
Prediction of Posterior-to-Anterior Corneal Curvature Radii Ratio in Myopic Patients after LASIK, SMILE, and PRK Using Multivariate Regression Analysis

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Data Collection
2.3. Statistics
3. Results
3.1. Population Characteristics
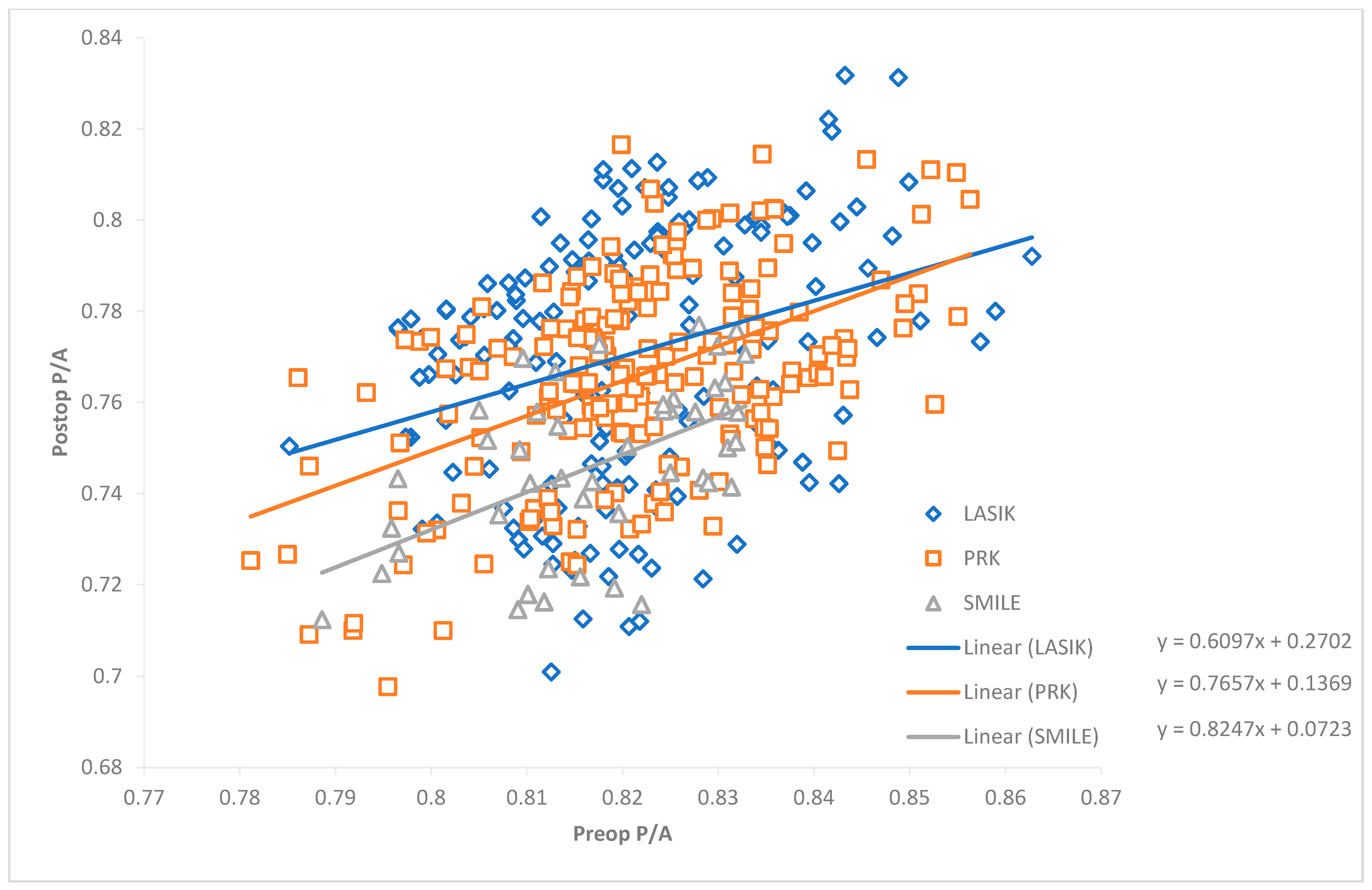
3.2. Linear Regression Analysis
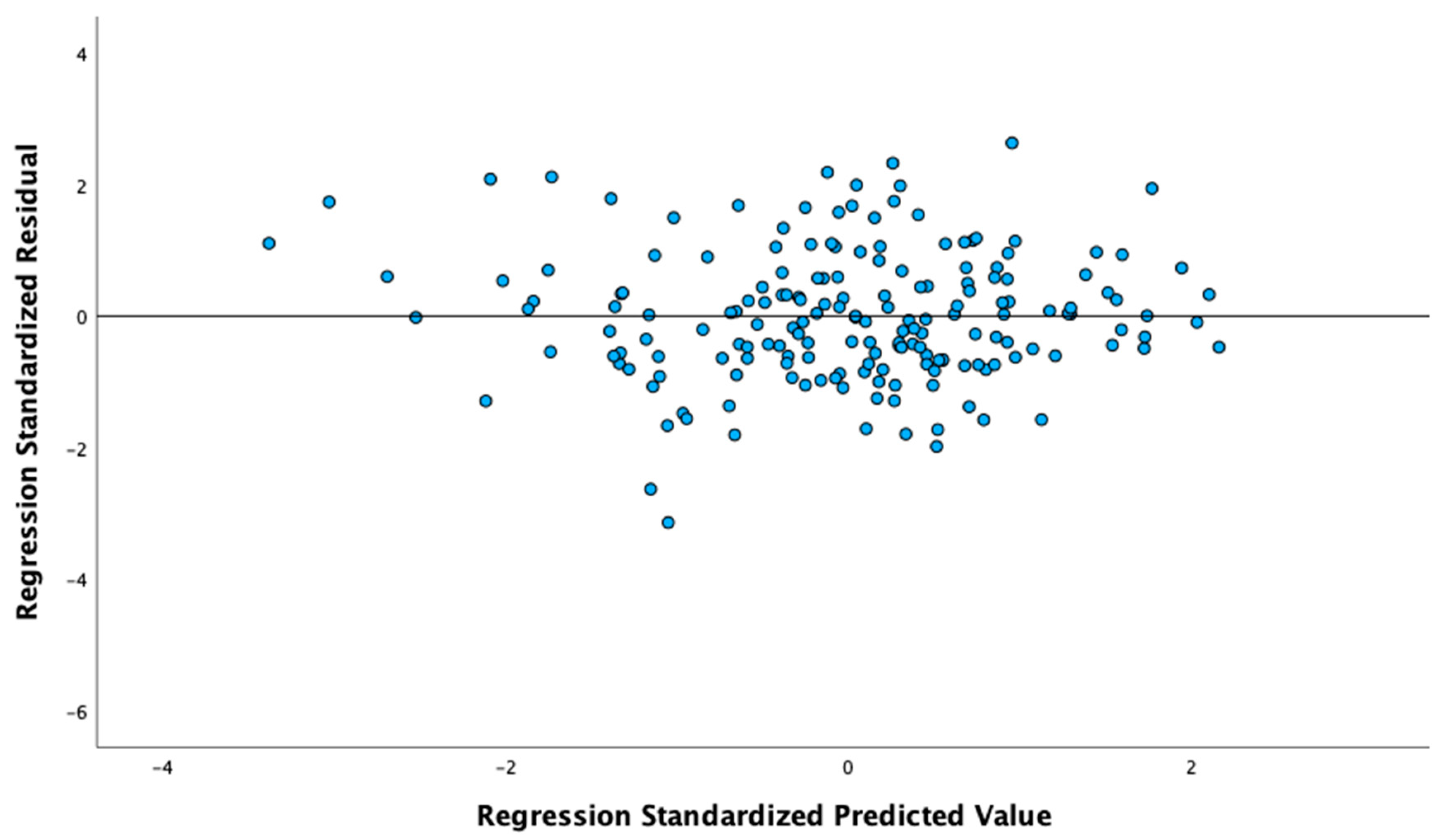
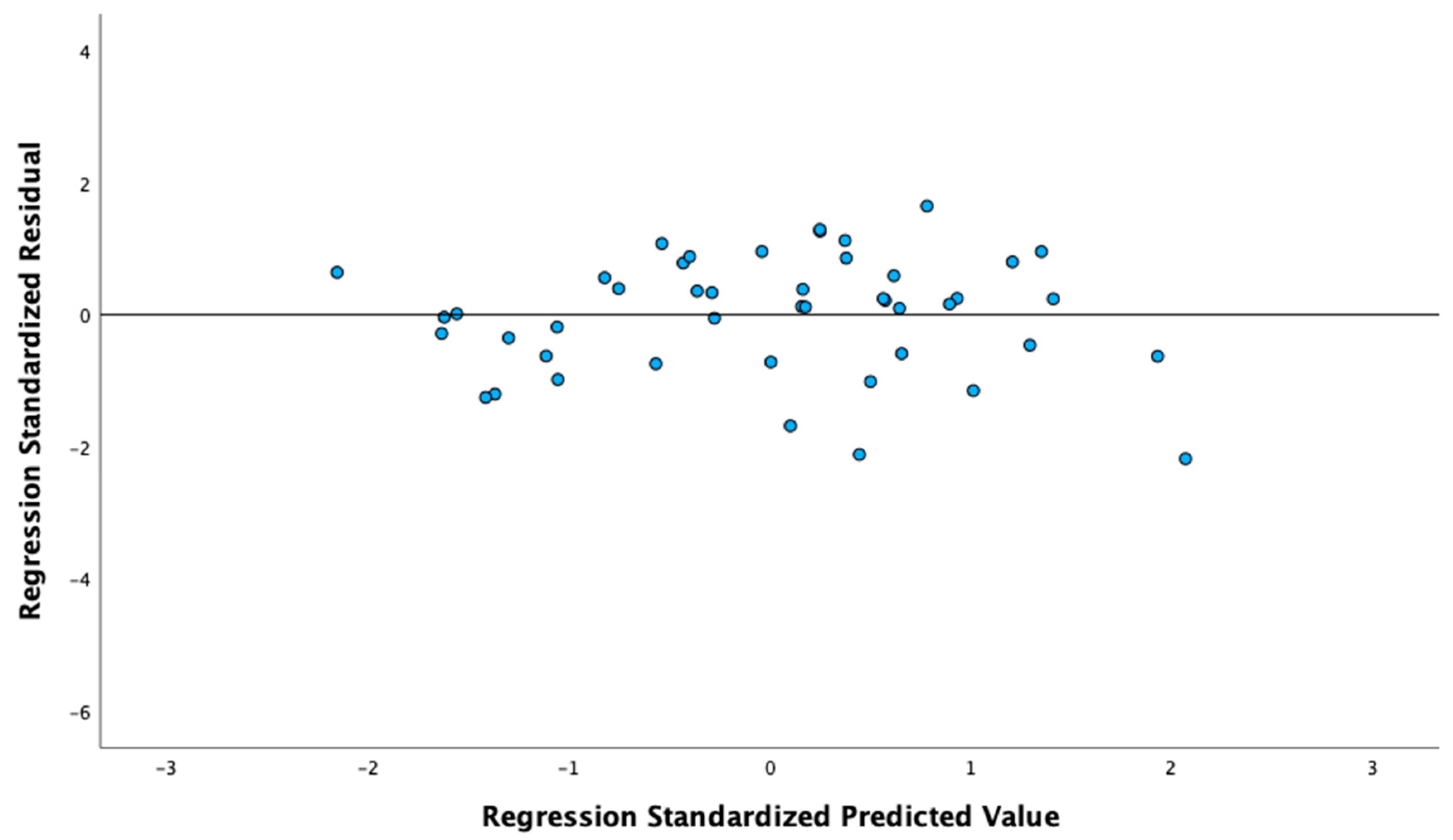
3.3. Multivariate Regression Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A










References
- Norrby, S. Sources of error in intraocular lens power calculation. J. Cataract Refract. Surg. 2008, 34, 368–376. [Google Scholar] [CrossRef] [PubMed]
- de Sanctis, U.; Loiacono, C.; Richiardi, L.; Turco, D.; Mutani, B.; Grignolo, F.M. Sensitivity and specificity of posterior corneal elevation measured by Pentacam in discriminating keratoconus/subclinical keratoconus. Ophthalmology 2008, 115, 1534–1539. [Google Scholar] [CrossRef] [PubMed]
- Moshirfar, M.; Brown, T.W.; Heiland, M.B.; Rosen, D.B.; Ronquillo, Y.C.; Hoopes, P.C. Comparative Analysis of LASIK Flap Diameter and its Centration Using Two Different Femtosecond Lasers. Med. Hypothesis Discov. Innov. Ophthalmol. 2019, 8, 241–249. [Google Scholar] [PubMed]
- Mifflin, M.D.; Betts, B.S.; Frederick, P.A.; Feuerman, J.M.; Fenzl, C.R.; Moshirfar, M.; Zaugg, B. Efficacy and safety of a 3-month loteprednol etabonate 0.5% gel taper for routine prophylaxis after photorefractive keratectomy compared to a 3-month prednisolone acetate 1% and fluorometholone 0.1% taper. Clin. Ophthalmol. 