
The Correlation of Sleep Disturbance and Location of Glioma Tumors: A Narrative Review


 and
and 
Abstract
:1. Introduction
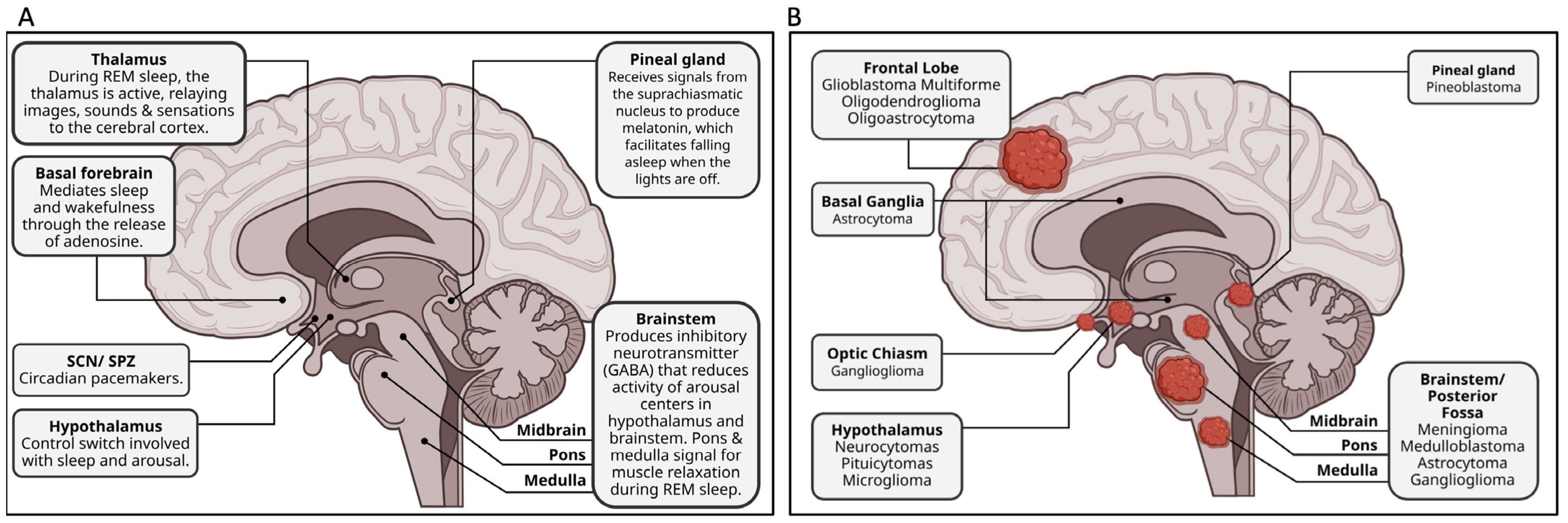
2. Brain Areas Implicated in Sleep Disturbance
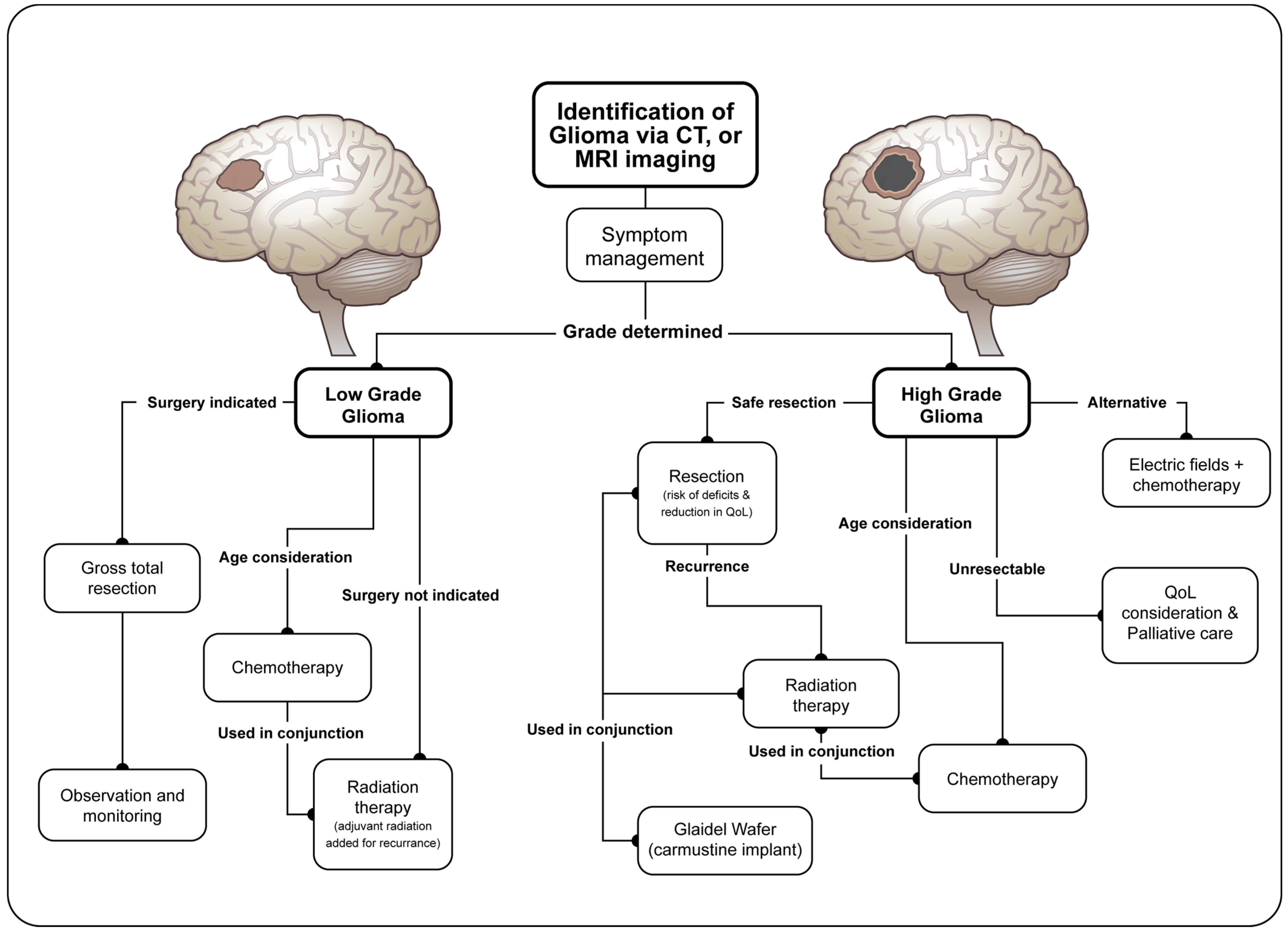
3. Characterization and Treatment of Gliomas
4. Correlation of Tumor Location and Sleep Disturbance
4.1. Sleep Apnea
4.2. Hypersomnia
4.3. Narcolepsy
4.4. Parasomnias
4.5. Insomnia
4.6. Other Brain Disorders
5. Future Considerations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zisapel, N. Sleep and sleep disturbances: Biological basis and clinical implications. Cell. Mol. Life Sci. 2007, 64, 1174–1186. [Google Scholar] [CrossRef] [PubMed]
- Sullan, M.J.; Asken, B.M.; Jaffee, M.S.; DeKosky, S.T.; Bauer, R.M. Glymphatic system disruption as a mediator of brain trauma and chronic traumatic encephalopathy. Neurosci. Biobehav. Rev. 2018, 84, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Hermann, D.M.; Bassetti, C.L. Sleep-related breathing and sleep-wake disturbances in ischemic stroke. Neurology 2009, 73, 1313–1322. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.L. Psychiatric disorders and sleep issues. Med. Clin. 2014, 98, 1123–1143. [Google Scholar] [CrossRef]
- Davidson, J.R.; MacLean, A.W.; Brundage, M.D.; Schulze, K. Sleep disturbance in cancer patients. Soc. Sci. Med. 2002, 54, 1309–1321. [Google Scholar] [CrossRef]
- Meltzer, L.J.; Mindell, J.A. Sleep and sleep disorders in children and adolescents. Psychiatr. Clin. 2006, 29, 1059–1076. [Google Scholar] [CrossRef]
- Sampasa-Kanyinga, H.; Colman, I.; Goldfield, G.S.; Janssen, I.; Wang, J.; Podinic, I.; Tremblay, M.S.; Saunders, T.J.; Sampson, M.; Chaput, J.-P. Combinations of physical activity, sedentary time, and sleep duration and their associations with depressive symptoms and other mental health problems in children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 72. [Google Scholar] [CrossRef]
- Hauglund, N.L.; Pavan, C.; Nedergaard, M. Cleaning the sleeping brain–the potential restorative function of the glymphatic system. Curr. Opin. Physiol. 2020, 15, 1–6. [Google Scholar] [CrossRef]
- Vyazovskiy, V.V. Sleep, recovery, and metaregulation: Explaining the benefits of sleep. Nat. Sci. Sleep 2015, 7, 171–184. [Google Scholar] [CrossRef] [Green Version]
- Blask, D.E. Melatonin, sleep disturbance and cancer risk. Sleep Med. Rev. 2009, 13, 257–264. [Google Scholar] [CrossRef]
- Strollo, S.E.; Fallon, E.A.; Gapstur, S.M.; Smith, T.G. Cancer-related problems, sleep quality, and sleep disturbance among long-term cancer survivors at 9-years post diagnosis. Sleep Med. 2020, 65, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Fox, I.K.; Brenner, M.J.; Johnson, P.J.; Hunter, D.A.; Mackinnon, S.E. Axonal regeneration and motor neuron survival after microsurgical nerve reconstruction. Microsurgery 2012, 32, 552–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, D.; Wang, M.; Chen, Y.; Gong, J.; Chen, L.; Shi, X.; Lan, F.; Chen, Z.; Xiong, T.; Sun, H. Trends in intracranial glioma incidence and mortality in the United States, 1975–2018. Front. Oncol. 2021, 11, 748061. