
Single versus Dual-Operator Approaches for Percutaneous Coronary Interventions within Chronic Total Occlusion—An Analysis of 27,788 Patients

 ,
,  ,
,  , , , , , and
, , , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Definitions
2.3. Study Endpoints
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics at Baseline
3.2. Procedural Indices, Pharmacotherapy, and Procedural Outcomes
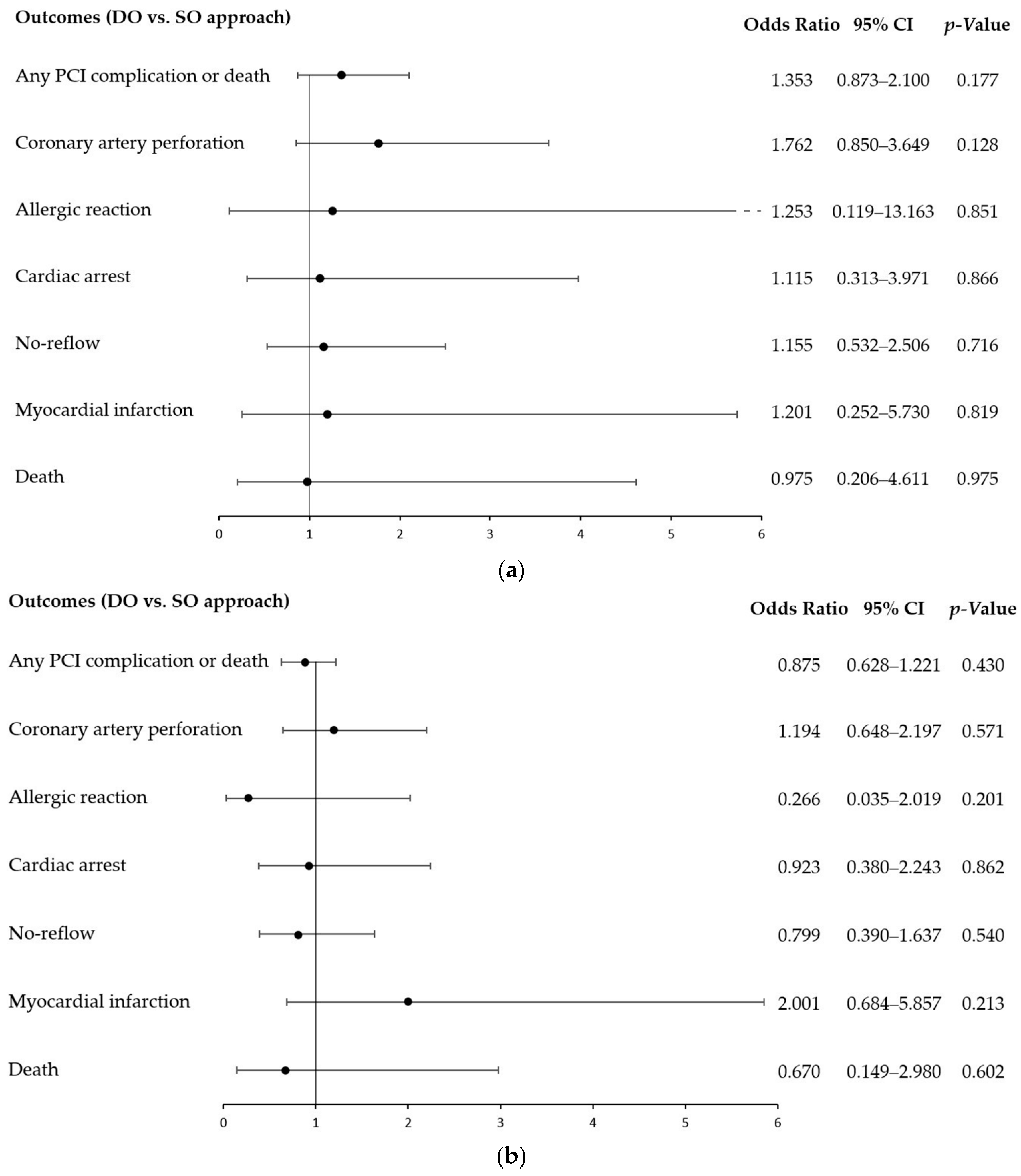
3.3. Procedure-Related Complications
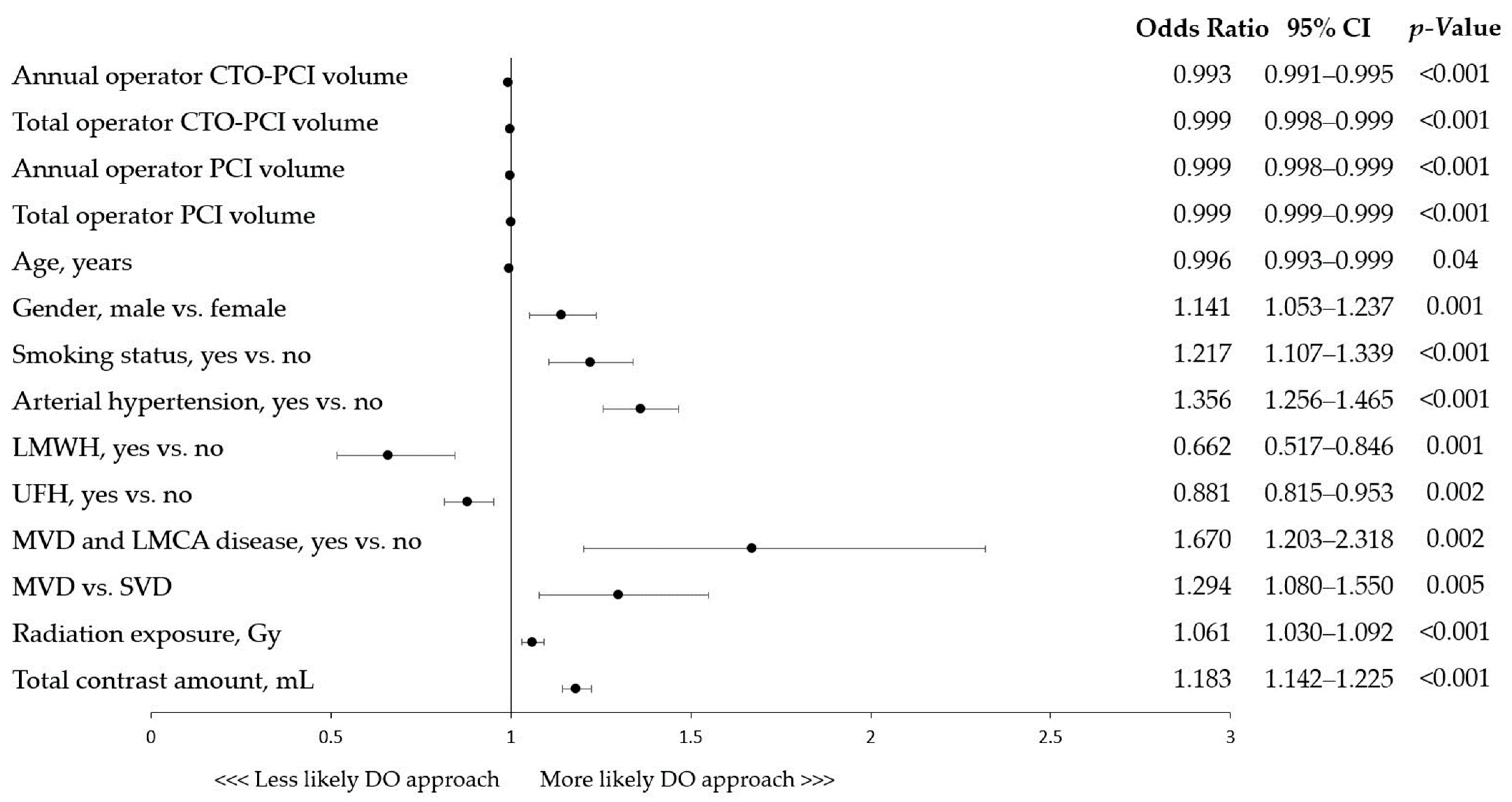
3.4. Factors Associated with Dual-Operator CTO-PCI
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waldo, S.W.; Secemsky, E.A.; O’Brien, C.; Kennedy, K.F.; Pomerantsev, E.; Sundt, T.M.; McNulty, E.J.; Scirica, B.M.; Yeh, R.W. Surgical Ineligibility and Mortality among Patients with Unprotected Left Main or Multivessel Coronary Artery Disease Undergoing Percutaneous Coronary Intervention. Circulation 2014, 130, 2295–2301. [Google Scholar] [CrossRef]
- Kirtane, A.J.; Doshi, D.; Leon, M.B.; Lasala, J.M.; Ohman, E.M.; O’Neill, W.W.; Shroff, A.; Cohen, M.G.; Palacios, I.F.; Beohar, N.; et al. Treatment of Higher-Risk Patients With an Indication for Revascularization: Evolution Within the Field of Contemporary Percutaneous Coronary Intervention. Circulation 2016, 134, 422–431. [Google Scholar] [CrossRef]
- Riley, R.F.; Henry, T.D.; Mahmud, E.; Kirtane, A.J.; Brilakis, E.S.; Goyal, A.; Grines, C.L.; Lombardi, W.L.; Maran, A.; Rab, T.; et al. SCAI Position Statement on Optimal Percutaneous Coronary Interventional Therapy for Complex Coronary Artery Disease. Catheter. Cardiovasc. Interv. 2020, 96, 346–362. [Google Scholar] [CrossRef]
- Kovach, C.P.; Hebbe, A.; Barón, A.E.; Strobel, A.; Plomondon, M.E.; Valle, J.A.; Waldo, S.W. Clinical Characteristics and Outcomes among Patients Undergoing High-Risk Percutaneous Coronary Interventions by Single or Multiple Operators: Insights from the Veterans Affairs Clinical Assessment, Reporting, and Tracking Program. J. Am. Heart Assoc. 2021, 10, e022131. [Google Scholar] [CrossRef]
- Galassi, A.R.; Tomasello, S.D.; Reifart, N.; Werner, G.S.; Sianos, G.; Bonnier, H.; Sievert, H.; Ehladad, S.; Bufe, A.; Shofer, J.; et al. In-Hospital Outcomes of Percutaneous Coronary Intervention in Patients with Chronic Total Occlusion: Insights from the ERCTO (European Registry of Chronic Total Occlusion) Registry. EuroIntervention 2011, 7, 472–479. [Google Scholar] [CrossRef]