2017, 11, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Payne, C.J.; Webster, C.R.; Moshirfar, M.; Handlon, J.J.; Ronquillo, Y.C.; Hoopes, P.C. One-Year Visual Outcomes and Corneal Higher-Order Aberration Assessment of Small-Incision Lenticule Extraction for the Treatment of Myopia and Myopic Astigmatism. J. Clin. Med. 2022, 11, 6294. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, A.; Kojima, T.; Yamamoto, M.; Kato, Y.; Tamaoki, A.; Ichikawa, K. Impact of the anterior-posterior corneal radius ratio on intraocular lens power calculation errors. Clin. Ophthalmol. 2018, 12, 1549–1558. [Google Scholar] [CrossRef] [PubMed]
- Dubbelman, M.; Weeber, H.A.; van der Heijde, R.G.; Völker-Dieben, H.J. Radius and asphericity of the posterior corneal surface determined by corrected Scheimpflug photography. Acta Ophthalmol. Scand. 2002, 80, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Wu, Q.; Liu, B.; Wu, G.; Fan, J.; Hu, Y.; Yu, H. A Multicenter Study of the Distribution Pattern of Posterior-To-Anterior Corneal Curvature Radii Ratio in Chinese Myopic Patients. Front. Med. 2021, 8, 724674. [Google Scholar] [CrossRef] [PubMed]
- Montalbán, R.; Alio, J.L.; Javaloy, J.; Piñero, D.P. Comparative analysis of the relationship between anterior and posterior corneal shape analyzed by Scheimpflug photography in normal and keratoconus eyes. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 251, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Muthu Krishnan, V.; Jayalatha, K.; Vijayakumar, C. Correlation of Central Corneal Thickness and Keratometry with Refraction and Axial Length: A Prospective Analytic Study. Cureus 2019, 11, e3917. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wu, J.; Wu, S.; Zhu, D.; Miao, Y.; Huang, C.; Akiti, S.; Vinciguerra, R.; Zhang, X.; Zhang, P.; et al. Regional Changes in Posterior Corneal Surface During a 6-Month Follow-up Period After tPRK, FS-LASIK, and SMILE. J. Refract. Surg. 2022, 38, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Diener, R.; Eter, N.; Alnawaiseh, M. Using the posterior to anterior corneal curvature radii ratio to minimize the risk of a postoperative hyperopic shift after Descemet membrane endothelial keratoplasty. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 1065–1071. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | LASIK | PRK | SMILE | |
|---|---|---|---|---|
| No. of Eyes | 393 | 164 | 183 | 46 |
| No. of Patients | 215 | 91 | 100 | 25 |
| Male | 116 | 55 | 50 | 11 |
| Female | 99 * | 36 | 50 | 14 |
| Age (y) | 33.45 ± 6.37 | 33.75 ± 7.14 | 33.273 ± 5.7 | 33.087 ± 5.92 |
| (20 to 51) | (20 to 51) | (20 to 45) | (22 to 45) | |
| Cylinder (D) | −0.759 ± 0.63 | −0.825 ± 0.65 | −0.793 ± 0.65 | −0.388 ± 0.34 |
| (−5.75 to 0) | (−5.75 to 0) | (−4.25 to 0) | (−1.25 to 0) | |
| MRSE (D) | −3.644 ± 1.7 | −3.308 ± 1.82 | −3.598 ± 1.46 | −5.025 ± 1.45 |
| (−7.71 to −2.66) | (−7.61 to −0.25) | (−7.30 to −0.37) | (−7.71 to −2.66) | |
| P/A 4 mm | 0.826 ± 0.02 | 0.826 ± 0.02 | 0.827 ± 0.02 | 0.823 ± 0.01 |
| (0.784 to 0.910) | (0.787 to 0.873) | (0.784 to 0.910) | (0.787 to 0.844) | |
| P/A 5 mm | 0.822 ± 0.02 | 0.822 ± 0.02 | 0.823 ± 0.02 | 0.819 ± 0.01 |
| (0.781 to 0.888) | (0.785 to 0.888) | (0.781 to 0.86) | (0.789 to 0.836) | |
| P/A 6 mm | 0.821 ± 0.01 | 0.821 ± 0.01 | 0.822 ± 0.02 | 0.818 ± 0.01 |
| (0.781 to 0.863) | (0.785 to 0.863) | (0.781 to 0.86) | (0.789 to 0.833) | |
| Pachymetry (µm) | 536.784 ± 31.23 | 547.793 ± 25.28 | 523.53 ± 30.29 | 550.261 ± 33.03 |
| (453 to 617) | (501 to 617) | (453 to 593) | (489 to 615) | |
| Anterior Q | −0.333 ± 0.12 | −0.326 ± 0.13 | −0.34 ± 0.12 | −0.33 ± 0.11 |
