Portal Vein Thrombosis in Liver Transplantation: A Retrospective Cohort Study



Abstract
:
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
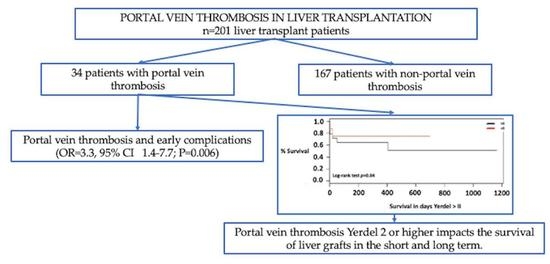
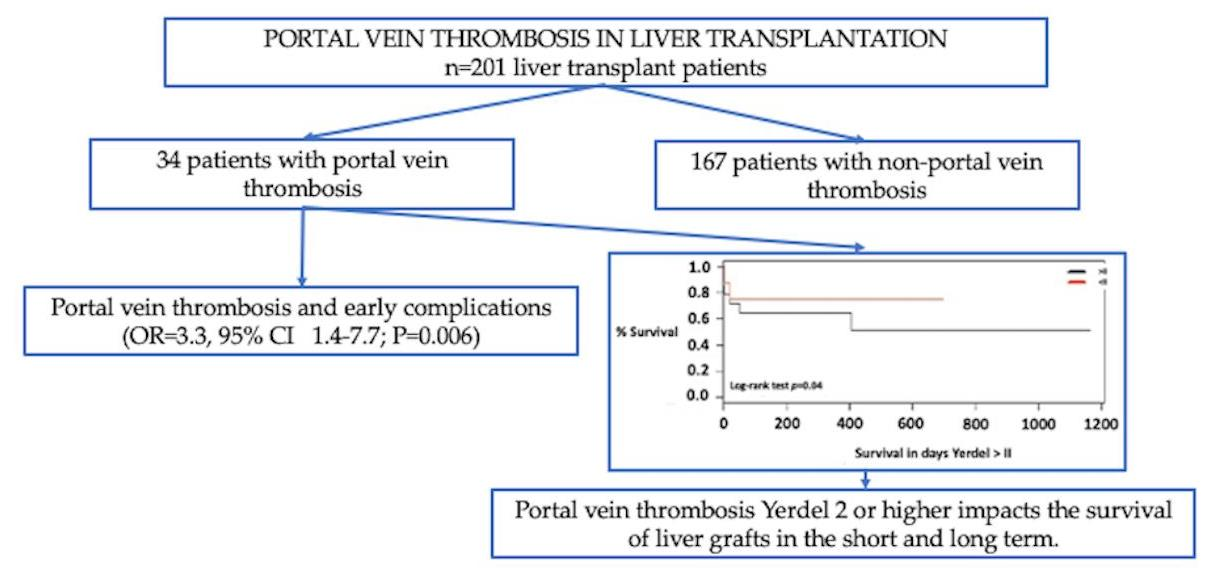
3.2. Early Transplant Complications
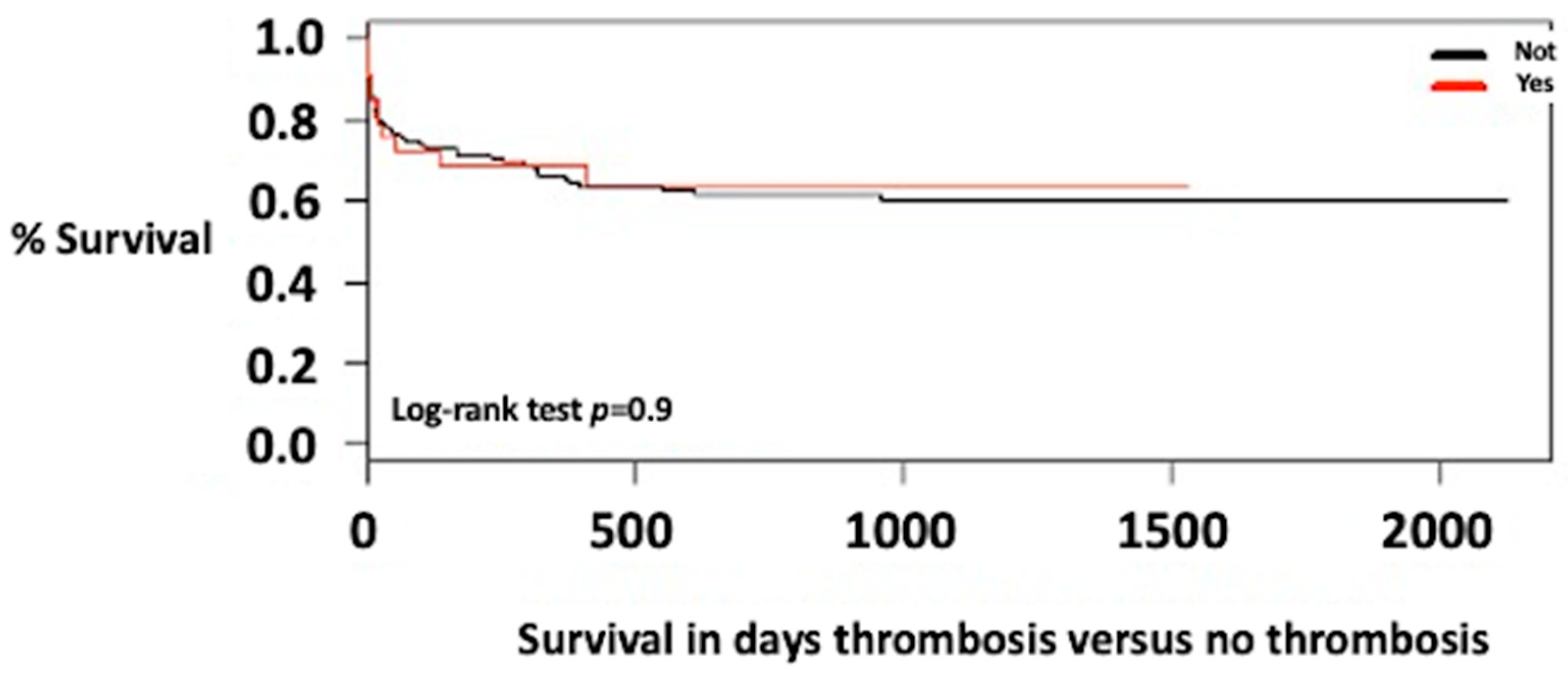
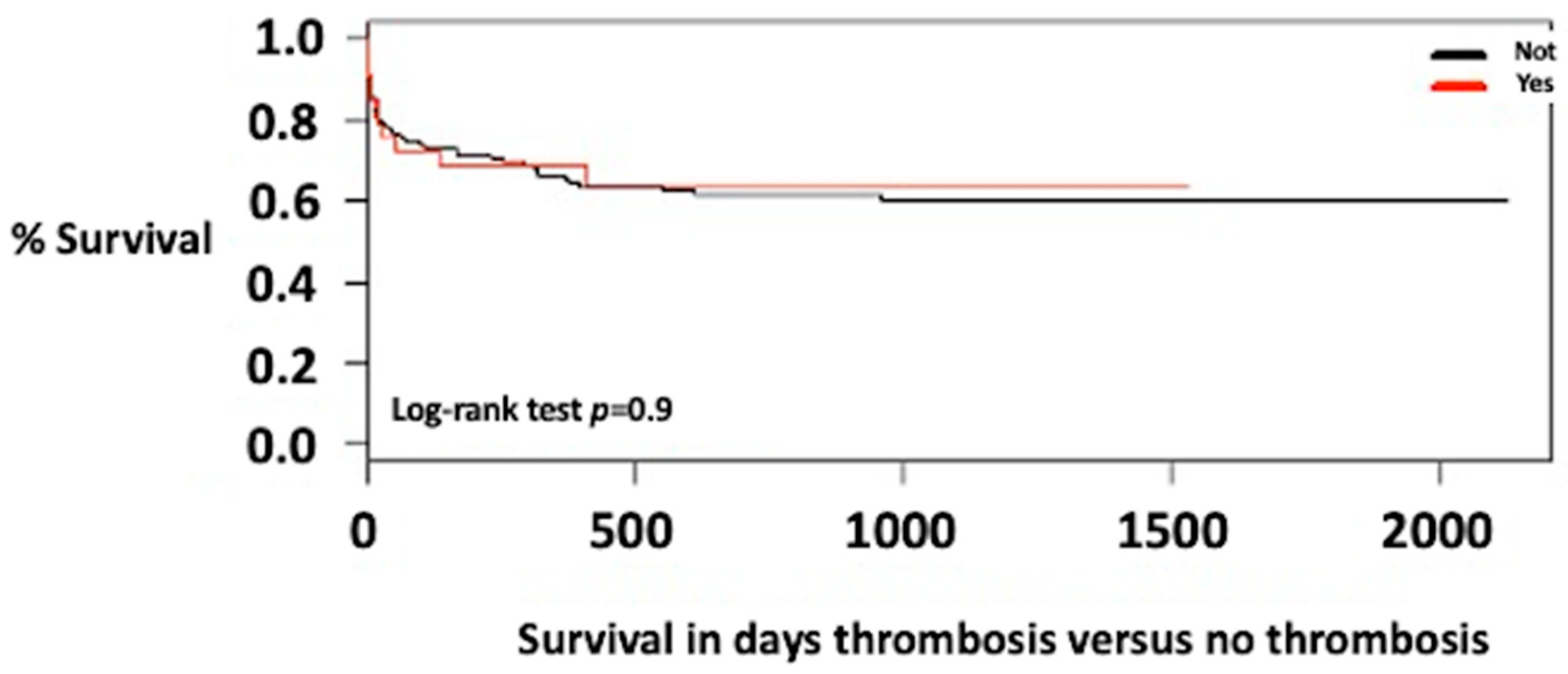
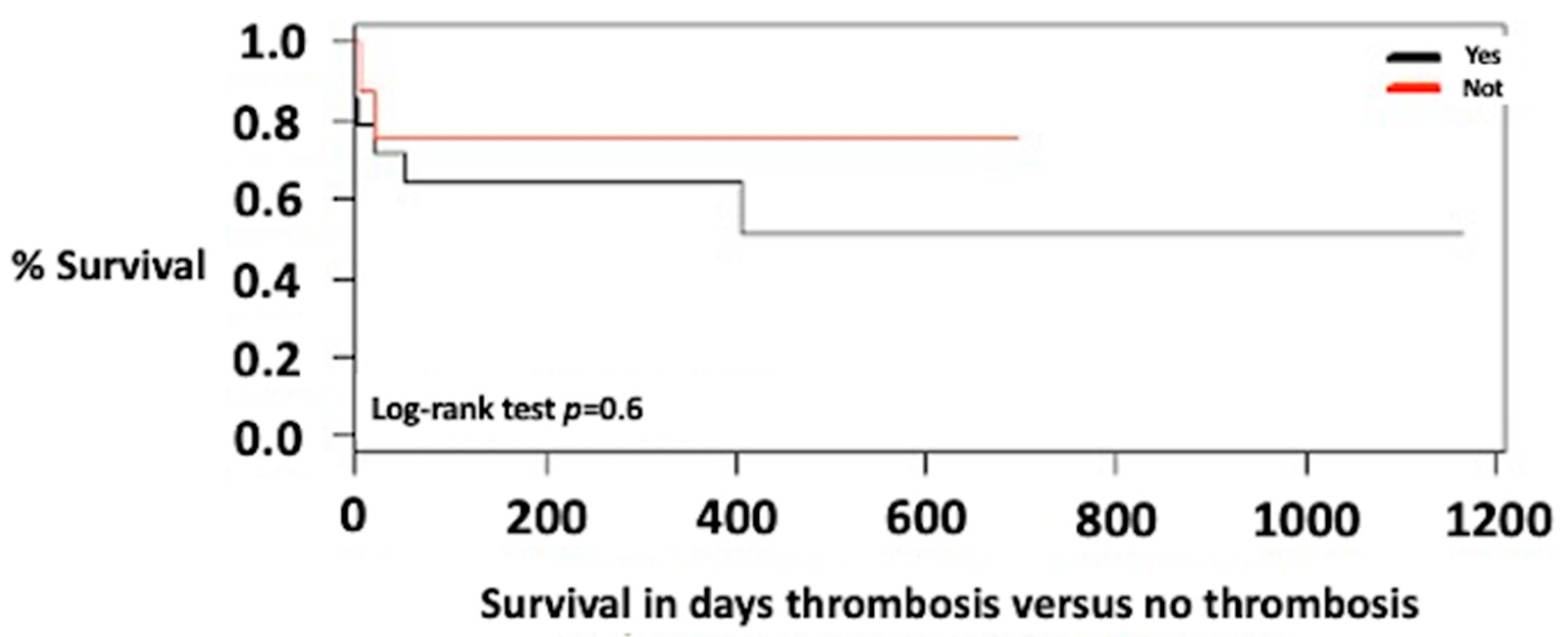
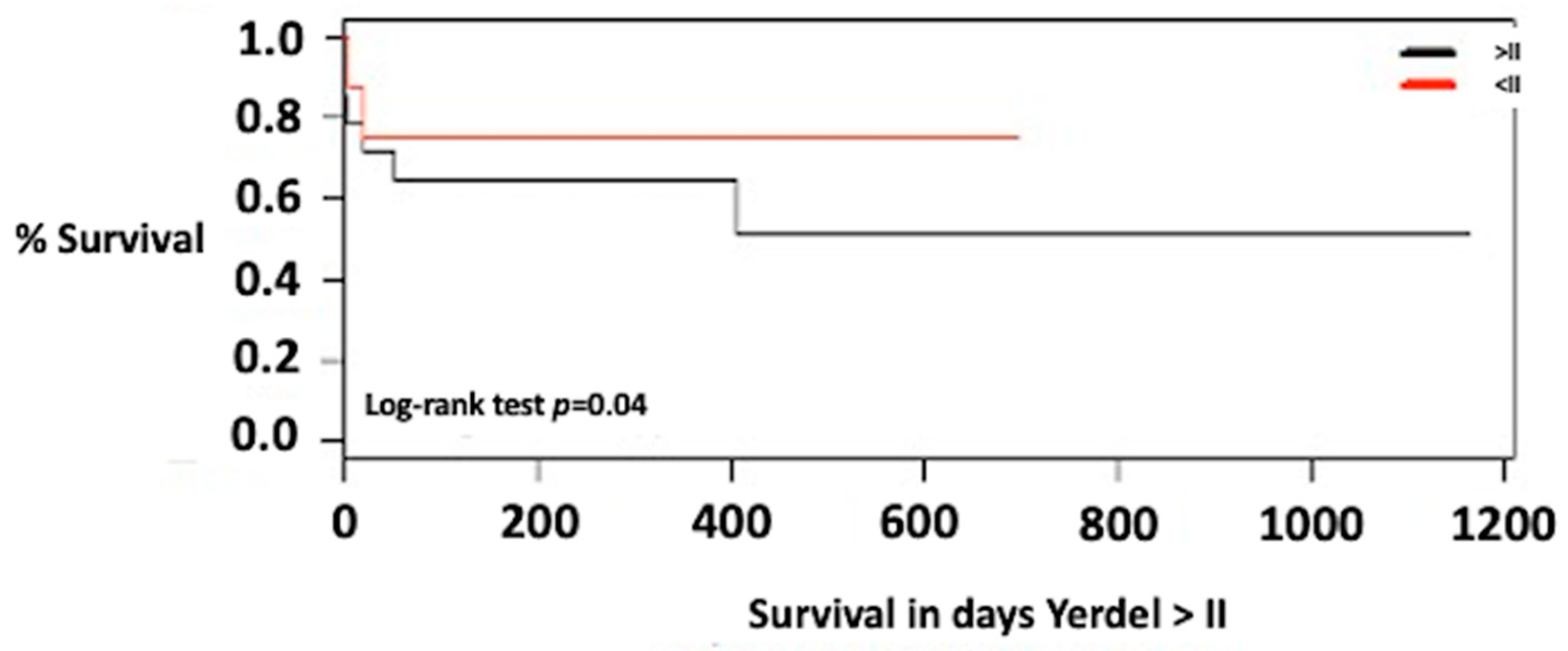
3.3. Survival of Patients with Portal Vein Thrombosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhangui, P.; Fernandes, E.S.; Di Benedetto, F.; Joo, D.-J.; Nadalin, S. Current management of portal vein thrombosis in liver transplantation. Int. J. Surg. 2020, 82, 122–127. [Google Scholar] [CrossRef]
- Agbim, U.; Satapathy, S.K. PRO: Portal Vein Thrombosis Impacts Liver Transplantation Outcomes. Clin. Liver Dis. 2020, 16, 127–131. [Google Scholar] [CrossRef]
- Teng, F.; Sun, K.-Y.; Fu, Z.-R. Tailored classification of portal vein thrombosis for liver transplantation: Focus on strategies for portal vein inflow reconstruction. World J. Gastroenterol. 2020, 26, 2691–2701. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Dai, J.; Jia, J.; Ren, W.; Yang, M.; Li, H.; Fan, D.; Guo, X. Association between Portal Vein Thrombosis and Survival of Liver Transplant Recipients: A Systematic Review and Meta-analysis of Observational Studies. J. Gastrointest. Liver