

Postoperative Rehabilitation after Anterior Cruciate Ligament Reconstruction through Telerehabilitation with Artificial Intelligence Brace during COVID-19 Pandemic
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient’s Population
2.2. Rehabilitation Protocol
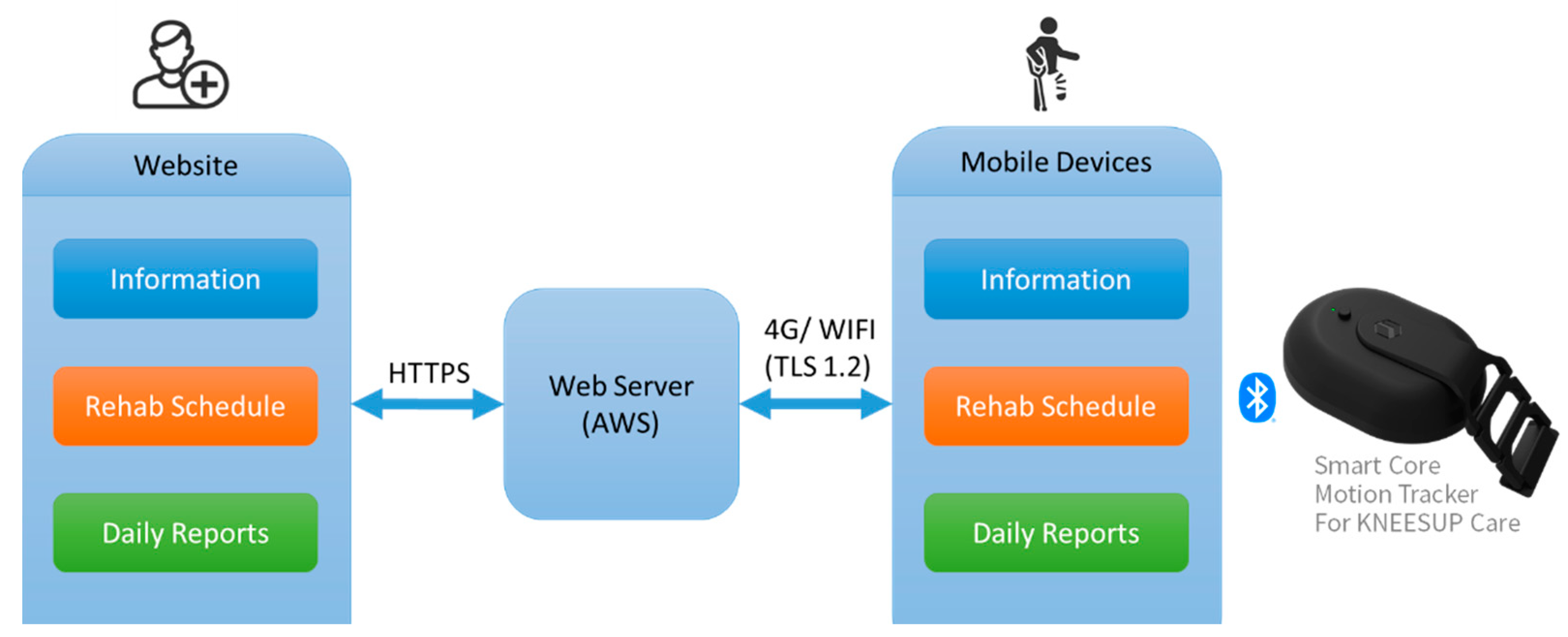
2.3. Home-Based Telerehabilitation
2.4. Face-to Face Hospital-Based Rehabilitation
2.5. Clinical Outcome Evaluation
2.6. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wright, R.W.; Preston, E.; Fleming, B.C.; Amendola, A.; Andrish, J.; Bergfeld, J.; Dunn, W.; Kaeding, C.; Kuhn, J.; Marx, R.; et al. A systematic review of anterior cruciate ligament reconstruction rehabilitation: Part II: Open versus closed kinetic chain exercises, neuromuscular electrical stimulation, accelerated rehabilitation, and miscellaneous topics. J. Knee Surg. 2008, 21, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Kruse, L.M.; Gray, B.; Wright, R.W. Rehabilitation after anterior cruciate ligament reconstruction: A systematic review. J. Bone Jt. Surg. Am. 2012, 94, 1737–1748. [Google Scholar] [CrossRef] [PubMed]
- Kannan, S.; Shaik Syed Ali, P.; Sheeza, A.; Hemalatha, K. COVID-19 (Novel Coronavirus 2019)—Recent trends. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2006–2011. [Google Scholar] [CrossRef] [PubMed]
- Russell, T.G.; Buttrum, P.; Wootton, R.; Jull, G.A. Internet-based outpatient telerehabilitation for patients following total knee arthroplasty: A randomized controlled trial. J. Bone Jt. Surg. Am. 2011, 93, 113–120. [Google Scholar] [CrossRef]
- Tousignant, M.; Moffet, H.; Boissy, P.; Corriveau, H.; Cabana, F.; Marquis, F. A randomized controlled trial of home telerehabilitation for post-knee arthroplasty. J. Telemed. Telecare 2011, 17, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Piqueras, M.; Marco, E.; Coll, M.; Ballester, A.; Cinca, C.; Belmonte, R.; Muniesa, J. Effectiveness of an interactive virtual telerehabilitation system in patients after total knee arthoplasty: A randomized controlled trial. J. Rehabil. Med. 2013, 45, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Moffet, H.; Tousignant, M.; Nadeau, S.; Mérette, C.; Boissy, P.; Corriveau, H.; Marquis, F.; Cabana, F.; Ranger, P.; Belzile, É.L.; et al. In-Home Telerehabilitation Compared with Face-to-Face Rehabilitation After Total Knee Arthroplasty: A Noninferiority Randomized Controlled Trial. J. Bone Jt. Surg. Am. 2015, 97, 1129–1141. [Google Scholar] [CrossRef]
- Shukla, H.; Nair, S.R.; Thakker, D. Role of telerehabilitation in patients following total knee arthroplasty: Evidence from a systematic literature review and meta-analysis. J. Telemed. Telecare 2017, 23, 339–346. [Google Scholar] [CrossRef]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef]
- Pastora-Bernal, J.M.; Martín-Valero, R.; Barón-López, F.J.; Estebanez-Pérez, M.J. Evidence of Benefit of Telerehabitation After Orthopedic Surgery: A Systematic Review. J. Med. Internet Res. 2017, 19, e142. [Google Scholar] [CrossRef]
- Burns, R.B.; Crislip, D.; Daviou, P.; Temkin, A.; Vesmarovich, S.; Anshutz, J.; Furbish, C.; Jones, M.L. Using telerehabilitation to support assistive technology. Assist. Technol. 1998, 10, 126–133. [Google Scholar] [CrossRef]
- Rennie, K.; Taylor, C.; Corriero, A.C.; Chong, C.; Sewell, E.; Hadley, J.; Ardani, S. The Current Accuracy, Cost-Effectiveness, and Uses of Musculoskeletal Telehealth and Telerehabilitation Services. Curr. Sports Med. Rep. 2022, 21, 247–260. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef]
- Rodríguez-Merchán, E.C. Knee Bracing After Anterior Cruciate Ligament Reconstruction. Orthopedics 2016, 39, e602–e609. [Google Scholar] [CrossRef]
- Kuster, M.S.; Grob, K.; Kuster, M.; Wood, G.A.; Gächter, A. The benefits of wearing a compression sleeve after ACL reconstruction. Med. Sci. Sports Exerc. 1999, 31, 368–371. [Google Scholar] [CrossRef][Green Version]
- Rebel, M.; Paessler, H.H. The effect of knee brace on coordination and neuronal leg muscle control: An early postoperative functional study in anterior cruciate ligament reconstructed patients. