
Effectiveness of Repetitive Transcranial Magnetic Stimulation in the Treatment of Depression in the Elderly: A Retrospective Natural Analysis

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borges, M.K.; Romanini, C.V.; Lima, N.A.; Petrella, M.; da Costa, D.L.; An, V.N.; Aguirre, B.N.; Galdeano, J.R.; Fernandes, I.C.; Cecato, J.F.; et al. Longitudinal Association between Late-Life Depression (LLD) and Frailty: Findings from a Prospective Cohort Study (MiMiCS-FRAIL). J. Nutr. Health Aging 2021, 25, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Avasthi, A.; Grover, S. Clinical practice guidelines for management of depression in elderly. Indian J. Psychiatry 2018, 60, S341–S362. [Google Scholar] [CrossRef]
- Luppa, M.; Sikorski, C.; Motzek, T.; Konnopka, A.; Konig, H.H.; G Riedel-Heller, S. Health Service Utilization and Costs of Depressive Symptoms in Late Life—A Systematic Review. Curr. Pharm. Des. 2012, 18, 5936–5957. [Google Scholar] [CrossRef]
- Hegeman, J.M.; Kok, R.M.; van der Mast, R.C.; Giltay, E.J. Phenomenology of depression in older compared with younger adults: Meta-analysis. Br. J. Psychiatry 2012, 200, 275–281. [Google Scholar] [CrossRef]
- Szymkowicz, S.M.; Gerlach, A.R.; Homiack, D.; Taylor, W.D. Biological factors influencing depression in later life: Role of aging processes and treatment implications. Transl. Psychiatry 2023, 13, 160. [Google Scholar] [CrossRef]
- Valiengo, L.; Pinto, B.S.; Marinho, K.A.; Santos, L.A.; Tort, L.C.; Benatti, R.G.; Teixeira, B.B.; Miranda, C.S.; Cardeal, H.B.; Suen, P.J.C.; et al. Treatment of depression in the elderly with repetitive transcranial magnetic stimulation using theta-burst stimulation: Study protocol or a randomized, double-blind, controlled trial. Front. Hum. Neurosci. 2022, 16, 941981. [Google Scholar] [CrossRef] [PubMed]
- Giron, M.S.T.; Fastbom, J.; Winblad, B. Clinical trials of potential antidepressants: To what extent are the elderly represented: A review. Int. J. Geriatr. Psychiatry 2005, 20, 201–217. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.D. Depression in the Elderly. N. Engl. J. Med. 2014, 371, 1228–1236. [Google Scholar] [CrossRef]
- Roose, S.P.; Rutherford, B.R.; Nelson, J.C.; Delucchi, K.L.; Schneider, L.S.; Alexopoulos, G.S.; Raskin, J.; Wiltse, C.G.; Siegal, A.; Sheikh, J.; et al. Antidepressant Pharmacotherapy in the Treatment of Depression in the Very Old: A Randomized, Placebo-Controlled Trial. Am. J. Psychiatry 2004, 161, 2050–2059. [Google Scholar] [CrossRef]
