
Benralizumab in Patients with Severe Eosinophilic Asthma: A Multicentre Real-Life Experience

 , ,
, ,  ,
,  , , ,
, , ,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Study Population at Baseline
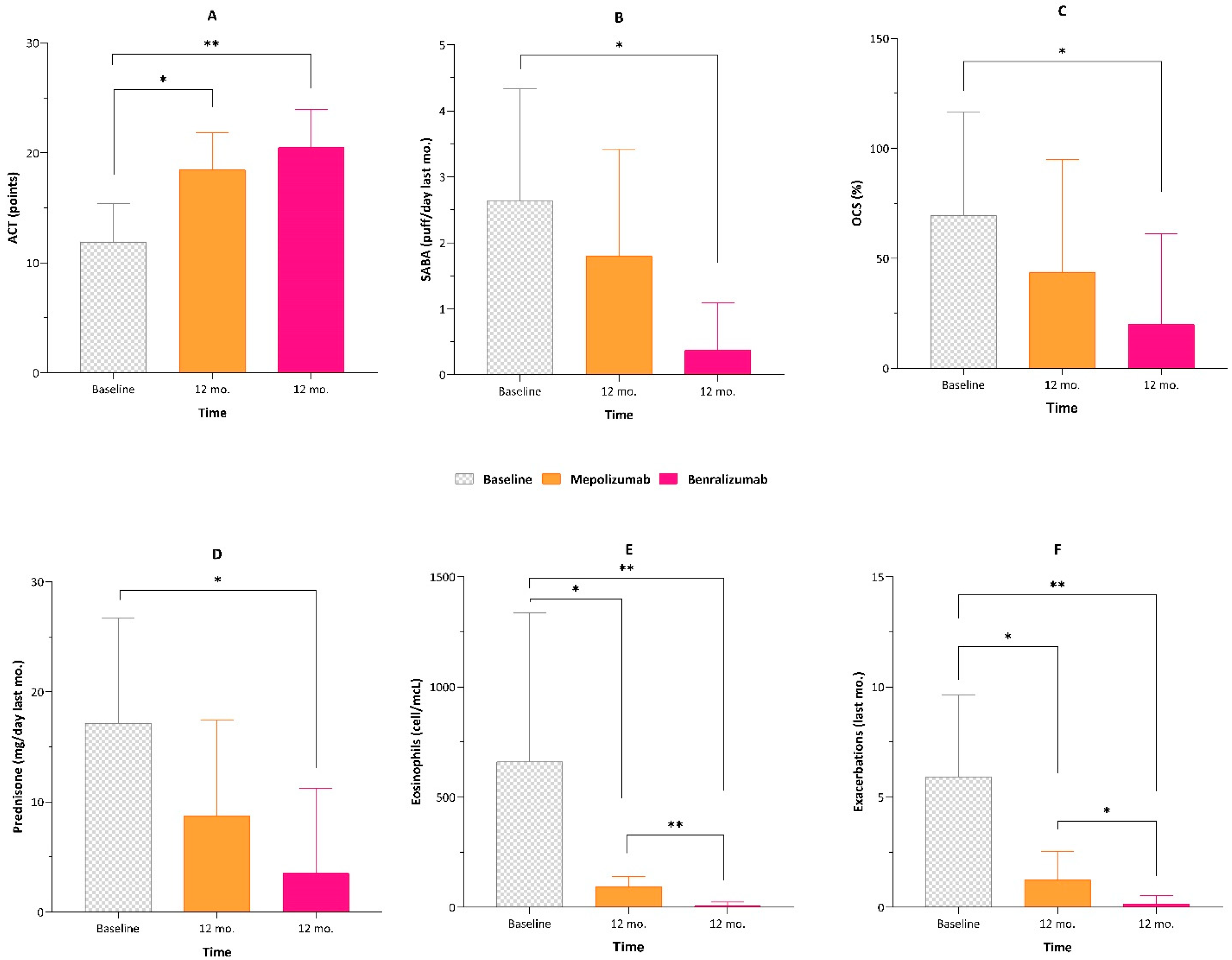
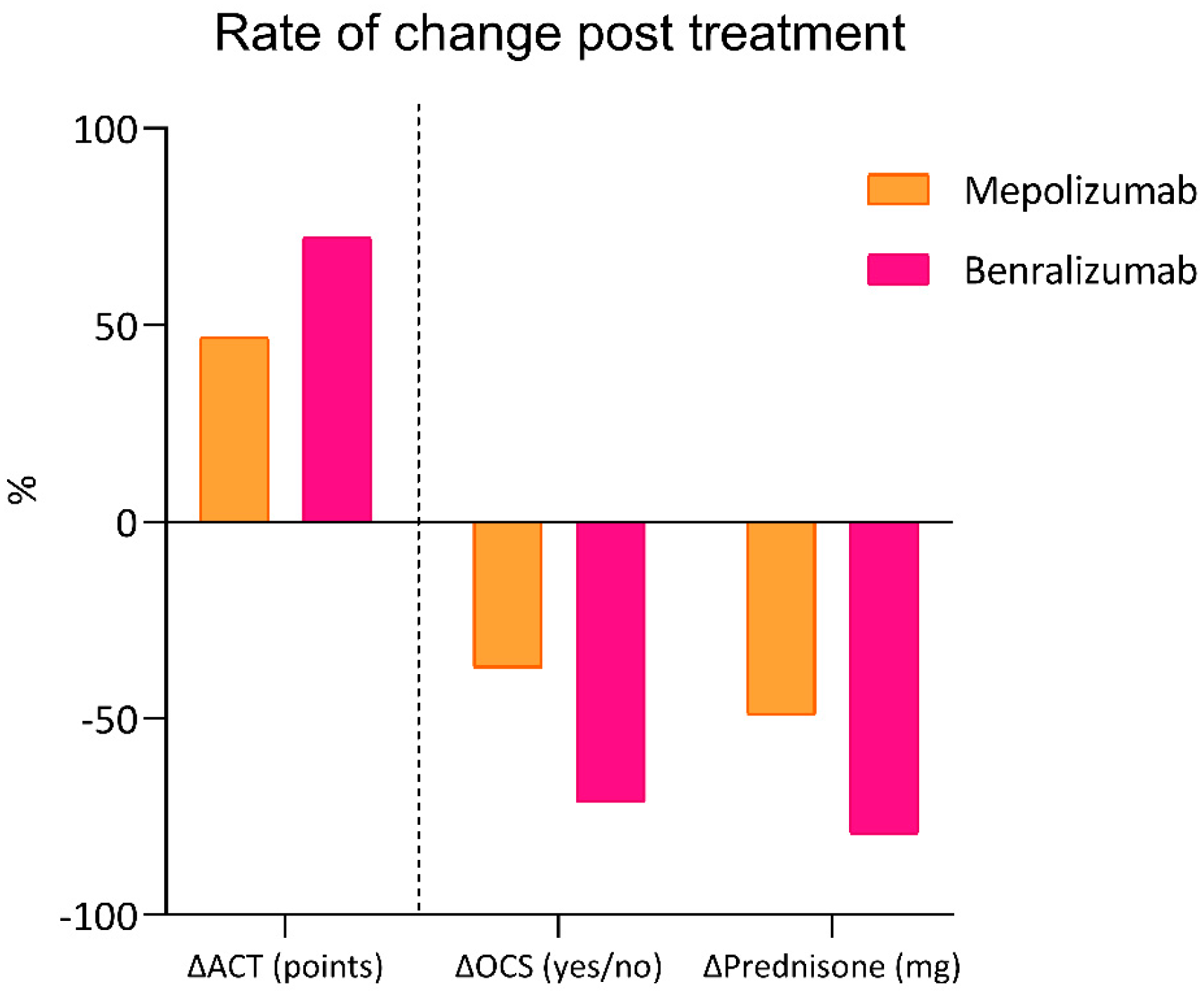
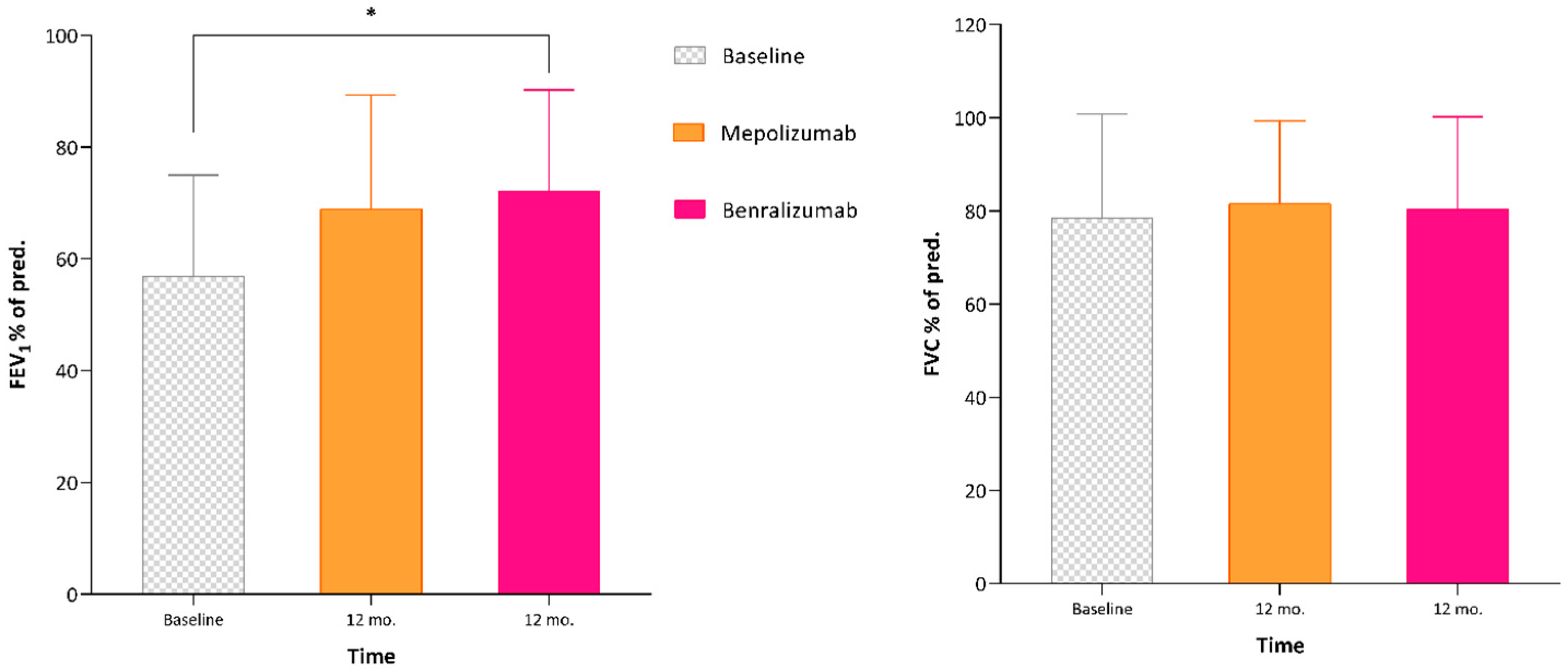
3.2. Effectiveness of Mepolizumab and Benralizumab at 6 and 12 Months
3.3. Effectiveness of Mepolizumab and Benralizumab in Patients with SEA and CRSwNP
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mims, J.W. Asthma: Definitions and pathophysiology. Int. Forum Allergy Rhinol. 2015, 5 (Suppl. S1), S2–S6. [Google Scholar] [CrossRef]
- Lai, C.K.; Beasley, R.; Crane, J.; Foliaki, S.; Shah, J.; Weiland, S.; International Study of Asthma and Allergies in Childhood Phase Three Study Group. Global variation in the prevalence and severity of asthma symptoms: Phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 2009, 64, 476–483. [Google Scholar] [CrossRef]
- Bagnasco, D.; Paggiaro, P.; Latorre, M.; Folli, C.; Testino, E.; Bassi, A.; Milanese, M.; Heffler, E.; Manfredi, A.; Riccio, A.M.; et al. Severe asthma: One disease and multiple definitions. World Allergy Organ J. 2021, 14, 100606. [Google Scholar] [CrossRef] [PubMed]
- McGregor, M.C.; Krings, J.G.; Nair, P.; Castro, M. Role of Biologics in Asthma. Am. J. Respir. Crit. Care Med. 2019, 199, 433–445. [Google Scholar] [CrossRef] [PubMed]
- Agache, I.; Beltran, J.; Akdis, C.; Akdis, M.; Canelo-Aybar, C.; Canonica, G.W.; Casale, T.; Chivato, T.; Corren, J.; Del Giacco, S.; et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines—Recommendations on the use of biologicals in severe asthma. Allergy 2020, 75, 1023–1042. [Google Scholar] [CrossRef] [PubMed]
- Heaney, L.G.; Perez de Llano, L.; Al-Ahmad, M.; Backer, V.; Busby, J.; Canonica, G.W.; Christoff, G.C.; Cosio, B.G.; FitzGerald, J.M.; Heffler, E.; et al. Eosinophilic and Noneosinophilic Asthma: An Expert Consensus Framework to Characterize Phenotypes in a Global Real-Life Severe Asthma Cohort. Chest 2021, 160, 814–830. