
Influence of the Therapeutic Alliance on the Rehabilitation of Stroke: A Systematic Review of Qualitative Studies

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
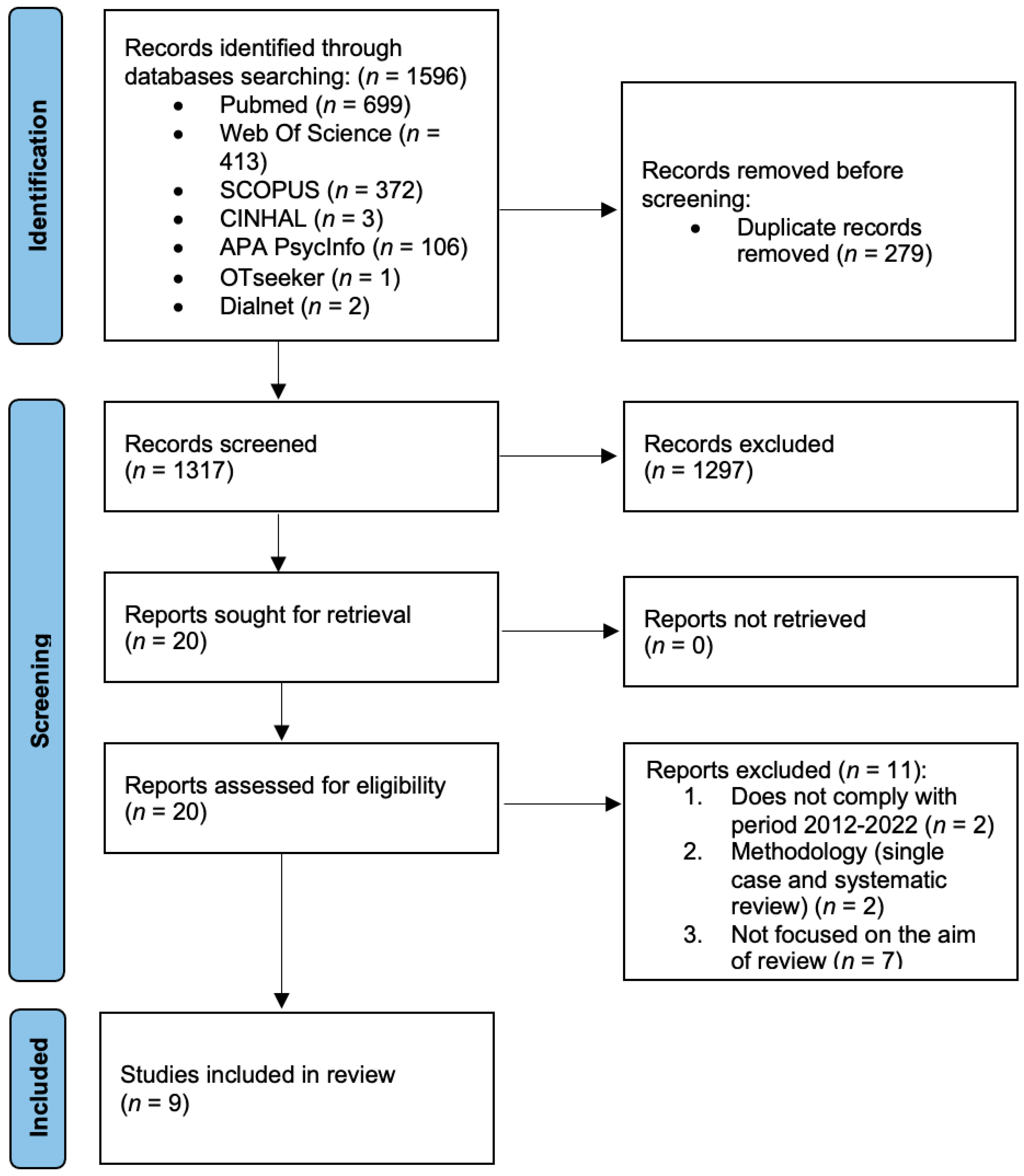
2.1. Information Sources and Search Strategy
2.2. Quality Assessment of Included Studies
2.3. Eligibility Criteria and Study Selection
3. Results
4. Discussion
4.1. Being Recognised as a Person
4.2. Empathy, Emotional Bonding and Trust
4.3. Collaboration
4.4. Individualising Rehabilitation
4.5. Control and Empowerment
4.6. Role of Health Professionals
4.7. Maintaining Hope
4.8. The Family
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fleminger, S.; Ponsford, J. Long Term Outcome after Traumatic Brain Injury. BMJ 2005, 331, 1419–1420. [Google Scholar] [CrossRef]
- Bruns, J.; Hauser, W.A. The Epidemiology of Traumatic Brain Injury: A Review. Epilepsia 2003, 44, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Goldman, L.; Siddiqui, E.M.; Khan, A.; Jahan, S.; Rehman, M.U.; Mehan, S.; Sharma, R.; Budkin, S.; Kumar, S.N.; Sahu, A.; et al. Understanding Acquired Brain Injury: A Review. Biomedicines 2022, 10, 2167. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Neurological Disorders: Public Health Challenges; World Health Organization: Geneva, Switzerland, 2006; Volume 218. [Google Scholar]
- Perin, C.; Bolis, M.; Limonta, M.; Meroni, R.; Ostasiewicz, K.; Cornaggia, C.M.; Alouche, S.R.; da Silva Matuti, G.; Cerri, C.G.; Piscitelli, D. Differences in Rehabilitation Needs after Stroke: A Similarity Analysis on the ICF Core Set for Stroke. Int. J. Environ. Res. Public Health 2020, 17, 4291. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, R.B.C.; Galvão, S.C.B.; Frederico, L.M.P.; Amaral, N.S.L.; Carneiro, M.I.S.; de Moura Filho, A.G.; Piscitelli, D.; Monte-Silva, K. Cortical and Spinal Excitability Changes after Repetitive Transcranial Magnetic Stimulation Combined to Physiotherapy in Stroke Spastic Patients. Neurol. Sci. 2019, 40, 1199–1207. [Google Scholar] [CrossRef]
- Monte-Silva, K.; Piscitelli, D.; Norouzi-Gheidari, N.; Batalla, M.A.P.; Archambault, P.; Levin, M.F. Electromyogram-Related Neuromuscular Electrical Stimulation for Restoring Wrist and Hand Movement in Poststroke Hemiplegia: A Systematic Review and Meta-Analysis. Neurorehabil. Neural Repair 2019, 33, 96–111. [Google Scholar] [CrossRef]
- World Health Organization (Ed.) International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001; ISBN 978-92-4-154542-6. [Google Scholar]
- Ardito, R.; Rabellino, D. Therapeutic Alliance and Outcome of Psychotherapy: Historical Excursus, Measurements, and Prospects for Research. Front. Psychol. 2011, 2, 270. [Google Scholar] [CrossRef]
- Graves, T.A.; Tabri, N.; Thompson-Brenner, H.; Franko, D.L.; Eddy, K.T.; Bourion-Bedes, S.; Brown, A.; Constantino, M.J.; Flückiger, C.; Forsberg, S.; et al. A Meta-Analysis of the Relation between Therapeutic Alliance and Treatment Outcome in Eating Disorders. Int. J. Eat. Disord. 2017, 50, 323–340. [Google Scholar] [CrossRef] [PubMed]
