
Histological Characteristics and Management of Hepatitis on Immune Checkpoint Inhibitors: A Retrospective Descriptive Study
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Histological Evaluation
- Acute granulomatous hepatitis, defined by the presence of granulomas;
- Acute hepatitis with an autoimmune profile, defined by the presence of plasma cells;
- Acute hepatitis with a toxic profile, defined by the presence of eosinophilic polynuclear cells.
2.3. Therapeutic Response
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics according to Liver Biopsy
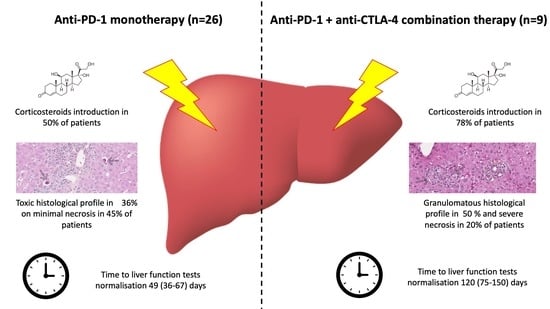
3.2. Clinical and Histological Characteristics by ICI Type
3.3. Response to Corticosteroids according to Histological and Biological Profile
3.4. Management of ICI-DILI
- Intense necrosis was observed in seven (35%) patients receiving corticosteroids and in no patient not treated with corticosteroids (p = 0.036).
- Granulomatous lesions were observed in four (20%) patients receiving corticosteroids and in two (13%) patients not treated with corticosteroids (p = 0.913).
- Toxic profile was observed in five (25%) patients receiving corticosteroids and in one (7%) patient not treated with corticosteroids (p = 0.406).
- Autoimmune profile was observed in one (5%) patient receiving corticosteroids and in no patient not treated with corticosteroids (p = 0.497) (Table 3).
3.5. Characteristics of Patients Retreated with ICI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolchok, J.D. PD-1 Blockers. Cell 2015, 162, 937. [Google Scholar] [CrossRef] [PubMed]
- De Martin, E.; Michot, J.-M.; Rosmorduc, O.; Guettier, C.; Samuel, D. Liver toxicity as a limiting factor to the increasing use of immune checkpoint inhibitors. JHEP Rep. 2020, 2, 100170. [Google Scholar] [CrossRef] [PubMed]
- Iwama, S.; De Remigis, A.; Callahan, M.K.; Slovin, S.F.; Wolchok, J.D.; Caturegli, P. Pituitary expression of CTLA-4 mediates hypophysitis secondary to admin-istration of CTLA-4 blocking antibody. Sci. Transl. Med. 2014, 6, 230–245. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Saini, S.; Prabhakar, B.S. Cancer immunotherapy with check point inhibitor can cause autoimmune adverse events due to loss of Treg homeostasis. Semin. Cancer Biol. 2020, 64, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Das, R.; Bar, N.; Ferreira, M.; Newman, A.M.; Zhang, L.; Bailur, J.K.; Bacchiocchi, A.; Kluger, H.; Wei, W.; Halaban, R.; et al. Early B cell changes predict autoimmunity following combination immune checkpoint blockade. J. Clin. Investig. 2018, 128, 715–720. [Google Scholar] [CrossRef]
- Peeraphatdit, T.; Wang, J.; Odenwald, M.A.; Hu, S.; Hart, J.; Charlton, M.R. Hepatotoxicity from Immune Checkpoint Inhibitors: A Systematic Review and Management Recommendation. Hepatology 2020, 72, 315–329. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. National Comprehensive Cancer Network. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology Clin-ical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef]
- Haanen, J.; Carbonnel, F.; Robert, C.; Kerr, K.; Peters, S.; Larkin, J.; Jordan, K. ESMO Guidelines Committee. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for di-agnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. S4), iv264–iv266. [Google Scholar] [CrossRef]
- Dougan, M.; Wang, Y.; Rubio-Tapia, A.; Lim, J.K. AGA clinical practice update on diagnosis and management of immune check-point inhibitor (ICI) colitis and hepatitis: Expert review. Gastroenterology 2021, 160, 1384–1393. [Google Scholar] [CrossRef]
- Li, M.; Sack, J.S.; Bell, P.; Rahma, O.E.; Srivastava, A.; Grover, S.; Zucker, S.D. Utility of Liver Biopsy in Diagnosis and Management of High-grade Immune Checkpoint Inhibi-tor Hepatitis in Patients with Cancer. JAMA Oncol. 2021, 7, 1711. [Google Scholar] [CrossRef]
- Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (accessed on 2 May 2023).
