

Optimizing Patient Care: A Systematic Review of Multidisciplinary Approaches for SLE Management

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics of Patients Included
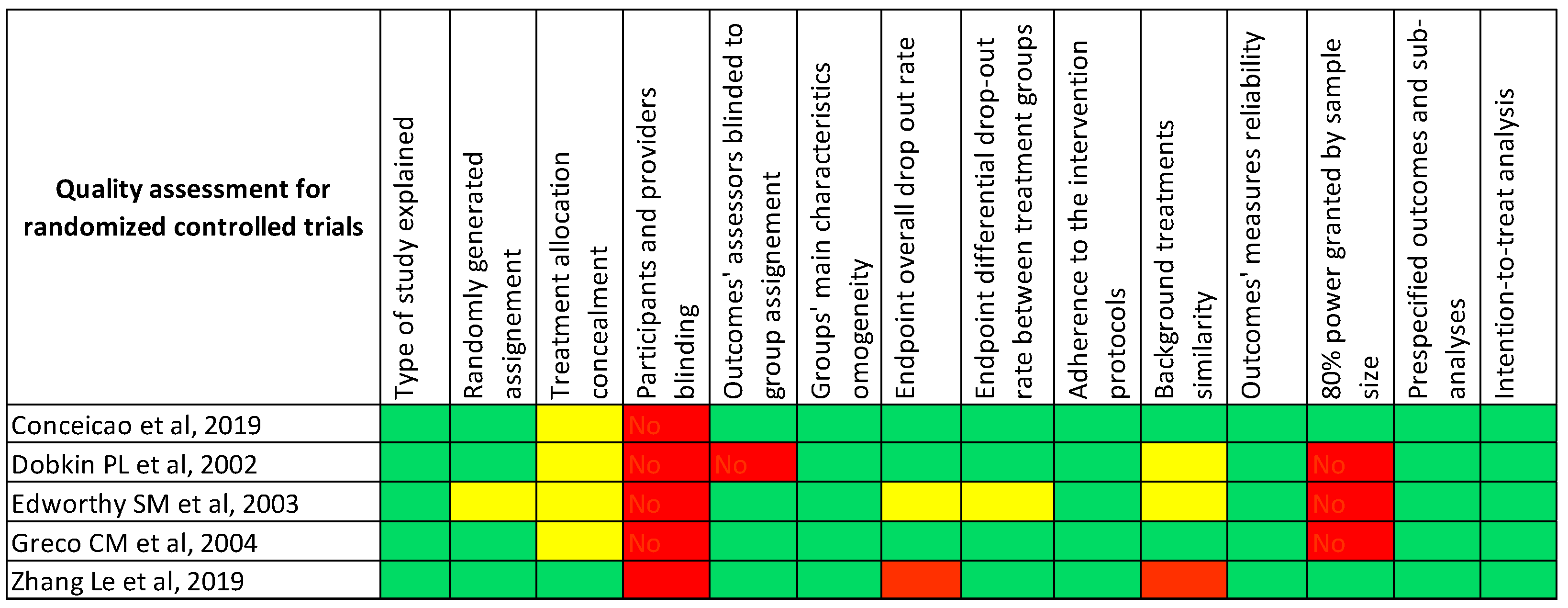
3.2. Risk of Bias
3.3. Composition of the MD Team
3.4. Characteristics of MD Intervention
3.5. Outcomes Evaluated
3.5.1. Pregnancy Outcomes
3.5.2. Disease Activity
3.5.3. Patient-Reported Outcomes
3.5.4. Other Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kiriakidou, M.; Ching, C.L. Systemic Lupus Erythematosus. Ann. Intern. Med. 2020, 172, ITC81–ITC96. [Google Scholar] [CrossRef]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat. Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLOS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Low, E.S.H.; Krishnaswamy, G.; Thumboo, J. Comparing the 1997 update of the 1982 American College of Rheumatology (ACR-97) and the 2012 Systemic Lupus International Collaborating Clinics (SLICC-12) criteria for systemic lupus erythematosus (SLE) classification: Which enables earlier classification of SLE in an urban Asian population? Lupus 2019, 28, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 1151–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petri, M.; Orbai, A.-M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef]
- Study Quality Assessment Tools. NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 20 January 2023).
