
Dual Antiplatelet Therapy or Antiplatelet Plus Anticoagulant Therapy in Patients with Peripheral and Chronic Coronary Artery Disease: An Updated Review



 , , ,
, , , 

Abstract
1. Introduction
2. Recognizing the Burden of Polyvascular Disease as a Chance to Improve Precision Medicine
3. Antithrombotic Therapy in the Chronic Phase of the Disease
3.1. Single Antiplatelet Strategy
3.2. Dual Antiplatelet Therapy
3.3. Therapy with Aspirin Combined with an Anticoagulant Drug
3.4. Antithrombotic Therapy after Revascularization
3.4.1. Lower Extremity Peripheral Revascularization
3.4.2. Carotid Revascularization
3.4.3. Coronary Revascularization in Chronic Coronary Syndrome
4. Primary Prevention
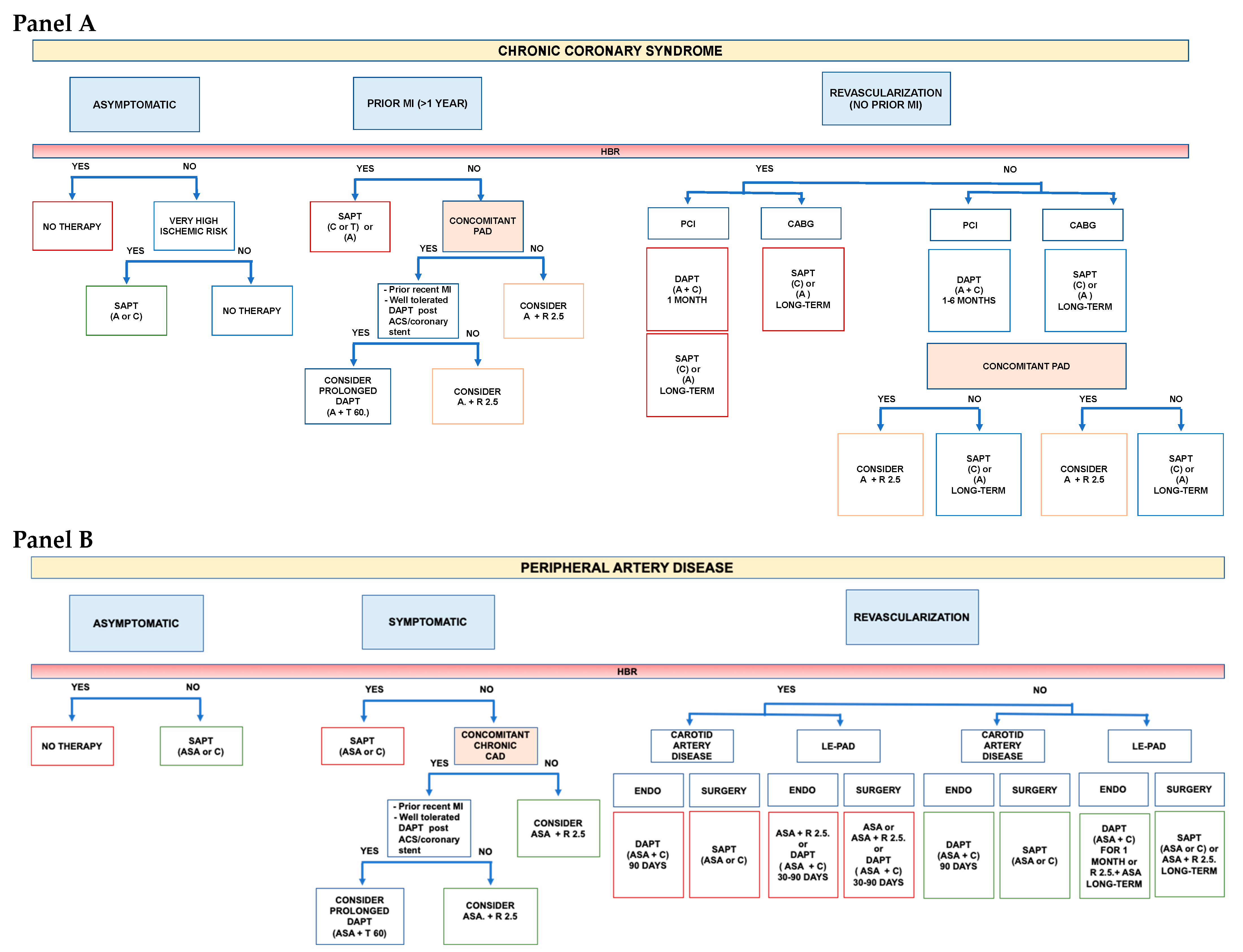
A Practical Approach
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 56. [Google Scholar] [CrossRef]
- Suarez, C.; Zeymer, U.; Limbourg, T.; Baumgartner, I.; Cacoub, P.; Poldermans, D.; Röther, J.; Bhatt, D.L.; Steg, P.G.; REACH Registry Investigators. Influence of polyvascular disease on cardiovascular event rates. Insights from the REACH Registry. Vasc. Med. 2010, 15, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Cotter, G.; Cannon, C.P.; McCabe, C.H.; Michowitz, Y.; Kaluski, E.; Charlesworth, A.; Milo, O.; Bentley, J.; Blatt, A.; Krakover, R.; et al. OPUS-TIMI 16 Investigators. Prior peripheral arterial disease and cerebrovascular disease are independent predictors of adverse outcome in patients with acute coronary syndromes: Are we doing enough? Results from the Orbofiban in Patients with Unstable Coronary Syndromes-Thrombolysis in Myocardial Infarction (OPUS-TIMI) 16 study. Am. Heart J. 2003, 145, 622–627. [Google Scholar] [PubMed]
- Hess, C.N.; Bonaca, M.P. Contemporary Review of Antithrombotic Therapy in Peripheral Artery Disease. Circ. Cardiovasc. Interv. 2020, 13, e009584. [Google Scholar] [CrossRef]
- Anand, S.S.; Caron, F.; Eikelboom, J.W.; Bosch, J.; Dyal, L.; Aboyans, V.; Abola, M.T.; Branch, K.R.H.; Keltai, K.; Bhatt, D.L.; et al. Major adverse limb events and mortality in patients with peripheral artery disease: The COMPASS trial. J. Am. Coll. Cardiol. 2018, 71, 2306. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. ESC Scientific Document Group. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries Endorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.R.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guide- lines. J. Am. Coll. Cardiol. 2017, 69, 1465–1508. [Google Scholar] [PubMed]
- CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE Steering Committee. Lancet 1996, 348, 1329–1339. [Google Scholar] [CrossRef]
- Hiatt, W.R.; Fowkes, F.G.; Heiyer, G.; Berger, J.S.; Baumgartner, I.; Held, P.; Katona, B.G.; Mahaffey, K.W.; Norgren, L.; Jones, W.S.; et al. EUCLID Trial Steering Committee and Investigators. Ticagrelor versus Clopidogrel in Symptomatic Peripheral Artery Disease. N. Engl. J. Med. 2017, 376, 32–40. [Google Scholar] [CrossRef]
- Berger, J.S.; Kranty, M.J.; Kittelson, J.M.; Hiatt, W.R. Aspirin for the prevention of cardiovascualr events in patients with peripheral artery disease: A meta-analysis of randomized trials. JAMA 2009, 301, 1909–1919. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Fox, K.A.; Hacke, W.; CHARISMA Investigators. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N. Engl. J. Med. 2006, 354, 1706–1717. [Google Scholar] [CrossRef] [PubMed]
