
Factors Contributing to the Link between Physical Well-Being and Chronic Pain in Young People from Galicia, Northwest Spain


Abstract
1. Introduction
2. Method
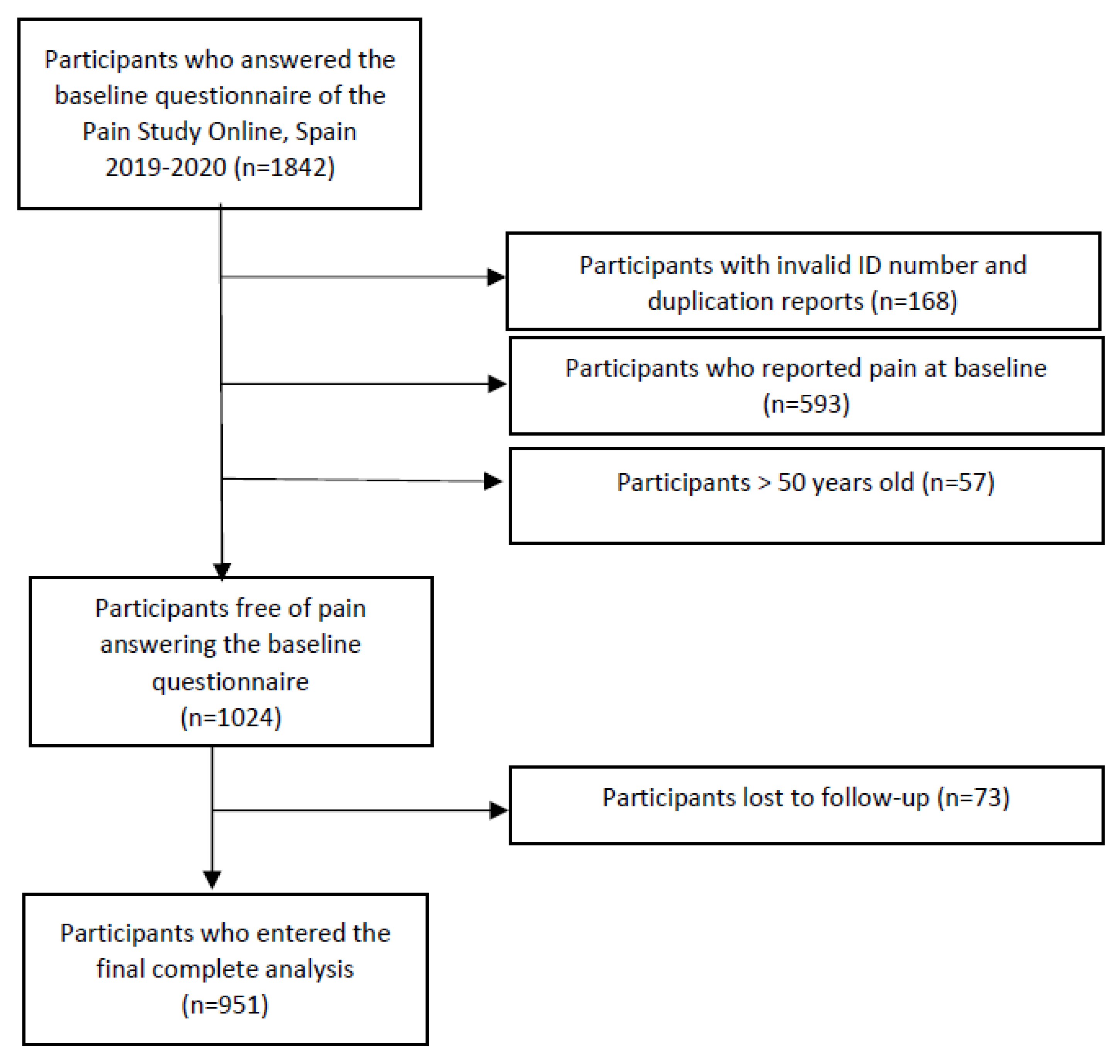
2.1. Study Sample and Procedure
2.2. Outcome Definition
2.3. Exposure Definition
2.4. Covariate Definition
2.5. Measures of Association
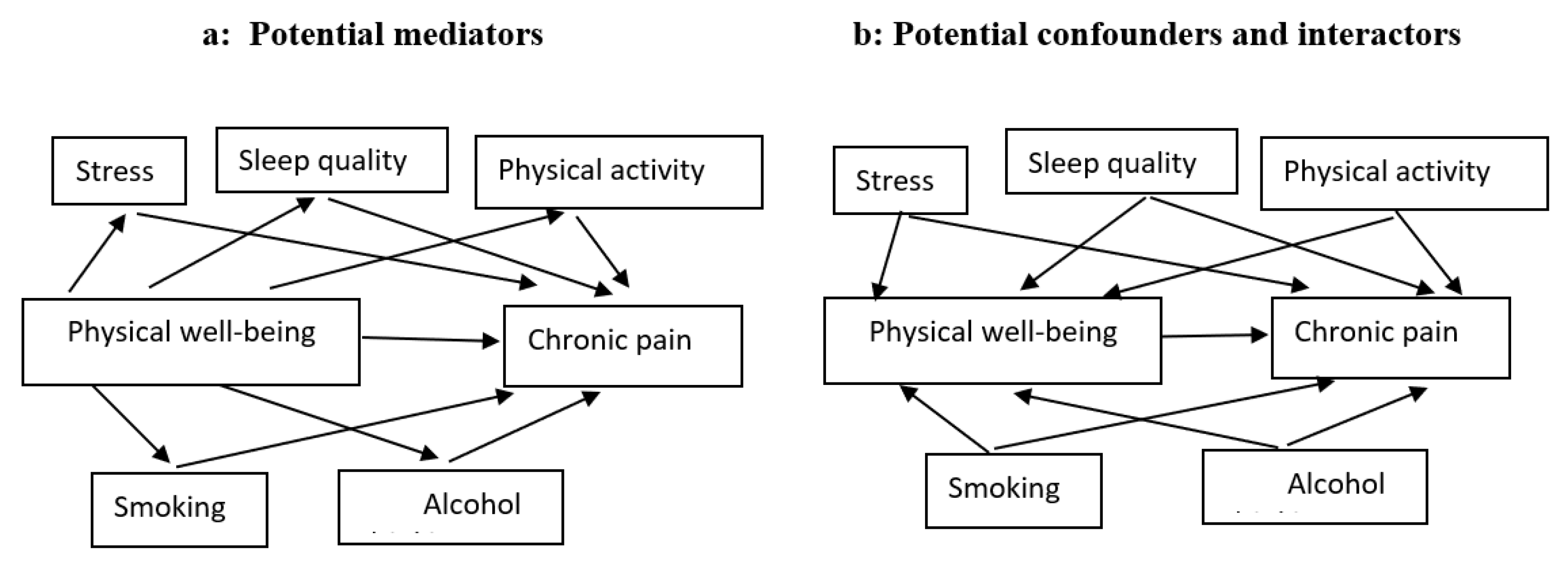
2.6. Mediation Analysis
2.7. Stratum-Specific Analysis
2.8. Interaction Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Mediation Analysis
3.3. Stratum-Specific Analysis
3.4. Interaction Analysis
4. Discussion
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garland, E.L. Pain Processing in the Human Nervous System: A Selective Review of Nociceptive and Biobehavioral Pathways. Prim. Care: Clin. Off. Pr. 2012, 39, 561–571. [Google Scholar] [CrossRef]
- Niv, D.; Devor, M. Chronic Pain as a Disease in its Own Right. Pain Pr. 2004, 4, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Fayaz, A.; Croft, P.; Langford, R.M.; Donaldson, L.J.; Jones, G.T. Prevalence of chronic pain in the UK: A systematic review and meta-analysis of population studies. BMJ Open 2016, 6, e010364. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.B.; de la Vega, R.; Murphy, L.K.; Kashikar-Zuck, S.; Palermo, T.M. The prevalence of chronic pain in young adults: A systematic review and meta-analysis. Pain 2021, 163, e972–e984. [Google Scholar] [CrossRef]
- GDB. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- Martínez-Romero, M.T.; Cejudo, A.; de Baranda, P.S. Prevalence and Characteristics of Back Pain in Children and Adolescents from the Region of Murcia (Spain): ISQUIOS Programme. Int. J. Environ. Res. Public Health 2022, 19, 946. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Estado de Salud: Cifras Absolutas. Encuesta Europea de Salud. 2020. Available online: https://www.ine.es/dynt3/inebase/es/index.htm?type=pcaxis&path=/t15/p420/a2019/p01/&file=pcaxis. (accessed on 23 January 2023).