Dis. 2015, 24, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Ren, W.; De Stefano, V.; Fan, D. Associations of Coagulation Factor V Leiden and Prothrombin G20210A Mutations with Budd–Chiari Syndrome and Portal Vein Thrombosis: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2014, 12, 1801–1812.e7. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, E.; Misawa, T.; Kitamura, H.; Fujioka, S.; Akiba, T.; Yanaga, K. A case of portal vein thrombosis caused by blunt abdominal trauma in a patient with low protein C activity. Clin. J. Gastroenterol. 2018, 11, 507–513. [Google Scholar] [CrossRef]
- Dumic, I.; Tankosic, N.; Stojkovic Lalosevic, M.; Alempijevic, T. Sport-Related Portal Vein Thrombosis: An Unusual Complication. Case Rep. Hepatol. 2017, 2017, 9324246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzubaidi, S.; Patel, I.; Saini, A.; Knuttinen, G.; Naidu, S.; Kriegshuaser, S.; Albadawi, H.; Oklu, R. Current concepts in portal vein thrombosis: Etiology, clinical presentation and management. Abdom. Imaging 2019, 44, 3453–3462. [Google Scholar] [CrossRef] [PubMed]
- Northup, P.G.; Garcia-Pagan, J.C.; Garcia-Tsao, G.; Intagliata, N.M.; Superina, R.A.; Roberts, L.N. Vascular Liver Disorders, Portal Vein Thrombosis, and Procedural Bleeding in Patients with Liver Disease: 2020 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 73, 366–413. [Google Scholar] [CrossRef]
