
Effect of Ketamine on Postoperative Neurocognitive Disorders: A Systematic Review and Meta-Analysis

 , , ,
, , ,  and
and
Abstract

1. Introduction
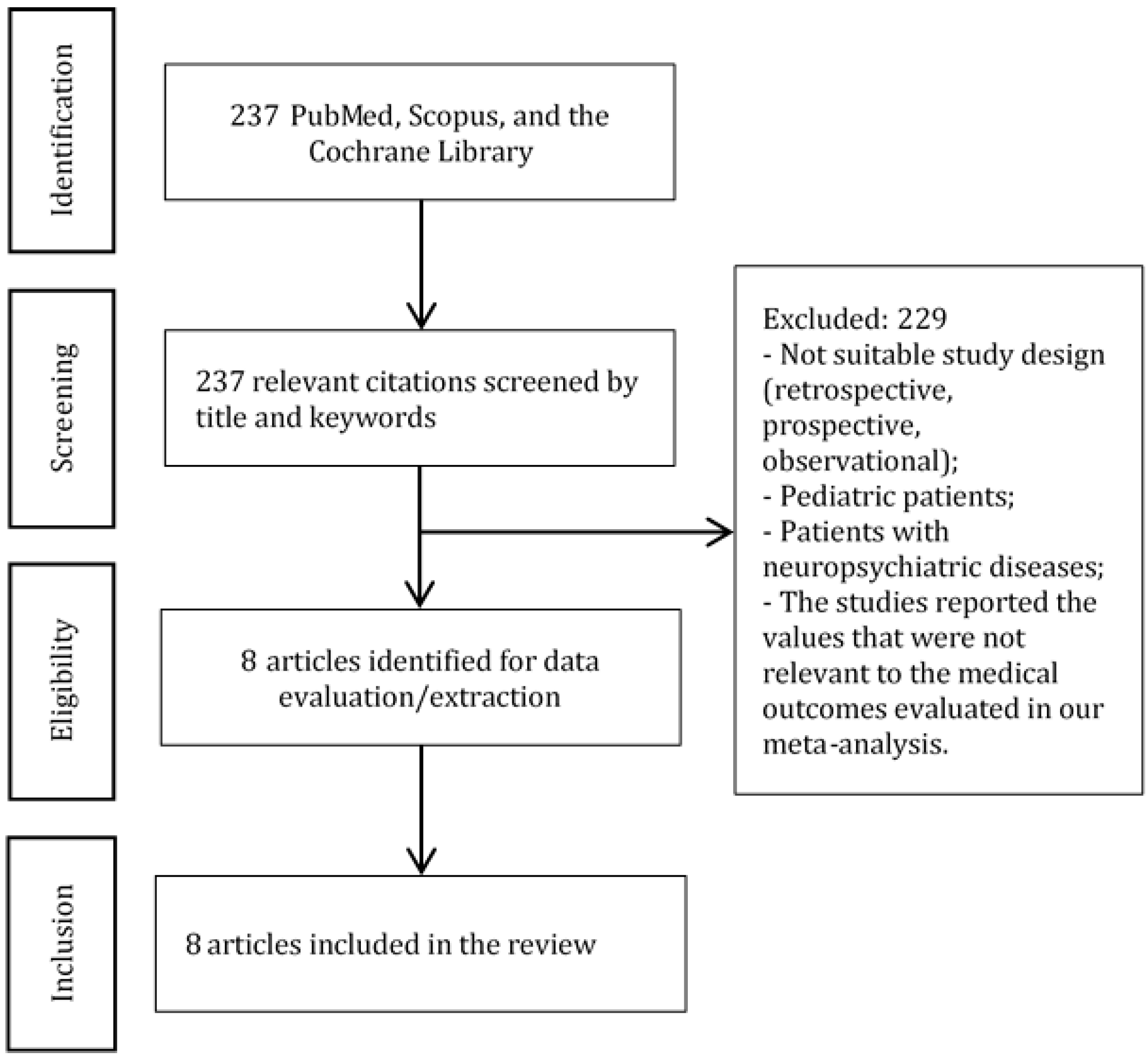
2. Materials and Methods
2.1. Protocol
2.2. Participants and Population
Inclusion criteria:
- Study types: RCTs;
- Study arms: comparison of ketamine and placebo;
- Age of patients: 18 years and older;
- Surgery: any type of surgery;
- Articles published in English.