- Fagerlund, A.J.; Iversen, M.; Ekeland, A.; Moen, C.M.; Aslaksen, P.M. Blame it on the weather? The association between pain in fibromyalgia, relative humidity, temperature and barometric pressure. PLoS ONE 2019, 14, e0216902. [Google Scholar] [CrossRef]
- Orosa, J.A.; Costa, A.M.; Rodríguez-Fernández, A.; Roshan, G. Effect of climate change on outdoor thermal comfort in humid climates. J. Environ. Health Sci. Eng. 2014, 12, 46. [Google Scholar] [CrossRef]
- Dixon, W.G.; Beukenhorst, A.L.; Yimer, B.B.; Cook, L.; Gasparrini, A.; El-Hay, T.; Hellman, B.; James, B.; Vicedo-Cabrera, A.M.; Maclure, M.; et al. How the weather affects the pain of citizen scientists using a smartphone app. NPJ Digit. Med. 2019, 2, 105. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Indicadores de Calidad de Vida/Análisis multidimensional. Encuesta Europea de Salud. 2020. Available online: https://www.ine.es/ss/Satellite?c=Page&pagename=ProductosYServicios%2FPYSLayout&cid=1259947314645&L=0#27sc. (accessed on 23 January 2023).
- Henares-Montiel, J.; Ruiz-Pérez, I.; Sordo, L. Salud mental en España y diferencias por sexo y por comunidades autónomas. Gac. Sanit. 2019, 34, 114–119. [Google Scholar] [CrossRef] [PubMed]
- WHOQOL. The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Fillingim, R.B. Individual differences in pain: Understanding the mosaic that makes pain personal. Pain 2016, 158, S11–S18. [Google Scholar] [CrossRef] [PubMed]
- Niv, D.; Kreitler, S. Pain and Quality of Life. Pain Pr. 2001, 1, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Calman, K.C. Quality of life in cancer patients—An hypothesis. J. Med. Ethic. 1984, 10, 124–127. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J. Confounding and Effect Modification: Distribution and Measure. Epidemiol. Methods 2012, 1, 55–82. [Google Scholar] [CrossRef]
- Hafeman, D.M.; Schwartz, S. Opening the Black Box: A motivation for the assessment of mediation. Int. J. Epidemiol. 2009, 38, 838–845. [Google Scholar] [CrossRef]
- Wang, X.; Ji, X. Sample size estimation in clinical research: From randomized controlled trials to observational studies. Chest 2020, 158, S12–S20. [Google Scholar] [CrossRef]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretación de los cuestionarios de salud SF-36 y SF-12 en España: Componentes físico y mental. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Kosinski, M.; Turner-Bowker, D.; Gandek, B.; Keller, S.D. How to Score Version 2 of the SF-12(R) Health Survey (with a Supplement Documenting Version 1); Qualitymetric: Lincoln, RI, USA, 2002. [Google Scholar]
- Vázquez, C.; Alonso, R.; Garriga, M.; de Cos, A.; de la Cruz, J.; Fuentes-Jiménez, F.; Salas-Salvadó, J.; Mata, P. Validation of a food frequency questionnaire in Spanish patients with familial hypercholesterolaemia. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Muñoz, S.; Corella, C.; Abarca-Sos, A.; Zaragoza, J. Validation of three short physical activity questionnaires with accelerometers among university students in Spain. J. Sports Med. Phys. Fit. 2017, 57, 1660–1668. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef]