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.W.; Fetzer, G.B. Bracing after ACL reconstruction: A systematic review. Clin. Orthop. Relat. Res. 2007, 455, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Agostini, M.; Moja, L.; Banzi, R.; Pistotti, V.; Tonin, P.; Venneri, A.; Turolla, A. Telerehabilitation and recovery of motor function: A systematic review and meta-analysis. J. Telemed. Telecare 2015, 21, 202–213. [Google Scholar] [CrossRef]
- Moffet, H.; Tousignant, M.; Nadeau, S.; Mérette, C.; Boissy, P.; Corriveau, H.; Marquis, F.; Cabana, F.; Belzile, L.; Ranger, P.; et al. Patient Satisfaction with In-Home Telerehabilitation After Total Knee Arthroplasty: Results from a Randomized Controlled Trial. Telemed. J. E Health 2017, 23, 80–87. [Google Scholar] [CrossRef]
- Correia, F.D.; Nogueira, A.; Magalhães, I.; Guimarães, J.; Moreira, M.; Barradas, I.; Molinos, M.; Teixeira, L.; Tulha, J.; Seabra, R.; et al. Medium-Term Outcomes of Digital Versus Conventional Home-Based Rehabilitation After Total Knee Arthroplasty: Prospective, Parallel-Group Feasibility Study. JMIR Rehabil. Assist. Technol. 2019, 6, e13111. [Google Scholar] [CrossRef]
- Kuether, J.; Moore, A.; Kahan, J.; Martucci, J.; Messina, T.; Perreault, R.; Sembler, R.; Tarutis, J.; Zazulak, B.; Rubin, L.E.; et al. Telerehabilitation for Total Hip and Knee Arthroplasty Patients: A Pilot Series with High Patient Satisfaction. HSS J. 2019, 15, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, L.; Lindström, B.; Gard, G.; Lysholm, J. Physiotherapy at a distance: A controlled study of rehabilitation at home after a shoulder joint operation. J. Telemed. Telecare 2009, 15, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Skolasky, R.L.; Maggard, A.M.; Li, D.; Riley, L.H., 3rd; Wegener, S.T. Health behavior change counseling in surgery for degenerative lumbar spinal stenosis. Part I: Improvement in rehabilitation engagement and functional outcomes. Arch. Phys. Med. Rehabil. 2015, 96, 1200–1207. [Google Scholar] [CrossRef] [PubMed]
