; Iijima, H.; Matsuoka, K.; Ohmiya, N.; Ishihara, S.; Hirai, F.; et al. Interim analysis of a multicenter registry study of COVID-19 patients with inflammatory bowel disease in Japan (J-COSMOS). J. Gastroenterol. 2022, 57, 174–184. [Google Scholar] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and immunogenicity of two RNA-Based Covid-19 vaccine candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; Chappell, J.D.; Flach, B.; Stevens, L.J.; Pruijssers, A.J. An mRNA vaccine against SARS-CoV-2—Preliminary report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef]
- Tanaka, A.; Mori, M.; Matsumoto, K.; Ohira, H.; Tazuma, S.; Takikawa, H. Increase trend in the prevalence and Male-to-female ratio of primary biliary cholangitis, autoimmune hepatitis, and primary sclerosing cholangitis in Japan. Hepatol. Res. 2019, 49, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, F.; Berg, P.A.; Bianchi, F.B.; Bianchi, L.; Burroughs, A.K.; Cancado, E.L.; Chapman, R.W.; Cooksley, W.G.; Czaja, A.J.; Desmet, V.J.; et al. International Autoimmune Hepatitis Group Report: Review of criteria for diagnosis of autoimmune hepatitis. J. Hepatol. 1999, 31, 929–938. [Google Scholar] [CrossRef]
- Duengelhoef, P.; Hartl, J.; Rüther, D.; Steinmann, S.; Brehm, T.T.; Weltzsch, J.P.; Glaser, F.; Schaub, G.M.; Sterneck, M.; Sebode, M.; et al. SARS-CoV-2 vaccination response in patients with autoimmune hepatitis and autoimmune cholestatic liver disease. United Eur. Gastroenterol. J. 2022, 10, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Ruether, D.F.; Schaub, G.M.; Duengelhoef, P.M.; Haag, F.; Brehm, T.T.; Fathi, A.; Wehmeyer, M.; Jahnke-Triankowski, J.; Mayer, L.; Hoffmann, A.; et al. SARS-CoV2-specific humoral and T-cell immune response after second vaccination in liver cirrhosis and transplant patients. Clin. Gastroenterol. Hepatol. 2022, 20, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Ragone, C.; Meola, S.; Fiorillo, P.C.; Penta, R.; Auriemma, L.; Tornesello, M.L.; Miscio, L.; Cavalcanti, E.; Botti, G.; Buonaguro, F.M.; et al. HLA does not impact on short-medium-term antibody response to preventive anti-SARS-cov-2 vaccine. Front. Immunol. 2021, 12, 734689. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.G.; Ferreira, V.H.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Chaparro, C.; Selzner, N.; Schiff, J.; McDonald, M.; Tomlinson, G.; et al. Randomized trial of a third dose of mRNA-1273 vaccine in transplant recipients. N. Engl. J. Med. 2021, 385, 1244–1246. [Google Scholar] [CrossRef]
- Resman Rus, K.; Korva, M.; Knap, N.; Avšič Županc, T.; Poljak, M. Performance of the rapid high-throughput automated electrochemiluminescence immunoassay targeting total antibodies to the SARS-CoV-2 spike protein receptor binding domain in comparison to the neutralization assay. J. Clin. Virol. 2021, 139, 104820. [Google Scholar] [CrossRef]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef]
- John, B.V.; Deng, Y.; Schwartz, K.B.; Taddei, T.H.; Kaplan, D.E.; Martin, P.; Chao, H.-H.; Dahman, B. Postvaccination COVID-19 infection is associated with reduced mortality in patients with cirrhosis. Hepatology 2022, 76, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and management of autoimmune hepatitis in adults and children: 2019 Practice guidance and guidelines from the American Association for the Study of Liver Diseases. Hepatology 2020, 72, 671–722. [Google Scholar]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar] [CrossRef]
- Brenner, E.J.; Ungaro, R.C.; Gearry, R.B.; Kaplan, G.G.; Hunt, M.K.; Lewis, J.D.; Ng, S.C.; Rahier, J.-F.; Reinisch, W.; Ruemmele, F.M.; et al. Corticosteroids, but not TNF antagonists, are associated with adverse COVID-19 outcomes in patients with inflammatory bowel diseases: Results from an international registry. Gastroenterology 2020, 159, 481–491.e3. [Google Scholar] [CrossRef]
- Rela, M.; Jothimani, D.; Vij, M.; Rajakumar, A.; Rammohan, A. Auto-immune hepatitis following COVID vaccination. J. Autoimmun. 2021, 123, 102688. [Google Scholar] [CrossRef] [PubMed]
- Goulas, A.; Kafiri, G.; Kranidioti, H.; Manolakopoulos, S. A typical autoimmune hepatitis case following Covid-19 mRNA vaccination. More than a coincidence? Liver Int. 2022, 42, 254–255. [Google Scholar] [CrossRef] [PubMed]
- Mathew, M.; John, S.B.; Sebastian, J.; Ravi, M.D. COVID-19 vaccine triggered autoimmune hepatitis: Case report. Eur. J. Hosp. Pharm. 2022, ejhpharm-2022-003485. [Google Scholar] [CrossRef] [PubMed]