- Bishop, M.; Kayes, N.; McPherson, K. Understanding the Therapeutic Alliance in Stroke Rehabilitation. Disabil. Rehabil. 2021, 43, 1074–1083. [Google Scholar] [CrossRef]
- Babatunde, F.; MacDermid, J.; MacIntyre, N. Characteristics of Therapeutic Alliance in Musculoskeletal Physiotherapy and Occupational Therapy Practice: A Scoping Review of the Literature. BMC Health Serv. Res. 2017, 17, 375. [Google Scholar] [CrossRef]
- Peiris, C.L.; Taylor, N.F.; Shields, N. Patients Value Patient-Therapist Interactions More than the Amount or Content of Therapy during Inpatient Rehabilitation: A Qualitative Study. J. Physiother. 2012, 58, 261–268. [Google Scholar] [CrossRef]
- McCormack, B.; Karlsson, B.; Dewing, J.; Lerdal, A. Exploring Person-Centredness: A Qualitative Meta-Synthesis of Four Studies. Scand. J. Caring Sci. 2010, 24, 620–634. [Google Scholar] [CrossRef]
- Søgaard, M.B.; Andresen, K.; Kristiansen, M. Systematic Review of Patient-Engagement Interventions: Potentials for Enhancing Person-Centred Care for Older Patients with Multimorbidity. BMJ Open 2021, 11, e048558. [Google Scholar] [CrossRef] [PubMed]
- Bordin, E.S. The Generalizability of the Psychoanalytic Concept of the Working Alliance. Psychother. Theory Res. Pract. 1979, 16, 252–260. [Google Scholar] [CrossRef]
- Muran, J.C.; Barber, J.P. (Eds.) The Therapeutic Alliance: An Evidence-Based Guide to Practice; Guilford Press: New York, NY, USA, 2011; Volume 41. [Google Scholar] [CrossRef]
- Rønnestad, M.H.; Willutzki, U.; Tarragona, M.; David, E. Orlinsky: Developing Psychotherapy Research, Researching Psychotherapist Development. In Bringing Psychotherapy Research to Life: Understanding Change through the Work of Leading Clinical Researchers; American Psychological Association: Washington, DC, USA, 2010; pp. 233–243. ISBN 978-1-4338-0774-9. [Google Scholar]
- Flückiger, C.; Del Re, A.C.; Wampold, B.E.; Znoj, H.; Caspar, F.; Jörg, U. Valuing Clients’ Perspective and the Effects on the Therapeutic Alliance: A Randomized Controlled Study of an Adjunctive Instruction. J. Couns. Psychol. 2012, 59, 18–26. [Google Scholar] [CrossRef]
- Mohr, W.; Rädke, A.; Afi, A.; Edvardsson, D.; Mühlichen, F.; Platen, M.; Roes, M.; Michalowsky, B.; Hoffmann, W. Key Intervention Categories to Provide Person-Centered Dementia Care: A Systematic Review of Person-Centered Interventions. J. Alzheimer’s Dis. 2021, 84, 343–366. [Google Scholar] [CrossRef] [PubMed]
- Flückiger, C.; Del Re, A.C.; Wampold, B.E.; Horvath, A.O. The Alliance in Adult Psychotherapy: A Meta-Analytic Synthesis. Psychotherapy 2018, 55, 316–340. [Google Scholar] [CrossRef] [PubMed]
- Danzl, M.M.; Etter, N.M.; Andreatta, R.D.; Kitzman, P.H. Facilitating Neurorehabilitation through Principles of Engagement. J. Allied Health 2012, 41, 35–41. [Google Scholar]
- Deuschl, G.; Beghi, E.; Fazekas, F.; Varga, T.; Christoforidi, K.A.; Sipido, E.; Bassetti, C.L.; Vos, T.; Feigin, V.L. The Burden of Neurological Diseases in Europe: An Analysis for the Global Burden of Disease Study 2017. Lancet Public Health 2020, 5, E551–E567. [Google Scholar] [CrossRef]