- Roussel Uclaf Causality Assessment Method (RUCAM) in Drug Induced Liver Injury. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012. Available online: http://www.ncbi.nlm.nih.gov/books/NBK548272/ (accessed on 28 May 2022).
- Miller, E.D.; Abu-Sbeih, H.; Styskel, B.; Gonzalez, G.M.N.; Blechacz, B.; Naing, A.; Chalasani, N. Clinical Characteristics and Adverse Impact of Hepatotoxicity due to Immune Checkpoint Inhibitors. Am. J. Gastroenterol. 2020, 115, 251–261. [Google Scholar] [CrossRef]
- Everett, J.; Srivastava, A.; Misdraji, J. Fibrin Ring Granulomas in Checkpoint Inhibitor-induced Hepatitis. Am. J. Surg. Pathol. 2017, 41, 134–137. [Google Scholar] [CrossRef]
- De Martin, E.; Michot, J.-M.; Papouin, B.; Champiat, S.; Mateus, C.; Lambotte, O.; Roche, B.; Antonini, T.M.; Coilly, A.; Laghouati, S.; et al. Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J. Hepatol. 2018, 68, 1181–1190. [Google Scholar] [CrossRef]
- Papouin, B.; Mussini, C.; De Martin, E.; Guettier, C. Hepatic and Digestive Adverse Events of Immune Checkpoint Inhibitors (An-ti-CTLA-4 and, Anti-PD-1/pd-L1): A Clinico-Pathological Review. Ann. Pathol. 2018, 38, 338–351. [Google Scholar] [CrossRef]
- Cohen, J.V.; Dougan, M.; Zubiri, L.; Reynolds, K.L.; Sullivan, R.J.; Misdraji, J. Liver biopsy findings in patients on immune checkpoint inhibitors. Mod. Pathol. 2021, 34, 426–437. [Google Scholar] [CrossRef]
- Doherty, G.J.; Duckworth, A.M.; Davies, S.E.; Mells, G.F.; Brais, R.; Harden, S.V.; Parkinson, C.A.; Corrie, P.G. Severe steroid-resistant anti-PD1 T-cell checkpoint inhibitor-induced hepato-toxicity driven by biliary injury. ESMO Open 2017, 2, e000268. [Google Scholar] [CrossRef]
- Pi, B.; Wang, J.; Tong, Y.; Yang, Q.; Lv, F.; Yu, Y. Immune-related cholangitis induced by immune checkpoint inhibitors: A systematic review of clinical features and management. Eur. J. Gastroenterol. Hepatol. 2021, 33 (Suppl. S1), e858–e867. [Google Scholar] [CrossRef]
- Hountondji, L.; De Matos, C.F.; Lebossé, F.; Quantin, X.; Lesage, C.; Palassin, P.; Rivet, V.; Faure, S.; Pageaux, G.-P.; Assenat, E.; et al. Clinical pattern of checkpoint inhibitor-induced liver injury in a multicentre cohort. JHEP Rep. 2023, 5, 100719. [Google Scholar] [CrossRef]
- Shimozaki, K.; Sukawa, Y.; Beppu, N.; Kurihara, I.; Suzuki, S.; Mizuno, R.; Funakoshi, T.; Ikemura, S.; Tsugaru, K.; Togasaki, K.; et al. Multiple Immune-Related Adverse Events and Anti-Tumor Efficacy: Real-World Data on Various Solid Tumors. Cancer Manag. Res. 2020, 12, 4585–4593. [Google Scholar] [CrossRef]
- Bouhlel, L.; Doyen, J.; Chamorey, E.; Poudenx, M.; Ilie, M.; Gal, J.; Guigay, J.; Benzaquen, J.; Marquette, C.H.; Berthet, J.P.; et al. Occurrence and number of immune-related adverse events are independently asso-ciated with survival in advanced non-small-cell lung cancer treated by nivolumab. Bull. Cancer 2020, 107, 946–958. [Google Scholar] [CrossRef]
- Das, S.; Johnson, D.B. Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 306. [Google Scholar] [CrossRef] [PubMed]
