

Depressive Symptoms and Their Impact on Quality of Life in Parkinson’s Disease: An Exploratory Network Analysis Approach

 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Extracted Variables
2.3. Statistical Analyses
3. Results
3.1. Descriptive Analyses
3.2. Network Analyses
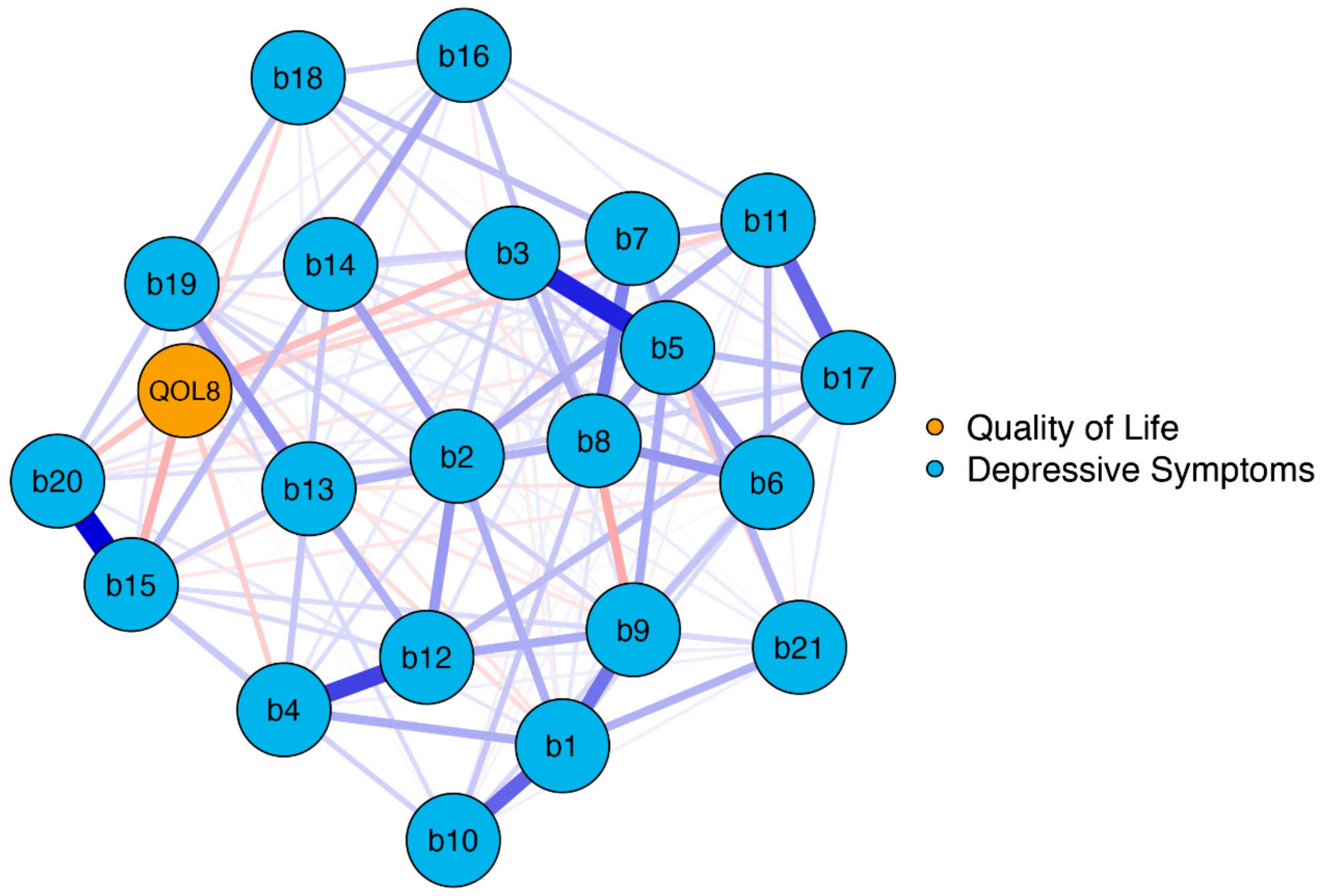
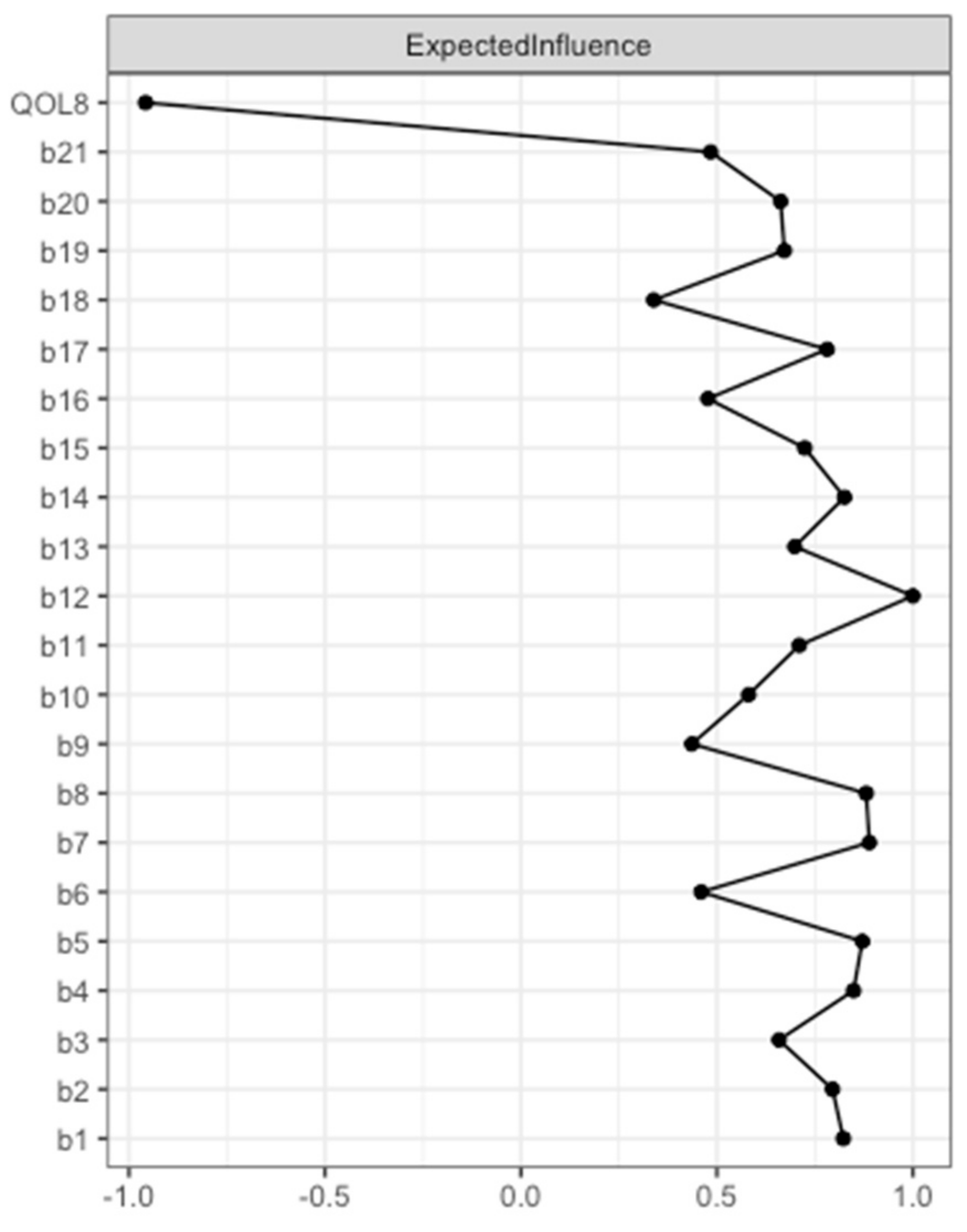
3.2.1. Network Model 1: Association between BDI-II Items and Overall QoL (EUROHIS-QOL 8-Item Index)
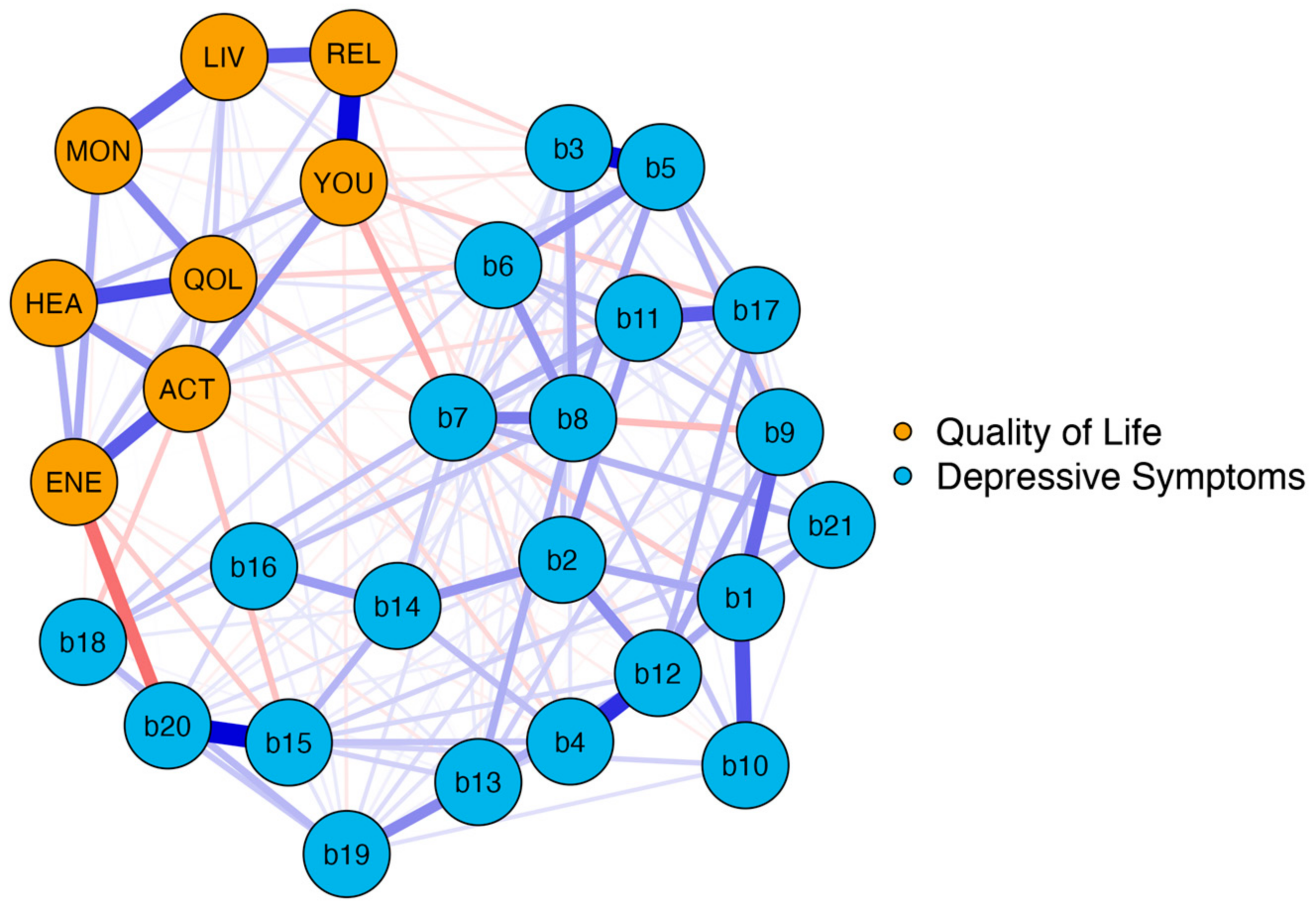
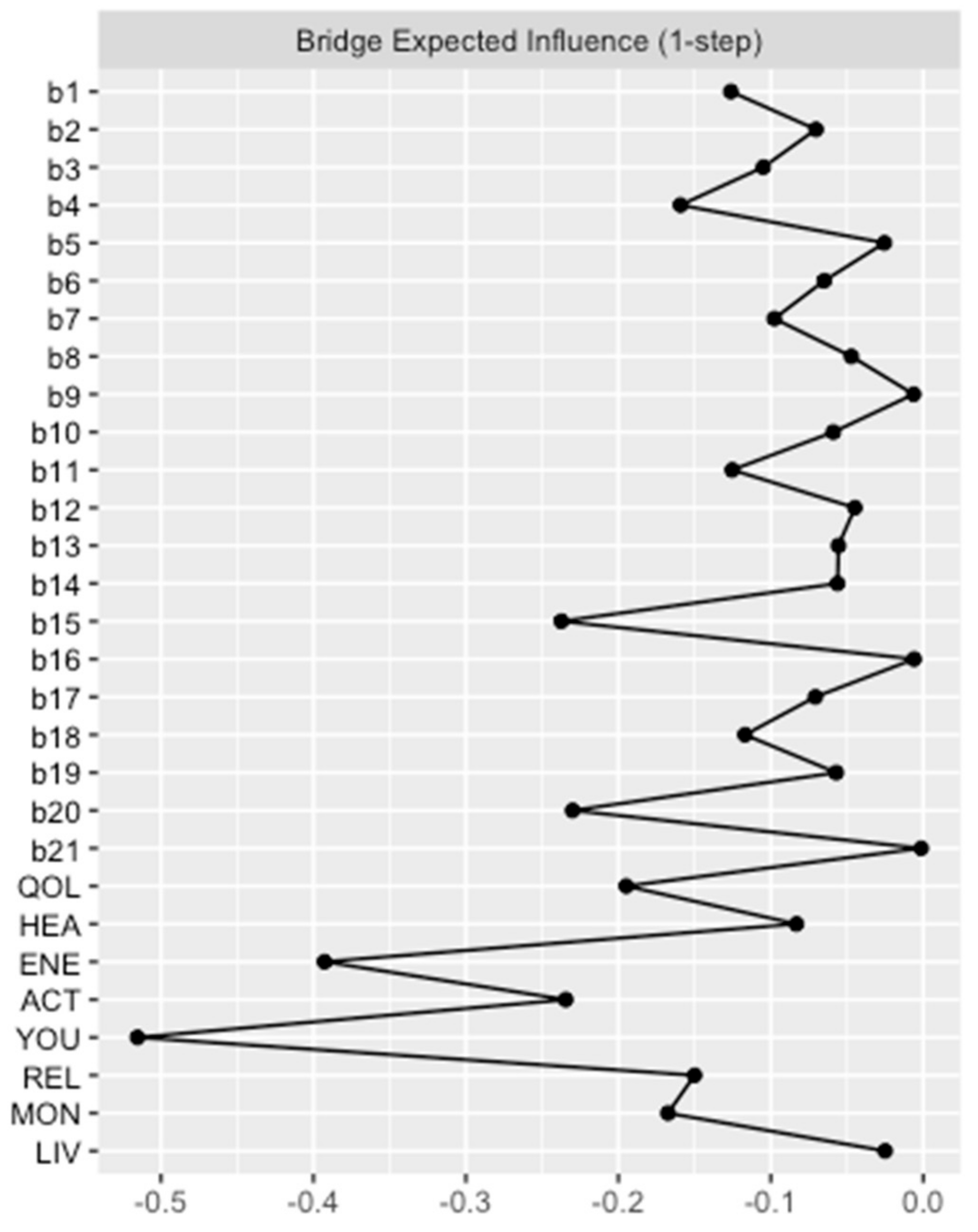
3.2.2. Network Model 2: Association between BDI-II Items and the Eight EUROHIS-QOL Items
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Titova, N.; Qamar, M.A.; Chaudhuri, K.R. The Nonmotor Features of Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 132, 33–54. [Google Scholar] [CrossRef] [PubMed]
- Menon, B.; Nayar, R.; Kumar, S.; Cherkil, S.; Venkatachalam, A.; Surendran, K.; Deepak, K.S. Parkinson’s Disease, Depression, and Quality-of-Life. Indian J. Psychol. Med. 2015, 37, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martin, P.; Rodriguez-Blazquez, C.; Kurtis, M.M.; Chaudhuri, K.R. The impact of non-motor symptoms on health-related quality of life of patients with Parkinson’s disease. Mov. Disord. 2011, 26, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Bock, M.A.; Brown, E.G.; Zhang, L.; Tanner, C. Association of Motor and Nonmotor Symptoms With Health-Related Quality of Life in a Large Online Cohort of People With Parkinson Disease. Neurology 2022, 98, e2194–e2203. [Google Scholar] [CrossRef] [PubMed]
- Santos-García, D.; de la Fuente-Fernández, R. Impact of non-motor symptoms on health-related and perceived quality of life in Parkinson’s disease. J. Neurol. Sci. 2013, 332, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Meyers, A.R.; Gage, H.; Hendricks, A. Health-related quality of life in neurology. Arch. Neurol. 2000, 57, 1224–1227. [Google Scholar] [CrossRef]