- Cacoub, P.P.; Bhatt, D.L.; Steg, P.G.; Topol, E.J.; Creager, M.A. CHARISMA Investigators. Patients with peripheral arterial disease in the CHARISMA trial. Eur. Heart J. 2009, 30, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Campo, G.; Monti, M.; Vranckx, P.; Percoco, G.; Tumscitz, C.; Castriota, F.; Colombo, F.; Tebaldi, M.; Fucà, G.; et al. Prolonging Dual Antiplatelet Treatment after Grading Stent-Induced Intimal Hyperplasia Study (PRODIGY) Investigators. Short- versus long-term duration of dual-antiplatelet therapy after coronary stenting: A randomized multicenter trial. Circulation 2012, 125, 2015–2026. [Google Scholar] [CrossRef] [PubMed]
- Franzone, A.; Piccolo, R.; Gargiulo, G.; Ariotti, S.; Marino, M.; Santucci, A.; Baldo, A.; Magnani, G.; Moschovitis, A.; Windecker, S.; et al. Prolonged vs Short Duration of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention in Patients with or without Peripheral Arterial Disease: A Subgroup Analysis of the PRODIGY Randomiyed Clinical Trial. JAMA Cardiol. 2016, 1, 795–803. [Google Scholar] [CrossRef]
- Secemsky, E.A.; Yeh, R.W.; Kereiakes, D.J.; Dual Antiplatelet Therapy Study Investigators. Extended Duration Dual Antiplatelet Therapy after Coronary Stenting Among Patients with Peripheral Arterial Disease: A Subanalysis of the Dual Antiplatelet Therapy Study. JACC Cardiovasc. Interv. 2017, 10, 942–954. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Creager, M.A.; Olin, J.; Scirica, B.M.; Gilchrist, I.C., Jr.; Murphy, S.A.; Goodrich, E.L.; Braunwald, E.; Morrow, D.A. Peripheral Revascularization in Patients with Peripheral Artery Disease with Vorapaxar: Insights from the TRA 2°P-TIMI 50 Trial. JACC Cardiovasc. Interv. 2016, 9, 2157–2164. [Google Scholar] [CrossRef]
- Magnani, G.; Bonaca, M.P.; Braunwald, E.; Dalby, A.J.; Fox, K.A.; Murphy, S.A.; Nicolau, J.C.; Oude Ophuis, T.; Scirica, B.M.; Spinar, J.; et al. Efficacy and safety of vorapaxar as approved for clinical use in the United States. J. Am. Heart Assoc. 2015, 4, e001505, Erratum in J. Am. Heart Assoc. 2015, 4, e000633. [Google Scholar] [CrossRef]
- Qamar, A.; Morrow, D.A.; Creager, M.A.; Scirica, B.M.; Olin, J.W.; Beckman, J.A.; Murphy, S.A.; Bonaca, M.P. Effect of vorapaxar on cardiovascular and limb outcomes in patients with peripheral artery disease with and without coronary artery disease: Analysis from the TRA 2°P-TIMI 50 trial. Vasc. Med. 2020, 25, 124–132. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Bhatt, D.L.; Storey, R.F.; Steg, P.G.; Cohen, M.; Kuder, J.; Goodrich, E.; Nicolau, J.C.; Parkhomenko, A.; López-Sendón, J.; et al. Ticagrelor for Prevention of Ischemic Events after Myocardial Infarction in Patients with Peripheral Artery Disease. J. Am. Coll. Cardiol. 2016, 67, 2719–2728. [Google Scholar] [CrossRef]