- Vallejo, M.A.; Vallejo-Slocker, L.; Fernández-Abascal, E.G.; Mañanes, G. Determining Factors for Stress Perception Assessed with the Perceived Stress Scale (PSS-4) in Spanish and Other European Samples. Front. Psychol. 2018, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.; Vansteelandt, S. Mediation Analysis with Multiple Mediators. Epidemiol. Methods 2014, 2, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Greenland, S. Basic methods for sensitivity analysis of biases. Int. J. Epidemiol. 1996, 25, 1107–1116. [Google Scholar] [CrossRef]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Knol, M.J.; VanderWeele, T.J.; Groenwold, R.H.H.; Klungel, O.H.; Rovers, M.M.; Grobbee, D.E. Estimating measures of interaction on an additive scale for preventive exposures. Eur. J. Epidemiol. 2011, 26, 433–438. [Google Scholar] [CrossRef]
- de Mutsert, R.; Jager, K.J.; Zoccali, C.; Dekker, F.W. The effect of joint exposures: Examining the presence of interaction. Kidney Int. 2009, 75, 677–681. [Google Scholar] [CrossRef]
- Karimi, R.; Mallah, N.; Nedjat, S.; Beasley, M.J.; Takkouche, B. Association between alcohol consumption and chronic pain: A systematic review and meta-analysis. Br. J. Anaesth. 2022, 129, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.W.; Hughes, R.A. Bootstrap inference for multiple imputation under uncongeniality and misspecification. Stat. Methods Med. Res. 2020, 29, 3533–3546. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2010, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap; CRC Press: Boca Raton, FL, USA, 1994. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Williams, J. Confidence Limits for the Indirect Effect: Distribution of the Product and Resampling Methods. Multivar. Behav. Res. 2004, 39, 99–128. [Google Scholar] [CrossRef] [PubMed]
- Heneweer, H.; Staes, F.; Aufdemkampe, G.; van Rijn, M.; Vanhees, L. Physical activity and low back pain: A systematic review of recent literature. Eur. Spine J. 2011, 20, 826–845. [Google Scholar] [CrossRef] [PubMed]
- Lindell, M.; Grimby-Ekman, A. Stress, non-restorative sleep, and physical inactivity as risk factors for chronic pain in young adults: A cohort study. PLoS ONE 2022, 17, e0262601. [Google Scholar] [CrossRef]
- Mills, S.E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- Shiri, R.; Karppinen, J.; Leino-Arjas, P.; Solovieva, S.; Viikari-Juntura, E. The Association between Smoking and Low Back Pain: A Meta-analysis. Am. J. Med. 2010, 123, 87.e7–87.e35. [Google Scholar] [CrossRef]
- Van Hecke, O.; Torrance, N.; Smith, B.H. Chronic pain epidemiology—Where do lifestyle factors fit in? Br. J. Pain 2013, 7, 209–217. [Google Scholar] [CrossRef]
- Zale, E.L.; Maisto, S.A.; Ditre, J.W. Interrelations between pain and alcohol: An integrative review. Clin. Psychol. Rev. 2015, 37, 57–71. [Google Scholar] [CrossRef]
- Messlinger, K.; Funakubo, M.; Sato, J.; Mizumura, K. Increases in Neuronal Activity in Rat Spinal Trigeminal Nucleus Following Changes in Barometric Pressure-Relevance for Weather-Associated Headaches? Headache 2010, 50, 1449–1463. [Google Scholar] [CrossRef] [PubMed]
- Gabler, R.E.; Petersen, J.F.; Trapasso, L.M.; Sack, D. Physical Geography; Cengage Learning: Belmont, NC, USA, 2008; p. 679. [Google Scholar]
- Gago-Ageitos, A.M.; Durán-Maseda, M.J.; Vidal-Millares, M.; Ares-Durán, J.; Carballal-Mariño, M.; Mental Health Care for Children and Adolescents in Galicia (Spain). Differences between Different Regions in Spain. Communication Presented at the 19th World Psychiatric Association World Congress. Lisbon, Portugal 2019. Available online: https://www.morressier.com/o/event/5ca1d27b57558b317a13f5a3/article/5d1a038357558b317a140c8c (accessed on 3 February 2023).