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Bastero Fernández, A.; Medina Gallardo, J.F.; Delgado Romero, J.; Romero Falcón, A.; Benito Bernáldez, C.; Gallego Borrego, J.; Álvarez-Gutiérrez, F.J. Effectiveness of Switching to Benralizumab in Severe Refractory Eosinophilic Asthma. J. Asthma Allergy 2022, 15, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Carpagnano, G.E.; Pelaia, C.; D’Amato, M.; Crimi, N.; Scichilone, N.; Scioscia, G.; Resta, O.; Calabrese, C.; Pelaia, G.; Quarato, C.M.I.; et al. Switching from omalizumab to mepolizumab: Real-life experience from Southern Italy. Ther. Adv. Respir. Dis. 2020, 14, 1753466620929231. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Resta, E.; Povero, M.; Pelaia, C.; D’Amato, M.; Crimi, N.; Scichilone, N.; Scioscia, G.; Resta, O.; Calabrese, C.; et al. Clinical and economic consequences of switching from omalizumab to mepolizumab in uncontrolled severe eosinophilic asthma. Sci. Rep. 2021, 11, 5453. [Google Scholar] [CrossRef]
- Numata, T.; Araya, J.; Miyagawa, H.; Okuda, K.; Fujita, Y.; Utsumi, H.; Takekoshi, D.; Hashimoto, M.; Minagawa, S.; Ishikawa, T.; et al. Effectiveness of Switching Biologics for Severe Asthma Patients in Japan: A Single-Center Retrospective Study. J. Asthma Allergy 2021, 14, 609–618. [Google Scholar] [CrossRef]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 43, 343–373, Erratum in Eur. Respir. J. 2014, 43, 1216; Erratum in Eur. Respir. J. 2018, 52, 1352020; Erratum in Eur. Respir. J. 2022, 59, 1362020. [Google Scholar] [CrossRef]
- Thomas, D.; McDonald, V.M.; Pavord, I.D.; Gibson, P.G. Asthma remission: What is it and how can it be achieved? Eur. Respir. J. 2022, 60, 2102583. [Google Scholar] [CrossRef]
- Bonini, M.; Di Paolo, M.; Bagnasco, D.; Baiardini, I.; Braido, F.; Caminati, M.; Carpagnano, E.; Contoli, M.; Corsico, A.; Del Giacco, S.; et al. Minimal clinically important difference for asthma endpoints: An expert consensus report. Eur. Respir. Rev. 2020, 29, 190137. [Google Scholar] [CrossRef]
- Farne, H.A.; Wilson, A.; Powell, C.; Bax, L.; Milan, S.J. Anti-IL5 therapies for asthma. Cochrane Database Syst. Rev. 2017, 9, CD010834. [Google Scholar] [CrossRef]