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, T.S.; Shade, M.Y.; Breton, G.; Gilbert, M.R.; Mahajan, A.; Scheurer, M.E.; Vera, E.; Berger, A.M. Sleep-wake disturbance in patients with brain tumors. Neuro-Oncology 2017, 19, 323–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willis, K.D.; Ravyts, S.G.; Lanoye, A.; Loughan, A.R. Sleep disturbance in primary brain tumor: Prevalence, risk factors, and patient preferences. Support Care Cancer 2022, 30, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Sadighi, Z.S.; Curtis, E.; Zabrowksi, J.; Billups, C.; Gajjar, A.; Khan, R.; Qaddoumi, I. Neurologic impairments from pediatric low-grade glioma by tumor location and timing of diagnosis. Pediatr. Blood Cancer 2018, 65, e27063. [Google Scholar] [CrossRef]
- Hansen, A.; Pedersen, C.B.; Minet, L.R.; Beier, D.; Jarden, J.O.; Søgaard, K. Hemispheric tumor location and the impact on health-related quality of life, symptomatology, and functional performance outcomes in patients with glioma: An exploratory cross-sectional study. Disabil. Rehabil. 2021, 43, 1443–1449. [Google Scholar] [CrossRef]
- Subramanian, S.; Gholami, A.; Biros, G. Simulation of glioblastoma growth using a 3D multispecies tumor model with mass effect. J. Math. Biol. 2019, 79, 941–967. [Google Scholar] [CrossRef] [Green Version]
- Aranda, M.L.; Schmidt, T.M. Diversity of intrinsically photosensitive retinal ganglion cells: Circuits and functions. Cell. Mol. Life Sci. 2021, 78, 889–907. [Google Scholar] [CrossRef]
- Hattar, S.; Liao, H.-W.; Takao, M.; Berson, D.M.; Yau, K.-W. Melanopsin-containing retinal ganglion cells: Architecture, projections, and intrinsic photosensitivity. Science 2002, 295, 1065–1070. [Google Scholar] [CrossRef] [Green Version]
- Lu, Q.; Kim, J.Y. Mammalian circadian networks mediated by the suprachiasmatic nucleus. FEBS J. 2022, 289, 6589–6604. [Google Scholar] [CrossRef] [PubMed]
- Hastings, M.; Brancaccio, M.; Maywood, E. Circadian pacemaking in cells and circuits of the suprachiasmatic nucleus. J. Neuroendocrinol. 2014, 26, 2–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.W.; Zhang, X.; Huang, W.J. Pain control by melatonin: Physiological and pharmacological effects. Exp. Ther. Med. 2016, 12, 1963–1968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mander, B.A.; Winer, J.R.; Walker, M.P. Sleep and human aging. Neuron 2017, 94, 19–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, J.M. The neurotransmitters of sleep. J. Clin. Psychiatry 2004, 65, 4–7. [Google Scholar]
- Brown, R.E.; Basheer, R.; McKenna, J.T.; Strecker, R.E.; McCarley, R.W. Control of sleep and wakefulness. Physiol. Rev. 2012, 92, 1087–1187. [Google Scholar] [CrossRef] [Green Version]
- Weber, F.; Dan, Y. Circuit-based interrogation of sleep control. Nature 2016, 538, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Gerashchenko, D.; Shiromani, P.J. Different neuronal phenotypes in the lateral hypothalamus and their role in sleep and wakefulness. Mol. Neurobiol. 2004, 29, 41–59. [Google Scholar] [CrossRef]
- Murillo-Rodriguez, E.; Arias-Carrion, O.; Zavala-Garcia, A.; Sarro-Ramirez, A.; Huitron-Resendiz, S.; Arankowsky-Sandoval, G. Basic sleep mechanisms: An integrative review. Cent. Nerv. Syst. Agents Med. Chem. (Former. Curr. Med. Chem.-Cent. Nerv. Syst. Agents) 2012, 12, 38–54. [Google Scholar] [CrossRef]