- Januszek, R.A.; Bryniarski, L.; Siudak, Z.; Malinowski, K.P.; Surowiec, S.; Bryniarski, K.; Jędrychowska, M.; Wańha, W.; Bartuś, K.; Wojakowski, W.; et al. Predictors and Trends of Contrast Use and Radiation Exposure in a Large Cohort of Patients Treated with Percutaneous Coronary Interventions: Chronic Total Occlusion Analysis Based on a National Registry. Cardiol. J. 2021. [Google Scholar] [CrossRef]
- Tajti, P.; Alaswad, K.; Karmpaliotis, D.; Jaffer, F.A.; Yeh, R.W.; Patel, M.; Mahmud, E.; Choi, J.W.; Burke, M.N.; Doing, A.H.; et al. Procedural Outcomes of Percutaneous Coronary Interventions for Chronic Total Occlusions Via the Radial Approach: Insights From an International Chronic Total Occlusion Registry. JACC Cardiovasc. Interv. 2019, 12, 346–358. [Google Scholar] [CrossRef] [PubMed]
- Januszek, R.; Bryniarski, L.; Siudak, Z.; Malinowski, K.P.; Bryniarski, K.L.; Surdacki, A.; Dziewierz, A.; Mika, P.; Wańha, W.; Wojakowski, W.; et al. Five-Year Report from the Polish National Registry on Percutaneous Coronary Interventions with a Focus on Coronary Artery Perforations within Chronic Total Occlusions. Postep. Kardiol. Interwencyjnej 2021, 16, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Karmpaliotis, D.; Lembo, N.; Kalynych, A.; Carlson, H.; Lombardi, W.L.; Anderson, C.N.; Rinehart, S.; Kirkland, B.; Shemwell, K.C.; Kandzari, D.E. Development of a High-Volume, Multiple-Operator Program for Percutaneous Chronic Total Coronary Occlusion Revascularization: Procedural, Clinical, and Cost-Utilization Outcomes. Catheter. Cardiovasc. Interv. 2013, 82, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Othman, H.; Seth, M.; Zein, R.; Rosman, H.; Lalonde, T.; Yamasaki, H.; Alaswad, K.; Menees, D.; Mehta, R.H.; Gurm, H.; et al. Percutaneous Coronary Intervention for Chronic Total Occlusion—The Michigan Experience: Insights From the BMC2 Registry. JACC Cardiovasc. Interv. 2020, 13, 1357–1368. [Google Scholar] [CrossRef]
- Boukerche, F.; Laredj, N. Prognostic Impact of CTO Lesion in NSE-ACS Patients: Three-Year Outcome. Arch. Cardiovasc. Dis. Suppl. 2022, 14, 17. [Google Scholar] [CrossRef]
- Riley, R.F. Complex, Higher-Risk, and Indicated PCI (CHIP) Fellowship: Putting Training Into Practice. J. Am. Coll. Cardiol. 2020, 75, 980–984. [Google Scholar] [CrossRef]