- Eikelboom, J.W.; Connolly, S.J.; Bosch, J.; Dagenais, G.R.; Hart, R.G.; Shestakovska, O.; Diaz, R.; Alings, M.; Lonn, E.M.; Anand, S.S.; et al. COMPASS Investigators. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease. N. Engl. J. Med. 2017, 377, 1319–1330. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Eikelboom, J.W.; Bosch, J.; Dagenais, G.; Dyal, L.; Lanas, F.; Metsarinne, K.; O’Donnell, M.; Dans, A.L.; Ha, J.W.; et al. COMPASS investigators. Rivaroxaban with or without aspirin in patients with stable coronary artery disease: An international, randomised, double-blind, placebo-controlled trial. Lancet 2018, 391, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Bauersachs, R.M.; Anand, S.S.; Debus, E.S.; Nehler, M.R.; Patel, M.R.; Fanelli, F.; Capell, W.H.; Diao, L.; Jaeger, N.; et al. Rivaroxaban in Peripheral Artery Disease after Revascularization. N. Engl. J. Med. 2020, 382, 1994–2004. [Google Scholar] [CrossRef] [PubMed]
- Canonico, M.E.; Piccolo, R.; Avvedimento, M.; Leone, A.; Esposito, S.; Franzone, A.; Giugliano, G.; Gargiulo, G.; Hess, C.N.; Berkowitz, S.D.; et al. Antithrombotic Therapy in Peripheral Artery Disease: Current Evidence and Future Directions. J. Cardiovasc. Dev. Dis. 2023, 10, 164. [Google Scholar] [CrossRef]
- Mehta, A.; Rigdon, J.; Tattersall, M.C.; German, C.A.; Barringer, T.A., 3rd; Joshi, P.H.; Sperling, L.S.; Budoff, M.J.; Bertoni, A.; Michos, E.D.; et al. Association of Carotid Artery Plaque with Cardiovascular Events and Incident Coronary Artery Calcium in Individuals with Absent Coronary Calcification: The MESA. Circ. Cardiovasc. Imaging 2021, 14, e011701. [Google Scholar] [CrossRef]
- Achim, A.; Kákonyi, K.; Nagy, F.; Jambrik, Z.; Varga, A.; Nemes, A.; Chan, J.S.K.; Toth, G.G.; Ruzsa, Z. Radial Artery Calcification in Predicting Coronary Calcification and Atherosclerosis Burden. Cardiol. Res. Pract. 2022, 2022, 5108389. [Google Scholar] [CrossRef]
- Valgimigli, M.; Aboyans, V.; Angiolillo, D.; Atar, D.; Capodanno, D.; Halvorsen, S.; James, S.; Jüni, P.; Kunadian, V.; Landi, A.; et al. Antithrombotic treatment strategies in patients with established coronary atherosclerotic disease: 2022 joint clinical consensus statement of the European Association of Percutaneous Cardiovascular Interventions (EAPCI), Association for Acute CardioVascular Care (ACVC) and European Association of Preventive Cardiology (EAPC). Eur. Heart J. Cardiovasc. Pharmacother. 2023, 9, 462–496. [Google Scholar] [CrossRef]
- Gutierrez, J.A.; Aday, A.W.; Patel, M.R.; Jones, W.S. Polyvascular Disease: Reappraisal of the Current Clinical Landscape. Circ. Cardiovasc. Interv. 2019, 2, e007385. [Google Scholar] [CrossRef]
- Lawler, P.R.; Bhatt, D.L.; Godoy, L.C.; Lüscher, T.F.; Bonow, R.O.; Verma, S.; Ridker, P.M. Targeting cardiovascular inflammation: Next steps in clinical translation. Eur. Heart J. 2021, 42, 113–131. [Google Scholar] [CrossRef]
- Denegri, A.; Magnani, G.; Kraler, S.; Bruno, F.; Klingenberg, R.; Mach, F.; Gencer, B.; Räber, L.; Rodondi, N.; Rossi, V.A.; et al. History of peripheral artery disease and cardiovascular risk of real-world patients with acute coronary syndrome: Role of inflammation and comorbidities. Int. J. Cardiol. 2023, 382, 76–82. [Google Scholar] [CrossRef]