- Fernández-Navarro, P.; Barrigón, M.L.; Lopez-Castroman, J.; Sanchez-Alonso, M.; Páramo, M.; Serrano, M.; Arrojo, M.; Baca-García, E. Suicide mortality trends in Galicia, Spain and their relationship with economic indicators. Epidemiol. Psychiatr. Sci. 2015, 25, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Mato, M.; Tsukasaki, K. Factors promoting sense of coherence among university students in urban areas of Japan: Individual-level social capital, self-efficacy, and mental health. Glob. Health Promot. 2017, 26, 60–68. [Google Scholar] [CrossRef]
- Ben-Ami, N.; Korn, L. Associations between backache and stress among undergraduate students. J. Am. Coll. Health 2018, 68, 61–67. [Google Scholar] [CrossRef]
- Bergenheim, A.; Juhlin, S.; Nordeman, L.; Joelsson, M.; Mannerkorpi, K. Stress levels predict substantial improvement in pain intensity after 10 to 12 years in women with fibromyalgia and chronic widespread pain: A cohort study. BMC Rheumatol. 2019, 3, 21. [Google Scholar] [CrossRef] [PubMed]
- Bottos, S.; Dewey, D. Perfectionists’ Appraisal of Daily Hassles and Chronic Headache. J. Headache Face Pain 2004, 44, 772–779. [Google Scholar] [CrossRef]
- Abdallah, C.G.; Geha, P. Chronic Pain and Chronic Stress: Two Sides of the Same Coin? Chronic Stress 2017, 1, 247054701770476. [Google Scholar] [CrossRef]
- Schultchen, D.; Reichenberger, J.; Mittl, T.; Weh, T.R.M.; Smyth, J.M.; Blechert, J.; Pollatos, O. Bidirectional relationship of stress and affect with physical activity and healthy eating. Br. J. Health Psychol. 2019, 24, 315–333. [Google Scholar] [CrossRef]
- Bobinski, F.; Ferreira, T.A.A.; Córdova, M.M.; Dombrowski, P.A.; da Cunha, C.; Santo, C.C.d.E.; Poli, A.; Pires, R.G.W.; Martins-Silva, C.; Sluka, K.A.; et al. Role of brainstem serotonin in analgesia produced by low-intensity exercise on neuropathic pain after sciatic nerve injury in mice. Pain 2015, 156, 2595–2606. [Google Scholar] [CrossRef]
- Sluka, K.A.; O’Donnell, J.M.; Danielson, J.; Rasmussen, L.A.; Jones, M.D.; Taylor, J.L.; Barry, B.K.; Zucker, I.H.; Schultz, H.D.; Patel, K.P.; et al. Regular physical activity prevents development of chronic pain and activation of central neurons. J. Appl. Physiol. 2013, 114, 725–733. [Google Scholar] [CrossRef]
- Stagg, N.J.; Mata, B.H.P.; Ibrahim, M.M.; Henriksen, E.J.; Porreca, F.; Vanderah, T.W.; Malan, T.P. Regular Exercise Reverses Sensory Hypersensitivity in a Rat Neuropathic Pain Model. Anesthesiology 2011, 114, 940–948. [Google Scholar] [CrossRef]
- Chastain, G. Alcohol, Neurotransmitter Systems, and Behavior. J. Gen. Psychol. 2006, 133, 329–335. [Google Scholar] [CrossRef] [PubMed]
- McGee, R.; Williams, S.; Nada-Raja, S.; Olsson, C.A. Tobacco Smoking in Adolescence Predicts Maladaptive Coping Styles in Adulthood. Nicotine Tob. Res. 2013, 15, 1971–1977. [Google Scholar] [CrossRef]
- Rimmele, U.; Seiler, R.; Marti, B.; Wirtz, P.H.; Ehlert, U.; Heinrichs, M. The level of physical activity affects adrenal and cardiovascular reactivity to psychosocial stress. Psychoneuroendocrinology 2009, 34, 190–198. [Google Scholar] [CrossRef]