- Fusaro, L.; Di Bella, S.; Martingano, P.; Crocè, L.S.; Giuffrè, M. Pylephlebitis: A Systematic Review on Etiology, Diagnosis, and Treatment of Infective Portal Vein Thrombosis. Diagnostics 2023, 13, 429. [Google Scholar] [CrossRef]
- Guerra, F.; Dorma, M.P.F.; Giuliani, G.; Caravaglios, G.; Coratti, A. Pylephlebitis: An uncommon complication of sigmoid diverticulitis. Am. J. Emerg. Med. 2023, 66, 174.e3–174.e5. [Google Scholar] [CrossRef] [PubMed]
- Van Thiel, D.H.; Schade, R.R.; Starzl, T.E.; Iwatsuki, S.; Shaw, B.W., Jr.; Gavaler, J.S.; Dugas, M. Liver transplantation in adults. Hepatology 1982, 2, 637–640. [Google Scholar] [CrossRef] [Green Version]
- Shaw, B.W., Jr.; Iwatsuki, S.; Bron, K.; Starzl, T.E.; Bran, K. Portal vein grafts in hepatic transplantation. Surg. Gynecol. Obstet. 1985, 161, 66–68. [Google Scholar] [PubMed]
- Rodríguez-Castro, K.I.; Porte, R.J.; Nadal, E.; Germani, G.; Burra, P.; Senzolo, M. Management of Nonneoplastic Portal Vein Thrombosis in the Setting of Liver Transplantation: A Systematic Review. Transplantation 2012, 94, 1145–1153. [Google Scholar] [CrossRef]
- Francoz, C.; Valla, D.; Durand, F. Portal vein thrombosis, cirrhosis, and liver transplantation. J. Hepatol. 2012, 57, 203–212. [Google Scholar] [CrossRef] [Green Version]