- Schrag, A. Quality of life and depression in Parkinson’s disease. J. Neurol. Sci. 2006, 248, 151–157. [Google Scholar] [CrossRef]
- Tandberg, E.; Larsen, J.P.; Aarsland, D.; Cummings, J.L. The Occurrence of Depression in Parkinson’s Disease: A Community-Based Study. Arch. Neurol. 1996, 53, 175–179. [Google Scholar] [CrossRef]
- Reijnders, J.S.; Ehrt, U.; Weber, W.E.; Aarsland, D.; Leentjens, A.F. A systematic review of prevalence studies of depression in Parkinson’s disease. Mov. Disord. 2008, 23, 183–189; quiz 313. [Google Scholar] [CrossRef]
- Schönenberg, A.; Zipprich, H.M.; Teschner, U.; Grosskreutz, J.; Witte, O.W.; Prell, T. Impact of subthreshold depression on health-related quality of life in patients with Parkinson’s disease based on cognitive status. Health Qual. Life Outcomes 2021, 19, 107. [Google Scholar] [CrossRef]
- Bahadoran, P.; Varela, R.; De Angelis, A.; Paviour, D.; Agrawal, N. Screening for depression in movement disorders clinic. Neurol. Sci. 2021, 42, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, Z.; Mrklas, K.J.; Roberts, D.J.; Jette, N.; Pringsheim, T.; Holroyd-Leduc, J. Detecting depression in Parkinson disease: A systematic review and meta-analysis. Neurology 2016, 87, 426–437. [Google Scholar] [CrossRef]
- Martinez-Martin, P.; Jeukens-Visser, M.; Lyons, K.E.; Rodriguez-Blazquez, C.; Selai, C.; Siderowf, A.; Welsh, M.; Poewe, W.; Rascol, O.; Sampaio, C.; et al. Health-related quality-of-life scales in Parkinson’s disease: Critique and recommendations. Mov. Disord. 2011, 26, 2371–2380. [Google Scholar] [CrossRef] [PubMed]
- Fried, E.I. Studying Mental Health Problems as Systems, Not Syndromes. Curr. Dir. Psychol. Sci. 2022, 31, 500–508. [Google Scholar] [CrossRef]