- Conceição, C.T.M.; Meinão, I.M.; Bombana, J.A.; Sato, E.I. Psychoanalytic psychotherapy improves quality of life, depression, anxiety and coping in patients with systemic lupus erythematosus: A controlled randomized clinical trial. Hortic. Bras. 2019, 59, 4. [Google Scholar] [CrossRef] [Green Version]
- Dobkin, P.L.; Da Costa, D.; Joseph, L.; Fortin, P.R.; Edworthy, S.; Barr, S.; Ensworth, S.; Esdaile, J.M.; Beaulieu, A.; Zummer, M.; et al. Counterbalancing patient demands with evidence: Results from a pan-canadian randomized clinical trial of brief supportive-expressive group psychotherapy for women with systemic lupus erythematosus. Ann. Behav. Med. 2002, 24, 88–99. [Google Scholar] [CrossRef]
- Edworthy, S.M.; Dobkin, P.L.; Clarke, A.E.; Da Costa, D.; Dritsa, M.; Fortin, P.R.; Barr, S.; Ensworth, S.; Esdaile, J.M.; Beaulieu, A.; et al. Group psychotherapy reduces illness intrusiveness in systemic lupus erythematosus. J. Rheumatol. 2003, 30, 1011–1016. [Google Scholar]
- Greco, C.M.; Rudy, T.E.; Manzi, S. Effects of a stress-reduction program on psychological function, pain, and physical function of systemic lupus erythematosus patients: A randomized controlled trial. Arthritis Rheum. 2004, 51, 625–634. [Google Scholar] [CrossRef]
- Zhang, L.; Geng, S.; Qian, L.; Ye, S.; Wang, X.; Lu, G.; Ding, Y.; Li, T. Multidisciplinary care in patients with systemic lupus erythematosus: A randomized controlled trial in China. Int. J. Clin. Pharm. 2019, 41, 1247–1255. [Google Scholar] [CrossRef]
- Añón-Oñate, I.; Cáliz-Cáliz, R.; Rosa-Garrido, C.; Pérez-Galán, M.J.; Quirosa-Flores, S.; Pancorbo-Hidalgo, P.L. Multidisciplinary Unit Improves Pregnancy Outcomes in Women with Rheumatic Diseases and Hereditary Thrombophilias: An Observational Study. J. Clin. Med. 2021, 10, 1487. [Google Scholar] [CrossRef]
- Ambrósio, P.; Lermann, R.; Cordeiro, A.; Borges, A.; Nogueira, I.; Serrano, F. Lupus and Pregnancy—15 Years of Experience in a Tertiary Center. Clin. Rev. Allergy Immunol. 2010, 38, 77–81. [Google Scholar] [CrossRef]
- Bowers, E.; Griffith, M.; Weinstein, E.; Pearson, D.; Kolfenbach, J. A quality improvement intervention to reduce 30-day hospital readmission rates among patients with systemic lupus erythematosus. Arthritis Rheumatol. 2019, 71, 2090–2091. [Google Scholar] [CrossRef]
- Brucato, A.; Doria, A.; Frassi, M.; Castellino, G.; Franceschini, F.; Faden, D.; Pisoni, M.P.; Solerte, L.; Muscarà, M.; Lojacono, A.; et al. Pregnancy outcome in 100 women with autoimmune diseases and anti-Ro/SSA antibodies: A prospective controlled study. Lupus 2002, 11, 716–721. [Google Scholar] [CrossRef]
- Carmona, F.; Font, J.; Cervera, R.; Muñoz, F.; Cararach, V.; Balasch, J. Obstetrical outcome of pregnancy in patients with systemic Lupus Erythematosus. A study of 60 cases. Eur. J. Obstet. Gynecol. Reprod. Biol. 1999, 83, 137–142. [Google Scholar] [CrossRef]
- Ceccarelli, F.; Pirone, C.; Perricone, C.; Selntigia, A.; Orefice, V.; Pacucci, V.A.; Truglia, S.; Spinelli, F.R.; Galoppi, P.; Alessandri, C.; et al. Pregnancy outcome in systemic lupus erythematosus patients: A monocentric cohort analysis. Rheumatology 2021, 60, 1747–1754. [Google Scholar] [CrossRef] [PubMed]
- Lima, F.; Buchanan, N.M.; Khamashta, M.A.; Kerslake, S.; Hughes, G.R. Obstetric outcome in systemic lupus erythematosus. Semin. Arthritis Rheum. 1995, 25, 184–192. [Google Scholar] [CrossRef]