- Blumberger, D.M.; Hsu, J.H.; Daskalakis, Z.J. A Review of Brain Stimulation Treatments for Late-Life Depression. Curr. Treat. Options Psychiatry 2015, 2, 413–421. [Google Scholar] [CrossRef]
- McDonald, W.M. Neuromodulation Treatments for Geriatric Mood and Cognitive Disorders. Am. J. Geriatr. Psychiatry 2016, 24, 1130–1141. [Google Scholar] [CrossRef]
- Rossi, S.; Antal, A.; Bestmann, S.; Bikson, M.; Brewer, C.; Brockmöller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin. Neurophysiol. 2021, 132, 269–306. [Google Scholar] [CrossRef]
- Lefaucheur, J.P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; Di Lazzaro, V.; Filipovic, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.C.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef]
- Klomjai, W.; Katz, R.; Lackmy-Vallée, A. Basic principles of transcranial magnetic stimulation (TMS) and repetitive TMS (rTMS). Ann. Phys. Rehabil. Med. 2015, 58, 208–213. [Google Scholar] [CrossRef]
- Hebel, T.; Grozinger, M.; Landgrebe, M.; Padberg, F.; Schecklmann, M.; Schlaepfer, T.; Schonfeldt-Lecuona, C.; Ullrich, H.; Zwanzger, P.; Langguth, B.; et al. Evidence and expert consensus based German guidelines for the use of repetitive transcranial magnetic stimulation in depression. World J. Biol. Psychiatry 2022, 23, 327–348. [Google Scholar] [CrossRef] [PubMed]
- Overvliet, G.M.; Jansen, R.A.C.; van Balkom, A.J.L.M.; van Campen, D.C.; Oudega, M.L.; van der Werf, Y.D.; van Exel, E.; Heuvel, O.A.V.D.; Dols, A. Adverse events of repetitive transcranial magnetic stimulation in older adults with depression, a systematic review of the literature. Int. J. Geriatr. Psychiatry 2020, 36, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Sabesan, P.; Lankappa, S.; Khalifa, N.; Krishnan, V.; Gandhi, R.; Palaniyappan, L. Transcranial magnetic stimulation for geriatric depression: Promises and pitfalls. World J. Psychiatry 2015, 5, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Iriarte, I.G.; George, M.S. Transcranial Magnetic Stimulation (TMS) in the Elderly. Curr. Psychiatry Rep. 2018, 20, 6. [Google Scholar] [CrossRef]
- George, M.S.; Lisanby, S.H.; Avery, D.; McDonald, W.M.; Durkalski, V.; Pavlicova, M.; Anderson, B.; Nahas, Z.; Bulow, P.; Zarkowski, P.; et al. Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: A sham-controlled randomized trial. Arch. Gen. Psychiatry 2010, 67, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Valiengo, L.; Maia, A.; Cotovio, G.; Gordon, P.C.; Brunoni, A.R.; Forlenza, O.V.; Oliveira-Maia, A.J. Repetitive Transcranial Magnetic Stimulation for Major Depressive Disorder in Older Adults: Systematic Review and Meta-analysis. J. Gerontol. Ser. A 2022, 77, 851–860. [Google Scholar] [CrossRef]