2.3. Outcomes
2.4. Data Extraction and Statistical Methods
2.5. Assessment of Methodological Quality
3. Results
3.1. Outcomes
3.1.1. Incidence of Delirium
3.1.2. Incidence of Hallucinations
3.1.3. Vasopressor Use
3.1.4. Fentanyl Consumption (μg)
3.1.5. Morphine Consumption (mg)
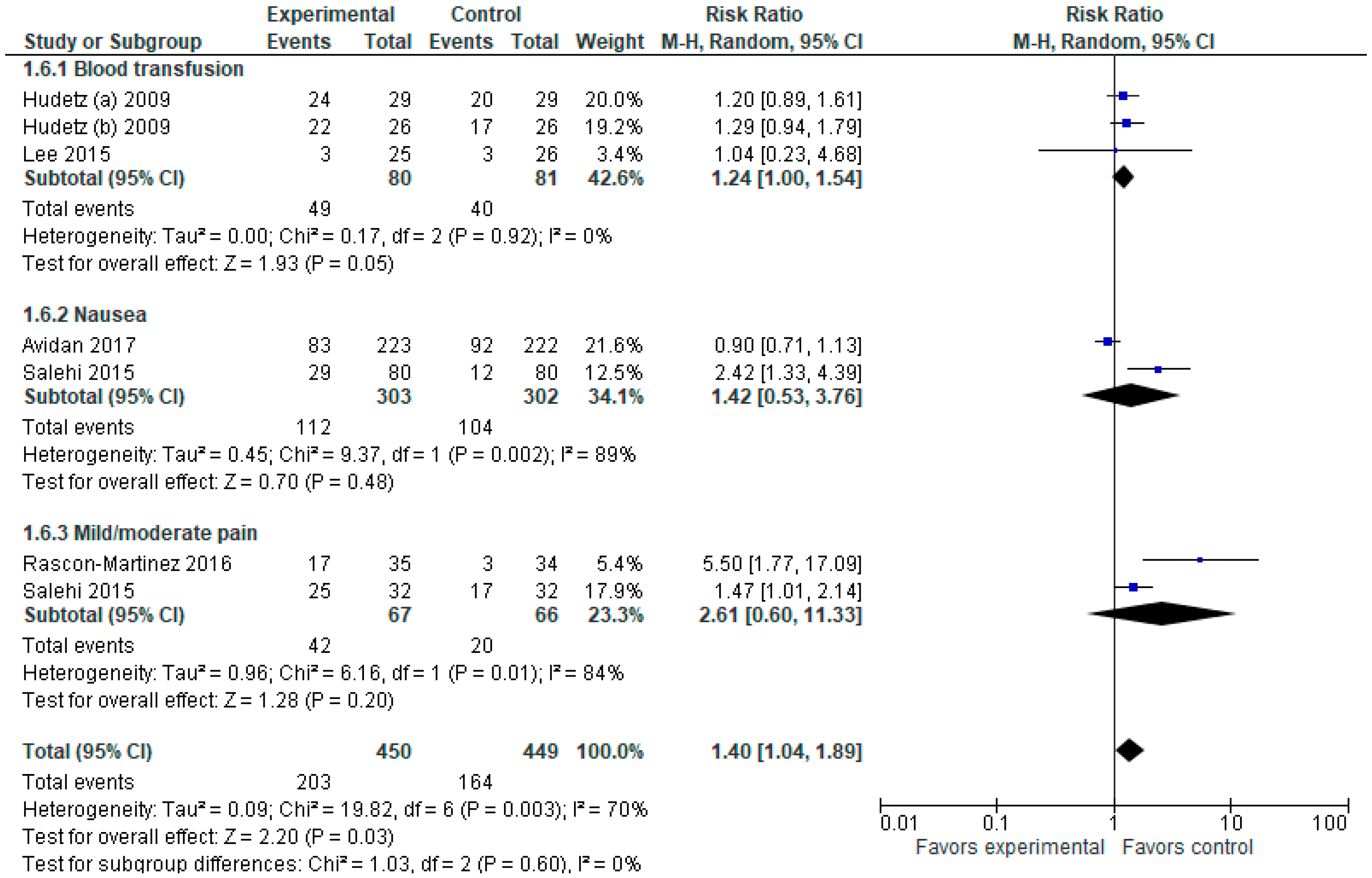
3.1.6. Adverse Events
3.1.7. Surgery Duration (min)
3.1.8. Readmission within 30 Days
3.2. Assessment of Methodological Quality
4. Discussion
- (1)
- Preoperative (advanced age, neurocognitive deterioration, depression, use of anti-depressants);
- (2)
- Intraoperative (blood loss, hypotension, pain, hypernatremia, hyponatremia, deep anesthesia (if the doses of anesthesia are higher than required, prolonged duration of anesthesia and surgery);
- (3)
- Postoperative factors (sleep deprivation, severe pain, electrolyte dysbalance, cerebrovascular events).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Incidences of Delirium | Incidences of Hallucinations | Vasopressor Use | Fentanyl Consumption (μg) | Morphine Consumption (mg) | Overall Adverse Events | Readmissions within 30 Days | |
|---|---|---|---|---|---|---|---|
| Risk of bias | Not serious | Not serious | Not serious | Serious | Not serious | Not serious | Not serious |
| Lack of allocation concealment | No | No | No | No | No | No | No |
| Lack of blinding | No | No | No | No | No | No | No |
| Incomplete accounting of patients and outcome events | No | No | No | Yes | No | No | No |
| Selective outcome reporting | No | No | No | No | No | No | No |
| Other limitations | No | No | No | No | No | No | No |
| Inconsistency | Very serious | Serious | Not serious | Not serious | Not serious | Not serious | Not serious |
| I2 (unexplained heterogeneity of results) | Yes | No | No | No | No | No | No |
| Wide variance of point estimates | Yes | No | No | No | No | Yes | No |
| Confidence intervals (CIs) do not overlap | Yes | No | No | No | No | No | No |
| Indirectness | Not serious | Not serious | Not serious | Not serious | Not serious | Not serious | Not serious |
| Differences in population | No | No | No | No | No | No | No |
| Differences in interventions | No | No | No | No | No | No | No |
| Differences in outcome measures | No | No | No | No | No | No | No |
| Indirect comparisons | No | No | No | No | No | No | No |
| Imprecision | Serious | Serious | Very serious | Serious | Not serious | Not serious | Serious |
| Few patients | No | No | Yes | Yes | No | No | Yes |
| Wide confidence interval (CI) | Yes | No | Yes | No | No | No | No |
| Other considerations | None | None | None | None | None | None | Not serious |
