
Impacts of Whole-Body Vibration on Muscle Strength, Power, and Endurance in Older Adults: A Systematic Review and Meta-Analysis

 ,
, 
 ,
,  ,
, 

Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Databases and Search Strategy
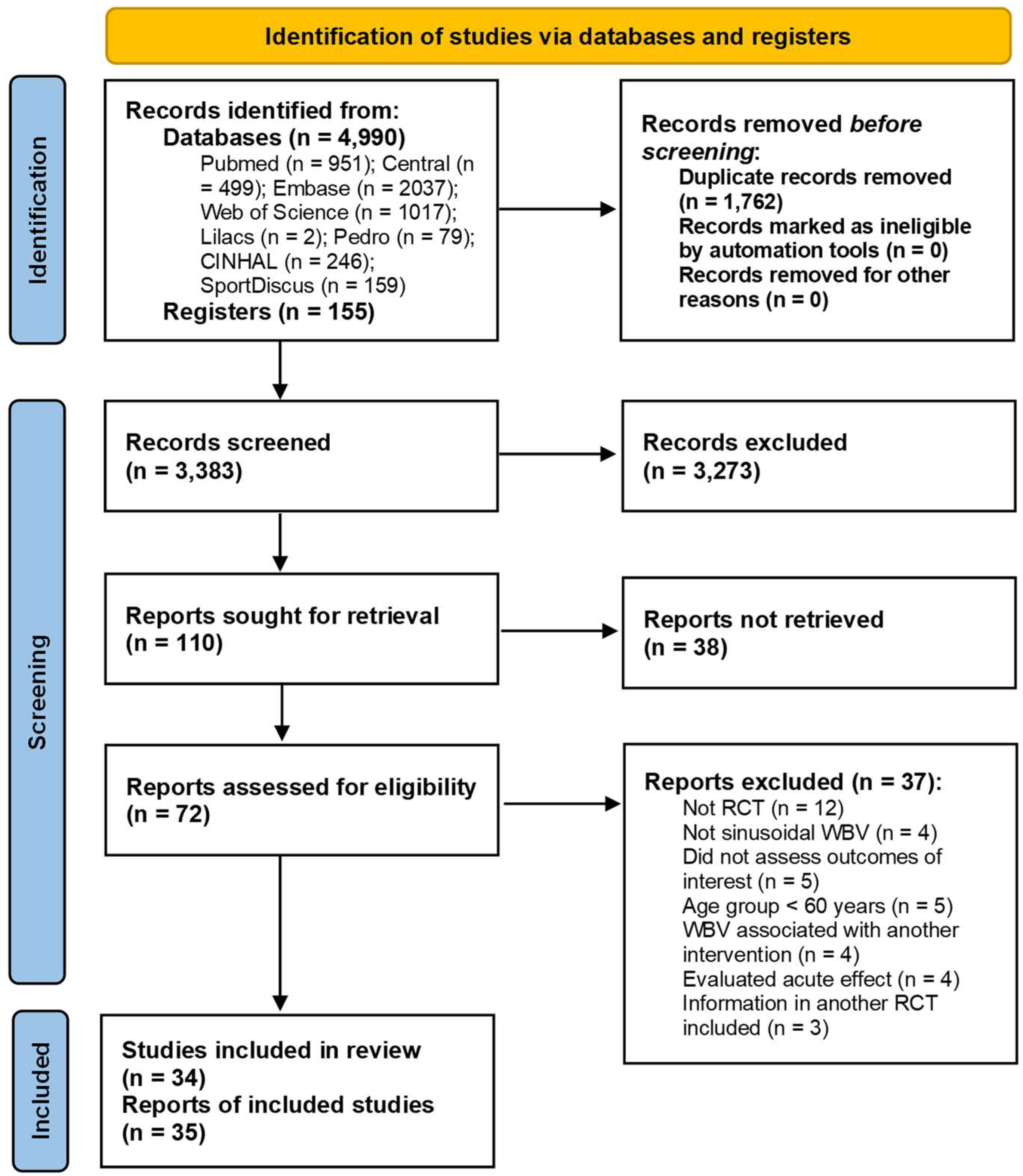
2.3. Selection of Studies
2.4. Data Extraction
2.5. Assessment of the Methodological Quality of Studies
2.6. Definition
2.7. Data Analysis
3. Results
3.1. Qualitative Synthesis of Studies
3.2. Methodological Quality of Studies
3.3. Quantitative Synthesis of Studies (Meta-Analysis)
3.3.1. Primary Analysis
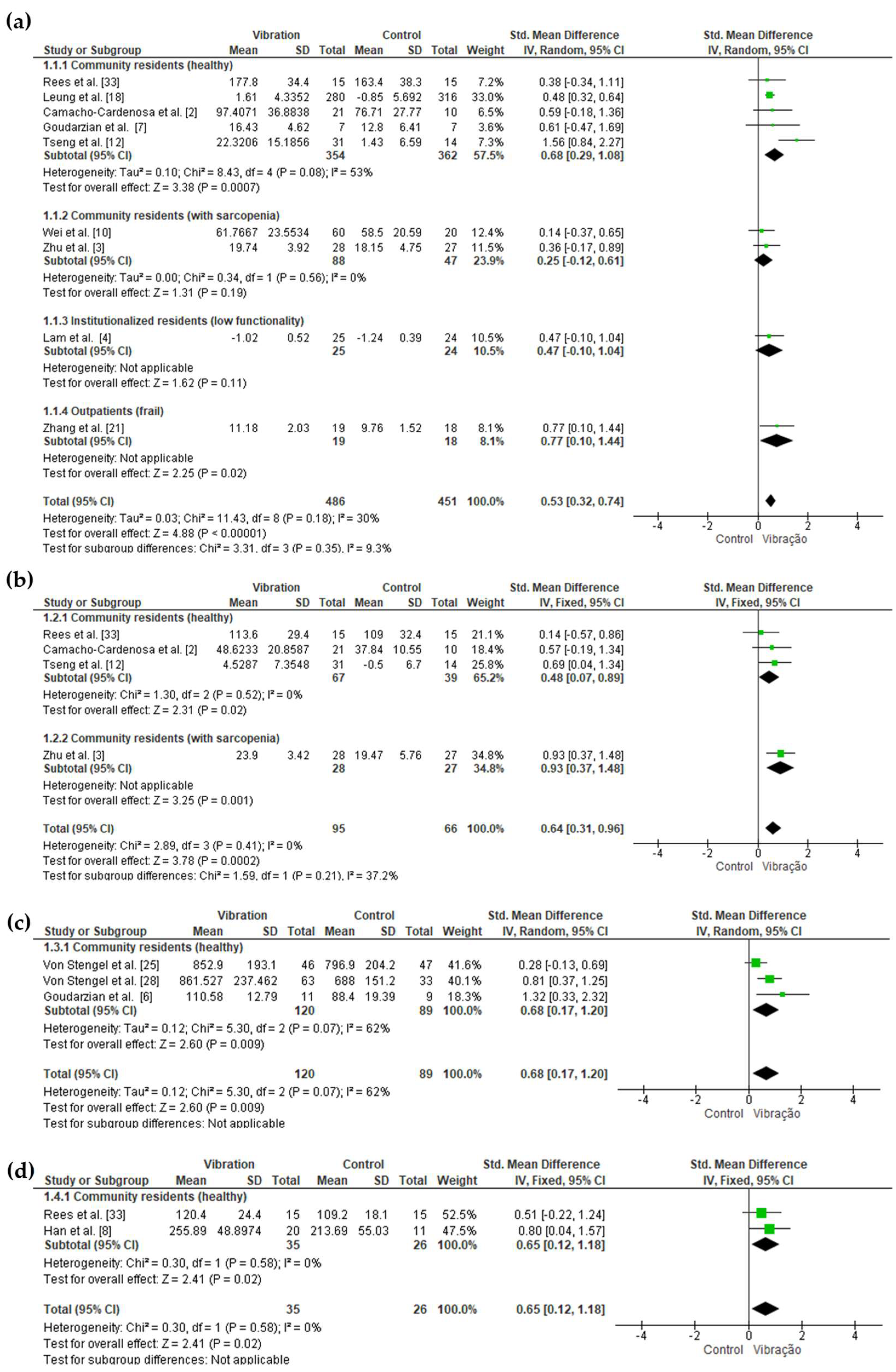
Muscle Strength
Muscle Power
Muscle Endurance
3.3.2. Sensitivity Analysis
3.3.3. WBV vs. Other Exercise Modalities
3.3.4. Static Positioning vs. Dynamic Exercises during WBV
3.3.5. Vibration Type (Synchronous vs. Side-Alternating)
3.3.6. Cumulative Dose of WBV
3.3.7. WBV Magnitude
4. Discussion
4.1. Summary of Main Results
4.2. Agreements and Disagreements with Other Studies
4.3. Quality of Evidence
4.4. Limitations of the Review Process
5. Conclusions
5.1. Implications for Practice
5.2. Implications for Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Genest, F.; Lindstrom, S.; Scherer, S.; Schneider, M.; Seefried, L. Feasibility of simple exercise interventions for men with osteoporosis—A prospective randomized controlled pilot study. Bone Rep. 2021, 15, 101099. [Google Scholar] [CrossRef] [PubMed]
- Camacho-Cardenosa, M.; Camacho-Cardenosa, A.; Brazo-Sayavera, J.; Olcina, G.; Tomas-Carus, P.; Timón, R. Evaluation of 18-Week Whole-Body Vibration Training in Normobaric Hypoxia on Lower Extremity Muscle Strength in an Elderly Population. High. Alt. Med. Biol. 2019, 20, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Peng, N.; Zhou, M.; Liu, P.P.; Qi, X.L.; Wang, N.; Wang, G.; Wu, Z.P. Tai Chi and whole-body vibrating therapy in sarcopenic men in advanced old age: A clinical randomized controlled trial. Eur. J. Ageing 2019, 16, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Lam, F.M.; Chan, P.F.; Liao, L.R.; Woo, J.; Hui, E.; Lai, C.W.; Kwok, T.C.; Pang, M.Y. Effects of whole-body vibration on balance and mobility in institutionalized older adults: A randomized controlled trial. Clin. Rehabil. 2018, 32, 462–472. [Google Scholar] [CrossRef]
- Pessoa, M.F.; Brandão, D.C.; Sá, R.B.; Aguiar, M.I.R.; de Souza, H.C.M.; de Melo Barcelar, J.; Reinaux, C.M.A.; de Andrade, A.D. Whole-Body Vibration Increases Cardiopulmonary Performance in the Elderly—A Randomized Double-Blind Clinical Trial. Top. Geriatr. Rehabil. 2018, 34, 245–250. [Google Scholar] [CrossRef]
- Goudarzian, M.; Ghavi, S.; Shariat, A.; Shirvani, H.; Rahimi, M. Effects of whole body vibration training and mental training on mobility, neuromuscular performance, and muscle strength in older men. J. Exerc. Rehabil. 2017, 13, 573–580. [Google Scholar] [CrossRef]
- Goudarzian, M.; Rahimi, M.; Karimi, N.; Samadi, A.; Ajudani, R.; Sahaf, R.; Ghavi, S. Mobility, Balance, and Muscle Strength Adaptations to Short-Term Whole Body Vibration Training Plus Oral Creatine Supplementation in Elderly Women. Asian J. Sports Med. 2017, 8, e36793. [Google Scholar] [CrossRef]
- Han, S.; Lee, D.; Choi, D.; Han, B.; Kim, J.S.; Lee, H.D. Asynchronous Alterations of Muscle Force and Tendon Stiffness Following 8-week Resistance Exercise with Whole-Body Vibration in Older Women. J. Aging Phys. Act. 2016, 25, 287–294. [Google Scholar] [CrossRef]
- Wei, N.; Pang, M.Y.; Ng, S.S.; Ng, G.Y. Optimal frequency/time combination of whole body vibration training for developing Physical performance of people with sarcopenia: A randomized controlled trial. Clin. Rehabil. 2017, 31, 1313–1321. [Google Scholar] [CrossRef]
- Wei, N.; Pang, M.Y.; Ng, S.S.; Ng, G.Y. Optimal frequency/time combination of whole-body vibration training for improving muscle size and strength of people with age-related muscle loss (sarcopenia): A randomized controlled trial. Geriatr. Gerontol. Int. 2017, 17, 1412–1420. [Google Scholar] [CrossRef]
- Smith, D.T.; Judge, S.; Malone, A.; Moynes, R.C.; Conviser, J.; Skinner, J.S. Effects of bioDensity Training and Power Plate Whole-Body Vibration on Strength, Balance, and Functional Independence in Older Adults. J. Aging Phys. Act. 2016, 24, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Tseng, S.Y.; Lai, C.L.; Chang, K.L.; Hsu, P.S.; Lee, M.C.; Wang, C.H. Influence of Whole-Body Vibration Training Without Visual Feedback on Balance and Lower-Extremity Muscle Strength of the Elderly: A Randomized Controlled Trial. Medicine 2016, 95, e2709. [Google Scholar] [CrossRef] [PubMed]