- Abdelnaim, M.A.; Langguth, B.; Deppe, M.; Mohonko, A.; Kreuzer, P.M.; Poeppl, T.B.; Hebel, T.; Schecklmann, M. Anti-Suicidal Efficacy of Repetitive Transcranial Magnetic Stimulation in Depressive Patients: A Retrospective Analysis of a Large Sample. Front. Psychiatry 2019, 10, 929. [Google Scholar] [CrossRef] [PubMed]
- Frank, E.; Eichhammer, P.; Burger, J.; Zowe, M.; Landgrebe, M.; Hajak, G.; Langguth, B. Transcranial magnetic stimulation for the treatment of depression: Feasibility and results under naturalistic conditions: A retrospective analysis. Eur. Arch. Psychiatry Clin. Neurosci. 2011, 261, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Hebel, T.; Abdelnaim, M.; Deppe, M.; Langguth, B.; Schecklmann, M. Attenuation of antidepressive effects of transcranial magnetic stimulation in patients whose medication includes drugs for psychosis. J. Psychopharmacol. 2020, 34, 1119–1124. [Google Scholar] [CrossRef] [PubMed]
- Hebel, T.; Abdelnaim, M.A.; Deppe, M.; Kreuzer, P.M.; Mohonko, A.; Poeppl, T.B.; Rupprecht, R.; Langguth, B.; Schecklmann, M. Antidepressant effect of repetitive transcranial magnetic stimulation is not impaired by intake of lithium or antiepileptic drugs. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 1245–1253. [Google Scholar] [CrossRef]
- Deppe, M.; Abdelnaim, M.; Hebel, T.; Kreuzer, P.M.; Poeppl, T.B.; Langguth, B.; Schecklmann, M. Concomitant lorazepam use and antidepressive efficacy of repetitive transcranial magnetic stimulation in a naturalistic setting. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 61–67. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Trajković, G.; Starčević, V.; Latas, M.; Leštarević, M.; Ille, T.; Bukumirić, Z.; Marinković, J. Reliability of the Hamilton Rating Scale for Depression: A meta-analysis over a period of 49 years. Psychiatry Res. 2011, 189, 1–9. [Google Scholar] [CrossRef]
- Kallioniemi, E.; Julkunen, P. Alternative Stimulation Intensities for Mapping Cortical Motor Area with Navigated TMS. Brain Topogr. 2016, 29, 395–404. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Kessler, R.C. Epidemiology of women and depression. J. Affect. Disord. 2003, 74, 5–13. [Google Scholar] [CrossRef]
- Girgus, J.S.; Yang, K.; Ferri, C.V. The Gender Difference in Depression: Are Elderly Women at Greater Risk for Depression Than Elderly Men? Geriatrics 2017, 2, 35. [Google Scholar] [CrossRef] [PubMed]