| (−0.71 to 0.01) | (−0.71 to 0.01) | (−0.69 to 0.01) | (−0.60 to −0.14) | |
| Posterior Q | −0.343 ± 0.14 | −0.338 ± 0.14 | −0.35 ± 0.14 | −0.333 ± 0.12 |
| (−0.76 to 0.03) | (−0.73 to 0.03) | (−0.76 to −0.03) | (−0.52 to −0.12) | |
| Keratometry (D) | 43.901 ± 1.24 | 43.695 ± 1.29 | 44.101 ± 1.21 | 43.837 ± 1.03 |
| (40.00 to 47.80) | (40.00 to 47.20) | (41.20 to 47.80) | (41.70 to 46.00) |
| All (n = 393) | LASIK (n = 164) | PRK (n = 183) | SMILE (n = 46) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameters | Preop P/A | Postop P/A | Postop P/A | Postop P/A | |||||
| r | p | r | p | r | p | r | p | ||
| Age | 0.195 ** | <0.001 | 0.115 | 0.141 | 0.051 | 0.496 | 0.131 | 0.386 | 4 mm |
| Sex | −0.007 | 0.886 | 0.060 | 0.447 | 0.121 | 0.103 | −0.005 | 0.974 | |
| Cylinder | 0.011 | 0.821 | 0.037 | 0.634 | 0.055 | 0.458 | 0.096 | 0.525 | |
| MRSE | −0.115 * | 0.023 | 0.833 ** | <0.001 | 0.791 ** | <0.001 | 0.747 ** | <0.001 | |
| Anterior Q | 0.031 | 0.544 | 0.200 * | 0.010 | 0.180 * | 0.015 | −0.083 | 0.583 | |
| Posterior Q | 0.400 ** | <0.001 | 0.277 ** | <0.001 | 0.177 * | 0.017 | 0.406 ** | 0.005 | |
| Pachymetry | −0.450 ** | <0.001 | −0.131 | 0.094 | −0.167 * | 0.024 | −0.169 | 0.262 | |
| Anterior Km | −0.105 * | 0.038 | 0.226 ** | 0.004 | −0.225 ** | 0.002 | −0.199 | 0.186 | |
| Posterior Km | 0.602 ** | <0.001 | −0.040 | 0.613 | 0.381 ** | <0.001 | 0.440 ** | 0.002 | |
| Preop P/A | 1 | 0.289 ** | <0.001 | 0.388 ** | <0.001 | 0.573 ** | <0.001 | ||
| Age | 0.213 ** | <0.001 | 0.133 | 0.091 | 0.072 | 0.335 | 0.167 | 0.267 | 5 mm |
| Sex | 0.013 | 0.797 | 0.072 | 0.360 | 0.130 | 0.079 | 0.008 | 0.956 | |
| Cylinder | −0.001 | 0.985 | 0.033 | 0.676 | 0.070 | 0.349 | 0.128 | 0.395 | |