- Casimiro, J.A.; Amaral, L.E.F.; Ferreira, P.C.; Coelho, M.A.G.M.; Borges, V.S. Efeitos de um protocolo de exercícios sobre a plataforma vibratória na força muscular, equilíbrio e desempenho de marcha em idosas comunitárias. Fisioter. Bras. 2015, 16, 25–31. [Google Scholar]
- Corrie, H.; Brooke-Wavell, K.; Mansfield, N.J.; Cowley, A.; Morris, R.; Masud, T. Effects of vertical and side-alternating vibration training on fall risk factors and bone turnover in older people at risk of falls. Age Ageing 2015, 44, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Santin-Medeiros, F.; Rey-Lopez, J.P.; Santos-Lozano, A.; Cristi-Montero, C.S.; Garatachea Vallejo, N. Effects of eight months of whole-body vibration training on the muscle mass and functional capacity of elderly women. J. Strength. Cond. Res. 2015, 29, 1863–1869. [Google Scholar] [CrossRef]
- Sitjà-Rabert, M.; Martínez-Zapata, M.J.; Fort Vanmeerhaeghe, A.; Rey Abella, F.; Romero-Rodríguez, D.; Bonfill, X. Effects of a Whole Body Vibration (WBV) Exercise Intervention for Institutionalized Older People: A Randomized, Multicentre, Parallel, Clinical Trial. J. Am. Med. Dir. Assoc. 2015, 16, 125–131. [Google Scholar] [CrossRef]
- Álvarez-Barbosa, F.; del Pozo-Cruz, J.; del Pozo-Cruz, B.; Alfonso-Rosa, R.M.; Rogers, M.E.; Zhang, Y. Effects of supervised whole body vibration exercise on fall risk factors, functional dependence and health-related quality of life in nursing home residents aged 80+. Maturitas 2014, 79, 456–463. [Google Scholar] [CrossRef]
- Leung, K.S.; Li, C.Y.; Tse, Y.K.; Choy, T.K.; Leung, P.C.; Hung, V.W.; Chan, S.Y.; Leung, A.H.; Cheung, W.H. Effects of 18-month low-magnitude high-frequency vibration on fall rate and fracture risks in 710 community elderly—A cluster-randomized controlled trial. Osteoporos. Int. 2014, 25, 1785–1795. [Google Scholar] [CrossRef]
- Osugi, T.; Iwamoto, J.; Yamazaki, M.; Takakuwa, M. Effect of a combination of whole body vibration exercise and squat training on body balance, muscle power, and walking ability in the elderly. Ther. Clin. Risk Manag. 2014, 10, 131–138. [Google Scholar]
- Sievänen, H.; Karinkanta, S.; Moisio-Vilenius, P.; Ripsaluoma, J. Feasibility of whole-body vibration training in nursing home residents with low physical function: A pilot study. Aging Clin. Exp. Res. 2014, 26, 511–517. [Google Scholar] [CrossRef]
- Zhang, L.; Weng, C.; Liu, M.; Wang, Q.; Liu, L.; He, Y. Effect of whole-body vibration exercise on mobility, balance ability and general health status in frail elderly patients: A pilot randomized controlled trial. Clin. Rehabil. 2014, 28, 59–68. [Google Scholar] [CrossRef]
- Calder, C.G.; Mannion, J.; Metcalf, P.A. Low-intensity whole-body vibration training to reduce fall risk in active, elderly residents of a retirement village. J. Am. Geriatr. Soc. 2013, 61, 1424–1426. [Google Scholar] [CrossRef]
- Dudoniene, V.; Sakaliene, R.; Svediene, L.; Kazlauskiene, D.; Szczegielniak, J.; Krutulyte, G. Impact of whole body vibration on balance improvement in elderly women. J. Vibroengineering 2013, 15, 1112–1118. [Google Scholar]
- Gómez-Cabello, A.; González-Agüero, A.; Ara, I.; Casajús, J.A.; Vicente-Rodríguez, G. Effects of a short-term whole body vibration intervention on physical fitness in elderly people. Maturitas 2013, 74, 276–278. [Google Scholar] [CrossRef] [PubMed]
- Von Stengel, S.; Kemmler, W.; Engelke, K.; Kalender, W.A. Effect of whole-body vibration on neuromuscular performance and body composition for females 65 years and older: A randomized-controlled trial. Scand. J. Med. Sci. Sports 2012, 22, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Marín, P.J.; Martín-López, A.; Vicente-Campos, D.; Angulo-Carrere, M.; García-Pastor, T.; Garatachea, N.; Chicharro, J.L. Effects of vibration training and detraining on balance and muscle strength in older adults. J. Sports Sci. Med. 2011, 10, 559–564. [Google Scholar]
- Verschueren, S.M.P.; Bogaerts, A.; Delecluse, C.; Claessens, A.L.; Haentjens, P.; Vanderschueren, D.; Boonen, S. The Effects of Whole-Body Vibration Training and Vitamin D Supplementation on Muscle Strength, Muscle Mass, and Bone Density in Institutionalized Elderly Women: A 6-Month Randomized, Controlled Trial. J. Bone Miner. 2011, 26, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Von Stengel, S.; Kemmler, W.; Bebenek, M.; Engelke, K.; Kalender, W.A. Effects of Whole-Body Vibration Training on Different Devices on Bone Mineral Density. Med. Sci. Sports Exerc. 2011, 43, 1071–1079. [Google Scholar] [CrossRef]