- Béjot, Y.; Daubail, B.; Jacquin, A.; Durier, J.; Osseby, G.-V.; Rouaud, O.; Giroud, M. Trends in the Incidence of Ischaemic Stroke in Young Adults between 1985 and 2011: The Dijon Stroke Registry. J. Neurol. Neurosurg. Psychiatry 2014, 85, 509–513. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Mudge, S.; Stretton, C.; Kayes, N. Are Physiotherapists Comfortable with Person-Centred Practice? An Autoethnographic Insight. Disabil. Rehabil. 2014, 36, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.; Sage, K.; Haddock, G.; Conroy, P.; Serrant, L. Speech and Language Therapists’ Perspectives of Therapeutic Alliance Construction and Maintenance in Aphasia Rehabilitation Post-Stroke. Int. J. Lang. Commun. Disord. 2018, 53, 550–563. [Google Scholar] [CrossRef]
- Hersh, D.; Wood, P.; Armstrong, E. Informal Aphasia Assessment, Interaction and the Development of the Therapeutic Relationship in the Early Period after Stroke. Aphasiology 2018, 32, 876–901. [Google Scholar] [CrossRef]
- Lawton, M.; Haddock, G.; Conroy, P. People with Aphasia’s Perception of the Therapeutic Alliance in Aphasia Rehabilitation Post Stroke: A Thematic Analysis. Aphasiology 2018, 32, 1397–1417. [Google Scholar] [CrossRef]
- Walder, K.; Molineux, M. Listening to the Client Voice—A Constructivist Grounded Theory Study of the Experiences of Client-Centred Practice after Stroke. Aust. Occup. Ther. J. 2020, 67, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Kayes, N.M.; Cummins, C.; McPherson, K.M.; Worrall, L.; Bright, F.A.S. Developing Connections for Engagement in Stroke Rehabilitation. Brain Impair. 2021, 23, 42–59. [Google Scholar] [CrossRef]
- Williams, L.M.; Douglas, J.M. It Takes Two to Tango: The Therapeutic Alliance in Community Brain Injury Rehabilitation. Brain Impair. 2021, 23, 24–41. [Google Scholar] [CrossRef]
- Gordon, C.; Ellis-Hill, C.; Dewar, B.; Watkins, C. Knowing-in-Action That Centres Humanising Relationships on Stroke Units: An Appreciative Action Research Study. Brain Impair. 2022, 23, 60–75. [Google Scholar] [CrossRef]
- Grohn, B.; Worrall, L.; Simmons-Mackie, N.; Hudson, K. Living Successfully with Aphasia during the First Year Post-Stroke: A Longitudinal Qualitative Study. Aphasiology 2014, 28, 1405–1425. [Google Scholar] [CrossRef]
- Pallesen, H. Body, Coping and Self-Identity. A Qualitative 5-Year Follow-up Study of Stroke. Disabil. Rehabil. 2014, 36, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Kayes, N.M.; McPherson, K.M. Human Technologies in Rehabilitation: “Who” and “How” We Are with Our Clients. Disabil. Rehabil. 2012, 34, 1907–1911. [Google Scholar] [CrossRef]
- Andrew, N.E.; Kilkenny, M.; Naylor, R.; Purvis, T.; Lalor, E.; Moloczij, N.; Cadilhac, D.A. National Stroke Foundation Understanding Long-Term Unmet Needs in Australian Survivors of Stroke. Int. J. Stroke 2014, 9 (Suppl. A100), 106–112. [Google Scholar] [CrossRef] [PubMed]