| RR > 2 or RR < 0.5 RR > 5 or RR < 0.2 | No | No | No | No | No | No | No |
| Dose-response gradient | No | No | No | No | No | No | No |
| Effect of plausible residual confounding | No | No | No | No | No | No | No |
References
- Rascón-Martínez, D.M.; Fresán-Orellana, A.; Ocharán-Hernández, M.E.; Genis-Zarate, J.H.; Castellanos-Olivares, A. The Effects of Ketamine on Cognitive Function in Elderly Patients Undergoing Ophthalmic Surgery: A Pilot Study. Anesth. Analg. 2016, 122, 969–975. [Google Scholar] [CrossRef]
- Hudetz, J.A.; Patterson, K.M.; Iqbal, Z.; Gandhi, S.D.; Byrne, A.J.; Hudetz, A.G.; Warltier, D.C.; Pagel, P.S. Ketamine Attenuates Delirium after Cardiac Surgery with Cardiopulmonary Bypass. J. Cardiothorac. Vasc. Anesth. 2009, 23, 651–657. [Google Scholar] [CrossRef]
- Bornemann-Cimenti, H.; Wejbora, M.; Michaeli, K.; Edler, A.; Sandner-Kiesling, A. The Effects of Minimal-Dose versus Low-Dose S-Ketamine on Opioid Consumption, Hyperalgesia, and Postoperative Delirium: A Triple-Blinded, Randomized, Active- and Placebo-Controlled Clinical Trial. Minerva Anestesiol. 2016, 82, 1069–1076. [Google Scholar]
- Hudetz, J.A.; Iqbal, Z.; Gandhi, S.D.; Patterson, K.M.; Byrne, A.J.; Hudetz, A.G.; Pagel, P.S.; Warltier, D.C. Ketamine Attenuates Post-Operative Cognitive Dysfunction after Cardiac Surgery. Acta Anaesthesiol. Scand. 2009, 53, 864–872. [Google Scholar] [CrossRef]
- Avidan, M.S.; Maybrier, H.R.; Abdallah, A.B.; Jacobsohn, E.; Vlisides, P.E.; Pryor, K.O.; Veselis, R.A.; Grocott, H.P.; Emmert, D.A.; Rogers, E.M.; et al. Intraoperative Ketamine for Prevention of Postoperative Delirium or Pain after Major Surgery in Older Adults: An International, Multicentre, Double-Blind, Randomised Clinical Trial. Lancet 2017, 390, 267–275. [Google Scholar] [CrossRef]
- Siripoonyothai, S.; Sindhvananda, W. Comparison of Postoperative Delirium within 24 Hours between Ketamine and Propofol Infusion during Cardiopulmonary Bypass Machine: A Randomized Controlled Trial. Ann. Card. Anaesth. 2021, 24, 294. [Google Scholar] [CrossRef]
- Lee, K.H.; Kim, J.Y.; Kim, J.W.; Park, J.S.; Lee, K.W.; Jeon, S.Y. Influence of Ketamine on Early Postoperative Cognitive Function After Orthopedic Surgery in Elderly Patients. Anesthesiol. Pain Med. 2015, 5, e28844. [Google Scholar] [CrossRef]
- Loo, C.K.; Katalinic, N.; Garfield, J.B.B.; Sainsbury, K.; Hadzi-Pavlovic, D.; Mac-Pherson, R. Neuropsychological and Mood Effects of Ketamine in Electroconvulsive Therapy: A Randomised Controlled Trial. J. Affect. Disord. 2012, 142, 233–240. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Salehi, B.; Mohammadbeigi, A.; Kamali, A.; Taheri-Nejad, M.; Moshiri, I. Impact Comparison of Ketamine and Sodium Thiopental on Anesthesia during Electroconvulsive Therapy in Major Depression Patients with Drug-Resistant; a Double-Blind Randomized Clinical Trial. Ann. Card. Anaesth. 2015, 18, 486. [Google Scholar] [CrossRef]