- Doll, J.A.; Hira, R.S.; Kearney, K.E.; Kandzari, D.E.; Riley, R.F.; Marso, S.P.; Grantham, J.A.; Thompson, C.A.; McCabe, J.M.; Karmpaliotis, D.; et al. Management of Percutaneous Coronary Intervention Complications: Algorithms from the 2018 and 2019 Seattle Percutaneous Coronary Intervention Complications Conference. Circ. Cardiovasc. Interv. 2020, 13, e008962. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Moses, J.W.; Kirtane, A.J. How Many Operators Are Optimal for Higher-Risk Percutaneous Coronary Intervention Procedures? J. Am. Heart Assoc. 2021, 10, e023567. [Google Scholar] [CrossRef] [PubMed]
- Karacsonyi, J.; Alaswad, K.; Krestyaninov, O.; Karmpaliotis, D.; Kirtane, A.; Ali, Z.; McEntegart, M.; Masoumi, A.; Poomipanit, P.; Jaffer, F.A.; et al. Single vs. Multiple Operators for Chronic Total Occlusion Percutaneous Coronary Interventions: From the PROGRESS-CTO Registry. Catheter. Cardiovasc. Interv. 2023, 101, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Ybarra, L.F.; Rinfret, S.; Brilakis, E.S.; Karmpaliotis, D.; Azzalini, L.; Grantham, J.A.; Kandzari, D.E.; Mashayekhi, K.; Spratt, J.C.; Wijeysundera, H.C.; et al. Definitions and Clinical Trial Design Principles for Coronary Artery Chronic Total Occlusion Therapies: CTO-ARC Consensus Recommendations. Circulation 2021, 143, 479–500. [Google Scholar] [CrossRef]
- BoganaShanmugam, V.; Psaltis, P.J.; Wong, D.T.; Seneviratne, S.; Cameron, J.; Meredith, I.T.; Malaiapan, Y. Chronic Total Occlusion—Percutaneous Coronary Intervention (CTO-PCI) Experience in a Single, Multi-Operator Australian Centre: Need for Dedicated CTO-PCI Programs. Heart Lung Circ. 2016, 25, 676–682. [Google Scholar] [CrossRef]
- Zein, R.; Seth, M.; Othman, H.; Rosman, H.S.; Lalonde, T.; Alaswad, K.; Menees, D.; Daher, E.; Mehta, R.H.; Gurm, H.S. Association of Operator and Hospital Experience With Procedural Success Rates and Outcomes in Patients Undergoing Percutaneous Coronary Interventions for Chronic Total Occlusions: Insights From the Blue Cross Blue Shield of Michigan Cardiovascular Consortium. Circ. Cardiovasc. Interv. 2020, 13, e008863. [Google Scholar] [CrossRef]