- Besley, J.; Kayes, N.M.; McPherson, K.M. Assessing Therapeutic Relationships in Physiotherapy: Literature Review. New Zealand J. Physiother. 2011, 39, 81–91. [Google Scholar]
- Bright, F.A.S.; Kayes, N.M.; McCann, C.M.; McPherson, K.M. Understanding Hope after Stroke: A Systematic Review of the Literature Using Concept Analysis. Top. Stroke Rehabil. 2011, 18, 490–508. [Google Scholar] [CrossRef] [PubMed]
- Soundy, A.; Sayers, J.; Stubbs, B.; Roskell, C. Don’t Take My Hope Away: Understanding the Patient’s Hope Inneurological Rehabilitation. Int. J. Ther. Rehabil. 2014, 21, 257–258. [Google Scholar] [CrossRef]
- Lawton, M.; Haddock, G.; Conroy, P.; Sage, K. Therapeutic Alliances in Stroke Rehabilitation: A Meta-Ethnography. Arch. Phys. Med. Rehabil. 2016, 97, 1979–1993. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.M.; Armstrong, J.; Buckley, A.; Sherry, J.; Young, T.; Foliaki, S.; James-Hohaia, T.M.; Theadom, A.; McPherson, K.M. Encouraging Family Engagement in the Rehabilitation Process: A Rehabilitation Provider’s Development of Support Strategies for Family Members of People with Traumatic Brain Injury. Disabil. Rehabil. 2012, 34, 1855–1862. [Google Scholar] [CrossRef]
- Lawton, M.; Conroy, P.; Sage, K.; Haddock, G. Aphasia and stroke therapeutic alliance measure (A-STAM): Development and preliminary psychometric evaluation. Int. J. Speech-Lang. Pathol. 2019, 21, 459–469. [Google Scholar] [CrossRef]


{kind=link}
| Search Strategy: (Therapeutic Alliance) or (Therapeutic Relationship) and (Stroke) and (Outcome) or (Recovery) | ||
|---|---|---|
| Databases Consulted | Filters | Results |
| PubMed |
| 699 |
| Web of science |
| 413 |
| SCOPUS |
| 372 |
| CINAHL |
| 3 |
| APA PsycInfo |
| 106 |
| OTseeker | Application of filters is not allowed | 1 |
| Dialnet |
| 2 |
| First Author and Year | Type of Study | Main Research Aim | Participants (N) | Instruments | Characteristics of the Intervention | Outcomes | Quality of the Studies |
|---|---|---|---|---|---|---|---|
| Mudge et al. (2014) [27] | Qualitative ethnographic study | Understand the shared conflictual response to and discomfort with person-centered rehabilitation in the rehabilitation context. | N = 2 physiotherapists | 10 written reflections and 5 joint discussions | Reflections following a coaching session. Discussion after reading them. Agreeing on the next topic and carrying out literature research and reading. | Biomedical dominance places the health professional as the expert, limiting the value they place on gaining the patient’s perspective and a collaborative working engagement. | COREQ: 26/32 |
| Lawton et al. (2018a) [28] | Qualitative exploratory study | To explore perceptions and experiences of developing and maintaining therapeutic alliances in aphasia rehabilitation post-stroke. | N = 22 speech and language therapists (24–58 years) | Semi- structured interviews | Included relationship, collaboration, expectations and roles, motivation, experience and family involvement. · Recordings and transcriptions · Inductive analysis | Therapists use multiple strategies to develop alliances with people with aphasia in order to establish the basis for therapeutic work. In addition, there are external variables that interact to impede or facilitate the development of the alliance. | COREQ: 25/32 |