- Avci, E.; Abasiyanik, F. Autoimmune hepatitis after SARS-CoV-2 vaccine: New-onset or flare-up? J. Autoimmun. 2021, 125, 102745. [Google Scholar] [CrossRef] [PubMed]
- Sgamato, C.; Rocco, A.; Compare, D.; Minieri, S.; Marchitto, S.A.; Maurea, S.; Nardone, G. Autoimmune liver diseases and SARS-CoV-2. World J. Gastroenterol. 2023, 29, 1838–1851. [Google Scholar] [CrossRef] [PubMed]
- Uzun, S.; Zinner, C.; Beenen, A.C.; Alborelli, I.; Bartoszek, E.M.; Yeung, J.; Calgua, B.; Reinscheid, M.; Bronsert, P.; Stalder, A.K.; et al. Morphologic and molecular analysis of liver injury after SARS-CoV-2 vaccination reveals distinct characteristics. J. Hepatol. 2023, 79, 666–676. [Google Scholar]
- Chen, C.; Xie, D.; Xiao, J. Real-world evidence of autoimmune hepatitis following COVID-19 vaccination: A population-based pharmacovigilance analysis. Front. Pharmacol. 2023, 14, 1100617. [Google Scholar] [CrossRef]
- Efe, C.; Lammert, C.; Taşçılar, K.; Dhanasekaran, R.; Ebik, B.; Higuera-de la Tijera, F.; Magro, B.; Snijders, R.; Barutçu, S.; Lytvyak, E.; et al. Effects of immunosuppressive drugs on COVID-19 severity in patients with autoimmune hepatitis. Liver Int. 2022, 42, 607–614. [Google Scholar] [PubMed]
- Efe, C.; Taşçılar, K.; Gerussi, A.; Bolis, F.; Lammert, C.; Ebik, B.; Adali, G.; Çalışkan, A.R.; Balaban, Y.; Eren, F.; et al. SARS-CoV-2 vaccination and risk of severe COVID-19 outcomes in patients with autoimmune hepatitis. J. Autoimmun. 2022, 132, 102906. [Google Scholar] [CrossRef] [PubMed]
- Schneider, L.; Schubert, L.; Winkler, F.; Munda, P.; Winkler, S.; Tobudic, S. SARS-CoV-2 vaccine response in patients with autoimmune hepatitis. Clin. Gastroenterol. Hepatol. 2022, 20, 2145–2147.e2. [Google Scholar] [CrossRef] [PubMed]
- Hartl, J.; Rüther, D.F.; Duengelhoef, P.M.; Brehm, T.T.; Steinmann, S.; Weltzsch, J.P.; Schaub, G.M.; Haag, F.; Schramm, C.; Wiesch, J.S.Z.; et al. Analysis of the humoral and cellular response after the third COVID-19 vaccination in patients with autoimmune hepatitis. Liver Int. 2023, 43, 393–400. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Originally Registered Cases (n = 831) | Propensity Score Matched Cases (n = 30) | |||||
|---|---|---|---|---|---|---|
| Controls (n = 809) | AIH Patients (n = 22) | p | Controls (n = 15) | AIH Patients (n = 15) | p | |
| Age (years) | 39.0 [28.0–49.0] | 65.0 [61.3–79.0] | <0.01 | 60.0 [54.0–68.0] | 61.0 [54.0–65.0] | 0.86 |
| Sex (male/female) | 186/623 | 4/18 | 0.79 | 2/32 | 3/12 | 1.00 |
| Prednisolone (yes/no) | no data | 16/6 | - | no data | 11/4 | - |
| Prednisolone (mg/day) | no data | 5.5 [5.0–6.0] | - | no data | 6.0 [5.0–6.5] | - |
| Azathioprine (yes/no) | no data | 4/18 | - | no data | 3/12 | - |
| Azathioprine (mg/day) | no data | 75.0 [75.0–93.8] | - | no data | 75.0 [75.0–112.5] | - |
| anti-allergic agents (yes/no) | no data | 0/22 | - | no data | 0/15 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moriya, K.; Nakakita, T.; Nakayama, N.; Matsuo, Y.; Komeda, Y.; Hanatani, J.; Kaya, D.; Nagamatsu, S.; Matsuo, H.; Uejima, M.; et al. SARS-CoV-2 Vaccination Response in Japanese Patients with Autoimmune Hepatitis: Results of Propensity Score-Matched Case–Control Study. J. Clin. Med. 2023, 12, 5411. https://doi.org/10.3390/jcm12165411
Moriya K, Nakakita T, Nakayama N, Matsuo Y, Komeda Y, Hanatani J, Kaya D, Nagamatsu S, Matsuo H, Uejima M, et al. SARS-CoV-2 Vaccination Response in Japanese Patients with Autoimmune Hepatitis: Results of Propensity Score-Matched Case–Control Study. Journal of Clinical Medicine. 2023; 12(16):5411. https://doi.org/10.3390/jcm12165411
Chicago/Turabian StyleMoriya, Kei, Tomoko Nakakita, Natsuki Nakayama, Yuya Matsuo, Yusuke Komeda, Junichi Hanatani, Daisuke Kaya, Shinsaku Nagamatsu, Hideki Matsuo, Masakazu Uejima, and et al. 2023. "SARS-CoV-2 Vaccination Response in Japanese Patients with Autoimmune Hepatitis: Results of Propensity Score-Matched Case–Control Study" Journal of Clinical Medicine 12, no. 16: 5411. https://doi.org/10.3390/jcm12165411
APA StyleMoriya, K., Nakakita, T., Nakayama, N., Matsuo, Y., Komeda, Y., Hanatani, J., Kaya, D., Nagamatsu, S., Matsuo, H., Uejima, M., & Nakamura, F. (2023). SARS-CoV-2 Vaccination Response in Japanese Patients with Autoimmune Hepatitis: Results of Propensity Score-Matched Case–Control Study. Journal of Clinical Medicine, 12(16), 5411. https://doi.org/10.3390/jcm12165411