- Zanetto, A.; Rodriguez-Kastro, K.-I.; Germani, G.; Ferrarese, A.; Cillo, U.; Burra, P.; Senzolo, M. Mortality in liver transplant recipients with portal vein thrombosis—An updated meta-analysis. Transplant. Int. 2018, 31, 1318–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhangui, P.; Lim, C.; Levesque, E.; Salloum, C.; Lahat, E.; Feray, C.; Azoulay, D. Novel classification of non-malignant portal vein thrombosis: A guide to surgical decision-making during liver transplantation. J. Hepatol. 2019, 71, 1038–1050. [Google Scholar] [CrossRef]
- Yerdel, M.A.; Gunson, B.; Mirza, D.; Karayalçin, K.; Olliff, S.; Buckels, J.; Pirenne, J. Portal vein thrombosis in adults undergoing liver transplantation: Risk factors, screening, management, and outcome. Transplantation 2020, 69, 1873–1881. [Google Scholar] [CrossRef]
- Molmenti, E.P.; Roodhouse, T.W.; Molmenti, H.; Jaiswal, K.; Jung, G.; Marubashi, S.; Sanchez, E.Q.; Gogel, B.; Levy, M.F.; Goldstein, R.M.; et al. Thrombendvenectomy for Organized Portal Vein Thrombosis at the Time of Liver Transplantation. Ann. Surg. 2002, 235, 292–296. [Google Scholar] [CrossRef]
- Dumortier, J.; Czyglik, O.; Poncet, G.; Blanchet, M.-C.; Boucaud, C.; Henry, L.; Boillot, O. Eversion Thrombectomy for Portal Vein Thrombosis During Liver Transplantation. Am. J. Transplant. 2002, 2, 934–938. [Google Scholar] [CrossRef]