- Machado, A.; Garcıa-Lopez, D.; Gonzalez-Gallego, J.; Garatachea, N. Whole-body vibration training increases muscle strength and mass in older women: A randomized-controlled trial. Scand. J. Med. Sci. Sports 2010, 20, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Bogaerts, A.C.G.; Delecluse, C.; Claessens, A.L.; Troosters, T.; Boonen, S.; Verschueren, S.M. Effects of whole body vibration training on cardiorespiratory fitness and muscle Strength in older individuals (a 1-year randomised controlled trial). Age Ageing 2009, 38, 448–454. [Google Scholar] [CrossRef]
- Furness, T.P.; Maschette, W.E. Influence of whole body vibration platform frequency on neuromuscular performance of community-dwelling older adults. J. Strength. Cond. Res. 2009, 23, 1508–1513. [Google Scholar] [CrossRef]
- Bogaerts, A.; Delecluse, C.; Claessens, A.L.; Coudyzer, W.; Boonen, S.; Verschueren, S.M. Impact of Whole-Body Vibration Training Versus Fitness Training on Muscle Strength and Muscle Mass in Older Men: A 1-Year Randomized Controlled Trial. J. Gerontol. Med. Sci. 2007, 62, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Rees, S.; Murphy, A.; Watsford, M. Effects of Vibration Exercise on Muscle Performance and Mobility in an Older Population. J. Aging Phys. Act. 2007, 15, 367–381. [Google Scholar] [CrossRef]
- Bautmans, I.; Hees, E.V.; Lemper, J.; Mets, T. The feasibility of whole body vibration in institutionalised elderly persons and its influence on muscle performance, balance and mobility: A randomised controlled trial. BMC Geriatr. 2005, 5, 17. [Google Scholar] [CrossRef]
- Runge, M.; Rehfeld, G.; Resnicek, E. Balance training and exercise in geriatric patients. J. Musculoskel Neuron Interact. 2000, 1, 61–65. [Google Scholar]
- Lau, R.W.K.; Liao, L.; Yu, F.; Teo, T.; Chung, R.C.K.; Pang, M.Y.C. The effects of whole body vibration therapy on bone mineral density and leg muscle strength in older adults: A systematic review and meta-analysis. Clin. Rehabil. 2011, 25, 975–988. [Google Scholar] [CrossRef] [PubMed]
- Osawa, Y.; Oguma, Y.; Ishii, N. The effects of whole-body vibration on muscle strength and power: A meta-analysis. J. Musculoskelet. Neuronal Interact. 2013, 13, 380–390. [Google Scholar] [PubMed]
- Rogan, S.; Bruin, E.D.; Radlinger, L.; Joehr, C.; Wyss, C.; Stuck, N.; Bruelhart, Y.; Bie, R.A.; Hilfiker, R. Effects of whole-body vibration on proxies of muscle strength in old adults: A systematic review and meta-analysis on the role of physical capacity level. Eur. Rev. Aging Phys. Act. 2015, 12, 12. [Google Scholar] [CrossRef]
- Pessoa, M.F.; Brandão, D.C.; Sá, R.B.; Souza, H.C.M.; Fuzari, H.K.B.; Andrade, A.D. Effects of whole body vibration on muscle strength and quality of life in health elderly: A meta-analysis. Fisioter. Mov. 2017, 30, 171–182. [Google Scholar] [CrossRef]
- Wu, S.; Ning, H.; Xiao, S.; Hu, M.; Wu, X.; Deng, H.; Feng, H. Effects of vibration therapy on muscle mass, muscle strength and physical function in older adults with sarcopenia: A systematic review and meta-analysis. Eur Rev Aging Phys Act. 2020, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Šarabon, N.; Kozinc, Z.; Löfler, S.; Hofer, C. Resistance Exercise, Electrical Muscle Stimulation, and Whole-Body Vibration in Older Adults: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 2902. [Google Scholar] [CrossRef]
- Eklund, G.; Hagbarth, K.E. Normal variability of tonic vibration reflexes in man. Exp. Neurol. 1966, 16, 80–92. [Google Scholar] [CrossRef]
- Bosco, C.; Iacovelli, M.; Tsarpela, O.; Cardinale, M.; Bonifazi, M.; Tihanyi, J.; Viru, M.; De Lorenzo, A.; Viru, A. Hormonal responses to whole-body vibration in men. Eur. J. Appl. Physiol. 2000, 81, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, M.; Wakeling, J. Whole body vibration exercise: Are vibrations good for you? Br. J. Sports Med. 2005, 39, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Patrizio, E.; Calvani, R.; Marzetti, E.; Cesari, M. Physical Functional Assessment in Older Adults. J. Frailty Aging. 2021, 10, 141–149. [Google Scholar] [CrossRef]
- Runge, M.; Rittweger, J. Whole-Body Vibration in Geriatric Rehabilitation. In Manual of Vibration Exercise and Vibration Therapy; Rittweger, J., Ed.; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). Cochrane. Available online: www.training.cochrane.org/handbook (accessed on 10 August 2022).