| Hersh et al. (2018) [29] | Qualitative study | Explore interactions during informal assessment, the balance of interactions and their impact on the development of the therapeutic relationship. | N = 3 men with aphasia (74, 48 and 80 years) | Assessment sessions | · Recordings and transcriptions · Reflections on the sessions | Informal assessment by clinicians can go beyond the choice of non-standardized tasks and materials. It also involves a number of interactive features aimed at normalising a set of potentially uncomfortable and challenging activities, forming a balance in interactions and facilitating relationships. | COREQ: 22/32 |
| Lawton et al. (2018b) [30] | Qualitative study | To investigate the experiences and reflections of people with aphasia about building and maintaining therapeutic alliances in rehabilitation. | N = 18 people with aphasia (45–88 years) | Semi- structured interviews | · Recordings and transcriptions · Field notes · Inductive thematic analysis | The therapist’s ability to adapt the alliance to the individual’s preferences and needs dictated the perceived success of the alliance. Positive alliances have the potential to stimulate both hope and engagement. | COREQ: 26/32 |
| Walder et al. (2020) [31] | Constructivist grounded theory qualitative study | To explore how stroke survivors perceive their relationship with the healthcare team as they adjust to life after stroke. | N = 6 (34–76 years) | Semi- structured interviews | Open-ended and probing questions · Transcriptions · Simultaneous data collection and analysis | Positive aspects of relationships were recognized, such as the provision of information, professional practice, hope and emotional support. | COREQ: 25/32 |
| Bishop et al. (2021) [11] | Qualitative study with interpretative description | To explore the basic components of a therapeutic alliance and the factors that are perceived to impact its development in a stroke rehabilitation unit. | N = 17 (29–76 years) Users (N = 10) Professionals (N = 7) | Semi-structured interviews and focus group discussions | Individual and focus group interviews · Recordings and transcriptions · Field notes · Conventional content analysis | Personal connection, professional collaboration and collaboration between family and clients appear to be the most prominent core components of the relationships. Given the value placed on it by participants, determining and addressing each client’s therapeutic relationship can augment rehabilitation processes and outcomes. | COREQ: 24/32 |