| MRSE | −0.106 * | 0.036 | 0.837 ** | <0.001 | 0.799 ** | <0.001 | 0.772 ** | <0.001 | |
| Anterior Q | 0.048 | 0.341 | 0.194 * | 0.013 | 0.183 * | 0.013 | −0.076 | 0.617 | |
| Posterior Q | 0.376 ** | <0.001 | 0.261 ** | <0.001 | 0.155 * | 0.037 | 0.374 * | 0.010 | |
| Pachymetry | −0.440 ** | <0.001 | −0.128 | 0.103 | −0.161 * | 0.029 | −0.167 | 0.266 | |
| Anterior Km | −0.092 | 0.069 | 0.224 ** | 0.004 | −0.197 ** | 0.008 | −0.204 | 0.175 | |
| Posterior Km | 0.580 ** | <0.001 | −0.062 | 0.431 | 0.369 ** | <0.001 | 0.396 ** | 0.006 | |
| Preop P/A | 1 | 0.298 ** | <0.001 | 0.391 ** | <0.001 | 0.536 ** | <0.001 | ||
| Age | 0.239 ** | <0.001 | 0.153 * | 0.050 | 0.093 | 0.210 | 0.231 | 0.123 | 6 mm |
| Sex | 0.017 | 0.731 | 0.079 | 0.317 | 0.144 | 0.052 | 0.022 | 0.887 | |
| Cylinder | −0.006 | 0.912 | 0.038 | 0.628 | 0.095 | 0.202 | 0.148 | 0.325 | |
| MRSE | −0.106 * | 0.036 | 0.825 ** | <0.001 | 0.779 ** | <0.001 | 0.749 ** | <0.001 | |
| Anterior Q | 0.064 | 0.208 | 0.197 * | 0.011 | 0.186 * | 0.012 | −0.077 | 0.609 | |
| Posterior Q | 0.336 ** | <0.001 | 0.251 ** | 0.001 | 0.131 | 0.077 | 0.351 * | 0.017 | |
| Pachymetry | −0.431 ** | <0.001 | −0.134 | 0.086 | −0.160 * | 0.030 | −0.188 | 0.212 | |
| Anterior Km | −0.077 | 0.128 | 0.240 ** | 0.002 | −0.194 ** | 0.009 | −0.219 | 0.144 | |
| Posterior Km | 0.556 ** | <0.001 | −0.070 | 0.371 | 0.379 ** | <0.001 | 0.392 ** | 0.007 | |
| Preop P/A | 1 | 0.324 ** | <0.001 | 0.410 ** | <0.001 | 0.503 ** | <0.001 | ||
| 4 mm | 5 mm | 6 mm | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Partial ß | Std. ß | p Value | Partial ß | Std. ß | p Value | Partial ß | Std. ß | p Value | |||
| Intercept | −0.0304 | 0.54 | Intercept | 0.0088 | 0.861 | Intercept | −0.0521 | 0.23 | |||