- Menzella, F.; Facciolongo, N.; Castagnetti, C.; Simonazzi, A.; Zucchi, L. Omalizumab: When the non-responder is a late-responder. Eur. Ann. Allergy Clin. Immunol. 2009, 41, 155–159. [Google Scholar]
- Pelaia, C.; Busceti, M.T.; Vatrella, A.; Rago, G.F.; Crimi, C.; Terracciano, R.; Pelaia, G. Real-life rapidity of benralizumab effects in patients with severe allergic eosinophilic asthma: Assessment of blood eosinophils, symptom control, lung function and oral corticosteroid intake after the first drug dose. Pulm. Pharmacol. Ther. 2019, 58, 101830. [Google Scholar] [CrossRef]
- Isoyama, S.; Ishikawa, N.; Hamai, K.; Matsumura, M.; Kobayashi, H.; Nomura, A.; Ueno, S.; Tanimoto, T.; Maeda, H.; Iwamoto, H.; et al. Switching Treatment from Mepolizumab to Benralizumab for Elderly Patients with Severe Eosinophilic Asthma: A Retrospective Observational Study. Intern. Med. 2022, 61, 1663–1671. [Google Scholar] [CrossRef]
- Scioscia, G.; Carpagnano, G.E.; Quarato, C.M.I.; Lacedonia, D.; Santamaria, S.; Soccio, P.; Depalo, A.; Fuso, P.; Foschino Barbaro, M.P. Effectiveness of Benralizumab in Improving the Quality of Life of Severe Eosinophilic Asthmatic Patients: Our Real-Life Experience. Front. Pharmacol. 2021, 12, 631660. [Google Scholar] [CrossRef]
- Salter, B.; Lacy, P.; Mukherjee, M. Biologics in Asthma: A Molecular Perspective to Precision Medicine. Front. Pharmacol. 2022, 12, 793409. [Google Scholar] [CrossRef]
- Pelaia, C.; Crimi, C.; Benfante, A.; Caiaffa, M.F.; Calabrese, C.; Carpagnano, G.E.; Ciotta, D.; D’Amato, M.; Macchia, L.; Nolasco, S.; et al. Therapeutic Effects of Benralizumab Assessed in Patients with Severe Eosinophilic Asthma: Real-Life Evaluation Correlated with Allergic and Non-Allergic Phenotype Expression. J. Asthma Allergy 2021, 14, 163–173. [Google Scholar] [CrossRef]
- FitzGerald, J.M.; Bleecker, E.R.; Nair, P.; Korn, S.; Ohta, K.; Lommatzsch, M.; Ferguson, G.T.; Busse, W.W.; Barker, P.; Sproule, S.; et al. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2016, 388, 2128–2141. [Google Scholar] [CrossRef] [PubMed]