- Achim, A.; Stanek, A.; Homorodean, C.; Spinu, M.; Onea, H.L.; Lazăr, L.; Marc, M.; Ruzsa, Z.; Olinic, D.M. Approaches to Peripheral Artery Disease in Diabetes: Are There Any Differences? Int. J. Environ. Res. Public Health 2022, 19, 9801. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Gutierrez, J.A.; Cannon, C.; Giugliano, R.; Blazing, M.; Park, J.G.; White, J.; Tershakovec, A.; Braunwald, E. Polyvascular disease, type 2 diabetes, and long-term vascular risk: A secondary analysis of the IMPROVE-IT trial. Lancet Diabetes Endocrinol. 2018, 6, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Achim, A.; Lackó, D.; Hüttl, A.; Csobay-Novák, C.; Csavajda, Á.; Sótonyi, P.; Merkely, B.; Nemes, B.; Ruzsa, Z. Impact of Diabetes Mellitus on Early Clinical Outcome and Stent Restenosis after Carotid Artery Stenting. J. Diabetes Res. 2022, 2022, 4196195. [Google Scholar] [CrossRef] [PubMed]
- Collaboration, A.T. Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high-risk patients. BMJ 2002, 324, 71–86. [Google Scholar] [CrossRef]
- Ferreiro, J.L.; Bhatt, D.L.; Ueno, M.; Bauer, D.; Angiolillo, D.J. Impact of smoking on long-term outcomes in patients with atherosclerotic vascular disease treated with aspirin or clopidogrel: Insights from the CAPRIE trial (Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events). J. Am. Coll. Cardiol. 2014, 63, 769–777. [Google Scholar] [CrossRef]
- Bauersachs, R.; Wu, O.; Briere, J.B.; Bowrin, K.; Borkowska, K.; Jakubowska, A.; Taieb, V.; Toumi, M.; Huelsebeck, M. Antithrombotic Treatments in Patients with Chronic Coronary Artery Disease or Peripheral Artery Disease: A Systematic Review of Randomised Controlled Trials. Cardiovasc. Ther. 2020, 2020, 3057168. [Google Scholar] [CrossRef] [PubMed]
- Hess, C.N.; Hiatt, W.R. Antithrombotic Therapy for Peripheral Artery Disease in 2018. JAMA 2018, 319, 2329–2330. [Google Scholar] [CrossRef]
- Clavijo, L.C.; Al-Asady, N.; Dhillon, A.; Matthews, R.V.; Caro, J.; Tun, H.; Rowe, V.; Shavelle, D.M. Prevalence of high on-treatment (aspirin and clopidogrel) platelet reactivity in patients with critical limb ischemia. Cardiovasc. Revasc. Med. 2018, 19, 516–520. [Google Scholar] [CrossRef]
- Capodanno, D.; Bhatt, D.L.; Eikelboom, J.W.; Fox, K.A.A.; Geisler, T.; Michael Gibson, C.; Gonzalez-Juanatey, J.R.; James, S.; Lopes, R.D.; Mehran, R.; et al. Dual-pathway inhibition for secondary and tertiary antithrombotic prevention in cardiovascular disease. Nat. Rev. Cardiol. 2020, 17, 242–257. [Google Scholar] [CrossRef]
- Criqui, M.H.; Matsushita, K.; Aboyans, V.; Hess, C.N.; Hicks, C.W.; Kwan, T.W.; McDermott, M.M.; Misra, S.; Ujueta, F.; American Heart Association Council on Epidemiology and Prevention; et al. Lower Extremity Peripheral Artery Disease: Contemporary Epidemiology, Management Gaps, and Future Directions: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e171–e191. [Google Scholar] [CrossRef]
- Merlini, P.A.; Bauer, K.A.; Oltrona, L.; Ardissino, D.; Cattaneo, M.; Belli, C.; Mannucci, P.M.; Rosenberg, R.D. Persistent activation of coagulation mechanism in unstable angina and myocardial infarction. Circulation 1994, 90, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Ardissino, D.; Merlini, P.A.; Bauer, K.A.; Galvani, M.; Ottani, F.; Franchi, F.; Bertocchi, F.; Rosenberg, R.D.; Mannucci, P.M. Coagulation activation and long-term outcome in acute coronary syndromes. Blood 2003, 102, 2731–2735. [Google Scholar] [CrossRef] [PubMed]