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Rauch, F.; Sievanen, H.; Boonen, S.; Cardinale, M.; Degens, H.; Felsenberg, D.; Roth, J.; Schoenau, E.; Verschueren, S.; Rittweger, J. Reporting whole-body vibration intervention studies: Recommendations of the International Society of Musculoskeletal and Neuronal Interactions. J. Musculoskelet. Neuronal Interact. 2010, 10, 193–198. [Google Scholar]
- Van Heuvelen, M.; Rittweger, J.; Judex, S.; Sañudo, B.; Seixas, A.; Fuermaier, A.; Tucha, O.; Nyakas, C.; Marín, P.J.; Taiar, R.; et al. Reporting guidelines for whole-body vibration studies in humans, animals and cell cultures: A consensus statement from an international group of experts. Biology 2021, 10, 965. [Google Scholar] [CrossRef]
- de Oliveira, R.D.J.; de Oliveira, R.G.; de Oliveira, L.C.; Santos-Filho, S.D.; Sá-Caputo, D.C.; Bernardo-Filho, M. Effectiveness of whole-body vibration on bone mineral density in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Osteoporos. Int. 2023, 34, 29–52. [Google Scholar] [CrossRef]
- Rønnestad, B.R.; Holden, G.; Samnøy, L.E.; Paulsen, G. Acute effect of whole-body vibration on power, one-repetition maximum, and muscle activation in power lifters. J. Strength. Cond. Res. 2012, 26, 531–539. [Google Scholar] [CrossRef]
- Da Silva-Grigoletto, M.E.; Vaamonde, D.M.; Castillo, E.; Poblador, M.S.; García-Manso, J.M.; Lancho, J.L. Acute and cumulative effects of different times of recovery from whole body vibration exposure on muscle performance. J. Strength. Cond. Res. 2009, 23, 2073–2082. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.T.; Martin, J.R.; Jagim, A.R.; Oliver, J.M. Effect of Direct Whole-Body Vibration on Upper-Body Muscular Power in Recreational, Resistance-Trained Men. J. Strength. Cond. Res. 2017, 31, 1371–1377. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Year and Location | Total Number of Participants, Dwelling/Health Condition, Distribution by Sex and by Groups | Mean and SD (or Range) of the Age | Time of Exposure to Vibration and Mean Cumulative (MC) | Frequency (Hz), Peak to Peak Displacement (mm) and/or Magnitude (g) and Vibration Type | Position/Activity on the Vibrating Platform | Activities of Other Intervention Groups | Activities of the Control Group (CON) | Assessment of Muscle Strength, Power and/or Endurance | Differences between Groups Reported in the Original Publication (p < 0.05) | Adverse Events | Adherence and Compliance ‡ |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Genest et al., 2021 [1] Germany | 47 community/osteoporosis: 47(m); 0(f) WBV = 13 RT = 11 QG = 10 SO = 13 | All: 77.0 ± 6.1 WBV: 77.9 ± 6.2 RT: 75.9 ± 5.6 QG: 77.0 ± 7.9 SO: 77.2 ± 5.5 | Six months 2× week 2 min 30 s–8 min MC: ≈ 429 min | 5–25.5 Hz; 3 mm; 0.15–3.9 g * Side-alternating | Strengthening exercises for lower limbs | RT: 8 exercises focused on core strength (30 min, 2× week); QG: exercises of coordinated body posture, low-impact movements, breathing and meditation (45 min, 2× week); SO: use of back brace (180 min, 7× week) | - | Muscle strength: trunk flexion, trunk extension; handgrip Muscle power: 5TSTS | RT: improved (vs. QG) for trunk extension | No adverse event | Adherence: 100% Compliance: WBV: 83.2% RT: 71.3% QG: 65.1% SO: 85.2% |
| Camacho-Cardenosa et al., 2019 [2] Spain | 31 community/healthy: 11(m); 20(f) NWBV = 11 HWBV = 10 CON = 10 | NWBV: 70.2 ± 6.4 HWBV: 73.5 ± 4.7 CON: 73.4 ± 5.0 | 18 weeks 2× week 4 × 30 min (2 min total) MC: ≈ 72 min | 12.6 Hz; 4 mm; 2.5 g Side-alternating | Semi-flexed knees | - | Usual routine | Muscle strength: peak torque of knee extensors and flexors (60°/s) Muscular endurance: total work of knee extensors and flexors (180°/s) | No difference | No adverse event | Adherence: 75% Compliance: NWBV: 100% HWBV: 91.4% |
| Zhu et al., 2019 [3] China | 79 community/sarcopenic: 79(m); 0(f) WBV = 28 TC = 24 CON = 27 | All: 88.6 (85–101) WBV: 89.5 ± 4.4 TC: 88.8 ± 3.7 CON: 87.5 ± 3.0 | 8 weeks 5× week 5 × 3 min (15 min total) MC: ≈ 600 min | 12–16 Hz; 3–5 mm; 0.9–14.2 g * Side-alternating | Semi-flexed knees | TC: 10 min warm-up, 20 min practice, and 10 min relaxation (40 min, 5× week) | Usual routine | Muscle strength: handgrip and lower limbs (ankle dorciflexors, hip flexors, knee extensors and flexors) Muscle power: 5TSTS | WBV: improved (vs. CON) for 5TSTS, ankle dorciflexors, knee extensors and flexors; TC: improved (vs. CON) for 5TSTS, ankle dorciflexors, hip flexors and knee extensors | WBV: “other disorders” (7.1%) TC: low back pain (8.3%) | Unreported |
| Lam et al., 2018 [4] China | 73 institutionalized/low functionality: 33(m); 40(f) WBV + CT = 25 CT = 24 CON = 24 | All: 82.3 ± 7.3 WBV + CT: 84.0 ± 6.7 CT: 82.4 ± 7.6 CON: 80.3 ± 7.3 | 8 weeks 3× week 4 × 1 min (4 min total) MC: ≈ 96 min | 30–40 Hz; 0.9 mm; 3.4–4.7 g Synchronous | Strengthening exercises for lower limbs | CT: warm-up, mobility, strengthening, balance, and cool-down exercises (60 min, 3× week) | CON: social and recreational activities that only involved the upper limbs | Muscle strength: knee extensors Muscle power: 5TSTS | CT: improved (vs. CON) for 5TSTS | No adverse event | Adherence: 85% Compliance: WBV + CT: 77.1% CT: 67.5% CON: 74.5% |
| Pessoa et al., 2018 [5] Brazil | 31 community/healthy: 17(m); 14(f) WBV = 10 RT = 10 WBV + RT = 11 | WBV: 66.4 ± 2.6 RT: 68.2 ± 2.4 WBV + RT: 64.9 ± 2.8 | 12 weeks 3× week 10 × 1 min (10 min total)–20 × 1 min (20 min total) MC: ≈ 540 min | 35 Hz; 2–4 mm; 4.9–9.8 g * Synchronous | Semi-flexed knees | RT: strengthening exercises for upper and lower limbs (40 min, 3× week) plus WBV Sham WBV + RT: true WBV plus RT | - | Muscle strength: handgrip | No difference | No adverse event | Adherence: 91% Compliance: unreported |