- Lowe, A.; Bailey, M.; O’Shaughnessy, T.; Macavei, V. Treatment of sleep disturbance following stroke and traumatic brain injury: A systematic review of conservative interventions. Disabil. Rehabil. 2022, 44, 2975–2987. [Google Scholar] [CrossRef]
- Huang, Y.; Jiang, Z.-J.; Deng, J.; Qi, Y.-J. Sleep quality of patients with postoperative glioma at home. World J. Clin. Cases 2020, 8, 4735. [Google Scholar] [CrossRef] [PubMed]
- Zeitzer, J.M.; Friedman, L.; O’Hara, R. Insomnia in the context of traumatic brain injury. J. Rehabil. Res. Dev. 2009, 46, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Rong, Y.; Durden, D.L.; Van Meir, E.G.; Brat, D.J. ‘Pseudopalisading’necrosis in glioblastoma: A familiar morphologic feature that links vascular pathology, hypoxia, and angiogenesis. J. Neuropathol. Exp. Neurol. 2006, 65, 529–539. [Google Scholar] [CrossRef]
- Brat, D.J.; Mapstone, T.B. Malignant glioma physiology: Cellular response to hypoxia and its role in tumor progression. Ann. Intern. Med. 2003, 138, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Wang, X.-P.; Yang, G.-Y. Sleep disorders in stroke: An update on management. Aging Dis. 2021, 12, 570. [Google Scholar] [CrossRef]
- Hervey-Jumper, S.L.; Berger, M.S. Maximizing safe resection of low-and high-grade glioma. J. Neuro-Oncol. 2016, 130, 269–282. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Price, M.; Neff, C.; Cioffi, G.; Waite, K.A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2015–2019. Neuro-Oncology 2022, 24, v1–v95. [Google Scholar] [CrossRef]
- Weller, M.; Wick, W.; Aldape, K.; Brada, M.; Berger, M.; Pfister, S.M.; Nishikawa, R.; Rosenthal, M.; Wen, P.Y.; Stupp, R. Glioma. Nat. Rev. Dis. Prim. 2015, 1, 15017. [Google Scholar] [CrossRef]
- Marquet, G.; Dameron, O.; Saikali, S.; Mosser, J.; Burgun, A. Grading glioma tumors using OWL-DL and NCI thesaurus. AMIA Annu. Symp. Proc. 2007, 2007, 508–512. [Google Scholar]
- Chen, R.; Smith-Cohn, M.; Cohen, A.L.; Colman, H. Glioma subclassifications and their clinical significance. Neurotherapeutics 2017, 14, 284–297. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, J. Clinical presentation, diagnosis, and initial surgical management of high-grade gliomas. In UpToDate; Uptodate: Waltham, MA, USA, 2022. [Google Scholar]
- McGirt, M.J.; Villavicencio, A.T.; Bulsara, K.R.; Friedman, A.H. MRI-guided stereotactic biopsy in the diagnosis of glioma: Comparison of biopsy and surgical resection specimen. Surg. Neurol. 2003, 59, 279–283. [Google Scholar] [CrossRef]
- Fox, S.W.; Lyon, D.; Farace, E. Symptom clusters in patients with high-grade glioma. J. Nurs. Scholarsh. 2007, 39, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Sizoo, E.M.; Braam, L.; Postma, T.J.; Pasman, H.R.W.; Heimans, J.J.; Klein, M.; Reijneveld, J.C.; Taphoorn, M.J. Symptoms and problems in the end-of-life phase of high-grade glioma patients. Neuro-Oncology 2010, 12, 1162–1166. [Google Scholar] [CrossRef] [PubMed]
- Mesfin, F.B.; Al-Dhahir, M.A. Gliomas. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2017. [Google Scholar]
- Haglund, M.M.; Berger, M.S.; Shamseldin, M.; Lettich, E.; Ojemann, G.A. Cortical localization of temporal lobe language sites in patients with gliomas. Neurosurgery 1994, 34, 567–576; discussion 576. [Google Scholar]