- Magro-Checa, C.; Zirkzee, E.J.; De Voorde, L.J.B.-V.; Middelkoop, H.A.; Van Der Wee, N.J.; Huisman, M.V.; Eikenboom, J.; Kruyt, N.D.; Van Buchem, M.A.; Huizinga, T.W.; et al. Value of multidisciplinary reassessment in attribution of neuropsychiatric events to systemic lupus erythematosus: Prospective data from the Leiden NPSLE cohort. Rheumatology 2017, 56, 1676–1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mecacci, F.; Simeone, S.; Cirami, C.L.; Cozzolino, M.; Serena, C.; Rambaldi, M.P.; Gallo, P.; Emmi, L.; Cammelli, D.; Mello, G.; et al. Preeclampsia in pregnancies complicated by systemic lupus erythematosus (SLE) nephritis: Prophylactic treatment with multidisciplinary approach are important keys to prevent adverse obstetric outcomes. J. Matern. Fetal Neonatal Med. 2019, 32, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Mintz, G.; Niz, J.; Gutierrez, G.; Garcia-Alonso, A.; Karchmer, S. Prospective study of pregnancy in systemic lupus erythematosus. Results of a multidisciplinary approach. J. Rheumatol. 1986, 13, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.N.; Taber, K.; Huang, W.; Collins, J.; Cunningham, R.; McLaughlin, K.; Vogeli, C.; Wichmann, L.; Feldman, C.H. The Impact of an Integrated Care Management Program on Acute Care Use and Outpatient Appointment Attendance Among High-Risk Patients With Lupus. ACR Open Rheumatol. 2022, 4, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Wind, M.; Hendriks, M.; van Brussel, B.T.J.; Eikenboom, J.; Allaart, C.F.; Lamb, H.J.; Siebelink, H.-M.J.; Ninaber, M.K.; van Geloven, N.; van Lith, J.M.M.; et al. Effectiveness of a multidisciplinary clinical pathway for women with systemic lupus erythematosus and/or antiphospholipid syndrome. Lupus Sci. Med. 2021, 8, e000472. [Google Scholar] [CrossRef] [PubMed]
- Zirkzee, E.J.; Steup-Beekman, G.M.; Van Der Mast, R.C.; Bollen, E.L.; Van Der Wee, N.J.A.; Baptist, E.; Slee, T.M.; Huisman, M.V.; Middelkoop, H.A.; Luyendijk, J.; et al. Prospective Study of Clinical Phenotypes in Neuropsychiatric Systemic Lupus Erythematosus; Multidisciplinary Approach to Diagnosis and Therapy. J. Rheumatol. 2012, 39, 2118–2126. [Google Scholar] [CrossRef]
- Giancotti, A.; Spagnuolo, A.; D’Ambrosio, V.; Pasquali, G.; Muto, B.; De Gado, F. Pregnancy in lupus patients: Our experience. Minerva Obstet. Gynecol. 2010, 62, 551–558. [Google Scholar]
- Conceicao, C.; Meinao, I.; Blay, S.; Sato, E. Brief group psychoanalytic psychotherapy improves qualityof life in patientswith systemic lupus erythematosus: A long-term follow-up study. J. Clin. Rheumatol. 2018, 24, S21. [Google Scholar]
- Romero-Diaz, J.; Isenberg, D.; Ramsey-Goldman, R. Measures of adult systemic lupus erythematosus: Updated version of British Isles Lupus Assessment Group (BILAG 2004), European Consensus Lupus Activity Measurements (ECLAM), Systemic Lupus Activity Measure, Revised (SLAM-R), Systemic Lupus Activity Questionnaire for Population Studies (SLAQ), Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K), and Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SDI). Arthritis Care Res. 2011, 63 (Suppl. 11), S37–S46. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Leong, K.P.; Kong, K.O.; Thong, B.; Koh, E.T.; Lian, T.Y.; Teh, C.L.; Cheng, Y.K.; Chng, H.H.; Badsha, H.; Law, W.G.; et al. Development and preliminary validation of a systemic lupus erythematosus-specific quality-of-life instrument (SLEQOL). Rheumatology 2005, 44, 1267–1276. [Google Scholar] [CrossRef] [Green Version]