- Caruso, C.; Cameli, P.; Altieri, E.; Aliani, M.; Bracciale, P.; Brussino, L.; Caiaffa, M.F.; Canonica, G.W.; Centanni, S.; D’Amato, M.; et al. Switching from one biologic to benralizumab in patients with severe eosinophilic asthma: An ANANKE study post hoc analysis. Front. Med. 2022, 9, 950883. [Google Scholar] [CrossRef]
- Mansur, A.H. Effect of benralizumab in a patient with uncontrolled severe eosinophilic asthma and comorbid chronic rhinosinusitis with nasal polyps refractory to mepolizumab treatment. Respir. Med. Case Rep. 2021, 35, 101559. [Google Scholar] [CrossRef] [PubMed]
- Charles, D.; Shanley, J.; Temple, S.N.; Rattu, A.; Khaleva, E.; Roberts, G. Real-world efficacy of treatment with benralizumab, dupilumab, mepolizumab and reslizumab for severe asthma: A systematic review and meta-analysis. Clin. Exp. Allergy 2022, 52, 616–627. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.; Lipworth, B.J. Impact of Biologic Therapy on the Small Airways Asthma Phenotype. Lung 2022, 200, 691–696. [Google Scholar] [CrossRef]
- Kavanagh, J.E.; Hearn, A.P.; d’Ancona, G.; Dhariwal, J.; Roxas, C.; Green, L.; Thomson, L.; Fernandes, M.; Kent, B.D.; Nanzer, A.M.; et al. Benralizumab after sub-optimal response to mepolizumab in severe eosinophilic asthma. Allergy 2021, 76, 1890–1893. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (N = 25) |
|---|---|
| Demographic | |
| Age (years) | 56.76 ± 11.97 |
| Sex (% female) | 64% |
| BMI (kg/m2) | 26.23 ± 5.74 |
| Smoking (%) | 39% |
| Pack/years (no.) | 9.77 ± 6.29 |
| Medical history | |
| Asthma (years of onset) | 34.48 ± 17.60 |
| Asthma, familiar history (%) | 48% |
| Menopause (%) | 46% |
| Atopy (%) | 57% |
| ASA sensitivity (%) | 9% |
| EGPA (%) | 9% |
| Hives (%) | 9% |
| Dermatitis (%) | 9% |
| GERD (%) | 26% |
| OSAS (%) | 13% |
| Osteoporosis (%) | 22% |
| Anxiety/Depression (%) | 47% |
| Bronchiectasis (%) | 35% |
| CRSwNP | |
| CRSwNP (%) | 48% |
| Lund–Mackay score (points) | 8.00 ± 5.94 |
| SNOT-22 (points) | 51.33 ± 17.18 |
| VAS (points) | 8.67 ± 1.15 |