| Goudarzian et al., 2017 [6] Iran | 42 community/healthy: 42(m); 0 (f) WBV = 11 MT = 12 WBV + MT = 10 CON = 9 | All: 68.0 ± 5.8 WBV: 66.6 ± 5.8 MT: 69.2 ± 3.9 WBV + MT: 67.8 ± 5.9 CON: 68.9 ± 7.5 | 8 weeks 3× week 6 × 45 s (4 min 30 s total)–6 × 80 s (8 min total) MC: ≈ 144 min | 30–35 Hz; 5–8 mm; 9.0–19.7 g * Side-alternating | Strengthening exercises for lower limbs | MT: Relaxation techniques, with breathing and mental training (3× week) | Usual routine | Muscle strength: lower limb isometry (leg press dynamometer) Muscle power: 5TSTS | WBV, MT and WBV + MT: improved (vs. CON) for lower limb isometry and 5TSTS | Unreported | Adherence: 87.5% Compliance: unreported |
| Goudarzian et al., 2017 [7] Iran | 22 institutionalized/healthy: 0(m); 22(f) WBV + P = 7 WBV + C = 8 CON = 7 | All: 66.0 ± 5.0 WBV + P: 66.0 ± 4.6 WBV + C: 64.9 ± 3.4 CON: 68.0 ± 9.2 | 10 consecutive days 6 × 45 s (4 min 30 s total)–6 × 65 s (6 min 30 s total) MC: ≈ 33 min | 30–35 Hz; 5 mm; 9–12.3 g * Side-alternating | Strengthening exercises for lower limbs | WBV + C: vibration associated with creatine supplementation (20 g/day [5 days] and 5 g/day [5 days]) | Usual routine | Muscle strength: handgrip, knee extensors (1RM) and back-leg-chest | WBV + P and WBV + C: improved (vs. CON) for knee extensors (1RM) WBV + P: improved (vs. CON) for back-leg-chest | No adverse event | Adherence: unreported Compliance: 97.8% |
| Han et al., 2017 [8] Korea | 40 community/healthy: 0(m); 40(f) WBV(I) = 13 WBV(E) = 12 CON = 15 | All: 69.0 ± 4.0 | 8 weeks 1× week WBV(I): 3 × 30 s (90 s total)–8 × 30 s (4 min total), MC: ≈ 23 min 30 s WBV(E): 3 × 30 s (90 s total)–8 × 60 s (8 min total), MC: ≈ 39 min | WBV(I): 25–40 Hz, 1.1–2.5 mm, 1.4–8.0 g * WBV(E): 25–35 Hz, 1.1 mm, 1.4–2.7 g * Synchronous | Strengthening exercises for lower limbs | - | Usual routine | Muscle strength: isometric ankle plantar flexion | No difference | Unreported | Unreported |
| Wei et al., 2017 [9,10] Hong Kong | 80 community/sarcopenic: 24(m); 56 (f) WBV(L) = 20 WBV(M) = 20 WBV(H) = 20 CON = 20 | WBV(L): 78 (4) WBV(M): 75 (6) WBV(H): 74 (5) CON: 76 (6) | 12 weeks 3× week WBV(L): 12 min, MC: ≈ 432 min WBV(M): 6 min, MC: ≈ 216 min WBV(H): 4 min, MC: ≈ 144 min | WBV(L): 20 Hz, 4 mm, 3.2 g WBV(M): 40 Hz, 4 mm, 12.9 g WBV(H): 60 Hz, 4 mm, 29.0 g Synchronous | Semi-flexed knees | - | Unreported | Muscle strength: isometric strength (90°) and peak torque of knee extensors (60°/s and 180°/s) Muscle power: 5TSTS | WBV(M): improved (vs. CON) for peak torque of knee extensors (180°/s) and 5TSTS | No adverse event | Adherence: 87.5% Compliance: unreported |
| Smith et al., 2016 [11] USA | 60 institutionalized/healthy: 24(m); 36(f) WBV = 13 BD = 16 WBV + BD = 17 CON = 14 | WBV: 82.2 ± 5.0 BD: 80.5 ± 6.2 WBV + BD: 83.4 ± 5.0 CON: 81.7 ± 5.7 | 12 weeks 2× week 3 min MC: ≈ 72 min | 30 Hz; 2 mm; 3.6 g * Synchronous | Unipodal support with semi-flexed knees | BD: Muscle strengthening in bioDensity equipment (5 min, 1× week) | Usual routine | Muscle strength: chest press, leg press, core pull and vertical lift | WBV + BD: improved for chest press, leg press (vs. CON and WBV), and vertical lift (vs. CON) BD: improved for chest press, leg press (vs. WBV), and vertical lift (vs. CON) | Unreported | Adherence: 82.2% Compliance: unreported |
| Tseng et al., 2016 [12] Taiwan | 45 community/healthy: 22(m); 23(f) WBV = 14 WBV(F) = 17 CON = 14 | All: 69.2 ± 3.9 WBV: 67.2 ± 2.3 WBV(F): 71.4 ± 5.0 CON: 68.6 ± 2.5 | Three months 3× week 3 × 2 min (6 min total) MC: ≈ 144 min | 20 Hz; 4 mm; 3.2 g * Side-alternating | Semi-flexed knees | - | Usual routine | Muscle strength: peak torque of knee extensors and flexors (60°/s) | WBV and WBV(F): improved (vs. CON) for peak torque of knee extensors WBV(F): improved (vs. CON) for peak torque of knee flexors | Unreported | Adherence: 100% Compliance: unreported |
| Casimiro et al., 2015 [13] Brazil | 21 community/healthy: 0(m); 21 (f) WBV + SBT = 10 SBT = 11 | WBV + SBT: 77.5 ± 4.2 SBT: 74.7 ± 3.2 | 12 weeks 3× week 30 min MC: ≈ 1080 min | 35–40 Hz; 2–4 mm; 4.9–12.9 g * Side-alternating | Postural balance exercises and lower limb strengthening | SBT: Postural balance exercises and lower limb strengthening (30 min, 3× week) | - | Muscle strength: handgrip | No difference | Unreported | Adherence: WBV + SBT (83.3%); SBT (91.7%) Compliance: unreported |
| Corrie et al., 2015 [14] UK | 61 community/risk of falls: 24(m); 37(f) WBV(V) = 21 WBV(S) = 20 SHAM = 20 | WBV(V): 81.9 ± 5.7 WBV(S): 79.5 ± 5.7 SHAM: 79.1 ± 7.8 | 12 weeks 3× week 2 × 30 s (1 min total)–6 × 1 min (6 min total) MC: ≈ 180 min | WBV(V): 28.4 Hz; 1.3 mm; 1.5 g; Synchronous WBV(S): 29.8 Hz; 2.9 mm; 3.6 g; Side-alternating | Semi-flexed knees | - | WBV Sham | Muscle power: 5TSTS, CMJ and power of knee extensors | WBV(V): improved (vs. SHAM) for the power of knee extensors | WVB(V) (14.3%) and WBV(S) (5%): injuries from a fall, deterioration of pre-existing arthritis, oedema and backache | Adherence: 83.6% Compliance: WBV(V): 63.4% WBV(S): 75% SHAM: 80.5% |
| Santin-Medeiros et al., 2015 [15] Spain | 37 institutionalized/healthy: 0(m); 37(f) WBV = 19 CON = 18 | All: 82.4 ± 5.7 | 8 months 2× week 2 × 3 min (6 min total)s MC: ≈ 420 min | 20 Hz; 2 mm; 1.6 g * Synchronous | Strengthening exercises for lower limbs | - | Usual routine | Muscle strength: handgrip Muscular endurance: 30-s Sit to Stand and 30-s Arm Curl | CON: improved (vs. WBV) for 30-s Sit to Stand | Unreported | Adherence: 76% Compliance: unreported |