- Gonzalez, V.M.; Bradizza, C.M.; Collins, R.L. Drinking to cope as a statistical mediator in the relationship between suicidal ideation and alcohol outcomes among underage college drinkers. Psychol. Addict. Behav. 2009, 23, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Balodis, I.M.; Wynne-Edwards, K.E.; Olmstead, M.C. The stress–response-dampening effects of placebo. Horm. Behav. 2011, 59, 465–472. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Exposure | Physical Well-Being (Physical Component Summary) | |
|---|---|---|
| Low Mean = 48.4 (n = 154) | High Mean = 58.07 (n = 460) | |
| Age; mean (SD) | 24.95 (6.2) | 24.61 (6.1) |
| Sex; n (%) | ||
| Male | 37 (24.50) | 93 (20.53) |
| Female | 114 (75.50) | 360 (79.47) |
| Physical activity; n (%) | ||
| High | 34 (21.12) | 127 (78.88) |
| Low | 108 (25.29) | 319 (74.71) |
| Perceived stress; n (%) | ||
| High (>8) | 88 (26.91) | 239 (73.09) |
| Low (<8) | 41 (17.01) | 200 (82.99) |
| Smoking; n (%) | ||
| Non-current smokers | 112 (22.72) | 381 (77.28) |
| Current smokers | 42 (34.71) | 79 (65.29) |
| Alcohol consumption; n (%) | ||
| Abstainers/low drinkers | 25 (25.77) | 72 (74.23) |
| Moderate drinkers | 30 (21.90) | 107 (78.10) |
| Sleep quality; n (%) | ||
| Low >5 | 56 (52.83) | 149 (36.97) |
| High <5 | 50 (47.17) | 254 (63.03) |
| Mediator | Unadjusted | Adjusted a | ||||||
|---|---|---|---|---|---|---|---|---|
| Natural Indirect Effect | Natural Direct Effect | Natural Total Effect | Proportion Mediated, % | Natural Indirect Effect | Natural Direct Effect | Natural Total Effect | Proportion Mediated, % | |
| IRR (95% CI) | IRR (95% CI) | IRR (95% CI) | IRR a (95% CI) | IRR a (95% CI) | IRR a (95% CI) | |||
| Physical activity (low vs. high) | 0.97 (0.87, 1.07) | 0.64 (0.45, 0.79) | 0.60 (0.44, 0.81) | 5.1 | 0.96 (0.85, 1.09) | 0.63 (0.50, 0.82) | 0.59 (0.49, 0.82) | 6.4 |
| Perceived stress (low vs. high) | 0.94 (0.91, 1.03) | 0.63 (0.45, 0.77) | 0.59 (0.46, 0.92) | 9.3 | 0.92 (0.89, 1.00) | 0.64 (0.48, 0.81) | 0.58 (0.50, 0.81) | 12.5 |
| Smoking (non-current vs. current) | 0.98 (0.89, 1.05) | 0.62 (0.45, 0.80) | 0.60 (0.44, 0.80) | 3.2 | 0.97 (0.84, 1.07) | 0.63 (0.49, 0.79) | 0.60 (0.50, 0.78) | 4.8 |
| Drinking (abstainers/low vs. moderate) | 1.02 (0.86, 1.15) | 0.63 (0.44, 0.80) | 0.60 (0.48, 0.82) | −3.5 | 1.03 (0.83, 1.16) | 0.63 (0.48, 0.78) | 0.65 (0.50, 0.79) | −5.3 |
| Sleep quality (good vs. poor) | 0.98 (0.84, 1.10) | 0.63 (0.48, 0.81) | 0.61 (0.47, 0.80) | 3.3 | 0.98 0.93, 1.07) | 0.64 (0.48, 0.84) | 0.62 (0.49, 0.85) | 3.4 |
| Covariates | Stratum-Specific IRR | IRR Crude | IRR Pooled |
|---|---|---|---|
| Low physical activity | 1.76 (1.28, 2.36) | 1.49 (1.24, 1.80) | 1.51 (1.20, 1.90) |
| High physical activity | 1.20 (1.06, 1.45) | ||
| Low stress | 1.27 (1.30, 1.79) | 1.49 (1.24, 1.80) | 1.47 (1.16, 1.86) |
| High stress | 1.68 (1.22, 2.32) | ||