- Tousignant, M.; Moffet, H.; Nadeau, S.; Mérette, C.; Boissy, P.; Corriveau, H.; Marquis, F.; Cabana, F.; Ranger, P.; Belzile, É.L.; et al. Cost analysis of in-home telerehabilitation for post-knee arthroplasty. J. Med. Internet Res. 2015, 17, e83. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Chang, J.; Hoit, G.; Chahal, J.; Dwyer, T.; Theodoropoulos, J. Conventional Follow-up Versus Mobile Application Home Monitoring for Postoperative Anterior Cruciate Ligament Reconstruction Patients: A Randomized Controlled Trial. Arthroscopy 2020, 36, 1906–1916. [Google Scholar] [CrossRef] [PubMed]
- Bauwens, P.H.; Fayard, J.M.; Tatar, M.; Abid, H.; Freychet, B.; Sonnery-Cottet, B.; Thaunat, M. Evaluation of a smartphone application for self-rehabilitation after anterior cruciate ligament reconstruction during a COVID-19 lockdown. Orthop. Traumatol. Surg. Res. 2023, 109, 103342. [Google Scholar] [CrossRef]
- Bouguennec, N.; Orce, A.; Laboudie, P.; Pelletier, S.; Dexhelet, J.; Graveleau, N. Association of COVID-19 Lockdown with Increased Rate of Cyclops Syndrome in Patients with Unexpected Home-Based Self-Guided Rehabilitation After ACL Reconstruction. Orthop. J. Sports Med. 2023, 11, 23259671221147869. [Google Scholar] [CrossRef]
- Collins, N.J.; Prinsen, C.A.; Christensen, R.; Bartels, E.M.; Terwee, C.B.; Roos, E.M. Knee Injury and Osteoarthritis Outcome Score (KOOS): Systematic review and meta-analysis of measurement properties. Osteoarthr. Cartil. 2016, 24, 1317–1329. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Post Operative Period | Rehabilitation Task |
|---|---|
| 1–2 weeks | Range of motion 0–45 degrees Partial weight bearing with crutch Quadriceps muscle isometric contraction Straight leg raise Ankle pumping |
| 3 weeks | Range of motion 0–60 degrees Full weight bearing as tolerated Gait and balance training Passive stretch for knee extension quadriceps Heel slide on wall |
| 4 weeks | Range of motion 0–90 degrees Passive stretch for knee extension in prone position Patella mobilization Semi-squat and heel-up |
| 5–8 weeks | Range of motion not restricted Wall squat Stairs up and stairs down |
| 8–12 weeks | Range of motion not restricted Plunk and bridging exercise Single leg squat Single leg stands with eyes closed Advanced stairs up and stairs down |