| Sitjà-Rabert et al. 2015 [16] Spain | 159 institutionalized/low functionality: 52(m); 107(f) WBV + CT = 81 CT = 78 | WBV + CT: 82.3 ± 7.8 CT: 82.6 ± 7.1 | Six weeks 3× week 3–6 min MC: ≈ 81 min | 30–35 Hz; 2–4 mm; 3.6–9.8 g * Synchronous | Strengthening exercises for lower limbs | CT: balance and strength training (30 min; 3× week) | - | Muscle power: 5TSTS | No difference | WBV: pain, itching, erythema and edema (16.3%) CT: pain, itching, erythema and edema (10%) | Adherence: WBV + CT: 82.7% CT: 82.1% Compliance: WBV + CT and CT: >75% |
| Álvarez-Barbosa et al., 2014 [17] Spain | 29 institutionalized/healthy: 5(m); 24(f) WBV = 14 CON = 15 | WBV: 84.0 ± 3.0 CON: 86.0 ± 7.5 | 8 weeks 3× week 12.3–17.1 min MC: ≈ 348 min | 30–35 Hz; 4 mm; 7.2–9.8 g * Synchronous | Strengthening exercises for lower limbs | - | Usual nursing home care | Muscular endurance: 30-s Sit to Stand | WBV: improved (vs. CON) for 30-s Sit to Stand | No adverse event | Adherence: 73.3% (WBV); 78.6 (CON) Compliance: unreported |
| Leung et al., 2014 [18] China | 596 community/healthy: 0(m); 596(f) WBV = 280 CON = 316 | WBV: 74.5 ± 7.1 CON: 71.3 ± 7.2 | 18 months 5× week 20 min MC: ≈ 7800 min | 35 Hz; <0.1 mm; 0.3 g Synchronous | Extended knees | - | Usual routine | Muscle strength: knee extensors | WBV: improved (vs. CON) for knee extensors | WBV: pain (2.7%), dizziness (1.4%) and hypertension (2.2%) CON: pain (3.8%), dizziness (0.3%), hypertension (4.3%) and depression (1.2%) | Adherence: 76.9% (WBV); 91.3% (CON) Compliance: 66% |
| Osugi et al., 2014 [19] Japan | 28 ambulatory/osteoarthritis and/or spondylosis: WBV = 14 WBV + ST = 14 | WBV: 72.5 ± 4.6 WBV + ST: 72.3 ± 6.5 | Six months 2× week 4 min MC: ≈ 208 min | 20 Hz; displacement or magnitude not reported Side-alternating | Semi-flexed knees | WBV + ST: WBV plus squat training (4 min; 2× week) | - | Muscle power: 5TSTS | WBV + ST: improved (vs. WBV) for 5TSTS | No adverse event | Adherence: 80% Compliance: 100% |
| Sievänen et al., 2014 [20] Finland | 15 institutionalized /low functionality: 3(m); 12(f) WBV = 8 SHAM = 7 | All: 84.0 ± 7.4 WBV: 84.4 ± 6.3 SHAM: 83.6 ± 8.9 | 10 weeks 2× week 1–5 min MC: ≈ 80 min | 12–18 Hz; 2–8 mm; 0.6–5.2 g *; Side-alternating | Strengthening exercises for lower limbs | - | WBV Sham plus strengthening exercises for lower limbs | Muscle strength: handgrip | No difference | Unreported | Adherence: WBV: 87.5% SHAM: 85.7% Compliance: WBV: 74% SHAM: 73% |
| Zhang et al., 2014 [21] China | 37 ambulatory/frail: 32(m); 5(f) WBV = 19 CON = 18 | All: 85.3 ± 3.6 WBV: 85.8 ± 3.6 CON: 84.7 ± 3.7 | 8 weeks 3–5× week 4–5 min MC: ≈ 144 min | 6–26 Hz; 1–3 mm; 0.1–4.1 g *; Side-alternating | Semi-flexed knees | - | Usual care, physical therapy and routine exercises (8 weeks) | Muscle strength: knee extensors Muscular endurance: 30-s Sit to Stand | WBV: improved (vs. CON) for knee extensors | No adverse event | Adherence: WBV: 86.4% CON: 81.8% Compliance: unreported |
| Calder et al., 2013 [22] New Zealand | 41 institutionalized/healthy: 11(m); 30(f) WBV + PT = Unreported PT = Unreported | All: 80.1 | Six weeks 3× week 4 × 75 s (5 min total) MC: ≈ 90 min | 20 Hz; 2 mm; 1.6 g * Side-alternating | Semi-flexed knees | PT: physical therapy program | - | Muscle power: 5TSTS | No difference | Unreported | Adherence: 92.7% Compliance: unreported |
| Dudoniene et al., 2013 [23] Lithuania | 40 community/healthy: 0(m); 40(f) WBV + CT = 20 CT = 20 | All: 67.7 ± 4.1 | 8 weeks 3× week 5 × 15–30 min (2 min total) MC: ≈ 48 min | 27 Hz; 3 mm; 4.4 g * Synchronous | Strengthening exercises for lower limbs | CT: strengthening, flexibility, postural control, balance and endurance exercises (50 min; 2× week) | - | Muscular endurance: 30-s Sit to Stand | No difference | Unreported | Adherence: 100% (WBV and CON) Compliance: unreported |
| Gómez-Cabello et al., 2013 [24] Spain | 49 community/healthy: 20(m); 29(f) WBV = 24 CON = 25 | All: 75.0 ± 4.7 | 11 weeks 3× week 10 × 45 min (7 min 30 s total) MC: ≈ 248 min | 40 Hz; 2 mm; 6.4 g Synchronous | Strengthening exercises for lower limbs | - | Usual routine | Muscular endurance: 30-s Sit to Stand and 30-s Arm Curl | No difference | No adverse event | Adherence: 100% (WBV and CON) Compliance: 90.2% |
| Von Stengel et al., 2012 [25] Germany | 141 community/healthy: 0(m); 141 (f) WBV + CT = 46 CT = 47 CON = 48 | WBV + CT: 68.8 ± 3.6 CT: 68.6 ± 3.0 CON: 68.1 ± 2.7 | 18 months 2× week 6 min MC: ≈ 936 min | 25–35 Hz; 1.7–2.0 mm; 2.1–4.9 g * Synchronous | Strengthening exercises for lower limbs | CT: aerobic dance, functional strength training coordination and balance (60 min; 2× week) | Light physical exercise and relaxation | Muscle strength: lower limb (leg press), trunk flexion and extensionMuscle power: CMJ | WBV + CT: improved (vs. CON) for lower limb, trunk flexion and extension CT: improved (vs. CON) for trunk extension | No adverse event | Adherence: WBV + CT (86%); CT (90%); CON (92%) Compliance: >75% |
| Marin et al., 2011 [26] Spain | 34 community/healthy: (16)m; 18(f) WBV(2) = 11 WBV(4) = 12 CON = 11 | All: 84.3 ± 7.4 | 8 weeks WBV(2): 2× week WBV(4): 4× week 4 × 30 s (2 min total)–8 × 30 s (4 min total) MC WBV(2): ≈ 52 min MC WBV(4): ≈ 104 min | 35–40 Hz; 1.1–2.1 mm; 2.1–6.5 g Synchronous | Strengthening exercises for lower limbs | - | Usual routine | Muscular endurance: 30-s Sit to Stand | No difference | No adverse event | Adherence: WBV(2) (91%); WBV(4) (91%); CON (83%) Compliance: unreported |