- Borsboom, D.; Cramer, A.O. Network analysis: An integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Santos-García, D.; Mir, P.; Cubo, E.; Vela, L.; Rodríguez-Oroz, M.C.; Martí, M.J.; Arbelo, J.M.; Infante, J.; Kulisevsky, J.; Martínez-Martín, P.; et al. COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015), a global--clinical evaluations, serum biomarkers, genetic studies and neuroimaging--prospective, multicenter, non-interventional, long-term study on Parkinson’s disease progression. BMC Neurol. 2016, 16, 26. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Nosikov, A.; Gudex, C. Development of a common instrument for quality of life. EUROHIS Dev. Common Instrum. Health Surv. 2003, 57, 145. [Google Scholar]
- WHOQOL Group. The World Health Organization Quality of Life Assessment (WHOQOL): Development and general psychometric properties. Soc. Sci. Med. 1998, 46, 1569–1585. [Google Scholar] [CrossRef]
- Schmidt, S.; Mühlan, H.; Power, M. The EUROHIS-QOL 8-item index: Psychometric results of a cross-cultural field study. Eur. J. Public. Health 2006, 16, 420–428. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef]
- Fahn, S.; Elton, R. Recent developments in Parkinson’s disease. Macmillan Health Care Inf. 1987, 2, 293–304. [Google Scholar]
- Chaudhuri, K.R.; Martinez-Martin, P.; Brown, R.G.; Sethi, K.; Stocchi, F.; Odin, P.; Ondo, W.; Abe, K.; Macphee, G.; Macmahon, D.; et al. The metric properties of a novel non-motor symptoms scale for Parkinson’s disease: Results from an international pilot study. Mov. Disord. 2007, 22, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. ‘Mini-mental state’. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Hevey, D. Network analysis: A brief overview and tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef] [PubMed]