- Brilakis, E.S.; Mashayekhi, K.; Tsuchikane, E.; Abi Rafeh, N.; Alaswad, K.; Araya, M.; Avran, A.; Azzalini, L.; Babunashvili, A.M.; Bayani, B.; et al. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention: A Global Expert Consensus Document. Circulation 2019, 140, 420–433. [Google Scholar] [CrossRef]
- Konstantinidis, N.V.; Werner, G.S.; Deftereos, S.; Di Mario, C.; Galassi, A.R.; Buettner, J.H.; Avran, A.; Reifart, N.; Goktekin, O.; Garbo, R.; et al. Temporal Trends in Chronic Total Occlusion Interventions in Europe: 17626 Procedures from the European Registry of Chronic Total Occlusion. Circ. Cardiovasc. Interv. 2018, 11, e006229. [Google Scholar] [CrossRef]
- Christopoulos, G.; Menon, R.V.; Karmpaliotis, D.; Alaswad, K.; Lombardi, W.; Grantham, A.; Patel, V.G.; Rangan, B.V.; Kotsia, A.P.; Lembo, N.; et al. The Efficacy and Safety of the “Hybrid” Approach to Coronary Chronic Total Occlusions: Insights from a Contemporary Multicenter US Registry and Comparison with Prior Studies. J. Invasive Cardiol. 2014, 26, 427–432. [Google Scholar] [PubMed]
- Christopoulos, G.; Wyman, R.M.; Alaswad, K.; Karmpaliotis, D.; Lombardi, W.; Grantham, J.A.; Yeh, R.; Jaffer, F.; Rangan, B.; Christakopoulos, G.; et al. Clinical Utility of the J-Cto Score in Coronary Chronic Total Occlusion Interventions: Results From a Multicenter Registry. J. Am. Coll. Cardiol. 2015, 65, A1807. [Google Scholar] [CrossRef]
- Zabojszcz, M.; Januszek, R.; Siudak, Z.; Janion-Sadowska, A.; Jedrychowska, M.; Pawlik, A.; Tokarek, T.; Staszczak, B.; Malinowski, K.P.; Bartus, S.; et al. Association between the Mortality Rate and Operator Volume in Patients Undergoing Emergency or Elective Percutaneous Coronary Interventions. Kardiol. Pol. 2020, 78, 138–146. [Google Scholar] [CrossRef]
- Fanaroff, A.C.; Zakroysky, P.; Dai, D.; Wojdyla, D.; Sherwood, M.W.; Roe, M.T.; Wang, T.Y.; Peterson, E.D.; Gurm, H.S.; Cohen, M.G.; et al. Outcomes of PCI in Relation to Procedural Characteristics and Operator Volumes in the United States. J. Am. Coll. Cardiol. 2017, 69, 2913–2924. [Google Scholar] [CrossRef] [PubMed]
- Brilakis, E.S.; Banerjee, S.; Karmpaliotis, D.; Lombardi, W.L.; Tsai, T.T.; Shunk, K.A.; Kennedy, K.F.; Spertus, J.A.; Holmes, D.R.; Grantham, J.A. Procedural Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention: A Report from the NCDR (National Cardiovascular Data Registry). JACC Cardiovasc. Interv. 2015, 8, 245–253. [Google Scholar] [CrossRef]