- Robles, R.; Fernandez, J.A.; Hernandez, Q.; Marin, C.; Ramirez, P.; Bueno, F.S.; Lujan, J.A.; Rodriguez, J.M.; Acosta, F.; Parrilla, P. Eversion thromboendovenectomy in organized portal vein thrombosis during liver transplantation. Clin. Transplant. 2004, 18, 79–84. [Google Scholar] [CrossRef]
- Nacif, L.S.; Zanini, L.Y.; Pinheiro, R.S.; Waisberg, D.R.; Rocha-Santos, V.; Andraus, W.; Carrilho, F.J.; Carneiro-D’albuquerque, L. Portal vein surgical treatment on non-tumoral portal vein thrombosis in liver transplantation: Systematic Review and Meta-Analysis. Clinics 2021, 76, e2184. [Google Scholar] [CrossRef]
- Kato, T.; Levi, D.M.; DeFaria, W.; Nishida, S.; Tzakis, A.G. Liver transplantation with renoportal anastomosis after distal splenorenal shunt. Arch. Surg. 2000, 135, 1401–1404. [Google Scholar] [CrossRef] [Green Version]
- Golse, N.; Bucur, P.O.; Faitot, F.; Bekheit, M.; Pittau, G.; Ciacio, O.; Antonio, S.A.; René, A.; Denis, D.; Didier, D.; et al. Spontaneous Splenorenal Shunt in Liver Transplantation: Results of Left Renal Vein Ligation Versus Renoportal Anastomosis. Transplantation 2015, 99, 2576–2585. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Hassan, A.; Diago Uso, T.; Hashmimoto, K.; Aucejo, F.N.; Fujiki, M.; Eghtesad, B.; Sasaki, K.; Lindenmeyer, C.C.; Miller, C.M.; et al. Renoportal anastomosis in liver transplantation and its impact on patient outcomes: A systematic literature review. Transplant. Int. 2019, 32, 117–1127. [Google Scholar] [CrossRef] [Green Version]