| 12–16 weeks | Jump rope Jogging straight on the even road |
| 16–24 weeks | Advanced stairs up and stairs down Advanced single leg squat Single leg crossing cone reach Jump and single leg land Single leg hops in place |
| After 24 weeks | Jogging on the uneven road or jogging with turns Acceleration or deceleration running Sports specific activity |
| Tele-AI Group | FTF Group | p Value | |
|---|---|---|---|
| No. | 15 | 15 | |
| Age at surgery (years) | |||
| Mean ± SD | 26.27 ± 8.59 | 28.60 ± 9.30 | 0.482 |
| Median | 24 | 26 | |
| Range | 17–43 | 17–50 | |
| No. of male/female patients | 11/4 | 10/5 | 0.787 |
| No. of right/left injuries | 8/7 | 7/8 | 0.608 |
| No. of sports/traumatic injuries | 13/2 | 13/2 | 1.000 |
| Tele-AI Group | FTF Group | ||
|---|---|---|---|
| Mean ± SD | Mean ± SD | p value | |
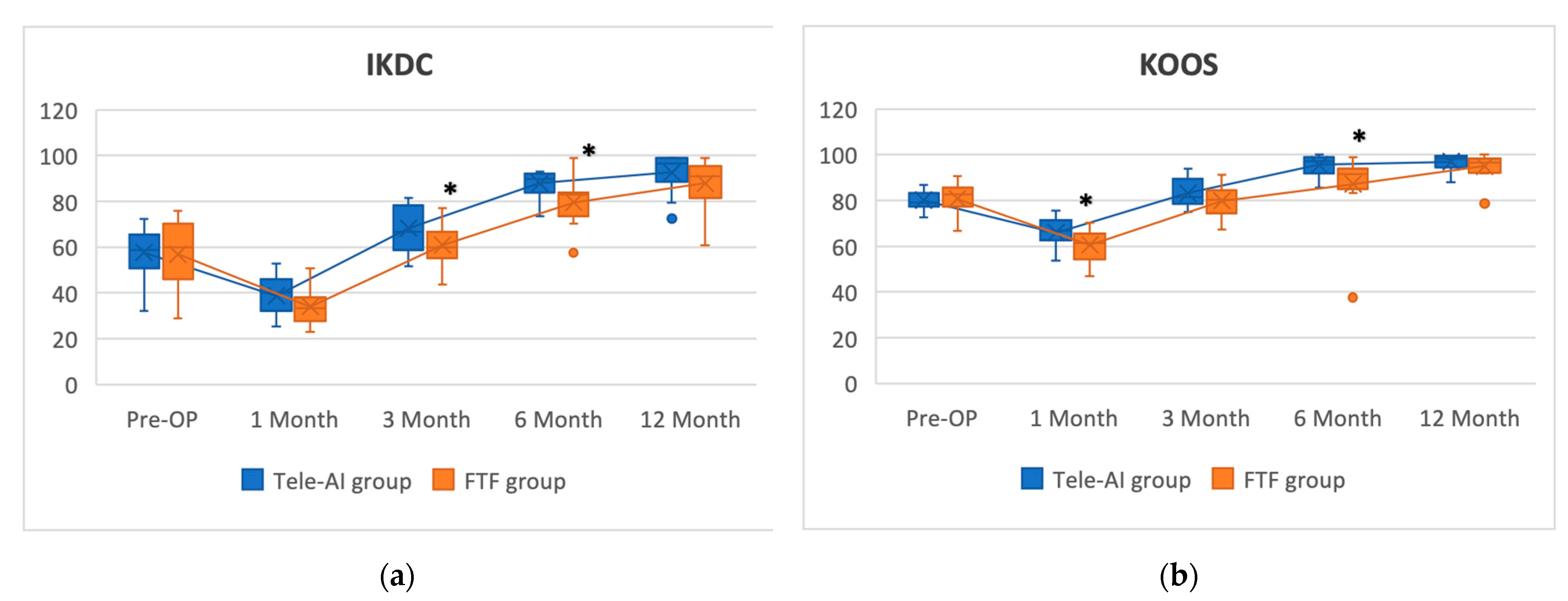
| IKDC | |||
| Pre-OP | 57.63 ± 10.95 | 56.78 ± 14.78 | 0.2738 |
| Post-OP 1 m | 38.62 ± 8.73 | 34.01 ± 8.16 | 0.1467 |
| Post-OP 3 m | 68.21 ± 9.66 | 60.77 ± 9.67 | 0.0443 * |
| Post-OP 6 m | 87.84 ± 5.55 | 79.49 ± 9.11 | 0.0052 * |
| Post-OP 12 m | 92.67 ± 8.27 | 87.83 ± 9.85 | 0.1568 |
| KOOS | |||
| Pre-OP | 80 ± 3.91 | 80.71 ± 7.04 | 0.734 |
| Post-OP 1 m | 65.85 ± 6.57 | 60.56 ± 6.61 | 0.0365 * |
| Post-OP 3 m | 83.18 ± 6.13 | 79.77 ± 6.02 | 0.1353 |
| Post-OP 6 m | 95.59 ± 4.19 | 87.13 ± 14.40 | 0.0375 * |
| Post-OP 12 m | 96.9 ± 32.8 | 94.9 ± 5.38 | 0.2306 |
| Tele-AI Group | FTF Group | Tele-AI Group | FTF Group | Tele-AI Group | FTF Group | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | p Value | Mean ± SD | Mean ± SD | p Value | Mean ± SD | Mean ± SD | p Value | |
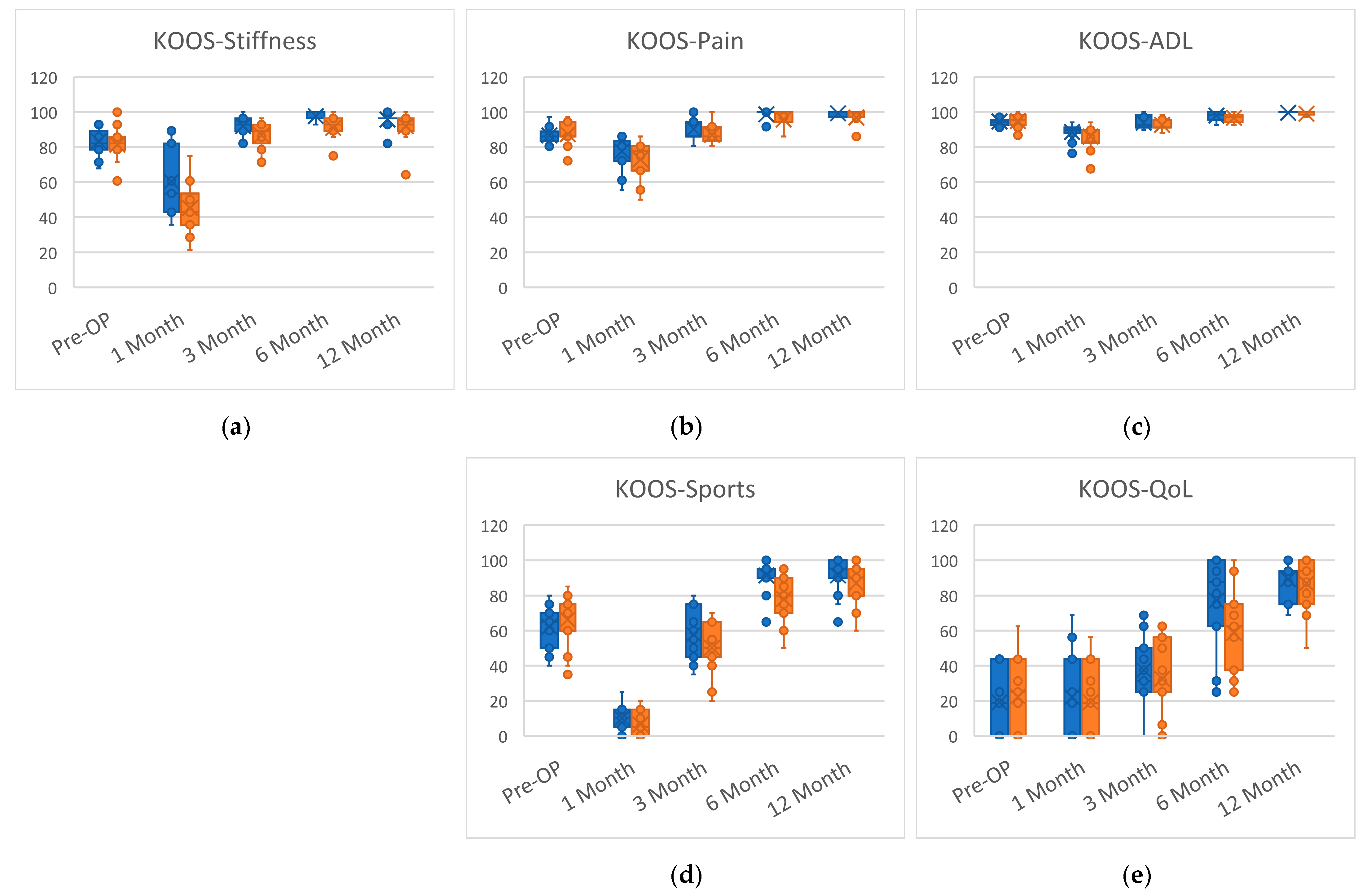
| KOOS-Symptoms | KOOS-Pain | KOOS-ADL | |||||||
| Pre-OP | 83.33 ± 7.72 | 81.43 ± 10.39 | 0.571 | 86.67 ± 4.72 | 87.41 ± 6.71 | 0.478 | 94.61 ± 2.13 | 94.81 ± 4.41 | 0.413 |
| Post-OP 1 m | 60.24 ± 18.65 | 45.24 ± 14.01 | 0.024 * | 77.59 ± 9.71 | 72.96 ± 11.47 | 0.134 | 88.63 ± 4.39 | 85.98 ± 6.92 | 0.221 |
| Post-OP 3 m | 91.91 ± 6.11 | 86.91 ± 8.17 | 0.093 | 90.37 ± 6.71 | 87.04 ± 5.52 | 0.14 | 93.92 ± 3.51 | 92.75 ± 3.21 | 0.239 |