- Thompson, C.A.; Jayne, J.E.; Robb, J.F.; Friedman, B.J.; Kaplan, A.V.; Hettleman, B.D.; Niles, N.W.; Lombardi, W.L. Retrograde Techniques and the Impact of Operator Volume on Percutaneous Intervention for Coronary Chronic Total Occlusions. An Early U.S. Experience. JACC Cardiovasc. Interv. 2009, 2, 834–842. [Google Scholar] [CrossRef]
- Galassi, A.R.; Werner, G.S.; Boukhris, M.; Azzalini, L.; Mashayekhi, K.; Carlino, M.; Avran, A.; Konstantinidis, N.V.; Grancini, L.; Bryniarski, L.; et al. Percutaneous Recanalisation of Chronic Total Occlusions: 2019 Consensus Document from the EuroCTO Club. EuroIntervention 2019, 15, 198–208. [Google Scholar] [CrossRef]
- Bryniarski, L.; Opolski, M.P.; Wójcik, J.; Lesiak, M.; Pawłowski, T.; Drozd, J.; Wojakowski, W.; Surowiec, S.; Dąbrowski, M.; Witkowski, A.; et al. Chronic Total Occlusion Percutaneous Coronary Intervention in Everyday Clinical Practice—An Expert Opinion of the Association of Cardiovascular Interventions of the Polish Cardiac Society. Postep. Kardiol. Interwencyjnej 2021, 17, 6–20. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total (n = 27,788) | 2 Operators (n = 3604) | 1 Operator (n = 24,184) | p-Value |
|---|---|---|---|---|
| Age, years | 66 (60; 73) | 66 (60; 73) | 66 (60; 73) | 0.02 |
| 66.4 ± 9.7 | 66.1 ± 9.8 | 66.5 ± 9.7 | ||
| Gender, males | 19,777 (72.9) | 2698 (75.1) | 17,079 (72.5) | 0.001 |
| Diabetes mellitus | 6318 (22.7) | 834 (23.1) | 5484 (22.7) | 0.53 |
| Prior cerebral stroke | 769 (2.8) | 107 (3.0) | 662 (2.7) | 0.43 |
| Prior myocardial infarction | 11,262 (40.5) | 1419 (39.4) | 9843 (40.7) | 0.13 |
| Prior PCI | 13,562 (59.5) | 1738 (48.2) | 11,824 (48.9) | 0.45 |
| Prior CABG | 1823 (6.6) | 247 (6.9) | 1576 (6.5) | 0.45 |
| Smoking | 3995 (14.4) | 598 (16.6) | 3397 (14.1) | <0.0001 |
| Psoriasis | 91 (0.3) | 13 (0.4) | 78 (0.3) | 0.71 |
| Arterial hypertension | 18,259 (65.7) | 2575 (71.5) | 15,684 (64.9) | <0.0001 |
| Kidney disease | 1295 (4.7) | 185 (5.1) | 1110 (4.6) | 0.15 |
| COPD | 586 (2.1) | 77 (2.1) | 509 (2.1) | 0.90 |
| Killip class | 0.39 | |||
| I | 10,258 (96.5) | 1493 (95.9) | 8765 (96.6) | |
| II | 326 (3.1) | 58 (3.7) | 268 (3.0) | |
| III | 30 (0.3) | 4 (0.3) | 26 (0.3) | |
| IV | 20 (0.2) | 2 (0.1) | 18 (0.2) | |
| Killip IV class | 20 (0.2) | 2 (0.1) | 18 (0.2) | 0.56 |
| Variables | 2 Operators (n = 3190) | 1 Operator (n = 12,760) | p-Value |