- Hebel, T.; Göllnitz, A.; Schoisswohl, S.; Weber, F.C.; Abdelnaim, M.; Wetter, T.C.; Rupprecht, R.; Langguth, B.; Schecklmann, M. A direct comparison of neuronavigated and non-neuronavigated intermittent theta burst stimulation in the treatment of depression. Brain Stimul. 2021, 14, 335–343. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| <60 Years (n = 427) | ≥60 Years (n = 78) | Statistics for Group Contrasts | |
|---|---|---|---|
| age (years) | 43 ± 11 | 66 ± 5 | T = 18.532; df = 503; p < 0.001 |
| sex (female/male) | 222/205 (52% female) | 51/27 (65% female) | χ2 = 4.764; df = 1; p = 0.029 |
| resting motor threshold | 43 ± 10 | 41 ± 9 | T = 1.591; df = 500; p = 0.112 |
| stimulation intensity | 45 ± 8 | 45 ± 9 | T = 0.557; df = 503; p = 0.578 |
| number of pulses per session | 1886 ± 395 | 1859 ± 450 | T = 0.538; df = 503; p = 0.591 |
| number of sessions per patient/treatment | 18 ± 7 | 15 ± 6 | T = 1.098; df = 503; p = 0.273 |
| diagnosis (unipolar/bipolar) | 389/38 | 70/8 | χ2 = 0.147; df = 1; p = 0.702 |
| HDRS-21 baseline | 22 ± 7 | 21 ± 6 | T = 0.705; df = 503; p = 0.481 |
| HDRS-21 absolute change (from pre to post treatment) | 7 ± 8 | 7 ± 7 | T = 0.124; df = 503; p = 0.902; d = 0.016 |
| HDRS-21 relative change (%; from pre to post treatment) | 30 ± 37 | 32 ± 33 | T = 0.445; df = 503; p = 0.657; d = 0.057 |
| response rate [yes/no] (relative frequency of responders) | 128/299 (30%) | 26/52 (33%) | χ2 = 0.351; df = 1; p = 0.554 |
| remission rate (yes/no) | 153/274 (36%) | 28/50 (36%) | χ2 < 0.001; df = 1; p = 0.991 |
| <60 Years (n = 366) | ≥60 Years (n = 68) | Statistics for Group Contrasts (df = 1) | |
|---|---|---|---|
| selective serotonin reuptake inhibitors | 117 (32%) | 23 (34%) | χ2 = 0.090; p = 0.764 |
| serotonin-norepinephrine reuptake inhibitors | 185 (51%) | 37 (55%) | χ2 = 0.343; p = 0.558 |
| tricyclic antidepressants | 111 (30%) | 15 (22%) | χ2 = 1.903; p = 0.168 |
| tetracyclic antidepressants | 0 (0%) | 2 (3%) | not interpretable |
| monoamine oxidase inhibitors | 11 (3%) | 2 (3%) | χ2 = 0.001; p = 0.977 |
| benzodiazepines | 115 (31%) | 22 (32%) | χ2 = 0.023; p = 0.879 |
| z-drugs | 41 (11%) | 6 (9%) | χ2 = 0.336; p = 0.562 |
| mood stabilizers | 122 (33%) | 31 (46%) | χ2 = 3.773; p = 0.052 |
| antipsychotics | 228 (62%) | 48 (71%) | χ2 = 1.704; p = 0.192 |
| other antidepressants | 148 (40%) | 32 (47%) | χ2 = 1.036; p = 0.309 |
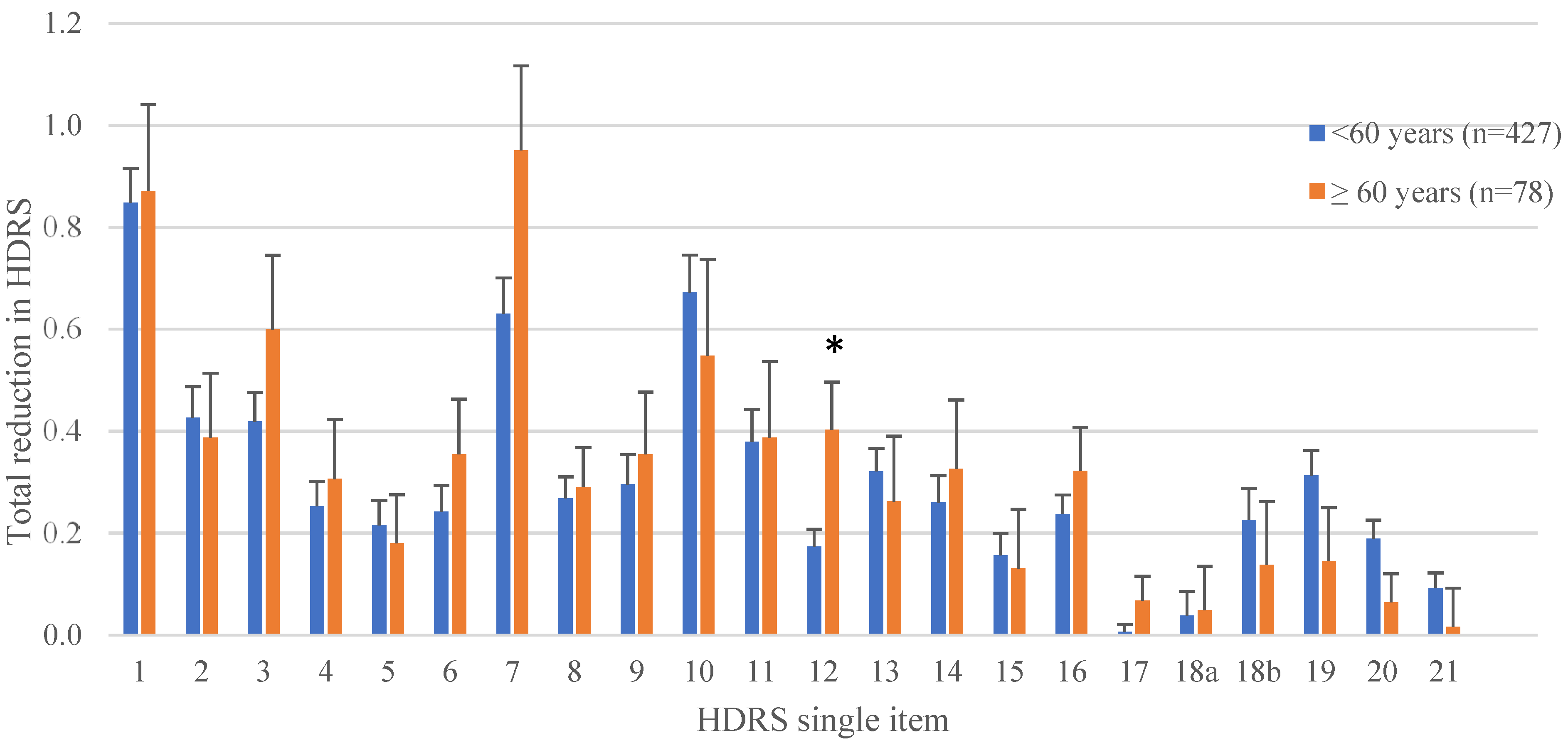
| Single Item | Total Reduction in Patients <60 Years (n = 427) | Total Reduction in Patients ≥60 Years (n = 78) | Statistics |
|---|---|---|---|
| 1—Depressed mood | 0.8 | 0.9 | p = 0.839, d = 0.019 |
| 2—Feelings of guilt | 0.4 | 0.4 | p = 0.788, d = 0.037 |