- Foygel, R.; Drton, M. Extended Bayesian information criteria for Gaussian graphical models. arXiv 2010, arXiv:1011.6640. [Google Scholar]
- Chen, J.; Chen, Z. Extended Bayesian information critera for model selection with large model spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics 2008, 9, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Olsson, U. Maximum likelihood estimation of the polychoric correlation coefficient. Psychometrika 1979, 44, 443–460. [Google Scholar] [CrossRef]
- Fruchterman, T.M.; Reingold, E.M. Graph drawing by force-directed placement. Softw. Pract. Exp. 1991, 21, 1129–1164. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Robinaugh, D.J.; Millner, A.J.; McNally, R.J. Identifying highly influential nodes in the complicated grief network. J. Abnorm. Psychol. 2016, 125, 747–757. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.J.; Ma, R.; McNally, R.J. Bridge Centrality: A Network Approach to Understanding Comorbidity. Multivar. Behav. Res. 2021, 56, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Haslbeck, J.M.B.; Waldorp, L.J. How well do network models predict observations? On the importance of predictability in network models. Behav. Res. Methods 2018, 50, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Reiff, J.; Schmidt, N.; Riebe, B.; Breternitz, R.; Aldenhoff, J.; Deuschl, G.; Witt, K. Subthreshold depression in Parkinson’s disease. Mov. Disord. 2011, 26, 1741–1744. [Google Scholar] [CrossRef]
- Krupp, L.B.; Pollina, D.A. Mechanisms and management of fatigue in progressive neurological disorders. Curr. Opin. Neurol. 1996, 9, 456–460. [Google Scholar] [CrossRef]