- Lerut, J.P.; Lai, Q.; Goyet, J.D.V.D. Cavoportal Hemitransposition in Liver Transplantation: Toward a More Safe and Efficient Technique. Liver Transplant. 2019, 26, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Bhangui, P.; Lim, C.; Salloum, C.; Andreani, P.; Sebbagh, M.; Hoti, E.; Azoulay, D. Caval inflow to the graft for liver transplantation in patients with diffuse portal vein thrombosis: A 12-year experience. Ann. Surg. 2017, 254, 1008–1116. [Google Scholar] [CrossRef]
- Vianna, R.M.; Mangus, R.S.; Kubal, C.; Fridell, J.A.; Beduschi, T.; Tector, A.J. Multivisceral transplantation for diffuse portomesenteric thrombosis. Ann. Surg. 2012, 255, 1144–1150. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Yang, L. Gastric coronary vein to portal vein reconstruction in liver transplant: Case report. Exp. Clin. Transplant. 2014, 12, 562–564. [Google Scholar]
- Bhangui, P.; Salloum, C.; Lim, C.; Andreani, P.; Ariche, A.; Adam, R.; Castaing, D.; Kerba, T.; Azoulay, D. Portal vein arterialization: A salvage procedure for a totally de-arterialized liver. The Paul Brousse Hospital experience. HPB 2014, 16, 723–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnickel, G.T.; Busuttil, R.W. Portal Vein Thrombosis and Other Venous Anomalies. In Transplantation of the Liver; Elsevier: Amsterdam, The Netherlands, 2015; pp. 785–792. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 20 November 2021).