| Nasal Polyp Score (points) | 3.00 ± 2.65 |
| Recurrence (n°) | 1.44 ± 0.88 |
| Current therapy | |
| ICS/LABA (%) | 100% |
| LAMA (%) | 87% |
| SABA (puff/day last mo.) | 2.63 ± 1.71 |
| LTRA (%) | 57% |
| Azithromycin (%) | 17% |
| OCS (%) | 70% |
| Prednisone (mg/day last mo.) | 17.16 ± 9.52 |
| Immunotherapy (%) | 4% |
| Methotrexate (%) | 20% |
| Questionnaires | |
| ACT (points) | 11.91 ± 3.50 |
| ACQ (points) | 3.22 ± 1.58 |
| AQLQ (points) | 5.52 ± 0.69 |
| TAI (points) | 49.67 ± 0.58 |
| Pulmonary Function | |
| FEV1 (% of pred.) | 56.93 ± 18.07 |
| FEV1 pre (L) | 1.57 ± 0.60 |
| FVC (% of pred.) | 78.57 ± 22.27 |
| FVC pre (L) | 2.69 ± 1.07 |
| FEV1/FVC% | 60.97 ± 14.44 |
| FEF25–75 (% of pred.) | 26.16 ± 17.88 |
| Biomarkers | |
| FeNO (ppb) | 73.6 ± 45.1 |
| Eosinophils (cell/mcL) | 660.2 ± 675.7 |
| Basophils (cell/mcL) | 51.8 ± 24.5 |
| Neutrophils (cell/mcL) | 4815.1 ± 1415.2 |
| Total IgE (IU/mL) | 446.0 ± 653.49 |
| Exacerbations | |
| Exacerbations (no.) | 5.91 ± 3.73 |
| A&E (no. admission) | 0.91 ± 1.23 |
| Hospitalisation (no. admission) | 0.26 ± 0.45 |
| Variable | Population (N = 25) | Mepolizumab | Benralizumab | ||
|---|---|---|---|---|---|
| Timeline (mo.) | Baseline | 6 mo. | 12 mo. | 6 mo. | 12 mo. |
| Current therapy | |||||
| ICS/LABA (%) | 100% | 100% | 100% | 100% | 100% |
| LAMA (%) | 87% | 73% | 69% | 70% | 70% |
| SABA (puff/day last mo.) | 2.63 ± 1.71 | 1.50 ± 1.76 e | 1.80 ± 1.61 | 0.19 ± 0.40 c*,e | 0.38 ± 0.72 d*,f |
| LTRA (%) | 57% | 55% | 69% | 65% | 70% |
| Azithromycin (%) | 17% | 9% | 19% | 10% | 5% |
| Theophylline (%) | 13% | 9% | 13% | 10% | 10% |
| OCS (%) | 70% | 59% e | 44% | 15% c*,e | 20% d* |
| Prednisone (mg/day last mo.) | 17.16 ± 9.52 | 12.75 ± 9.62 e | 8.75 ± 8.66 b | 2.95 ± 5.14 c*,e | 3.54 ± 7.72 d* |
| Immunotherapy (%) | 4% | 0% | 0% | 0% | 0% |
| Questionnaires | |||||
| ACT (points) | 11.91 ± 3.50 | 16.77 ± 3.48 a*,e | 18.44 ± 3.39 b* | 20.24 ± 3.38 c*,e | 20.50 ± 3.45 d* |
| ACQ (points) | 3.22 ± 1.58 | 2.54 ± 0.99 e | 1.36 ± 1.15 b | 0.90 ± 0.97 c,e | 1.92 ± 2.15 |
| AQLQ (points) | 5.52 ± 0.69 | 4.50 ± 1.78 | 5.86 ± 0.77 | 7.00 ± 1.14 | 5.95 ± 0.89 |