|---|---|---|---|
| Age, years | 65.99 ± 9.75 | 66.00 ± 9.76 | 0.96 |
| Gender, males | 2406 (75.4) | 9608 (75.3) | 0.90 |
| Diabetes mellitus | 790 (24.8) | 3120 (24.5) | 0.73 |
| Prior cerebral stroke | 96 (3.0) | 396 (3.1) | 0.83 |
| Prior myocardial infarction | 1343 (42.1) | 5449 (42.7) | 0.55 |
| Prior PCI | 1628 (51.0) | 6605 (51.8) | 0.47 |
| Prior CABG | 234 (7.3) | 922 (7.2) | 0.86 |
| Smoking | 562 (17.6) | 2172 (17.0) | 0.44 |
| Psoriasis | |||
| Arterial hypertension | 2304 (72.2) | 9155 (71.7) | 0.61 |
| Kidney disease | 173 (5.4) | 681 (5.3) | 0.88 |
| COPD | 66 (2.1) | 269 (2.1) | 0.95 |
| Variables | Total (n = 27,788) | 2 Operators (n = 3604) | 1 Operator (n = 24,184) | p-Value |
|---|---|---|---|---|
| Fractional flow reserve | 264 (1.0) | 37 (1.0) | 227 (0.9) | 0.61 |
| IVUS | 622 (2.2) | 92 (2.6) | 530 (2.2) | 0.17 |
| OCT | 81 (0.3) | 16 (0.4) | 65 (0.3) | 0.07 |
| Rotablation | 293 (1.1) | 29 (0.8) | 264 (1.1) | 0.12 |
| Mean TIMI grade after PCI | 2.16 ± 1.31 | 2.13 ± 1.33 | 2.17 ± 1.31 | 0.18 |
| TIMI grade after PCI | ||||
| 0 | 4752 (25.5) | 685 (26.6) | 4067 (25.3) | 0.52 |
| 1 | 418 (2.2) | 55 (2.1) | 363 (2.3) | |
| 2 | 473 (2.5) | 68 (2.6) | 405 (2.5) | |
| 3 | 12,978 (69.7) | 1763 (68.6) | 11,215 (69.9) | |
| TIMI grade 2/3 after PCI | 13,451 (72.2) | 1831 (71.2) | 11,620 (72.4) | 0.19 |
| Contrast volume, mL | 170 (120; 230) | 200 (150; 250) | 170 (120; 230) | <0.0001 |
| Radiation dose, Gy | 0.92 (0.50; 1.69) | 1.05 (0.62; 1.85) | 0.90 (0.48; 1.66) | <0.0001 |
| Vascular access | ||||
| Femoral | 7050 (25.4) | 1127 (31.3) | 5923 (24.5) | |
| Radial | 20,372 (73.4) | 2451 (68.1) | 17,921 (74.2) | <0.0001 |
| Other | 340 (1.2) | 24 (0.7) | 316 (1.3) | |
| Access site crossover | 536 (3.1) | 86 (3.9) | 450 (3.0) | 0.02 |
| PCI within bifurcation | 1939 (7.0) | 242 (6.7) | 1697 (7.0) | 0.51 |
| Type of stent implanted | ||||
| BMS | 323 (1.2) | 48 (1.3) | 275 (1.1) | 0.31 |
| BVS | 110 (0.4) | 24 (0.7) | 86 (0.4) | 0.006 |
| DES | 18,163 (65.4) | 2316 (64.3) | 15,847 (65.5) | 0.14 |
| Drug-eluting balloon | 677 (2.7) | 105 (3.2) | 572 (2.7) | 0.08 |
| Implanted stent | 18,549 (66.8) | 2382 (66.1) | 16,167 (66.9) | 0.37 |
| Number of implanted stents | ||||
| No stent used | 9239 (33.3) | 1222 (33.9) | 8017 (33.2) | |
| 1 | 14,640 (52.7) | 1873 (52.0 | 12,767 (52.8) | 0.73 |