- Tripodi, A.; Mannucci, P.M. The Coagulopathy of Chronic Liver Disease. N. Engl. J. Med. 2011, 365, 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Northup, P.G. Hypercoagulation in Liver Disease. Clin. Liver Dis. 2009, 13, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Francoz, C.; Belghiti, J.; Vilgrain, V.; Sommacale, D.; Paradis, V.; Condat, B.; Denninger, M.H.; Sauvanet, A.; Valla, D.; Durand, F. Splanchnic vein thrombosis in candidates for liver transplantation: Usefulness of screening and anticoagulation. Gut 2005, 54, 691–697. [Google Scholar] [CrossRef]
- de Franchis, R.; Faculty, B.V. Revising consensus in portal hypertension: Report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension. J. Hepatol. 2010, 53, 762–768. [Google Scholar] [CrossRef] [Green Version]
- Amitrano, L.; Guardascione, M.A.; Menchise, A.; Martino, R.; Scaglione, M.; Giovine, S.; Romano, L.; Balzano, A. Safety and efficacy of anticoagulation therapy with low molecular weight heparin for portal vein thrombosis in patients with liver cirrhosis. J. Clin. Gastroenterol. 2010, 44, 448–451. [Google Scholar] [CrossRef] [Green Version]
- de Franchis, R.; Faculty, B.V. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J. Hepatol. 2015, 63, 743–752. [Google Scholar] [CrossRef] [Green Version]
- Francoz, C.; Dondero, D.; Abdel-Razek, W. Screening for portal vein thrombosis in candidates for liver transplantation and anticoagulation until transplantation: Results of a prospective assessment. Liver Transplant. 2008, 14, S245. [Google Scholar]
- Simón-Talero, M.; Roccarina, D.; Martínez, J.; Lampichler, K.; Baiges, A.; Low, G.; Botella, E.R. Association Between Portosystemic Shunts and Increased Complications and Mortality in Patients with Cirrhosis. Gastroenterology 2018, 154, 1694–1705.e4. [Google Scholar] [CrossRef] [Green Version]
- Gavara, C.G.; Bhangui, P.; Salloum, C.; Osseis, M.; Esposito, F.; Moussallem, T.; Lahat, E.; Fuentes, L.; Compagnon, P.; Ngongang, N.; et al. Ligation versus no ligation of spontaneous portosystemic shunts during liver transplantation: Audit of a prospective series of 66 consecutive patients. Liver Transplant. 2017, 24, 505–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lendoire, J.; Raffin, G.; Cejas, N.; Duek, F.; Schelotto, P.B.; Trigo, P.; Quarin, C.; Garay, V.; Imventarza, O. Liver transplantation in adult patients with portal vein thrombosis: Risk factors, management and outcome. HPB 2007, 9, 352–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hibi, T.; Nishida, S.; Levi, D.M.; Selvaggi, G.; Tekin, A.; Fan, J.; Tzakis, A.G. When and why portal vein thrombosis matters in liver transplantation: A critical audit of 174 cases. Ann. Surg. 2014, 259, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Ponziani, F.R.; Zocco, M.A.; Senzolo, M.; Pompili, M.; Gasbarrini, A.; Avolio, A.W. Portal vein thrombosis and liver transplantation: Implications for waiting list period, surgical approach, early and late follow-up. Transplant. Rev. 2014, 28, 92–101. [Google Scholar] [CrossRef]
- Duffy, J.P.; Hong, J.C.; Farmer, D.G.; Ghobrial, R.M.; Yersiz, H.; Hiatt, J.R.; Busuttil, R.W. Vascular complications of orthotopic liver transplantation: Experience in more than 4,200 patients. J. Am. Coll. Surg. 2009, 208, 896–903. [Google Scholar] [CrossRef]
- Manzanet, G.; Sanjuán, F.; Orbis, P.; López, R.; Moya, A.; Juan, M.; Mir, J. Liver transplantation in patients with portal vein thrombosis. Liver Transplant. 2001, 7, 125–131. [Google Scholar] [CrossRef]