- Urban, M.K.; Ya Deau, J.T.; Wukovits, B.; Lipnitsky, J.Y. Ketamine as an Adjunct to Postoperative Pain Management in Opioid Tolerant Patients after Spinal Fusions: A Prospective Randomized Trial. HSS J. ® Musculoskelet. J. Hosp. Spec. Surg. 2008, 4, 62–65. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the Quality of Reports of Randomized Clinical Trials: Is Blinding Necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Schünemann, H.J.; Tugwell, P.; Knottnerus, A. GRADE Guidelines: A New Series of Articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally Estimating the Sample Mean from the Sample Size, Median, Mid-Range, and/or Mid-Quartile Range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Viderman, D.; Brotfain, E.; Bilotta, F.; Zhumadilov, A. Risk factors and mechanisms of postoperative delirium after intracranial neurosurgical procedures. Asian J. Anesthesiol. 2020, 58, 5–13. [Google Scholar]
- Viderman, D.; Nabidollayeva, F.; Aubakirova, M.; Yessimova, D.; Badenes, R.; Abdildin, Y. Postoperative Delirium and Cognitive Dysfunction after General and Regional Anesthesia: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 3549. [Google Scholar] [CrossRef]
- Glumac, S.; Kardum, G.; Karanovic, N. Postoperative Cognitive Decline After Cardiac Surgery: A Narrative Review of Current Knowledge in 2019. Med. Sci. Monit. 2019, 25, 3262–3270. [Google Scholar] [CrossRef]
- Dale, O.; Somogyi, A.A.; Li, Y.; Sullivan, T.; Shavit, Y. Does Intraoperative Ketamine Attenuate Inflammatory Reactivity Following Surgery? A Systematic Review and Meta-Analysis. Anesth. Analg. 2012, 115, 934–943. [Google Scholar] [CrossRef]
- Zanos, P.; Moaddel, R.; Morris, P.J.; Riggs, L.M.; Highland, J.N.; Georgiou, P.; Pereira, E.F.R.; Albuquerque, E.X.; Thomas, C.J.; Zarate, C.A.; et al. Ketamine and Ketamine Metabolite Pharmacology: Insights into Therapeutic Mechanisms. Pharmacol. Rev. 2018, 70, 621–660. [Google Scholar] [CrossRef]
- Malhotra, A.K.; Pinals, D.A.; Weingartner, H.; Sirocco, K.; Missar, C.D.; Pickar, D.; Breier, A. NMDA Receptor Function and Human Cognition: The Effects of Ketamine in Healthy Volunteers. Neuropsychopharmacology 1996, 14, 301–307. [Google Scholar] [CrossRef]