- Wernicke, A.G.; Smith, A.W.; Taube, S.; Mehta, M.P. Glioblastoma: Radiation treatment margins, how small is large enough? Pract. Radiat. Oncol. 2016, 6, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Diwanji, T.P.; Engelman, A.; Snider, J.W.; Mohindra, P. Epidemiology, diagnosis, and optimal management of glioma in adolescents and young adults. Adolesc. Health Med. Ther. 2017, 8, 99–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehman, A.A.; Elmore, K.B.; Mattei, T.A. The effects of alternating electric fields in glioblastoma: Current evidence on therapeutic mechanisms and clinical outcomes. Neurosurg. Focus 2015, 38, E14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dirven, L.; Aaronson, N.K.; Heimans, J.J.; Taphoorn, M.J. Health-related quality of life in high-grade glioma patients. Chin. J. Cancer 2014, 33, 40. [Google Scholar] [CrossRef]
- Song, L.; Quan, X.; Su, L.; Wang, K.; Wang, H.; Wu, L.; Chen, C.; Li, S.; Xiang, W.; Chen, L. Inflammation and behavioral symptoms in preoperational glioma patients: Is depression, anxiety, and cognitive impairment related to markers of systemic inflammation? Brain Behav. 2020, 10, e01771. [Google Scholar] [CrossRef]
- Fyllingen, E.H.; Bø, L.E.; Reinertsen, I.; Jakola, A.S.; Sagberg, L.M.; Berntsen, E.M.; Salvesen, Ø.; Solheim, O. Survival of glioblastoma in relation to tumor location: A statistical tumor atlas of a population-based cohort. Acta Neurochir. 2021, 163, 1895–1905. [Google Scholar] [CrossRef]
- Discolo, C.M.; Akst, L.M.; Schlossberg, L.; Greene, D. Anterior cranial fossa glioblastoma with sleep apnea as the initial manifestation. Am. J. Otolaryngol. 2005, 26, 327–329. [Google Scholar] [CrossRef] [PubMed]
- Osanai, S.; Iida, Y.; Nomura, T.; Takahashi, F.; Tsuji, S.; Fujiuchi, S.; Akiba, Y.; Nakano, H.; Yahara, O.; Kikuchi, K. A case of unilateral brain-stem tumor and impaired ventilatory response. Jpn. J. Thorac. Dis. 1994, 32, 990–995. [Google Scholar]
- Ioos, C.; Estournet-Mathiaud, B.; Pinard, J.-M.; Cheliout-Héraut, F. Sleep disorders caused by brainstem tumor: Case report. J. Child Neurol. 2001, 16, 767–770. [Google Scholar] [CrossRef]
- Greenough, G.; Sateia, M.; Fadul, C.E. Obstructive sleep apnea syndrome in a patient with medulloblastoma. Neuro-Oncology 1999, 1, 289–291. [Google Scholar] [CrossRef] [PubMed]
- Manning, H.L.; Leiter, J.C. Respiratory control and respiratory sensation in a patient with a ganglioglioma within the dorsocaudal brain stem. Am. J. Respir. Crit. Care Med. 2000, 161, 2100–2106. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Murofushi, T.; Mizuno, M.; Semba, T. Pediatric brain stem gliomas with the predominant symptom of sleep apnea. Int. J. Pediatr. Otorhinolaryngol. 1996, 37, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.H.; Krishnamoorthy, K.S.; Shannon, D.C. Astrocytoma in an infant with prolonged apnea. Pediatrics 1980, 66, 429–431. [Google Scholar] [CrossRef]
- Nakajima, M.; Katsura, K.-I.; Hashimoto, Y.; Terasaki, T.; Uchino, M. A case of Ondine curse associated with a medullary tumor. Rinsho Shinkeigaku Clin. Neurol. 2000, 40, 811–815. [Google Scholar]