- Weitz, J.I. Insights into the role of thrombin in the pathogenesis of recurrent ischaemia after acute coronary syndrome. Thromb. Haemost. 2014, 112, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Mega, J.L.; Braunwald, E.; Wiviott, S.D.; Bassand, J.P.; Bhatt, D.L.; Bode, C.; Burton, P.; Cohen, M.; Cook-Bruns, N.; Fox, K.A.; et al. ATLAS ACS 2–TIMI 51 Investigators. Rivaroxaban in patients with a recent acute coronary syndrome. N. Engl. J. Med. 2012, 366, 9–19. [Google Scholar] [CrossRef]
- Tepe, G.; Bantleon, R.; Brechtel, K.; Schmehl, J.; Zeller, T.; Claussen, C.D.; Strobl, F.F. Management of peripheral arterial interventions with mono or dual antiplatelet therapy--the MIRROR study: A randomised and double-blinded clinical trial. Eur. Radiol. 2012, 22, 1998–2006. [Google Scholar] [CrossRef]
- Belch, J.J.; Dormandy, J.; Biasi, G.M.; Cairols, M.; Diehm, C.; Eikelboom, B.; Golledge, J.; Jawien, A.; Lepäntalo, M.; Norgren, L.; et al. Results of the randomized, placebo-controlled clopidogrel and acetylsalicylic acid in bypass surgery for peripheral arterial disease (CASPAR) trial. J. Vasc. Surg. 2010, 52, 825–833.e2. [Google Scholar] [CrossRef]
- Moll, F.; Baumgartner, I.; Jaff, M.; Nwachuku, C.; Tangelder, M.; Ansel, G.; Adams, G.; Zeller, T.; Rundback, J.; Grosso, M.; et al. ePAD Investigators. Edoxaban Plus Aspirin vs Dual Antiplatelet Therapy in Endovascular Treatment of Patients with Peripheral Artery Disease: Results of the ePAD Trial. J. Endovasc. Ther. 2018, 25, 158–168. [Google Scholar] [CrossRef]
- Efficacy of oral anticoagulants compared with aspirin after infrainguinal bypass surgery (The Dutch Bypass Oral Anticoagulants or Aspirin Study): A randomised trial. Lancet 2000, 355, 346–351. [CrossRef]
- Hess, C.N.; Debus, E.S.; Nehler, M.R.; Anand, S.S.; Patel, M.R.; Szarek, M.; Capell, W.H.; Hsia, J.; Beckman, J.A.; Brodmann, M.; et al. Reduction in Acute Limb Ischemia with Rivaroxaban versus Placebo in Peripheral Artery Disease after Lower Extremity Revascularization: Insights from VOYAGER PAD. Circulation 2021, 144, 1831–1841. [Google Scholar] [CrossRef]
- McKevitt, F.M.; Randall, M.S.; Cleveland, T.J.; Gaines, P.A.; Tan, K.T.; Venables, G.S. The Benefits of Combined Anti-platelet Treatment in Carotid Artery Stenting. Eur. J. Vasc. Endovasc. Surg. 2005, 29, 522–527. [Google Scholar] [CrossRef]
- Dalainas, I.; Nano, G.; Bianchi, P.; Stegher, S.; Malacrida, G.; Tealdi, D.G. Dual Antiplatelet Regime versus Acetyl-acetic Acid for Carotid Artery Stenting. Cardiovasc. Interv. Radiol. 2006, 29, 519–521. [Google Scholar] [CrossRef] [PubMed]
- Gensicke, H.; van der Worp, H.B.; Nederkoorn, P.J.; Macdonald, S.; Gaines, P.A.; van der Lugt, A.; Mali, W.P.; Lyrer, P.A.; Peters, N.; Featherstone, R.L.; et al. ICSS-MRI Substudy Investigators. Ischemic brain lesions after carotid artery stenting increase future cerebrovascular risk. J. Am. Coll. Cardiol. 2015, 65, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Barkat, M.; Hajibandeh, S.; Hajibandeh, S.; Torella, F.; Antoniou, G.A. Systematic Review and Meta-analysis of Dual versus Single Antiplatelet Therapy in Carotid Interventions. Eur. J. Vasc. Endovasc. Surg. 2017, 53, 53–67. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.A.; Galli, M.; Collet, J.P.; Kastrati, A.; O’Donoghue, M.L. Antiplatelet therapy after percutaneous coronary intervention. EuroIntervention 2022, 17, e1371–e1396. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Montalto, C.; Branca, M.; Hong, S.J.; Watanabe, H.; Franzone, A.; Vranckx, P.; Hahn, J.Y.; Gwon, H.C.; Feres, F.; et al. Dual antiplatelet therapy duration after percutaneous coronary intervention in high bleeding risk: A meta-analysis of randomized trials. Eur. Heart J. 2023, 44, 954–968. [Google Scholar] [CrossRef]
- Capodanno, D.; Greco, A. Dual antiplatelet therapy in patients at high bleeding risk: Less is more-more or less. Eur. Heart J. 2023, 44, 969–971. [Google Scholar] [CrossRef]
- Lamy, A.; Eikelboom, J.; Sheth, T.; Connolly, S.; Bosch, J.; Fox, K.A.A.; Zhu, J.; Lonn, E.; Dagenais, G.; Widimsky, P.; et al. Rivaroxaban, aspirin, or both to prevent early coronary bypass graft occlusion: The COMPASS-CABG study. J. Am. Coll. Cardiol. 2019, 73, 121–130. [Google Scholar] [CrossRef]
- Galli, M.; Franchi, F.; Rollini, F.; Cavallari, L.H.; Capodanno, D.; Crea, F.; Angiolillo, D.J. Genetic testing in patients undergoing percutaneous coronary intervention: Rationale, evidence and practical recommendations. Expert Rev. Clin. Pharmacol. 2021, 14, 963–978. [Google Scholar] [CrossRef]
- McNeil, J.J.; Wolfe, R.; Woods, R.L.; Tonkin, A.M.; Donnan, G.A.; Nelson, M.R.; Reid, C.M.; Lockery, J.E.; Kirpach, B.; Storey, E.; et al. Effect of Aspirin on Cardiovascular Events and Bleeding in the Healthy Elderly. N. Engl. J. Med. 2018, 379, 1509–1518. [Google Scholar] [CrossRef]
- ASCEND Study Collaborative Group. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus. N. Engl. J. Med. 2018, 379, 1529–1539. [Google Scholar] [CrossRef]
- De Berardis, G.; Sacco, M.; Evangelista, V.; Filippi, A.; Giorda, C.B.; Tognoni, G.; Valentini, U.; Nicolucci, A.; ACCEPT-D Study Group. Aspirin and Simvastatin Combination for Cardiovascular Events Prevention Trial in Diabetes (ACCEPT-D): Design of a randomized study of the efficacy of low-dose aspirin in the prevention of cardiovascular events in subjects with diabetes mellitus treated with statins. Trials 2007, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, J.M.; Brotons, C.; Coppolecchia, R.; Cricelli, C.; Darius, H.; Gorelick, P.B.; Howard, G.; Pearson, T.A.; Rothwell, P.M.; Ruilope, L.; et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): A randomised, double-blind, placebo-controlled trial. Lancet 2018, 392, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Ajufo, E.; Ayers, C.R.; Vigen, R.; Joshi, P.H.; Rohatgi, A.; de Lemos, J.A.; Khera, A. Value of Coronary Artery Calcium Scanning in Association with the Net Benefit of Aspirin in Primary Prevention of Atherosclerotic Cardiovascular Disease. JAMA Cardiol. 2021, 6, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Belch, J.; MacCuish, A.; Campbell, I.; Cobbe, S.; Taylor, R.; Prescott, R.; Lee, R.; Bancroft, J.; MacEwan, S.; Shepherd, J.; et al. Prevention of Progression of Arterial Disease and Diabetes Study Group; Diabetes Registry Group; Royal College of Physicians Edinburgh. The prevention of progression of arterial disease and diabetes (POPADAD) trial: Factorial randomised placebo controlled trial of aspirin and antioxidants in patients with diabetes and asymptomatic peripheral arterial disease. BMJ 2008, 337, a1840. [Google Scholar] [CrossRef]