- Holcomb, H.H.; Lahti, A.C.; Medoff, D.R.; Weiler, M.; Tamminga, C.A. Sequential Regional Cerebral Blood Flow Brain Scans Using PET with H215O Demonstrate Ketamine Actions in CNS Dynamically. Neuropsychopharmacology 2001, 25, 165–172. [Google Scholar] [CrossRef]
- Sakai, T.; Ichiyama, T.; Whitten, C.W.; Giesecke, A.H.; Lipton, J.M. Ketamine Suppresses Endotoxin-Induced NF-KappaB Expression. Can. J. Anaesth. J. Can. Anesth. 2000, 47, 1019–1024. [Google Scholar] [CrossRef]
- Baldwin, A.S. The NF-Kappa B and I Kappa B Proteins: New Discoveries and Insights. Annu. Rev. Immunol. 1996, 14, 649–683. [Google Scholar] [CrossRef]
- Långsjö, J.W.; Kaisti, K.K.; Aalto, S.; Hinkka, S.; Aantaa, R.; Oikonen, V.; Sipilä, H.; Kurki, T.; Silvanto, M.; Scheinin, H. Effects of Subanesthetic Doses of Ketamine on Regional Cerebral Blood Flow, Oxygen Consumption, and Blood Volume in Humans. Anesthesiology 2003, 99, 614–623. [Google Scholar] [CrossRef]









| First Author Year | Study Goals | Procedure | Ketamine Dose | Conclusions |
|---|---|---|---|---|
| Avidan 2017 [5] | To assess the effect of ketamine on delirium in the post-surgical elderly | Various types of surgeries | Low-dose: 0.5 mg/kg High-dose: 1.0 mg/kg | No lowering effect of ketamine on delirium, opioid use, or pain |
| Bornemann-Cimenti 2016 [3] | To evaluate the use of low-dose ketamine as part of multimodal analgesia to reduce pain and opioid consumption | Elective colorectal and hepatic surgery | Low-dose: 0.25 mg/kg bolus and 0.125 mg/kg/h infusion for 48 h Minimal-dose: 0.015 mg/kg/h infusion following a saline bolus | Minimal dose ketamine had no superiority on pain control or opioid consumption, but it lowered the incidence of delirium |
| Hudetz 2009 [2] | To examine the effect of ketamine on the incidence of delirium in older cardiac surgery patients | CABG, valvular surgery, coronary artery disease, valvular disease | 0.5 mg/kg IV | Incidence of delirium was lower in the ketamine group |
| Hudetz 2009 [4] | To assess the incidence of delirium following ketamine use in cardiac surgery | Cardiac surgery | 0.5 mg/kg IV | Ketamine reduced post-operative cognitive dysfunction seven days after cardiac surgery |
| Lee 2015 [7] | To assess the effect of ketamine on postoperative cognitive dysfunction in orthopedic surgery patients | Acromioplasty, open reduction and internal fixation, spine surgery, total hip replacement arthroplasty, total knee replacement arthroplasty/Carpal tunnel syndrome, fractures | Ketamine: 0.5 mg/kg IV Placebo: 3 mL 0.9% saline | No effect of ketamine on postoperative cognitive dysfunction |
| Rascon-Martinez 2016 [1] | To examine the effect of ketamine on cognitive status in the elderly | Ophthalmic surgery: vitrectomy or cataract surgery/Cataract | 0.3 mg/kg dose | Improved cognitive status following ketamine use |