- Marin-Sanabria, E.A.; Kobayashi, N.; Miyake, S.; Kohmura, E. Snoring associated with Ondine’s curse in a patient with brainstem glioma. J. Clin. Neurosci. 2006, 13, 370–373. [Google Scholar] [CrossRef]
- Huang, S.-W.; Lee, P.-L.; Fan, P.-C.; Kuo, M.-F.; Chen, C.-A.; Chiu, S.-N.; Lin, M.-T.; Lu, C.-W.; Wang, J.-K.; Wu, M.-H. Diffuse midline glioma presenting with central sleep apnea and pulmonary hypertension in a 4-year-old patient: A case report. J. Clin. Sleep Med. 2021, 17, 325–328. [Google Scholar] [CrossRef]
- Hui, S.; Wing, Y.; Poon, W.; Chan, Y.; Buckley, T. Alveolar hypoventilation syndrome in brainstem glioma with improvement after surgical resection. Chest 2000, 118, 266–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valente, S.; De Rosa, M.; Culla, G.; Corbo, G.M.; Ciappi, G. An uncommon case of brainstem tumor with selective involvement of the respiratory centers. Chest 1993, 103, 1909–1910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, K.; Yaworski, A.; Bussiere, M.; Ba, F. Pearls & Oy-sters: A Case Report of Holmes Tremor Due to Nigrostriatal Dopamine Disruption That Responded to Dopamine Replacement Therapy. Neurology 2022, 99, 480–483. [Google Scholar]
- Anderson, M.; Salmon, M. Symptomatic cataplexy. J. Neurol. Neurosurg. Psychiatry 1977, 40, 186–191. [Google Scholar] [CrossRef]
- Liao, Y.; He, Y.; Yang, Y.; Li, X.; Huang, F. Case report: Narcolepsy type 2 due to temporal lobe glioma. Medicine 2020, 99, e21002. [Google Scholar] [CrossRef] [PubMed]
- Laus, B.; Caroleo, A.M.; Colafati, G.S.; Carai, A.; Moavero, R.; Ferilli, M.A.N.; Valeriani, M.; Mastronuzzi, A.; Cacchione, A. Secondary Narcolepsy as Worsening Sign in a Pediatric Case of Optic Pathway Glioma. Children 2022, 9, 1455. [Google Scholar] [CrossRef] [PubMed]
- Rosen, G.M.; Bendel, A.E.; Neglia, J.P.; Moertel, C.L.; Mahowald, M. Sleep in children with neoplasms of the central nervous system: Case review of 14 children. Pediatrics 2003, 112, e46–e54. [Google Scholar] [CrossRef] [Green Version]
- Butts, A.; Johnson, D.; Brown, P.; Cerhan, J. QL-07TREATMENT of Fatigue in a Patient with Corpus-Callosum Glioma and Atypical Sleep Disorder. Neuro-Oncology 2014, 16, v179. [Google Scholar] [CrossRef] [Green Version]
- Mendez, M. Pavor nocturnus from a brainstem glioma. J. Neurol. Neurosurg. Psychiatry 1992, 55, 860. [Google Scholar] [CrossRef] [Green Version]
- Di Gennaro, G.; Autret, A.; Mascia, A.; Onorati, P.; Sebastiano, F.; Quarato, P.P. Night terrors associated with thalamic lesion. Clin. Neurophysiol. 2004, 115, 2489–2492. [Google Scholar] [CrossRef]
- Duffau, H.; Kujas, M.; Taillandier, L. Episodic nocturnal wandering in a patient with epilepsy due to a right temporoinsular low-grade glioma: Relief following resection: Case report. J. Neurosurg. 2006, 104, 436–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reim, A.; Strobl, D.; Saletu-Zyhlarz, G.; Preusser, M.; Schmook, M.; Dieckmann, K. Successful treatment of insomnia with melatonin in a patient with malignant glioma after radiotherapy-involving the pineal gland. Rem. Open Access 2016, 1, 1017. [Google Scholar] [CrossRef]
- Fukushima, T.; Sakamoto, S.; Iwaasa, M.; Hayashi, S.; Yamamoto, M.; Utsunomiya, H.; Tomonaga, M. Intramedullary Hemangioblastoma of the Medulla Oblongata—Two Case Reports and Review of the Literature. Neurol. Med.-Chir. 1998, 38, 489–498. [Google Scholar] [CrossRef] [Green Version]