| Verschueren et al., 2011 [27] Belgium | 111 institutionalized/healthy: 0(m); 111(f) WBV (NS) = 28 WBV (AS) = 26 CON (NS) = 28 CON (AS) = 29 | WBV (NS): 79.8 ± 5.3 WBV (AS): 80.3 ± 5.3 CON (NS): 79.6 ± 5.2 CON (AS): 78.7 ± 5.6 | Six months 3× week 1 s–12 min MC: ≈ 507 min | 30–40 Hz; 1.6–2.2 g Synchronous | Strengthening exercises for lower limbs | - | Usual routine | Muscle strength: knee extensors (isometric and dynamic) | No difference | No adverse event | Adherence: WBV (NS) (86%); WBV (AS) (93%); CON (NS) (93%); CON (AS) (93%) Compliance: >90% |
| Von Stengel et al., 2011 [28] Germany | 96 community/healthy: 0(m); 96(f) WBV(V) = 34 WBV(S) = 36 CON = 36 | WBV(V): 68.1 ± 4.0 WBV(S): 67.9 ± 3.8 CON: 67.6 ± 4.1 | 12 months 3× week 15 min MC: ≈ 540 min | WBV(V): 35 Hz; 1.7 mm; 8 g Synchronous WBV(S): 12.5 Hz; 12 mm; 8 g Side-alternating | Strengthening exercises for lower limbs | - | Light physical exercise and relaxation | Muscle strength: lower limb isometry (leg press dynamometer) Muscle power: CMJ | WBV(V) and WBV(S): improved (vs. CON) for lower limb isometry | No adverse event | Adherence: WBV(V) (94%); WBV(S) (81%); CON (92%) Compliance: WBV(V) (73%); WBV(S) (68%); CON (71%) |
| Machado et al., 2010 [29] Spain | 26 community/healthy: 0(m); 26(f) WBV = 13 CON = 13 | WBV: 79.3 ± 7.3 CON: 76.2 ± 8.4 | 10 weeks 3–5× week 3 × 30 min (1 min 30 s total)–8 × 1 min (8 min total) MC: ≈ 174 min | 20–40 Hz; 2–4 mm; 1.6–9.8 g * Synchronous | Strengthening exercises for lower limbs | - | Usual routine | Muscle strength: lower limb (leg press) Muscle power: lower limb (leg press) | No difference | No adverse event | Adherence: WBV (87%); CON (93%) Compliance: 95% |
| Bogaerts et al., 2009 [30] Belgium | 214 community/healthy: 114(m); 106(f) WBV = 94 CT = 60 CON = 66 | All: 67.1 WBV = 66.8 CT = 66.8 CON = 67.8 (SD not reported) | 12 months 3× week 4 × 30 s (2 min total)–15 × 60 s (15 min total) MC: ≈ 1248 min | 35–40 Hz; 2.5–5 mm; 6.2–16.1 g * Synchronous | Strengthening exercises for upper and lower limbs | CT: cardiovascular, resistance, balance and flexibility exercises (60 min–90 min; 3× week) | Usual routine | Muscle strength: isometric strength (120°) of knee extensors | WBV and CT: improved (vs. CON) for isometric strength (120°) of knee extensors | No adverse event | Adherence: WBV (74%); CT (82%); CON (92%) Compliance: WBV (88%); CT (86%) |
| Furness et al., 2009 [31] Australia | 73 community/healthy: 35(m); 38(f) WBV(1) = 18 WBV(2) = 18 WBV(3) = 19 CON = 18 | All: 72 ± 8 | Six weeks5 × 1 min (5 min total) WBV(1): 1× week; MC: ≈ 30 min WBV(2): 2× week; MC: ≈ 60 s WBV(3): 3× week; MC: ≈ 90 min | 15–25 Hz; 0.5 mm; 0.45–1.26 g Side-alternating | Semi-flexed knees | - | Usual routine | Muscle power: 5TSTS | WBV(3): improved (vs. CON) for 5TSTS | Unreported | Adherence: unreported Compliance: 100% |
| Bogaerts et al., 2007 [32] Belgium | 82 community/healthy: 82(m); 0(f) WBV = 25 CT = 25 CON = 32 | WBV: 66.9 ± 0.7 CT: 67.6 ± 0.9 CON: 68.6 ± 1.0 | 12 months 3× week 4 × 30 s (2 min total)–15 × 60 s (15 min total) MC: ≈ 1248 min | 35–40 Hz; 2.5–5 mm; 6.2–16.1 g * Synchronous | Strengthening exercises for lower limbs | CT: cardiovascular, resistance, balance, and flexibility exercises (90 min, 3× week) | Usual routine | Muscle strength: isometric strength (120°) of knee extensors Muscle power: CMJ | WBV and CT: improved (vs. CON) for isometric strength (120°) of knee extensors and CMJ | No adverse event | Adherence: WBV (81%); CT (83%); CON (89%) Compliance: WBV (88%); CT (87%) |
| Rees et al., 2007 [33] Australia | 43 community/healthy: 23(m); 20(f) WBV + EX = 15 EX = 13 CON = 15 | WBV + EX: 74.3 ± 5.0 EX: 73.1 ± 4.1 CON: 73.1 ± 4.6 | 8 weeks 3× week 6 × 45 s (4 min 30 s total)–6 × 80 s (8 min total) MC: ≈ 150 min | 26 Hz; 5–8 mm; 6.8–10.9 g Side-alternating | Strengthening exercises for lower limbs | EX: Strengthening exercises for lower limbs–6 × 45 s (4 min 30 s total)–6 × 80 s (8 min total), 3× week | Unreported | Muscle strength: peak torque of knee, hip (60°/s) and ankle (30°/s) extensors and flexors Muscle power: 5TSTS | WBV + EX and EX: improved (vs. CON) for peak torque of knee extension and 5TSTS WBV + EX: improved (vs. EX and CON) for peak torque of ankle plantar-flexor | Unreported | Adherence: WBV + EX and EX (100%); EX (87%); CON (100%) Compliance: WBV + EX and EX (99%) |
| Bautmans et al., 2005 [34] Belgium | 24 institutionalized/low functionality: 9(m); 15(f) WBV = 13 SHAM = 11 | All: 77.5 ± 11.0 WBV: 76.6 ± 11.8 SHAM: 78.6 ± 10.4 | Six weeks 3× week 2 × 30 s (1 min total)–4 × 1 min (4 min total) MC: ≈ 36 min | 35–40 Hz; 2–5 mm; 4.9–16.1 g Synchronous | Strengthening exercises for lower limbs | - | WBV Sham: Strengthening exercises for lower limbs | Muscle strength: handgrip, leg extension Muscular endurance: 30-s Sit to Stand | No difference | WBV: groin pain (8%) and airway infection (8%) | Adherence: WBV (77%); SHAM (100%) Compliance: WBV (96%); SHAM (86%) |
| Runge et al., 2000 [35] Germany | 34 community/healthy: 23(m); 11(f) WBV = 17 CON = 17 | All: 67 (61–85) | Two months 3× week 5 min MC: ≈ 144 min | 27 Hz; 7–14 mm; 10.3–20.5 g * Side-alternating | Semi-flexed knees | - | Unreported | Muscle power: 5TSTS | No difference | WBV: inflammation in the forefoot (6%) | Adherence: 87.2% Compliance: unreported |