| MRSE | 0.0154 | 0.935 | <0.001 | MRSE | 0.0152 | 0.942 | <0.001 | MRSE | 0.0142 | 0.925 | <0.001 |
| Preop P/A | 0.9048 | 0.468 | <0.001 | Preop P/A | 0.8492 | 0.446 | <0.001 | Preop P/A | 0.9512 | 0.478 | <0.001 |
| Posterior Km | −0.0156 | −0.114 | <0.001 | Age | 0.0005 | 0.128 | <0.001 | Age | 0.0004 | 0.102 | <0.001 |
| Age | 0.0004 | 0.086 | <0.001 | Posterior Km | −0.0150 | −0.113 | <0.001 | Posterior Km | −0.0125 | −0.096 | <0.001 |
| Anterior Q | 0.0103 | 0.043 | 0.023 | Anterior Q | 0.0087 | 0.039 | 0.021 | ||||
| Adjusted R2: 0.944 | Adjusted R2: 0.941 | Adjusted R2: 0.956 | |||||||||
| 4 mm | 5 mm | 6 mm | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Partial ß | Std. ß | p Value | Partial ß | Std. ß | p Value | Partial ß | Std. ß | p Value | |||
| Intercept | 0.2887 | <0.001 | Intercept | 0.2136 | <0.001 | Intercept | 0.1675 | <0.001 | |||
| MRSE | 0.0136 | 0.816 | <0.001 | MRSE | 0.0135 | 0.831 | <0.001 | MRSE | 0.0128 | 0.821 | <0.001 |
| Preop P/A | 0.6831 | 0.476 | <0.001 | Preop P/A | 0.7547 | 0.493 | <0.001 | Preop P/A | 0.8084 | 0.526 | <0.001 |
| Anterior Q | 0.0203 | 0.098 | <0.001 | Anterior Q | 0.0172 | 0.086 | <0.001 | Anterior Q | 0.0154 | 0.080 | <0.001 |
| Pachymetry | −5.84 × 10−5 | −0.073 | 0.007 | Age | 0.0003 | 0.060 | 0.003 | Age | 0.0003 | 0.066 | <0.001 |
| Pachymetry | −4.72 × 10−5 | −0.060 | 0.008 | Pachymetry | −4.41 × 10−5 | −0.059 | 0.007 | ||||
| Adjusted R2: 0.900 | Adjusted R2: 0.930 | Adjusted R2: 0.934 | |||||||||
| 4 mm | 5 mm | 6 mm | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Partial ß | Std. ß | p Value | Partial ß | Std. ß | p Value | Partial ß | Std. ß | p Value | |||
| Intercept | 0.2756 | 0.001 | Intercept | 0.3848 | <0.001 | Intercept | 0.3815 | <0.001 | |||