- Barone, P.; Antonini, A.; Colosimo, C.; Marconi, R.; Morgante, L.; Avarello, T.; Bottacchi, E.; Cannas, A.; Ceravolo, G.; Ceravolo, R.; et al. The PRIAMO study: A multicenter assessment of nonmotor symptoms and their impact on quality of life in Parkinson’s disease. Mov. Disord. 2009, 24, 1641–1649. [Google Scholar] [CrossRef]
- Pont-Sunyer, C.; Hotter, A.; Gaig, C.; Seppi, K.; Compta, Y.; Katzenschlager, R.; Mas, N.; Hofeneder, D.; Brücke, T.; Bayés, A.; et al. The onset of nonmotor symptoms in Parkinson’s disease (the ONSET PD study). Mov. Disord. 2015, 30, 229–237. [Google Scholar] [CrossRef]
- Friedman, J.H.; Friedman, H. Fatigue in Parkinson’s disease: A nine-year follow-up. Mov. Disord. 2001, 16, 1120–1122. [Google Scholar] [CrossRef]
- Alves, G.; Wentzel-Larsen, T.; Larsen, J.P. Is fatigue an independent and persistent symptom in patients with Parkinson disease? Neurology 2004, 63, 1908–1911. [Google Scholar] [CrossRef]
- Herlofson, K.; Kluger, B.M. Fatigue in Parkinson’s disease. J. Neurol. Sci. 2017, 374, 38–41. [Google Scholar] [CrossRef]
- Stocchi, F.; Abbruzzese, G.; Ceravolo, R.; Cortelli, P.; D’Amelio, M.; De Pandis, M.F.; Fabbrini, G.; Pacchetti, C.; Pezzoli, G.; Tessitore, A.; et al. Prevalence of fatigue in Parkinson disease and its clinical correlates. Neurology 2014, 83, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Evans, M.; Brown, M.; Porter, N. What is fatigue? Pathological and nonpathological fatigue. PM&R 2010, 2, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Franssen, M.; Winward, C.; Collett, J.; Wade, D.; Dawes, H. Interventions for fatigue in Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2014, 29, 1675–1678. [Google Scholar] [CrossRef]
- Elbers, R.G.; Berendse, H.W.; Kwakkel, G. Treatment of Fatigue in Parkinson Disease. JAMA 2016, 315, 2340–2341. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.; Barreto, M.; Oliveira, S. The Link Between Major Life Events and Quality of Life: The Role of Compassionate Abilities. Community Ment. Health J. 2021, 57, 219–227. [Google Scholar] [CrossRef]