| Author | Eligibility Criteria | Random Allocation | Concealed Allocation | Baseline Comparability | Blind Subjects | Blind Therapists | Blind Assessor | Follow-Up Dropout <15% | Intention-to-Treat Analysis | Between-Group Comparisons | Point Estimates and Variability | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Genest et al., 2021 [1] | No | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Camacho-Cardenosa et al., 2019 [2] | Yes | Yes | No | No | No | No | Yes | No | No | Yes | Yes | 4 |
| Zhu et al., 2019 [3] | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Lam et al., 2018 [4] | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7 |
| Pessoa et al., 2018 [5] | No | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | 7 |
| Goudarzian et al., 2017 [6] | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Goudarzian et al., 2017 [7] | Yes | Yes | No | Yes | No | No | Yes | No | No | Yes | Yes | 5 |
| Han et al., 2017 [8] | No | Yes | No | No | No | No | No | No | No | Yes | Yes | 3 |
| Wei et al., 2017 [9,10] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6 |
| Smith et al., 2016 [11] | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Tseng et al., 2016 [12] | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Casimiro et al., 2015 [13] | Yes | Yes | No | Yes | No | No | Yes | Yes | No | Yes | Yes | 6 |
| Corrie et al., 2015 [14] | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Santin-Medeiros et al., 2015 [15] | Yes | Yes | No | No | No | No | No | Yes | No | Yes | Yes | 4 |
| Sitja-Rabert et al., 2015 [16] | Yes | Yes | Yes | Yes | No | No | Yes | No | Yes | Yes | Yes | 7 |
| Álvarez-Barbosa et al., 2014 [17] | Yes | Yes | No | Yes | No | No | No | No | Yes | Yes | Yes | 5 |
| Leung et al., 2014 [18] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Osugi et al., 2014 [19] | Yes | Yes | No | Yes | No | No | No | No | No | Yes | Yes | 4 |
| Sievänen et al., 2014 [20] | Yes | No | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7 |
| Zhang et al., 2014 [21] | Yes | Yes | Yes | Yes | No | No | Yes | No | Yes | Yes | Yes | 7 |
| Calder et al., 2013 [22] | No | Yes | No | No | No | No | Yes | Yes | No | Yes | Yes | 5 |
| Dudoniene et al., 2013 [23] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6 |
| Gómez-Cabello et el., 2013 [24] | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Von Stengel et al., 2012 [25] | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7 |
| Marin et al., 2011 [26] | No | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Verschueren et al. 2011 [27] | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7 |
| Von Stengel et al., 2011 [28] | Yes | Yes | No | Yes | No | No | Yes | Yes | No | Yes | Yes | 6 |
| Machado et al., 2010 [29] | Yes | Yes | No | No | No | No | Yes | Yes | No | Yes | Yes | 5 |
| Bogaerts et al., 2009 [30] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6 |
| Furness et al., 2009 [31] | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Bogaerts et al., 2007 [32] | No | Yes | No | Yes | No | No | No | No | No | Yes | Yes | 4 |
| Rees et al., 2007 [33] | No | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Bautmans et al., 2005 [34] | Yes | Yes | No | Yes | Yes | No | Yes | Yes | No | Yes | Yes | 7 |
| Runge et al., 2000 [35] | Yes | Yes | No | No | No | No | No | Yes | No | No | No | 2 |
| Measurements | Std. Mean Difference | 95% CI | n | Studies | I2 | p | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Muscle Strength | |||||||
| Knee extensors | 0.53 | 0.32 | 0.74 | 937 | 9 | 30% | <0.00001 |
| Knee flexors | 0.64 | 0.31 | 0.96 | 161 | 4 | 0% | 0.0002 |
| Leg extensors | 0.68 | 0.17 | 1.20 | 209 | 3 | 62% | 0.009 |
| Ankle plantar-flexors | 0.65 | 0.12 | 1.18 | 61 | 2 | 0% | 0.02 |
| Ankle dorciflexors | 0.31 | −0.43 | 1.05 | 85 | 2 | 63% | 0.41 |
| Hip flexors | 0.17 | −0.26 | 0.59 | 85 | 2 | 0% | 0.44 |
| Handgrip | 0.13 | −0.31 | 0.57 | 184 | 7 | 50% | 0.55 |
| Muscle Power | |||||||
| Five-times-sit-to-stand | −0.31 | −0.63 | 0.02 | 386 | 6 | 50% | 0.07 |
| Countermovement jump | 0.17 | −0.12 | 0.47 | 189 | 2 | 0% | 0.24 |
| Muscle endurance | |||||||
| 30-s sit-to-stand | 0.10 | −0.19 | 0.39 | 184 | 5 | 42% | 0.51 |
| 30-s arm curl | 0.01 | −0.87 | 0.90 | 86 | 2 | 76% | 0.97 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonçalves de Oliveira, R.; Coutinho, H.M.E.L.; Martins, M.N.M.; Bernardo-Filho, M.; de Sá-Caputo, D.d.C.; Campos de Oliveira, L.; Taiar, R. Impacts of Whole-Body Vibration on Muscle Strength, Power, and Endurance in Older Adults: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 4467. https://doi.org/10.3390/jcm12134467
Gonçalves de Oliveira R, Coutinho HMEL, Martins MNM, Bernardo-Filho M, de Sá-Caputo DdC, Campos de Oliveira L, Taiar R. Impacts of Whole-Body Vibration on Muscle Strength, Power, and Endurance in Older Adults: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(13):4467. https://doi.org/10.3390/jcm12134467
Chicago/Turabian StyleGonçalves de Oliveira, Raphael, Heloísa Maria Elaine Licha Coutinho, Maiara Naldi Mansano Martins, Mario Bernardo-Filho, Danúbia da Cunha de Sá-Caputo, Laís Campos de Oliveira, and Redha Taiar. 2023. "Impacts of Whole-Body Vibration on Muscle Strength, Power, and Endurance in Older Adults: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 13: 4467. https://doi.org/10.3390/jcm12134467
APA StyleGonçalves de Oliveira, R., Coutinho, H. M. E. L., Martins, M. N. M., Bernardo-Filho, M., de Sá-Caputo, D. d. C., Campos de Oliveira, L., & Taiar, R. (2023). Impacts of Whole-Body Vibration on Muscle Strength, Power, and Endurance in Older Adults: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(13), 4467. https://doi.org/10.3390/jcm12134467