- Prashad, P.S.; Marcus, C.L.; Brown, L.W.; Dlugos, D.J.; Feygin, T.; Harding, B.N.; Heuer, G.G.; Mason, T.B.A. Brain tumor presenting as somnambulism in an adolescent. Pediatr. Neurol. 2013, 49, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Weil, A.G.; Muir, K.; Hukin, J.; Desautels, A.; Martel, V.; Perreault, S. Narcolepsy and hypothalamic region tumors: Presentation and evolution. Pediatr. Neurol. 2018, 84, 27–31. [Google Scholar] [CrossRef]
- Mendoza, M.; Latorre, J.G. Pearls & Oy-sters: Reversible Ondine’s curse in a case of lateral medullary infarction. Neurology 2013, 80, e13–e16. [Google Scholar]
- Dauvilliers, Y.; Buguet, A. Hypersomnia. Dialogues Clin. Neurosci. 2005, 7, 347–356. [Google Scholar] [CrossRef]
- Powell, C.; Guerrero, D.; Sardell, S.; Cumins, S.; Wharram, B.; Traish, D.; Gonsalves, A.; Ashley, S.; Brada, M. Somnolence syndrome in patients receiving radical radiotherapy for primary brain tumours: A prospective study. Radiother. Oncol. 2011, 100, 131–136. [Google Scholar] [CrossRef]
- Trotti, L.M. Idiopathic hypersomnia. Sleep Med. Clin. 2017, 12, 331–344. [Google Scholar] [CrossRef]
- Kornum, B.R.; Knudsen, S.; Ollila, H.M.; Pizza, F.; Jennum, P.J.; Dauvilliers, Y.; Overeem, S. Narcolepsy. Nat. Rev. Dis. Prim. 2017, 3, 16100. [Google Scholar] [CrossRef]
- Boele, F.W.; Douw, L.; de Groot, M.; van Thuijl, H.F.; Cleijne, W.; Heimans, J.J.; Taphoorn, M.J.B.; Reijneveld, J.C.; Klein, M. The effect of modafinil on fatigue, cognitive functioning, and mood in primary brain tumor patients: A multicenter randomized controlled trial. Neuro-Oncology 2013, 15, 1420–1428. [Google Scholar] [CrossRef]
- Bjorvatn, B.; Grønli, J.; Pallesen, S. Prevalence of different parasomnias in the general population. Sleep Med. 2010, 11, 1031–1034. [Google Scholar] [CrossRef] [PubMed]
- Galbiati, A.; Rinaldi, F.; Giora, E.; Ferini-Strambi, L.; Marelli, S. Behavioural and Cognitive-Behavioural Treatments of Parasomnias. Behav. Neurol. 2015, 2015, 786928. [Google Scholar] [CrossRef] [PubMed]
- Boele, F.W.; Rooney, A.G.; Grant, R.; Klein, M. Psychiatric symptoms in glioma patients: From diagnosis to management. Neuropsychiatr. Dis. Treat. 2015, 11, 1413–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mainio, A.; Hakko, H.; Niemelä, A.; Koivukangas, J.; Räsänen, P. Insomnia among brain tumor patients: A population-based prospective study of tumor patients in northern Finland. J. Psychosoc. Oncol. 2013, 31, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.E.; McSherry, F.; Herndon, J.E.; Peters, K.B. Insomnia and its associations in patients with recurrent glial neoplasms. Springerplus 2016, 5, 823. [Google Scholar] [CrossRef] [Green Version]
- Savard, J.; Morin, C.M. Insomnia in the context of cancer: A review of a neglected problem. J. Clin. Oncol. 2001, 19, 895–908. [Google Scholar] [CrossRef]
- O’Donnell, J.F. Insomnia in cancer patients. Clin. Cornerstone 2004, 6, S6–S14. [Google Scholar] [CrossRef]
- Loughan, A. Cognitive Behavioral Therapy for Insomnia in Patients with Glioma. Ph.D. Thesis, Virginia Commonwealth University, Richmond, VA, USA, 30 November 2020. [Google Scholar]