- Fanouriakis, A.; Kostopoulou, M.; Cheema, K.; Anders, H.-J.; Aringer, M.; Bajema, I.; Boletis, J.; Frangou, E.; Houssiau, F.A.; Hollis, J.; et al. 2019 Update of the Joint European League Against Rheumatism and European Renal Association–European Dialysis and Transplant Association (EULAR/ERA–EDTA) recommendations for the management of lupus nephritis. Ann. Rheum. Dis. 2020, 79, 713–723. [Google Scholar] [CrossRef] [Green Version]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [Green Version]
- Talarico, R.; Cannizzo, S.; Lorenzoni, V.; Marinello, D.; Palla, I.; Pirri, S.; Ticciati, S.; Trieste, L.; Triulzi, I.; Terol, E.; et al. RarERN Path: A methodology towards the optimisation of patients’ care pathways in rare and complex diseases developed within the European Reference Networks. Orphanet J. Rare Dis. 2020, 15, 347. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; Mcleod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year, Type of Study | Number of Participants, Intervention |Control | Mean Age (Years), Intervention |Control | Mean Disease Duration (Months), Intervention |Control | Physicians Involved in the MD Team (Non-Medical Professionals) | Type of Intervention | Outcome |
|---|---|---|---|---|---|---|
| Conceicao, 2019, RCT [8] | 80, 37|43 | 42|42.7 | 148|139 | Rheumatologist, Psychologist | Group psychotherapy | SLEDAI; SLICC-ACR-DI; SLEQOL |
| Dobkin PL, 2002, RCT [9] | 133, 64|69 | 42|43 | 136|126 | Rheumatologist, Psychologist | Group psychotherapy | Disease activity, health quality, social and psychological support |
| Edworthy, 2003, RCT [10] | 124, 58|66 | 42.5, 42|43 | 130, 137|126 | Rheumatologist, Psychologist | Group psychotherapy | SLAM; illness intrusiveness |
| Greco, 2004, RCT [11] | 92, 32|60 | 48.2|47 | 120|96 | Rheumatologist, Psychologist | Biofeedback cognitive behavioral treatment | SLAM; SF-36; pain (AIMS2-Pain); depression (CES-D) |
| Zhang LE, 2019, RCT [12] | 82, 42|40 | 31.5|30.3 | - | Rheumatologist, (Pharmacist, Nurse) | Pharmacist-led multidisciplinary care | SLEDAI, SLICC-SDI, quality of life, and patient-reported outcomes |
| Anon, 2021, RC [13] | 49 | - | - | Rheumatologist, Gynecologist | Clinical, laboratory, and instrumental pregnancy follow-up by a rheumatological–gynecological team | Materno-fetal outcomes |
| Ambrosio, 2010, RC [14] | 107 | 29 | 75.6 | Rheumatologist, Obstetricians | Clinical, laboratory, and instrumental pregnancy follow-up by a rheumatological–gynecological team | Pregnancy complications, delivery outcome, newborn outcome |
| Bowers E, 2019, PC [15] | 104, 56|48 | 39.4|43.4 | - | Rheumatologist, Faculty Physician (Nurse) | Phone call by a nurse 48 h after hospital discharge | Hospital readmission rate |
| Brucato A, 2002, RC-PC [16] | 111 | - | - | Rheumatologist, Gynecologist | Clinical, laboratory, and instrumental pregnancy follow-up by a rheumatological–gynecological team | Obstetric and fetal outcomes, flares during pregnancy |
| Carmona F, 1999, PC [17] | 46 | 28.6 | 75 | Rheumatologist, Obstetricians | MD approach during pregnancy | Obstetric outcomes, flares during pregnancy |
| Ceccarelli F, 2021, PC [18] | 150, 50|100 | 33|31 | 72 | Rheumatologist, Gynecologist | Pre-gestational counseling and a multidisciplinary approach during pregnancy | Obstetric and fetal outcomes, disease activity |