| TAI (points) | 49.67 ± 0.58 | 49.67 ± 0.58 | 49.00 ± 1.32 | 50.00 ± 0.00 | 52.67 ± 2.31 |
| CRSwNP | |||||
| CRSwNP (%) | 48% | 69% | 73% | 75% | 75% |
| SNOT-22 (points) | 51.33 ± 17.18 | 31.00 ± 1.41 | 45.00 ± 8.28 | 20.67 ± 9.29 c | 38.80 ± 18.25 |
| Recurrence (no.) | 1.44 ± 0.88 | 0.50 ± 1.00 | 0.17 ± 0.41 b | 0.20 ± 0.45 | 0.25 ± 0.46 d |
| Pulmonary Function Test | |||||
| FEV1 (% of pred.) | 56.93 ± 18.07 | 58.36 ± 19.56 e | 69.00 ± 20.32 | 73.20 ± 16.52 c,e | 72.18 ± 18.06 d |
| FEV1 pre (L) | 1.57 ± 0.60 | 1.59 ± 0.64 e | 1.87 ± 0.70 | 2.13 ± 0.70 c,e | 2.14 ± 0.71 d |
| FVC (% of pred.) | 78.57 ± 22.27 | 76.33 ± 16.95 | 81.57 ± 17.74 | 81.27 ± 25.52 | 80.35 ± 19.88 |
| FVC pre (L) | 2.69 ± 1.07 | 2.53 ± 0.77 | 2.80 ± 0.87 | 10.40 ± 28.12 | 2.96 ± 0.96 |
| FEV1/FVC% | 60.97 ± 14.44 | 63.88 ± 17.75 | 67.35 ± 12.79 | 69.96 ± 15.24 | 69.66 ± 24.30 |
| FEF25–75 (% of pred.) | 26.16 ± 17.88 | 30.33 ± 19.87 | 34.18 ± 20.31 | 43.13 ± 23.94 c | 48.00 ± 23.94 d |
| Biomarkers | |||||
| FeNO (ppb) | 73.6 ± 45.1 | 49.24 ± 38.9 | 51.90 ± 46.59 | 34.45 ± 27.81 | 30.17 ± 16.51 |
| Eosinophils (cell/mcL) | 660.2 ± 675.7 | 116.22 ± 87.42 a,e* | 92.71 ± 46.32 b | 8.0 ± 30.98 c*,e* | 5.23 ± 18.86 d,f* |
| Basophils (cell/mcL) | 51.8 ± 24.5 | 11.75 ± 9.3 a* | 18.4 ± 12.36 b | 6.0 ± 6.35 c* | 5.63 ± 10.28 d* |
| Neutrophils (cell/mcL) | 4815.2 ± 1415.3 | 4150.3 ± 1031.36 | 4288.33 ± 1225.71 | 4520.0 ± 800.17 | 5112.0 ± 1500.24 |
| Exacerbations | |||||
| Exacerbation (no.) | 5.91 ± 3.73 | 1.18 ± 1.62 a*,e | 1.25 ± 1.29 b* | 0 c*,e | 0.15 ± 0.37 d*,f* |
| A&E (no. admission) | 0.91 ± 1.23 | 0.17 ± 0.51 a | 0.07 ± 0.26 b | 0 c | 0 d |
| Hospitalisation (no. admission) | 0.26 ± 0.45 | 0 a | 0.07 ± 0.26 | 0 c | 0 d |
| Variable | Group A (CRSwNP) | Group B (no CRSwNP) | p |
|---|---|---|---|
| N = 12 | N = 13 | ||
| Current therapy | |||
| ICS/LABA (%) | 100% | 100% | — |
| LAMA (%) | 100% | 75% | 0.082 |
| SABA (puff/day last mo.) | 2.78 ± 1.92 | 2.5 ± 1.58 | 0.708 |
| LTRA (%) | 55% | 58% | 0.863 |
| Azithromycin (%) | 27% | 8% | 0.251 |