- Dohrenwend, B.P. Inventorying stressful life events as risk factors for psychopathology: Toward resolution of the problem of intracategory variability. Psychol. Bull. 2006, 132, 477–495. [Google Scholar] [CrossRef]
- Mundt, C.; Reck, C.; Backenstrass, M.; Kronmüller, K.; Fiedler, P. Reconfirming the role of life events for the timing of depressive episodes. A two-year prospective follow-up study. J. Affect. Disord. 2000, 59, 23–30. [Google Scholar] [CrossRef]
- Kessing, L.V.; Agerbo, E.; Mortensen, P.B. Does the impact of major stressful life events on the risk of developing depression change throughout life? Psychol. Med. 2003, 33, 1177–1184. [Google Scholar] [CrossRef]
- Lickel, B.; Kushlev, K.; Savalei, V.; Matta, S.; Schmader, T. Shame and the motivation to change the self. Emotion 2014, 14, 1049–1061. [Google Scholar] [CrossRef]
- Rubenstein, L.M.; Freed, R.D.; Shapero, B.G.; Fauber, R.L.; Alloy, L.B. Cognitive Attributions in Depression: Bridging the Gap between Research and Clinical Practice. J. Psychother. Integr. 2016, 26, 103–115. [Google Scholar] [CrossRef]
- Ferreira, C.; Mendes, A.L.; Marta-Simões, J. The Role of Maladaptive Psychological Strategies in the Association between Shame and Psychological Quality of Life. Eur. Psychiatry 2017, 41, S86. [Google Scholar] [CrossRef]
- Zhang, H.; Carr, E.R.; Garcia-Williams, A.G.; Siegelman, A.E.; Berke, D.; Niles-Carnes, L.V.; Patterson, B.; Watson-Singleton, N.N.; Kaslow, N.J. Shame and Depressive Symptoms: Self-compassion and Contingent Self-worth as Mediators? J. Clin. Psychol. Med. Settings 2018, 25, 408–419. [Google Scholar] [CrossRef] [PubMed]
- Berrios, G.E.; Olivares, J.M. The anhedonias: A conceptual history. Hist. Psychiatry 1995, 6, 453–470. [Google Scholar] [CrossRef]