| Lima, 1995, PC [19] | 90 | 30.7 | 76 | Rheumatologist, Gynecologist, Hematologist | Clinical, laboratory, and instrumental pregnancy follow-up by a rheumatological–gynecological team | Fetal outcomes: successful pregnancies, prematurity, IUGR. Maternal outcomes: SLE flares |
| Magro-Checa, 2017, PC [20] | 304 | 42.5 | 55.2 | Rheumatologist, Neurologist, Psychiatrist, Vascular Physician | MD assessment in suspected NPSLE | Correct attributions of NP events |
| Mecacci F, 2019, RC [21] | 86, 27|59 | 32.1|34.1 | 99.6|68.4 | Rheumatologist, Gynecologist, Nephrologist | Clinical, laboratory, and instrumental pregnancy follow-up by a rheumatological–gynecological team | Disease flare (especially renal), maternal–fetal outcomes (especially preeclampsia and IUGR) |
| Mintz G, 1986, PC [22] | 225, 102|123 | 27.2|30.3 | 58.8|- | Rheumatologist, Gynecologist, Neonatologist | Clinical, laboratory, and instrumental pregnancy follow-up by a rheumatological–gynecological team | Disease activity (clinically attested), maternal–fetal outcomes |
| Williams J, 2022, PC [23] | 67 | 60 | 180 | Rheumatologist (only if needed), (Nurse, Pharmacist, Community Resource Specialist) | Referral of the patient to the most appropriate professional | Risk of potentially avoidable healthcare service use |
| Wind M, 2021, RC-PC [24] | 78, 30|48 | 32|31 | 108|108 | Rheumatologist, Gynecologist, Nephrologist, Hematologist | Clinical, laboratory, and instrumental pregnancy follow-up by a rheumatological–gynecological team | Disease flares and maternal–fetal outcomes |
| Zerkzee EJM, 2012, PC [25] | 71 | 42 | 101 | Rheumatologist, Neuropsychologist, Neurologist, Psychiatric, Radiologist, and Resident in Internal Medicine | MD assessment in suspected NPSLE | Diagnosis of neuropsychiatric SLE and classification into 3 different phenotypes (ischemic, inflammatory, and undefined) |
| Giancotti, 2010, CS [26] | 20 | 32.9 | 104.16 | Rheumatologist, Gynecologist | Clinical, laboratory, and instrumental pregnancy follow-up by a rheumatological–gynecological team | Maternal outcomes: number of SLE flares |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galoppini, G.; Marangoni, A.; Cirilli, F.; Ruffilli, F.; Garaffoni, C.; Govoni, M.; Scirè, C.A.; Silvagni, E.; Bortoluzzi, A. Optimizing Patient Care: A Systematic Review of Multidisciplinary Approaches for SLE Management. J. Clin. Med. 2023, 12, 4059. https://doi.org/10.3390/jcm12124059
Galoppini G, Marangoni A, Cirilli F, Ruffilli F, Garaffoni C, Govoni M, Scirè CA, Silvagni E, Bortoluzzi A. Optimizing Patient Care: A Systematic Review of Multidisciplinary Approaches for SLE Management. Journal of Clinical Medicine. 2023; 12(12):4059. https://doi.org/10.3390/jcm12124059
Chicago/Turabian StyleGaloppini, Giorgio, Antonio Marangoni, Francesca Cirilli, Francesca Ruffilli, Carlo Garaffoni, Marcello Govoni, Carlo Alberto Scirè, Ettore Silvagni, and Alessandra Bortoluzzi. 2023. "Optimizing Patient Care: A Systematic Review of Multidisciplinary Approaches for SLE Management" Journal of Clinical Medicine 12, no. 12: 4059. https://doi.org/10.3390/jcm12124059
APA StyleGaloppini, G., Marangoni, A., Cirilli, F., Ruffilli, F., Garaffoni, C., Govoni, M., Scirè, C. A., Silvagni, E., & Bortoluzzi, A. (2023). Optimizing Patient Care: A Systematic Review of Multidisciplinary Approaches for SLE Management. Journal of Clinical Medicine, 12(12), 4059. https://doi.org/10.3390/jcm12124059