| Post-OP 6 m | 97.62 ± 2.58 | 90.95 ± 6.87 | 0.001 * | 98.70 ± 2.75 | 95.74 ± 4.05 | 0.020 * | 97.94 ± 2.65 | 96.77 ± 2.37 | 0.093 |
| Post-OP 12 m | 95.8 ± 4.31 | 91.9 ± 8.69 | 0.146 | 99.26 ± 4.31 | 96.85 ± 4.68 | 0.096 | 99.61 ± 0.87 | 99.02 ± 1.98 | 0.334 |
| KOOS-Sport/Rec | KOOS-QoL | ||||||||
| Pre-OP | 62.33 ± 11.63 | 66.33 ± 15.17 | 0.178 | 19.17 ± 18.37 | 22.50 ± 21.62 | 0.68 | |||
| Post-OP 1 m | 10.00 ± 6.81 | 6.33 ± 7.19 | 0.183 | 22.08 ± 22.76 | 19.17 ± 20.66 | 0.777 | |||
| Post-OP 3 m | 58.00 ± 14.12 | 50.33 ± 14.07 | 0.24 | 37.50 ± 19.48 | 32.50 ± 21.29 | 0.537 | |||
| Post-OP 6 m | 91.33 ± 8.96 | 78.00 ± 13.99 | 0.004 * | 77.08 ± 28.02 | 58.75 ± 23.36 | 0.039 * | |||
| Post-OP 12 m | 91.33 ± 10.43 | 87 ± 11.62 | 0.359 | 89.17 ± 10.42 | 86.67 ± 14.92 | 0.618 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, W.-J.; Lee, K.-T.; Chiang, L.-Y.; Liang, C.-H.; Chen, C.-P. Postoperative Rehabilitation after Anterior Cruciate Ligament Reconstruction through Telerehabilitation with Artificial Intelligence Brace during COVID-19 Pandemic. J. Clin. Med. 2023, 12, 4865. https://doi.org/10.3390/jcm12144865
Liao W-J, Lee K-T, Chiang L-Y, Liang C-H, Chen C-P. Postoperative Rehabilitation after Anterior Cruciate Ligament Reconstruction through Telerehabilitation with Artificial Intelligence Brace during COVID-19 Pandemic. Journal of Clinical Medicine. 2023; 12(14):4865. https://doi.org/10.3390/jcm12144865
Chicago/Turabian StyleLiao, Wei-Jen, Kun-Tsan Lee, Liang-Yu Chiang, Che-Han Liang, and Chao-Ping Chen. 2023. "Postoperative Rehabilitation after Anterior Cruciate Ligament Reconstruction through Telerehabilitation with Artificial Intelligence Brace during COVID-19 Pandemic" Journal of Clinical Medicine 12, no. 14: 4865. https://doi.org/10.3390/jcm12144865
APA StyleLiao, W.-J., Lee, K.-T., Chiang, L.-Y., Liang, C.-H., & Chen, C.-P. (2023). Postoperative Rehabilitation after Anterior Cruciate Ligament Reconstruction through Telerehabilitation with Artificial Intelligence Brace during COVID-19 Pandemic. Journal of Clinical Medicine, 12(14), 4865. https://doi.org/10.3390/jcm12144865