| MRSE | 0.0103 | 0.680 | <0.001 | MRSE | 0.0108 | 0.762 | <0.001 | MRSE | 0.0100 | 0.774 | <0.001 |
| Preop P/A | 0.6570 | 0.454 | <0.001 | Preop P/A | 0.5001 | 0.343 | <0.001 | Preop P/A | 0.4972 | 0.349 | <0.001 |
| Post. Q | 0.0474 | 0.291 | <0.001 | Post. Q | 0.0421 | 0.278 | <0.001 | Post. Q | 0.0349 | 0.251 | <0.001 |
| Age | 0.0006 | 0.181 | 0.008 | Age | 0.0006 | 0.217 | 0.002 | ||||
| Adjusted R2: 0.873 | Adjusted R2: 0.890 | Adjusted R2: 0.894 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cha, D.S.; Moshirfar, M.; Herron, M.S.; Santos, J.M.; Hoopes, P.C. Prediction of Posterior-to-Anterior Corneal Curvature Radii Ratio in Myopic Patients after LASIK, SMILE, and PRK Using Multivariate Regression Analysis. J. Clin. Med. 2023, 12, 4536. https://doi.org/10.3390/jcm12134536
Cha DS, Moshirfar M, Herron MS, Santos JM, Hoopes PC. Prediction of Posterior-to-Anterior Corneal Curvature Radii Ratio in Myopic Patients after LASIK, SMILE, and PRK Using Multivariate Regression Analysis. Journal of Clinical Medicine. 2023; 12(13):4536. https://doi.org/10.3390/jcm12134536
Chicago/Turabian StyleCha, David S., Majid Moshirfar, Michael S. Herron, Jordan M. Santos, and Phillip C. Hoopes. 2023. "Prediction of Posterior-to-Anterior Corneal Curvature Radii Ratio in Myopic Patients after LASIK, SMILE, and PRK Using Multivariate Regression Analysis" Journal of Clinical Medicine 12, no. 13: 4536. https://doi.org/10.3390/jcm12134536
APA StyleCha, D. S., Moshirfar, M., Herron, M. S., Santos, J. M., & Hoopes, P. C. (2023). Prediction of Posterior-to-Anterior Corneal Curvature Radii Ratio in Myopic Patients after LASIK, SMILE, and PRK Using Multivariate Regression Analysis. Journal of Clinical Medicine, 12(13), 4536. https://doi.org/10.3390/jcm12134536