- Snow, A.; Gozal, E.; Malhotra, A.; Tiosano, D.; Perlman, R.; Vega, C.; Shahar, E.; Gozal, D.; Hochberg, Z.E.; Pillar, G. Severe hypersomnolence after pituitary/hypothalamic surgery in adolescents: Clinical characteristics and potential mechanisms. Pediatrics 2002, 110, e74. [Google Scholar] [CrossRef] [Green Version]
- Aoun, R.; Rawal, H.; Attarian, H.; Sahni, A. Impact of traumatic brain injury on sleep: An overview. Nat. Sci. Sleep 2019, 11, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Piantino, J.; Lim, M.M.; Newgard, C.D.; Iliff, J. Linking traumatic brain injury, sleep disruption and post-traumatic headache: A potential role for glymphatic pathway dysfunction. Curr. Pain Headache Rep. 2019, 23, 62. [Google Scholar] [CrossRef] [PubMed]
- Luther, M.; Poppert Cordts, K.M.; Williams, C.N. Sleep disturbances after pediatric traumatic brain injury: A systematic review of prevalence, risk factors, and association with recovery. Sleep 2020, 43, zsaa083. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, K.A.; Edmed, S.L.; Allan, A.C.; Karlsson, L.J.; Smith, S.S. Characterizing self-reported sleep disturbance after mild traumatic brain injury. J. Neurotrauma 2015, 32, 474–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathias, J.; Alvaro, P. Prevalence of sleep disturbances, disorders, and problems following traumatic brain injury: A meta-analysis. Sleep Med. 2012, 13, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Rao, V.; Bergey, A.; Hill, H.; Efron, D.; McCann, U. Sleep disturbance after mild traumatic brain injury: Indicator of injury? J. Neuropsychiatry Clin. Neurosci. 2011, 23, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, E.; Egorova, N.; Khlif, M.S.; Khan, W.; Werden, E.; Pase, M.P.; Howard, M.; Brodtmann, A. Regional neurodegeneration correlates with sleep–wake dysfunction after stroke. Sleep 2020, 43, zsaa054. [Google Scholar] [CrossRef]
- Bollu, P.; Pandey, A.; Pesala, S.; Nalleballe, K. Sleepiness after stroke: Case report and review of literature on hypersomnia as a result of stroke. Madr. J. Neurosci. 2017, 1, 4–6. [Google Scholar] [CrossRef]
- Tauman, R. Metabolic and hormonal regulation during sleep. In Sleep Disordered Breathing in Children: A Comprehensive Clinical Guide to Evaluation and Treatment; Humana Press: Totowa, NJ, USA, 2012; pp. 121–132. [Google Scholar]
- Fox, R.S.; Ancoli-Israel, S.; Roesch, S.C.; Merz, E.L.; Mills, S.D.; Wells, K.J.; Sadler, G.R.; Malcarne, V.L. Sleep disturbance and cancer-related fatigue symptom cluster in breast cancer patients undergoing chemotherapy. Support. Care Cancer 2020, 28, 845–855. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Year | Patient Age | Patient Gender | Tumor Location | Tumor Type | Sleep Disturbance |
|---|---|---|---|---|---|---|
| Discolo et al. [53] | 2005 | 71 | Male | Right frontal lobe | Glioblastoma Multiforme | Sleep apnea |
| Osanai et al. [54] | 1994 | 44 | Male | Left cerebellar peduncle, medulla | Ganglioglioma | Sleep apnea |
| Ioos et al. [55] | 2016 | 4 | Female | Posterior fossa | Meningioma | Sleep apnea |
| Greenough et al. [56] | 1999 | 34 | Male | Bilateral medulla | Medulloblastoma | Sleep apnea |
| Manning and Leiter [57] | 2000 | 18 | Female | Medulla | Ganglioglioma | Somnolence, sleep apnea |