| Kayes et al. (2021) [32] | Qualitative exploratory study | Identify key processes for engagement in stroke rehabilitation. | N = 19 users (46–83 years) | Semi- structured interviews | Individual interviews · Recordings and transcriptions · Collaborative and iterative analysis. ·Coding, note taking, diagramming and group discussions. | Engagement is a complex, nuanced, responsive, flexible and bidirectional process. The development of connections appears to be central to engagement, and connections take many forms. The most fundamental was the therapeutic connection between the person with stroke and their professional. | COREQ: 27/32 |
| Williams et al. (2021) [33] | Qualitative study with grounded theory methodology | To obtain an understanding of the therapeutic alliance in community rehabilitation from the perspective of adults with traumatic brain injury and their relatives. | N = 6 (30–45 years) Users (N= 3) Relatives (N = 3) | Semi- structured interviews | Individual interviews · Recordings and transcriptions · Field notes | Therapeutic alliance is an important concept for the rehabilitation experience of people with traumatic brain injury and their relatives. It involves being recognized as an individual, working together and feeling personally connected. | COREQ: 24/32 |
| Gordon et al. (2022) [34] | Appreciative action research study | Describe the processes involved in the creation of meaningful relationships in stroke units. | N = 89 (46–95 years) Professionals (N = 65) Users (N = 17) Relatives (N = 7). | Informal observation, informal discussions, focus groups and semi- structured interviews | Four stages: discover, envision, design and integrate. Iterative cycles of feedback, reflection and evaluation. | The processes that support human connections in practice were sensitising to humanize relational knowledge; valuing, reflecting on and sharing relational experiences; and having the freedom to act, enabling human connections. | COREQ: 23/32 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heredia-Callejón, A.; García-Pérez, P.; Armenta-Peinado, J.A.; Infantes-Rosales, M.Á.; Rodríguez-Martínez, M.C. Influence of the Therapeutic Alliance on the Rehabilitation of Stroke: A Systematic Review of Qualitative Studies. J. Clin. Med. 2023, 12, 4266. https://doi.org/10.3390/jcm12134266
Heredia-Callejón A, García-Pérez P, Armenta-Peinado JA, Infantes-Rosales MÁ, Rodríguez-Martínez MC. Influence of the Therapeutic Alliance on the Rehabilitation of Stroke: A Systematic Review of Qualitative Studies. Journal of Clinical Medicine. 2023; 12(13):4266. https://doi.org/10.3390/jcm12134266
Chicago/Turabian StyleHeredia-Callejón, Alejandra, Patricia García-Pérez, Juan Antonio Armenta-Peinado, Miguel Ángel Infantes-Rosales, and María Carmen Rodríguez-Martínez. 2023. "Influence of the Therapeutic Alliance on the Rehabilitation of Stroke: A Systematic Review of Qualitative Studies" Journal of Clinical Medicine 12, no. 13: 4266. https://doi.org/10.3390/jcm12134266
APA StyleHeredia-Callejón, A., García-Pérez, P., Armenta-Peinado, J. A., Infantes-Rosales, M. Á., & Rodríguez-Martínez, M. C. (2023). Influence of the Therapeutic Alliance on the Rehabilitation of Stroke: A Systematic Review of Qualitative Studies. Journal of Clinical Medicine, 12(13), 4266. https://doi.org/10.3390/jcm12134266