- Fowkes, F.G.; Price, J.F.; Stewart, M.C.; Butcher, I.; Leng, G.C.; Pell, A.C.; Sandercock, P.A.; Fox, K.A.; Lowe, G.D.; Murray, G.D. Aspirin for Asymptomatic Atherosclerosis Trialists. Aspirin for prevention of cardiovascular events in a general population screened for a low ankle brachial index: A randomized controlled trial. JAMA 2010, 303, 841–848. [Google Scholar] [CrossRef]
- Magnani, G.; Ardissino, D.; Im, K.; Budaj, A.; Storey, R.F.; Steg, P.G.; Bhatt, D.L.; Cohen, M.; Oude Ophius, T.; Goudev, A.; et al. Predictors, Type, and Impact of Bleeding on the Net Clinical Benefit of Long-Term Ticagrelor in Stable Patients with Prior Myocardial Infarction. J. Am. Heart Assoc. 2021, 10, e017008. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Im, K.; Magnani, G.; Bansilal, S.; Dellborg, M.; Storey, R.F.; Bhatt, D.L.; Steg, P.G.; Cohen, M.; Johanson, P.; et al. Patient selection for long-term secondary prevention with ticagrelor: Insights from PEGASUS-TIMI 54. Eur. Heart J. 2022, 43, 5037–5044. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Trial | First Author, Year | Population | Total n | Proportion with Both CAD and PAD | Comparison | Median FUP | PEP MACE HR (95% CI) | MAJOR BLEEDING HR (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Single antiplatelet therapy (more vs. less potent) | ||||||||
| CAPRIE | CAPRIE Steering Committee, 1996 [9] | Recent MI (n = 6302) or Symptomatic LE PAD (n = 6452) or Ischemic stroke (n = 6431) | 19,185 | N.A. | Clopidogrel 75 mg vs. Asprin 325 | 22.9 | LE-PAD: 0.76 (0.64–0.91) | Overall population Severe GI bleeding: 0.49% (clopidogrel) vs. 0.71% (aspirin) p < 0.05 |
| EUCLID | Hiatt WR, 2017 [10] Berger J, 2018 [11] | Symptomatic LE PAD | 13,885 | 29.0% | Ticagrelor 90 mg b.i.d. vs. Clopidogrel 75 mg | 30 | 1.02 (0.92–1.13) | 1.10 (0.84–1.43) |
| DAPT vs. Single antiplatelet therapy | ||||||||
| CHARISMA | Bhatt DL, 2006 [12] Cacoub P, 2009 [13] | CCS (n = 5835) or LE PAD (n = 2838) or Ischemic stroke/TIA (n = 4290) or multiple atherosclerotic risk factors (n = 3284) | 15,603 | N.A. | Clopidogrel 75 mg + Aspirin 75–162 mg vs. Aspirin 75–162 mg | 28 | Prior MI: 0.77 (0.62–0.98) LE-PAD: 0.85 (0.66–1.08), | Overall secondary prevention population: 1.10 (0.81–1.54) LE-PAD: 0.97 (0.56–1.66) |
| PRODIGY | Valgimigli M, 2012 [14] Franzone A, 2016 [15] | CCS (n = 505) or ACS (n = 1465) | 1970 | 12.5% | Clopidogrel 75 mg + Aspirin 80–160 mg for 24 months vs. 6 months | 28 | LE-PAD: 0.54 (0.31–0.95) NO-LE-PAD:1.28 (0.92–1.77) p-int = 0.01 | LE-PAD: 0.76 (0.17–3.40) NO-LE-PAD: 2.07 (1.12–3.83) p-int = 0.22 |
| DAPT | Secemsky EA, 2017 [16] | Patients free from ischemic and bleeding events 12 months after coronary stenting | 11,648 | 5.57% | Continued thienopyridine (clopidogrel 75 mg or prasugrel 10 mg) + Aspirin therapy for an additional 18 months vs. Aspirin 100 mg | 18 | LE-PAD: 0.63 (0.32–1.22) NO-LE-PAD: 0.53 (0.42–0.66) p-int = 0.63 | LE-PAD: 1.82 (0.87–3.83) NO-LE-PAD: 1.66 (1.23–2.24) p-int: 0.81 |