| Ito et al. [58] | 1996 | 12, 6 | Male | Medulla, pons | Glioma | Sleep apnea |
| Kelly et al. [59] | 1980 | 4 weeks | Male | Left middle fossa | Astrocytoma | Sleep apnea |
| Nakajima et al. [60] | 2000 | 49 | Female | Medulla, pons | Astrocytoma | Sleep apnea (Ondine’s curse) |
| Marin-Sanabria [61] | 2005 | 52 | Female | Medulla | Glioma | Sleep apnea (Ondine’s curse) |
| Huang et al. [62] | 2021 | 4 | Male | Medulla, pons | Glioma | Sleep apnea |
| Hui et al. [63] | 2000 | 3 | Male | Posterior fossa | Pilocytic astrocytoma | Hypersomnia, sleep apnea |
| Valente et al. [64] | 1993 | 24 | Male | Pons | Fibrillary astrocytoma | Sudden awakenings, hypersomnia, sleep apnea |
| Yen et al. [65] | 2022 | 48 | Male | Right side thalamus and midbrain | Glioma | Hypersomnia |
| Anderson et al. [66] | 1977 | 23 | Male | Hypothalamus | Glioma | Narcolepsy, hypersomnia, sleep paralysis |
| Liao et al. [67] | 2020 | 44 | Male | Hippocampal formation | Glioma | Somnolence, Narcolepsy type 2 |
| Laus et al. [68] | 2022 | 3 | Male | Optic chiasm | Ganglioglioma | Somnolence, Narcolepsy |
| Rosen et al. [69] | 2003 | 5–15 | Males and Females | Hypothalamus, optic chiasm, brainstem, pineal gland, pituitary gland | Pineoblastoma, craniopharyngioma, medulloblastoma, astrocytoma | Narcolepsy |
| Butts et al. [70] | 2014 | 53 | Male | Corpus callosum | Glioma | Somnolence, Narcolepsy |
| Mendez [71] | 1992 | 15 | Male | Fourth ventricle and brainstem | Astrocytoma | Night terrors |
| Di Gennaro et al. [72] | 2004 | 48 | Female | Right thalamus | Patient refused biopsy | Night terrors |
| Duffau et al. [73] | 2006 | 38 | Female | Right paralimbic region | Oligodendroglioma | Epileptic somnambulism |
| Reim et al. [74] | 2016 | 29 | Female | Right basal ganglia | Astrocytoma | Insomnia |
| Fukushima et al. [75] | 1998 | 16, 33 | Female, Male | Medulla | Hemangioblastoma | Sleep apnea |
| Prashad. [76] | 2013 | 15 | Male | Parietal lobe | Dysembryoplastic neuroepithelial tumor | Sleepwalking |
| Weil et al. [77] | 2017 | 11 | Female | Sellar and suprasellar region | Germinoma | Narcolepsy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allgood, J.E.; Roe, A.; Sparks, B.B.; Castillo, M.; Cruz, A.; Brooks, A.E.; Brooks, B.D. The Correlation of Sleep Disturbance and Location of Glioma Tumors: A Narrative Review. J. Clin. Med. 2023, 12, 4058. https://doi.org/10.3390/jcm12124058
Allgood JE, Roe A, Sparks BB, Castillo M, Cruz A, Brooks AE, Brooks BD. The Correlation of Sleep Disturbance and Location of Glioma Tumors: A Narrative Review. Journal of Clinical Medicine. 2023; 12(12):4058. https://doi.org/10.3390/jcm12124058
Chicago/Turabian StyleAllgood, JuliAnne E., Avery Roe, Bridger B. Sparks, Mercedes Castillo, Angel Cruz, Amanda E. Brooks, and Benjamin D. Brooks. 2023. "The Correlation of Sleep Disturbance and Location of Glioma Tumors: A Narrative Review" Journal of Clinical Medicine 12, no. 12: 4058. https://doi.org/10.3390/jcm12124058
APA StyleAllgood, J. E., Roe, A., Sparks, B. B., Castillo, M., Cruz, A., Brooks, A. E., & Brooks, B. D. (2023). The Correlation of Sleep Disturbance and Location of Glioma Tumors: A Narrative Review. Journal of Clinical Medicine, 12(12), 4058. https://doi.org/10.3390/jcm12124058