| Salehi 2015 [10] | To study the effect of ketamine on delirium and depression after electro-convulsive therapy | Electroconvulsive therapy/Drug-resistant major depression | Ketamine 0.8 mg/kgSodium thiopental 1–1.5 mg/kg | Comparable effect on depression, higher incidence of complications in the ketamine group |
| Urban 2008 [11] | To study the effect of ketamine as part of multimodal analgesia for managing acute pain following spinal fusions | Spinal fusions | 0.2 mg/kg on induction; 2 mcg/kg/hour for the next 24 h | Improved pain scores in the ketamine group, but no difference in opioid consumption or cognitive function |
| First Author Year | Study Design | Country | Groups | Age | Sample Size |
|---|---|---|---|---|---|
| Avidan 2017 [5] | RCT | USA, Korea, Canada, India | Placebo Low-dose ketamine High-dose ketamine | 70 (6.9) 70 (7.2) 70 (7.3) | 654 (217/221/216) |
| Bornemann-Cimenti 2016 [3] | RCT | Austria | Low-dose Minimal dose Placebo | 62.2 (9.8) 58.4 (8.1) 61 (12.4) | 56 (19/18/19) |
| Hudetz 2009 [2] | RCT | USA | Placebo Ketamine | 60 (8) 68 (8) | 58 (29/29) |
| Hudetz 2009 [4] | RCT | USA | Placebo Ketamine Control nonsurgical | 67 (8) 68 (7) 64 (7) | 78 (26/26/26) |
| Lee 2015 [7] | RCT | Korea | Ketamine Placebo | 68.38 (6.54) 68.32 (5.34) | 51 (25/26) |
| Rascon-Martinez 2016 [1] | RCT | Mexico | Ketamine Placebo | 70.5 (4.7) 68.7 (7.1) | 65 (33/32) |
| Salehi 2015 [10] | RCT | Iran | Ketamine Sodium thiopental | 20–60 | 160 (80/80) |
| Urban 2008 [11] | RCT | USA | Ketamine Control | 53 (12) 48 (9) | 24 (12/12) |
| Study or Subgroup | Was This Study Described as Randomized? | Was the Method Used to Generate the Sequence of Randomization Appropriate and Described? | Was the Study Described as Double-Blind? | Was the Method of Double Blind Appropriate and Described? | Was there a Description of Withdraw and Dropouts? | Total Score |
|---|---|---|---|---|---|---|
| Avidan 2017 [5] | 1 | 1 | 1 | 1 | 1 | 5 |
| Bornemann-Cimenti 2016 [3] | 1 | 1 | 1 | 1 | 1 | 5 |
| Hudetz 2009 [2] | 1 | 1 | 1 | 1 | 0 | 4 |
| Hudetz 2009 [4] | 1 | 1 | 1 | 1 | 1 | 5 |
| Lee 2015 [7] | 1 | 1 | 1 | 1 | 1 | 5 |
| Rascon-Martinez 2016 [1] | 1 | 1 | 1 | 0 | 1 | 4 |
| Salehi 2015 [10] | 1 | 1 | 1 | 0 | 0 | 3 |
| Urban 2008 [11] | 1 | 1 | 1 | 1 | 1 | 5 |
| Study (First Author, Year) | Risk of Bias Arising from the Randomization Process | Risk of Bias Due to Deviations from the Intended Interventions | Missing Outcome Data | Risk of Bias in Measurement of the Outcome | Risk of Bias in Selection of the Reported Result | Overall Risk of Bias |