| Non-current smokers | 1.80 (1.05, 2.81) | 1.49 (1.24, 1.80) | 1.59 (1.39, 1.62) |
| Current smokers | 1.52 (1.35, 1.62) | ||
| Low/non-drinkers | 1.59 (1.19, 2.75) | 1.49 (1.24, 1.80) | 1.44 (1.22, 1.58) |
| Moderate drinkers | 1.44 (1.10, 1.58) | ||
| Low sleep quality | 1.54 (1.01, 2.26) | 1.49 (1.24, 1.80) | 1.50 (1.13, 1.98) |
| High sleep quality | 1.52 (0.97, 2.20) |
| Interaction | Adjusted * IRR (95% CI) | Univariate RERI (95% CI) | Adjusted RERI * (95% CI) | AP (95% CI) | S (95% CI) |
|---|---|---|---|---|---|
| Physical activity/physical well-being | 0.25 (0.13, 0.60) | 0.27 (0.12, 0.51) | 0.19 (0.13, 0.58) | 3.79 (1.29, 7.84) | |
| High activity, high well-being | 1 (ref) | ||||
| Low activity, high well-being | 0.89 (0.77, 1.04) | ||||
| High activity, low well-being | 1.20 (1.06, 1.45) | ||||
| Low activity, low well-being | 1.34 (1.07, 1.59) | ||||
| Perceived stress/physical well-being | 0.02 (−0.89, 0.16) | 0.01(−0.92, 0.17) | 0.02(−0.83, 0.23) | 1.07 (0.59, 1.27) | |
| Low stress, high well-being | 1 (ref) | ||||
| High stress, high well-being | 1.03 (0.73, 1.09) | ||||
| Low stress, low well-being | 1.27 (1.30, 1.79) | ||||
| High stress, low well-being | 1.37 (0.79, 1.10) | ||||
| Smoking status/physical well-being | −0.07 (−0.15, 0.01) | −0.04 (−0.24, 0.10) | −0.08 (−0.10, 0.11) | 0.64 (0.32, 0.70) | |
| Non-current smokers, high well-being | 1 (ref) | ||||
| Smokers, high well-being | 0.74 (0.45, 1.30) | ||||
| Non-current smokers, low well-being | 1.52 (1.35, 1.62) | ||||
| Smokers, low well-being | 1.17 (0.92, 1.26) | ||||
| Drinking status/physical well-being | 0.11 (0.06, 0.36) | 0.09 (0.04, 0.28) | 0.08 (0.05, 0.30) | 1.81 (1.51, 2.12) | |
| Moderate drinkers, high well-being | 1 (ref) | ||||
| Abstainers, high well-being | 0.68 (0.56, 0.81) | ||||
| Moderate drinkers, low well-being | 1.44 (1.10, 1.58) | ||||
| Abstainers, low well-being | 1.24 (1.12, 1.36) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karimi, R.; Prego-Domínguez, J.; Takkouche, B. Factors Contributing to the Link between Physical Well-Being and Chronic Pain in Young People from Galicia, Northwest Spain. J. Clin. Med. 2023, 12, 4228. https://doi.org/10.3390/jcm12134228
Karimi R, Prego-Domínguez J, Takkouche B. Factors Contributing to the Link between Physical Well-Being and Chronic Pain in Young People from Galicia, Northwest Spain. Journal of Clinical Medicine. 2023; 12(13):4228. https://doi.org/10.3390/jcm12134228
Chicago/Turabian StyleKarimi, Roya, Jesús Prego-Domínguez, and Bahi Takkouche. 2023. "Factors Contributing to the Link between Physical Well-Being and Chronic Pain in Young People from Galicia, Northwest Spain" Journal of Clinical Medicine 12, no. 13: 4228. https://doi.org/10.3390/jcm12134228
APA StyleKarimi, R., Prego-Domínguez, J., & Takkouche, B. (2023). Factors Contributing to the Link between Physical Well-Being and Chronic Pain in Young People from Galicia, Northwest Spain. Journal of Clinical Medicine, 12(13), 4228. https://doi.org/10.3390/jcm12134228