| 3—Suicide | 0.4 | 0.6 | p = 0.216, d = 0.175 |
| 4—Initial insomnia | 0.3 | 0.3 | p = 0.660, d = 0.061 |
| 5—Insomnia during the night | 0.2 | 0.2 | p = 0.761, d = 0.043 |
| 6—Delayed insomnia | 0.2 | 0.4 | p = 0.364, d = 0.127 |
| 7—Work and interests | 0.6 | 1.0 | p = 0.068, d = 0.256 |
| 8—Retardation | 0.3 | 0.3 | p = 0.828, d = 0.030 |
| 9—Agitation | 0.3 | 0.4 | p = 0.676, d = 0.058 |
| 10—Psychiatric anxiety | 0.7 | 0.5 | p = 0.506, d = 0.093 |
| 11—Somatic anxiety | 0.4 | 0.4 | p = 0.963, d = 0.007 |
| 12—Appetite | 0.2 | 0.4 | p = 0.009, d = 0.365 |
| 13—General somatic symptoms | 0.3 | 0.3 | p = 0.608, d = 0.072 |
| 14—Genital symptoms | 0.3 | 0.3 | p = 0.640, d = 0.072 |
| 15—Hypochondriasis | 0.2 | 0.1 | p = 0.813, d = 0.033 |
| 16—Weight loss | 0.2 | 0.3 | p = 0.357, d = 0.128 |
| 17—Illness insight | 0 | 0.1 | p = 0.104, d = 0.232 |
| 18a—Diurnal variation “when” | 0 | 0 | p = 0.924, d = 0.013 |
| 18b—Diurnal variation “severity” | 0.2 | 0.1 | p = 0.553, d = 0.085 |
| 19—Depersonalization | 0.3 | 0.1 | p = 0.160, d = 0.196 |
| 20—Paranoid symptoms | 0.2 | 0.1 | p = 0.147, d = 0.202 |
| 21—Obsessive symptoms | 0.1 | 0 | p = 0.312, d = 0.142 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almheiri, E.; Alhelali, A.; Abdelnaim, M.A.; Weber, F.C.; Langguth, B.; Schecklmann, M.; Hebel, T. Effectiveness of Repetitive Transcranial Magnetic Stimulation in the Treatment of Depression in the Elderly: A Retrospective Natural Analysis. J. Clin. Med. 2023, 12, 4748. https://doi.org/10.3390/jcm12144748
Almheiri E, Alhelali A, Abdelnaim MA, Weber FC, Langguth B, Schecklmann M, Hebel T. Effectiveness of Repetitive Transcranial Magnetic Stimulation in the Treatment of Depression in the Elderly: A Retrospective Natural Analysis. Journal of Clinical Medicine. 2023; 12(14):4748. https://doi.org/10.3390/jcm12144748
Chicago/Turabian StyleAlmheiri, Eisa, Abdullah Alhelali, Mohamed A. Abdelnaim, Franziska C. Weber, Berthold Langguth, Martin Schecklmann, and Tobias Hebel. 2023. "Effectiveness of Repetitive Transcranial Magnetic Stimulation in the Treatment of Depression in the Elderly: A Retrospective Natural Analysis" Journal of Clinical Medicine 12, no. 14: 4748. https://doi.org/10.3390/jcm12144748
APA StyleAlmheiri, E., Alhelali, A., Abdelnaim, M. A., Weber, F. C., Langguth, B., Schecklmann, M., & Hebel, T. (2023). Effectiveness of Repetitive Transcranial Magnetic Stimulation in the Treatment of Depression in the Elderly: A Retrospective Natural Analysis. Journal of Clinical Medicine, 12(14), 4748. https://doi.org/10.3390/jcm12144748