|---|---|---|---|---|---|---|
| Avidan et al., 2017 [5] | Low risk | Low risk | Some concerns | Low risk | Low risk | Low risk |
| Rascón-Martínez et al., 2016 [1] | Low risk | Low risk | Some concerns | Low Risk | Low risk | Low risk |
| Hudetz et al., 2009 [2] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Hudetz et al., 2009 [4] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Salehi et al., 2015 [10] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Urban et al., 2008 [11] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Lee et al., 2015 [7] | Low risk | Low risk | Some concerns | Low risk | Low risk | Low risk |
| Bornemann-Cimenti et al., 2016 [3] | Low risk | Low risk | Some concerns | Low risk | Low risk | Low risk |
| Outcomes | Risk Ratio [95% CI] | Standardized Mean Difference [95% CI] | Number of Participants (Studies) | Certainty of the Evidence (GRADE) |
|---|---|---|---|---|
| Incidence of delirium | 1.03 [0.61, 1.73] | - | 663 (3) | Low ⨁⨁⊖⊖ |
| Incidence of hallucinations | 1.54 [1.09, 2.19] | - | 469 (2) | High ⨁⨁⨁⨁ |
| Morphine consumption (mg) | - | −0.19 [−0.43, 0.06] | 377 (3) | High ⨁⨁⨁⨁ |
| Overall adverse events | 1.40 [1.04, 1.89] | - | 899 (6) | High ⨁⨁⨁⨁ |
| Fentanyl consumption (μg) | - | −0.23 [−0.53, 0.07] | 175 (3) | Low ⨁⨁⊖⊖ |
| Vasopressor use | 1.03 [0.78, 1.36] | - | 110 (2) | Moderate ⨁⨁⨁⊖ |
| Readmissions within 30 days | 0.25 [0.09, 0.70] | - | 110 (2) | Moderate ⨁⨁⨁⊖ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viderman, D.; Aubakirova, M.; Nabidollayeva, F.; Yegembayeva, N.; Bilotta, F.; Badenes, R.; Abdildin, Y. Effect of Ketamine on Postoperative Neurocognitive Disorders: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 4314. https://doi.org/10.3390/jcm12134314
Viderman D, Aubakirova M, Nabidollayeva F, Yegembayeva N, Bilotta F, Badenes R, Abdildin Y. Effect of Ketamine on Postoperative Neurocognitive Disorders: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(13):4314. https://doi.org/10.3390/jcm12134314
Chicago/Turabian StyleViderman, Dmitriy, Mina Aubakirova, Fatima Nabidollayeva, Nurgul Yegembayeva, Federico Bilotta, Rafael Badenes, and Yerkin Abdildin. 2023. "Effect of Ketamine on Postoperative Neurocognitive Disorders: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 13: 4314. https://doi.org/10.3390/jcm12134314
APA StyleViderman, D., Aubakirova, M., Nabidollayeva, F., Yegembayeva, N., Bilotta, F., Badenes, R., & Abdildin, Y. (2023). Effect of Ketamine on Postoperative Neurocognitive Disorders: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(13), 4314. https://doi.org/10.3390/jcm12134314