- Kaji, Y.; Hirata, K. Apathy and anhedonia in Parkinson’s disease. ISRN Neurol. 2011, 2011, 219427. [Google Scholar] [CrossRef]
- Billones, R.R.; Kumar, S.; Saligan, L.N. Disentangling fatigue from anhedonia: A scoping review. Transl. Psychiatry 2020, 10, 273. [Google Scholar] [CrossRef] [PubMed]
- Heimrich, K.G.; Schönenberg, A.; Mühlhammer, H.M.; Mendorf, S.; Santos-García, D.; Prell, T. Longitudinal analysis of the Non-Motor Symptoms Scale in Parkinson’s Disease (NMSS): An exploratory network analysis approach. Front. Neurol. 2023, 14, 972210. [Google Scholar] [CrossRef] [PubMed]
- Heimrich, K.G.; Schönenberg, A.; Santos-García, D.; Mir, P.; Group, C.S.; Prell, T. The Impact of Nonmotor Symptoms on Health-Related Quality of Life in Parkinson’s Disease: A Network Analysis Approach. J. Clin. Med. 2023, 12, 2573. [Google Scholar] [CrossRef]
- Stohlman, S.L.; Barrett, M.J.; Sperling, S.A. Factor structure of the BDI-II in Parkinson’s disease. Neuropsychology 2021, 35, 540–546. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Age | 64 (57–70) |
| Disease duration | 5 (2–8) |
| HY off | 2 (2–2) |
| UPDRS III off | 21 (14–30) |
| UPDRS IV off | 1 (0–3) |
| NMSS, total score | 35 (19–61) |
| MMSE, total score | 30 (29–30) |
| BDI-II, total score | 7 (3–13) |
| 1. Sadness | 0 (0–1) |
| 2. Pessimism | 0 (0–1) |
| 3. Past failure | 0 (0–0) |
| 4. Loss of pleasure | 0 (0–1) |
| 5. Guilty feelings | 0 (0–0) |
| 6. Punishment feelings | 0 (0–0) |
| 7. Self-dislike | 0 (0–0) |
| 8. Self-criticalness | 0 (0–1) |
| 9. Suicidal thoughts or wishes | 0 (0–0) |
| 10. Crying | 0 (0–1) |
| 11. Agitation | 0 (0–1) |
| 12. Loss of interest | 0 (0–1) |
| 13. Indecisiveness | 0 (0–1) |
| 14. Worthlessness | 0 (0–1) |
| 15. Loss of energy | 1 (0–1) |
| 16. Changes in sleeping pattern | 1 (0–2) |