| OCS (%) | 82% | 58% | 0.240 |
| Prednisone (mg/day last mo.) | 16.5 ± 11.07 | 18.11 ± 7.51 | 0.685 |
| Immunotherapy (%) | 0% | 8% | 0.350 |
| Questionnaires | |||
| ACT (points) | 12 ± 4.4 | 11.83 ± 2.76 | 0.914 |
| ACQ (points) | 2.48 ± 1.78 | 4.2 ± 0.4 | 0.004 |
| Pulmonary Function Test | |||
| FEV1 (% of pred.) | 64.09 ± 21.27 | 50.38 ± 11.98 | 0.067 |
| FEV1 pre (L) | 1.93 ± 0.6 | 1.24 ± 0.38 | 0.003 |
| FVC (% of pred.) | 88 ± 25.51 | 69.92 ± 15.15 | 0.049 |
| FVC pre (L) | 3.37 ± 1.15 | 2.07 ± 0.45 | 0.002 |
| FEV1/FVC% | 62.02 ± 16.02 | 60 ± 13.46 | 0.746 |
| FEF25–75 (% of pred.) | 33.25 ± 21.57 | 21 ± 13.44 | 0.144 |
| Biomarkers | |||
| FeNO (ppb) | 73.38 ± 46.84 | 74.33 ± 49.92 | 0.963 |
| Eosinophils (cell/mcL) | 513.56 ± 291.55 | 794.58 ± 891.52 | 0.331 |
| Basophils (cell/mcL) | 71.6 ± 21.74 | 35.33 ± 10.39 | <0.001 |
| Neutrophils (cell/mcL) | 4762.0 ± 1009.1 | 4868.33 ± 1838.88 | 0.867 |
| Total IgE (IU/mL) | 584.0 ± 878.58 | 308.01 ± 304.49 | 0.317 |
| Exacerbations | |||
| Exacerbation (no.) | 6.36 ± 4.72 | 5.5 ± 2.68 | 0.591 |
| A&E (no. admission) | 1.18 ± 1.47 | 0.64 ± 0.92 | 0.295 |
| Hospitalisation (no. admission) | 0.22 ± 0.44 | 0.3 ± 0.48 | 0.692 |
| Variable | Baseline | Mepolizumab | Benralizumab |
|---|---|---|---|
| Current therapy | |||
| ICS/LABA (%) | 100% | 100% | 100% |
| LAMA (%) | 100% | 75% | 73% |
| SABA (puff/day last mo.) | 2.78 ± 1.92 | 1.5 ± 1.69 | 0.22 ± 0.67 β |
| LTRA (%) | 55% | 75% | 73% |
| Azithromycin (%) | 27% | 13% | 9% |
| OCS (%) | 82% | 50% | 27% β |
| Prednisone (mg/day last mo.) | 16.5 ± 11.07 | 7.5 ± 5.92 | 4.17 ± 8.84 β |
| Questionnaires | |||
| ACT (points) | 12 ± 4.4 | 18.25 ± 3.54 α | 21.27 ± 3.2 β |
| ACQ (points) | 2.48 ± 1.78 | 1.02 ± 1.06 | 2.17 ± 2.57 |
| AQLQ (points) | 5.52 ± 0.69 | 5.86 ± 0.77 | 6.21 ± 0.88 |
| CRSwNP | |||
| SNOT-22 (points) | 51.33 ± 17.18 | 45 ± 8.28 | 38.8 ± 18.25 |
| Recurrence (no.) | 1.44 ± 0.88 | 0.17 ± 0.41 α | 0.29 ± 0.49 β |
| Pulmonary Function | |||
| FEV1 (% of pred.) | 64.09 ± 21.27 | 76.25 ± 22.94 | 78.36 ± 15.36 |
| FEV1 pre (L) | 1.93 ± 0.6 | 2.18 ± 0.69 | 2.39 ± 0.63 |