| 2 | 3133 (11.3) | 413 (11.5) | 2720 (11.3) | |
| >2 | 776 (2.8) | 96 (2.7) | 680 (2.8) | |
| ASA | 7055 (25.4) | 927 (25.7) | 6128 (25.3) | 0.62 |
| UFH | 20,563 (74.0) | 2589 (71.8) | 17,974 (74.3) | 0.002 |
| LMWH | 784 (2.8) | 71 (2.0) | 713 (3.0) | <0.001 |
| Bivalirudin | 25 (0.1) | 5 (0.1) | 20 (0.1) | 0.30 |
| Thrombolysis during PCI | 19 (0.1) | 3 (0.1) | 16 (0.1) | 0.71 |
| Site volume total | 6548 (4748.00; 8602.00) | 6054 (4232.00; 8745.00) | 6747 (4843.00; 8602.00) | 0.04 |
| Site volume annual | 818.50 (593.50; 1075.25) | 756.75 (529.00; 1093.13) | 843.38 (605.38; 1075.25) | 0.04 |
| Operator volume total | 1617 (1096.00; 2261.00) | 1368 (857.25; 1970.25) | 1676 (1104.00; 2261.00) | <0.0001 |
| Annual operator volume | 202.13 (137.00; 282.63) | 171.00 (107.16; 246.28) | 209.50 (138.00; 282.63) | <0.0001 |
| Operator CTO volume total | 92.00 (39.00; 197.00) | 80.00 (30.00; 179.00) | 93.00 (40.00; 211.00) | <0.0001 |
| Operator CTO volume annual | 11.50 (4.88; 24.63) | 10.00 (3.75; 22.38) | 11.63 (5.00; 26.38) | <0.0001 |
| Variables | 2 Operators (n = 3190) | 1 Operator (n = 12,760) | p-Value |
|---|---|---|---|
| Fractional flow reserve | 32 (1.0) | 120 (0.9) | 0.82 |
| IVUS | 87 (2.7) | 347 (2.7) | 1.0 |
| OCT | 15 (0.5) | 50 (0.4) | 0.64 |
| Contrast volume, mL | 200 (150, 250) | 180 (130, 250) | <0.001 |
| Radiation dose, Gy | 1.05 (0.62, 1.84) | 0.98 (0.53, 1.76) | <0.001 |
| Vascular access | 0.45 | ||
| Femoral | 1066 (33.4) | 4122 (32.3) | |
| Radial | 2105 (66.0) | 8568 (67.1) | |
| Other | 19 (0.6) | 70 (0.5) | |
| PCI within bifurcation | 212 (27.6) | 857 (6.7) | 0.92 |
| Implanted stent | 2134 (66.9) | 8522 (66.8) | 0.92 |
| ASA | 879 (27.6) | 3516 (27.6) | 1.0 |
| UFH | 2304 (72.2) | 9441 (74.0) | 0.046 |
| LMWH | 67 (2.1) | 252 (2.0) | 0.70 |
| Site volume annual | 809.00 (534.75, 1093.12) | 818.50 (608.00, 1075.25) | 0.75 |
| Operator CTO volume annual | 10.00 (4.25, 24.25) | 9.88 (4.25, 24.12) | 0.75 |
| Variables | Total (n = 27,788) | 2 Operators (n = 3604) | 1 Operator (n = 24,184) | p-Value |
|---|---|---|---|---|
| All complications | 358 (1.3) | 45 (1.3) | 313 (1.3) | 0.82 |
| Death | 22 (0.1) | 2 (0.1) | 20 (0.1) | 0.60 |
| Myocardial infarction | 26 (0.1) | 5 (0.1) | 21 (0.1) | 0.34 |
| No-reflow phenomenon | 83 (0.3) | 9 (0.3) | 74 (0.3) | 0.56 |