| 17. Irritability | 0 (0–1) |
| 18. Changes in appetite | 0 (0–1) |
| 19. Concentration difficulty | 1 (0–1) |
| 20. Tiredness or fatigue | 1 (0–1) |
| 21. Loss of interest in sex | 0 (0–1) |
| EUROHIS-QOL 8-item index | 31 (28–33) |
| 1. QOL, quality | 4 (3–4) |
| 2. HEA, health | 3 (3–4) |
| 3. ENE, energy | 4 (3–4) |
| 4. ACT, activities | 4 (3–4) |
| 5. YOU, yourself | 4 (3–4) |
| 6. REL, relationships | 4 (4–4) |
| 7. MON, money | 4 (3–4) |
| 8. LIV, living | 4 (4–5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heimrich, K.G.; Mendorf, S.; Schönenberg, A.; Santos-García, D.; Mir, P.; COPPADIS Study Group; Prell, T. Depressive Symptoms and Their Impact on Quality of Life in Parkinson’s Disease: An Exploratory Network Analysis Approach. J. Clin. Med. 2023, 12, 4616. https://doi.org/10.3390/jcm12144616
Heimrich KG, Mendorf S, Schönenberg A, Santos-García D, Mir P, COPPADIS Study Group, Prell T. Depressive Symptoms and Their Impact on Quality of Life in Parkinson’s Disease: An Exploratory Network Analysis Approach. Journal of Clinical Medicine. 2023; 12(14):4616. https://doi.org/10.3390/jcm12144616
Chicago/Turabian StyleHeimrich, Konstantin G., Sarah Mendorf, Aline Schönenberg, Diego Santos-García, Pablo Mir, COPPADIS Study Group, and Tino Prell. 2023. "Depressive Symptoms and Their Impact on Quality of Life in Parkinson’s Disease: An Exploratory Network Analysis Approach" Journal of Clinical Medicine 12, no. 14: 4616. https://doi.org/10.3390/jcm12144616
APA StyleHeimrich, K. G., Mendorf, S., Schönenberg, A., Santos-García, D., Mir, P., COPPADIS Study Group, & Prell, T. (2023). Depressive Symptoms and Their Impact on Quality of Life in Parkinson’s Disease: An Exploratory Network Analysis Approach. Journal of Clinical Medicine, 12(14), 4616. https://doi.org/10.3390/jcm12144616