- Chen, H.; Turon, F.; Hernández-Gea, V.; Fuster, J.; Garcia-Criado, A.; Barrufet, M.; Garcia-Pagán, J.C. Nontumoral portal vein thrombosis in patients awaiting liver transplantation. Liver Transplant. 2016, 22, 352–365. [Google Scholar] [CrossRef] [Green Version]
- Ravaioli, M.; Zanello, M.; Grazi, G.L.; Ercolani, G.; Cescon, M.; Del Gaudio, M.; Pinna, A.D. Portal vein thrombosis and liver transplantation: Evolution during 10 years of experience at the University of Bologna. Ann. Surg. 2011, 253, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Padilla-Machaca, P.M.; Chaman Ortiz, J.C. Portal vein thrombosis in patients undergoing to liver transplantation. Rev. Gastroenterol. Peru 2019, 39, 258–264. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | No Portal Vein Thrombosis n = 167 | Portal Vein Thrombosis n = 34 | p-Value |
|---|---|---|---|
| Gender, n % | |||
| Male | 91 (55%) | 22 (65%) | 0.3 |
| Female | 75 (45%) | 12 (35%) | 0.4 |
| Age, mean (SD) | 56 (12.2) | 59 (9.2) | 0.1 |
| Hospital stays, mean (SD) | 24 (34.9) | 37 (64.6) | 0.25 |
| Body mass index, mean (SD) | 26 (4.8) | 27 (5) | 0.29 |
| Hepatocellular carcinoma, n % | |||
| Yes | 59 (35%) | 14 (41%) | 0.65 |
| Child | |||
| A | 36 (21%) | 4 (12%) | 0.28 |
| B | 73 (44%) | 16 (47%) | 0.86 |
| C | 58 (35%) | 14 (41%) | 0.64 |
| Type of early vascular complication | |||
| Hepatic artery thrombosis | 14 (8%) | 4 (12%) | 0.76 |
| Hepatic artery stenosis | 1 (0.6%) | 1 (3%) | 0.78 |
| Portal Vein thrombosis | 2 (1%) | 4 (12%) | 0.006 |
| Meld, mean (SD) | 20 | 19 | 0.41 |
| Death in the first month, n % | 42 (25%) | 8 (24%) | 1 |
| Characteristic | n | Percentage |
|---|---|---|
| Yerdel | ||
| I | 20 | 58.8% |
| II | 12 | 35.2% |
| III | 1 | 3% |
| IV | 1 | 3% |
| Shunt presence | ||
| Yes | 23 | 68% |
| Not | 11 | 32% |
| Shunt type | ||
| Splenorenal | 21 | 62% |
| Gastric | 2 | 6% |
| Physiological | ||
| >1 cm | 9 | 26% |
| <1 cm | 14 | 41% |
| Child | ||
| A | 4 | 12% |
| B | 16 | 47% |
| C | 14 | 41% |
| Early Vascular Complication | ||
| Yes | 11 | 32% |
| Not | 23 | 68% |
| Type of Early Vascular Complication | ||
| Hepatic artery thrombosis | 4 | 12% |
| Hepatic artery stenosis | 1 | 3% |
| Portal Vein Thrombosis | 4 | 12% |
| Hepatic Vein Stenosis | 1 | 3% |
| Portal vein thrombosis and Hepatic Artery | 1 | 3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrera-Lozano, L.M.; Ramírez-Arbeláez, J.A.; Muñoz, C.L.; Becerra, J.A.; Toro, L.G.; Ardila, C.M. Portal Vein Thrombosis in Liver Transplantation: A Retrospective Cohort Study. J. Clin. Med. 2023, 12, 3951. https://doi.org/10.3390/jcm12123951
Barrera-Lozano LM, Ramírez-Arbeláez JA, Muñoz CL, Becerra JA, Toro LG, Ardila CM. Portal Vein Thrombosis in Liver Transplantation: A Retrospective Cohort Study. Journal of Clinical Medicine. 2023; 12(12):3951. https://doi.org/10.3390/jcm12123951
Chicago/Turabian StyleBarrera-Lozano, Luis Manuel, Jaime Alberto Ramírez-Arbeláez, Cristian Leonardo Muñoz, Jorge Andrés Becerra, Luis Guillermo Toro, and Carlos M. Ardila. 2023. "Portal Vein Thrombosis in Liver Transplantation: A Retrospective Cohort Study" Journal of Clinical Medicine 12, no. 12: 3951. https://doi.org/10.3390/jcm12123951
APA StyleBarrera-Lozano, L. M., Ramírez-Arbeláez, J. A., Muñoz, C. L., Becerra, J. A., Toro, L. G., & Ardila, C. M. (2023). Portal Vein Thrombosis in Liver Transplantation: A Retrospective Cohort Study. Journal of Clinical Medicine, 12(12), 3951. https://doi.org/10.3390/jcm12123951