| FVC (% of pred.) | 88 ± 25.51 | 90.13 ± 16.79 | 89.45 ± 13.53 |
| FVC pre (L) | 3.37 ± 1.15 | 3.3 ± 0.68 | 3.28 ± 0.91 |
| FEV1/FVC% | 62.02 ± 16.02 | 65.61 ± 14.16 | 67.66 ± 29.22 |
| FEF25–75 (% of pred.) | 33.25 ± 21.57 | 33.6 ± 27 | 53.36 ± 24.44 |
| Biomarkers | |||
| FeNO (ppb) | 73.38 ± 46.84 | 61.85 ± 56.47 | 24.95 ± 10.9 |
| Eosinophils (cell/mcL) | 513.56 ± 291.55 | 95.0 ± 33.04 α,γ | 7.56 ± 22.67 β,γ |
| Exacerbations | |||
| Exacerbation (no.) | 6.36 ± 4.72 | 1 ± 1.2 α,γ | 0.09 ± 0.3 β,γ |
| A&E (no. admission) | 1.18 ± 1.47 | 0.13 ± 0.35 | 0 β |
| Hospitalisation (no. admission) | 0.22 ± 0.44 | 0.13 ± 0.35 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scioscia, G.; Tondo, P.; Nolasco, S.; Pelaia, C.; Carpagnano, G.E.; Caiaffa, M.F.; Valenti, G.; Maglio, A.; Papia, F.; Triggiani, M.; et al. Benralizumab in Patients with Severe Eosinophilic Asthma: A Multicentre Real-Life Experience. J. Clin. Med. 2023, 12, 4362. https://doi.org/10.3390/jcm12134362
Scioscia G, Tondo P, Nolasco S, Pelaia C, Carpagnano GE, Caiaffa MF, Valenti G, Maglio A, Papia F, Triggiani M, et al. Benralizumab in Patients with Severe Eosinophilic Asthma: A Multicentre Real-Life Experience. Journal of Clinical Medicine. 2023; 12(13):4362. https://doi.org/10.3390/jcm12134362
Chicago/Turabian StyleScioscia, Giulia, Pasquale Tondo, Santi Nolasco, Corrado Pelaia, Giovanna Elisiana Carpagnano, Maria Filomena Caiaffa, Giuseppe Valenti, Angelantonio Maglio, Francesco Papia, Massimo Triggiani, and et al. 2023. "Benralizumab in Patients with Severe Eosinophilic Asthma: A Multicentre Real-Life Experience" Journal of Clinical Medicine 12, no. 13: 4362. https://doi.org/10.3390/jcm12134362
APA StyleScioscia, G., Tondo, P., Nolasco, S., Pelaia, C., Carpagnano, G. E., Caiaffa, M. F., Valenti, G., Maglio, A., Papia, F., Triggiani, M., Crimi, N., Pelaia, G., Vatrella, A., Foschino Barbaro, M. P., & Crimi, C. (2023). Benralizumab in Patients with Severe Eosinophilic Asthma: A Multicentre Real-Life Experience. Journal of Clinical Medicine, 12(13), 4362. https://doi.org/10.3390/jcm12134362