| TRA-2°P-TIMI 50 | Bonaca MP, 2012 [17] Magnani G, 2015 [18] Qamar A, 2020 [19] | Stable MI (n = 17,779) or LE PAD (n = 3787) or Ischemic stroke (n = 4883) | 26,449 | 76.3% of 6136 patients with PAD regardless of stratum | Vorapaxar 2.5 mg vs. Placebo | 30 | PAD + CAD: 0.82 (0.69–0.97) ARD −2.2 (−4.0, −0.4) PAD only: 1.0 (0.69−1.46) ARD 0.1 (−2.6, 2.9) | LE-PAD (overall population): 1.39 (1.12–1.71) |
| PEGASUS TIMI-54 | Bonaca MP, 2016 [20] | Stable MI | 21,162 | CAD + PAD 5.2% | Ticagrelor 60 or 180 mg b.i.d. + Aspirin 75–150 mg o.d. vs. or Aspirin 75–150 mg o.d. | 33 | LE-PAD (60 mg): 0.69 (0.47–0.99) | LE-PAD: (dose pooled) 1.32 (0.41–4.20) |
| Therapy with aspirin combined with an anticoagulant drug | ||||||||
| COMPASS | Eikelboom JW, 2017 [21] Connolly S, 2018 [22] Anand SS, 2018 [5] | Stable CAD (n = 24,828) or [Symptomatic LE PAD or carotid artery disease or ABI < 0.9 with CAD (n = 7470)] | 27,395 | COMPASS-CAD: 17.9% COMPASS-PAD:44.1% | Rivaroxaban 2.5 b.i.d. + Aspirin 100 mg or Rivaroxaban 5 mg b.i.d. vs. Aspirin 100 mg | 23 | Overall population: 0.76 (0.66–0.86) | Overall population: 1.49 (0.67–3.33) |
| VOYAGER-PAD | Bonaca MP, 2020 [23] | LE PAD with recent peripheral revascularization | 6564 | PAD + CAD 23.6% | Rivaroxaban 2.5 mg b.i.d. + Aspirin 100 mg vs. Aspirin 100 mg | 28 | 0.85 (0.76–0.96) | 1.42 (1.10–1.84) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magnani, G.; Denegri, A.; Gurgoglione, F.L.; Barocelli, F.; Indrigo, E.; Catellani, D.; Signoretta, G.; Bettella, A.; Tuttolomondo, D.; Solinas, E.; et al. Dual Antiplatelet Therapy or Antiplatelet Plus Anticoagulant Therapy in Patients with Peripheral and Chronic Coronary Artery Disease: An Updated Review. J. Clin. Med. 2023, 12, 5284. https://doi.org/10.3390/jcm12165284
Magnani G, Denegri A, Gurgoglione FL, Barocelli F, Indrigo E, Catellani D, Signoretta G, Bettella A, Tuttolomondo D, Solinas E, et al. Dual Antiplatelet Therapy or Antiplatelet Plus Anticoagulant Therapy in Patients with Peripheral and Chronic Coronary Artery Disease: An Updated Review. Journal of Clinical Medicine. 2023; 12(16):5284. https://doi.org/10.3390/jcm12165284
Chicago/Turabian StyleMagnani, Giulia, Andrea Denegri, Filippo Luca Gurgoglione, Federico Barocelli, Elia Indrigo, Davide Catellani, Gianluca Signoretta, Alberto Bettella, Domenico Tuttolomondo, Emilia Solinas, and et al. 2023. "Dual Antiplatelet Therapy or Antiplatelet Plus Anticoagulant Therapy in Patients with Peripheral and Chronic Coronary Artery Disease: An Updated Review" Journal of Clinical Medicine 12, no. 16: 5284. https://doi.org/10.3390/jcm12165284
APA StyleMagnani, G., Denegri, A., Gurgoglione, F. L., Barocelli, F., Indrigo, E., Catellani, D., Signoretta, G., Bettella, A., Tuttolomondo, D., Solinas, E., Nicolini, F., Niccoli, G., & Ardissino, D. (2023). Dual Antiplatelet Therapy or Antiplatelet Plus Anticoagulant Therapy in Patients with Peripheral and Chronic Coronary Artery Disease: An Updated Review. Journal of Clinical Medicine, 12(16), 5284. https://doi.org/10.3390/jcm12165284