| Cardiac arrest | 45 (0.2) | 6 (0.2) | 39 (0.2) | 0.94 |
| Allergic reaction | 32 (0.1) | 2 (0.1) | 30 (0.1) | 0.26 |
| Coronary artery perforation | 125 (0.5) | 19 (0.5) | 106 (0.4) | 0.46 |
| Puncture-site bleeding | 45 (0.2) | 2 (0.1) | 43 (0.2) | 0.09 |
| Variables | 2 Operators (n = 3190) | 1 Operator (n = 12,760) | p-Value |
|---|---|---|---|
| All complications | 53 (1.7) | 225 (1.8) | 0.75 |
| Death | 2 (0.1) | 12 (0.1) | 0.84 |
| Myocardial infarction | 5 (0.2) | 10 (0.1) | 0.33 |
| No-reflow phenomenon | 9 (0.3) | 45 (0.4) | 0.66 |
| Cardiac arrest | 9 (0.3) | 32 (0.3) | 0.91 |
| Allergic reaction | 1 (0.0) | 15 (0.1) | 0.29 |
| Coronary artery perforation | 19 (0.6) | 67 (0.5) | 0.73 |
| Puncture-site bleeding | 2 (0.1) | 37 (0.3) | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Januszek, R.; De Luca, G.; Siłka, W.; Bryniarski, L.; Malinowski, K.P.; Surdacki, A.; Wańha, W.; Bartuś, S.; Piotrowska, A.; Bartuś, K.; et al. Single versus Dual-Operator Approaches for Percutaneous Coronary Interventions within Chronic Total Occlusion—An Analysis of 27,788 Patients. J. Clin. Med. 2023, 12, 4684. https://doi.org/10.3390/jcm12144684
Januszek R, De Luca G, Siłka W, Bryniarski L, Malinowski KP, Surdacki A, Wańha W, Bartuś S, Piotrowska A, Bartuś K, et al. Single versus Dual-Operator Approaches for Percutaneous Coronary Interventions within Chronic Total Occlusion—An Analysis of 27,788 Patients. Journal of Clinical Medicine. 2023; 12(14):4684. https://doi.org/10.3390/jcm12144684
Chicago/Turabian StyleJanuszek, Rafał, Giuseppe De Luca, Wojciech Siłka, Leszek Bryniarski, Krzysztof Piotr Malinowski, Andrzej Surdacki, Wojciech Wańha, Stanisław Bartuś, Aleksandra Piotrowska, Krzysztof Bartuś, and et al. 2023. "Single versus Dual-Operator Approaches for Percutaneous Coronary Interventions within Chronic Total Occlusion—An Analysis of 27,788 Patients" Journal of Clinical Medicine 12, no. 14: 4684. https://doi.org/10.3390/jcm12144684
APA StyleJanuszek, R., De Luca, G., Siłka, W., Bryniarski, L., Malinowski, K. P., Surdacki, A., Wańha, W., Bartuś, S., Piotrowska, A., Bartuś, K., Pytlak, K., & Siudak, Z. (2023). Single versus Dual-Operator Approaches for Percutaneous Coronary Interventions within Chronic Total Occlusion—An Analysis of 27,788 Patients. Journal of Clinical Medicine, 12(14), 4684. https://doi.org/10.3390/jcm12144684