- Riveiro-Barciela, M.; Barreira-Díaz, A.; Callejo-Pérez, A.; Muñoz-Couselo, E.; Díaz-Mejía, N.; Díaz-González, Á.; Londoño, M.-C.; Salcedo, M.-T.; Buti, M. Retreatment with Immune Checkpoint Inhibitors after a Severe Immune-Related Hepatitis: Results from a Prospective Multicenter Study. Clin. Gastroenterol. Hepatol. 2023, 21, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Tsung, I.; Dolan, R.; Lao, C.D.; Fecher, L.; Riggenbach, K.; Yeboah-Korang, A.; Fontana, R.J. Liver injury is most commonly due to hepatic metastases rather than drug hepatotoxicity during pembrolizumab immunotherapy. Aliment. Pharmacol. Ther. 2019, 50, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Gauci, M.L.; Baroudjian, B.; Zeboulon, C.; Pages, C.; Poté, N.; Roux, O.; Bouattour, M.; Lebbé, C. Immune-related hepatitis with immunotherapy: Are corticosteroids always needed? J. Hepatol. 2018, 69, 548–550. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Population | Biopsy, N (%) | p-Value | |
|---|---|---|---|---|
| Non | Yes | |||
| Patients, n (%) | 35 (100) | 15 (43) | 20 (57) | |
| Median age at ICI-DILI, years (IQR) | 62 (48–73) | 69 (45–77) | 59 (49–65) | 0.383 |
| Sex, male, n (%) | 14 (40) | 6 (40) | 8 (40) | 0.999 |
| Non-smoker, n (%) | 17 (48) | 8 (53) | 9 (45) | 0.630 |
| Alcohol use, n (%) | 5 (14) | 1 (7) | 4 (20) | 0.272 |
| Pre-existing chronic liver disease, n (%) | 0 (0) | 0 (0) | 0 (0) | 0.999 |
| Underlying cancer | ||||
| Melanoma, n (%) | 19 (54) | 9 (60) | 10 (50) | 0.698 |
| Lymphoma, n (%) | 1 (3) | 1 (7) | 0 (0) | |
| Non-small-cell lung cancer, n (%) | 10 (28) | 3 (20) | 7 (35) | |
| Other, n (%) | 5 (14) | 2 (13) | 3 (15) | |
| Presence of liver metastases, n (%) | 5 (14) | 2 (13) | 3 (15) | 0.272 |
| Other immuno-mediated side effects, n(%) | 12 (34) | 7 (47) | 5 (25) | 0.188 |
| Anti-PD-1 monotherapy, n (%) | 26 (74) | 12 (80) | 14 (70) | 0.509 |
| Anti-PD-1/anti-CTLA-4 combination therapy, n (%) | 9 (25) | 3 (20) | 6 (30) | 0.509 |
| Previous chemotherapy, n (%) | 15 (43) | 8 (53) | 7 (35) | 0.285 |
| Median of liver function tests at ICI-DILI (IQR) | ||||
| Aspartate aminotransferase (AST), U/L (IQR) | 163 (68–489) | 119 (51–207) | 281 (80–550) | 0.059 |
| Alanine amino transferase (ALT), U/L (IQR) | 344 (114–667) | 154 (57–481) | 642 (123–796) | 0.022 |
| Alkaline phosphatase, U/L (IQR) | 144 (108–226) | 133 (111–199) | 171 (108–246) | 0.676 |
| Gamma-GT, U/L (IQR) | 162 (71–523) | 180 (124–342) | 121 (53–527) | 0.389 |
| Total bilirubin (umol/L) (IQR) | 8.2 (5.2–15.2) | 6.4 (5.6–14.2) | 8.7 (5–22.7) | 0.325 |
| Prothrombin time, (PT) (%) | 80 (71–100) | 100 (94–100) | 83 (73.5–101) | 0.383 |
| Platelets × 103/μL (IQR) | 218 (190–259) | 232 (193–242) | 227 (195–295) | 0.460 |
| R-factor (IQR) | 4.8 (2.4–9.1) | 2.5 (2.2–4) | 5.9 (4–14.9) | 0.004 |
| RUCAM score (IQR) | 7 (6–9) | 7 (5.5–9.5) | 7.5 (6–8.7) | 0.999 |
| Time until liver function tests normalization, days (IQR) | 60 (40–120) | 49 (37–97) | 60 (42–135) | 0.205 |
| ICI discontinuation, n (%) | 32 (91) | 13 (87) | 19 (95) | 0.390 |
| Reduction of ICI dosage, n (%) | 4 (11) | 2 (13) | 2 (10) | 0.776 |
| Corticosteroid therapy, n (%) | 20 (57) | 6 (40) | 14 (70) | 0.080 |
| Rechallenge N (%) yes | ||||
| same ICI | 4 (11) | 2 (13) | 2 (10) | 0.762 |
| other ICI | 4 (11) | 2 (13) | 2 (10) | 0.762 |
| non | 27 (77) | 11 (73) | 16 (80) | |
| Characteristics | Population (35) | Anti-PD-1 Monotherapy (26) | Anti-PD-1 + Anti-CTLA-4 Combination Therapy (9) | p-Value | |
|---|---|---|---|---|---|
| Median age at ICI-DILI, years (IQR) | 62 (48–73) | 65 (55–73) | 48 (45–62) | 0.043 | |
| Sex, male, n (%) | 14 (40) | 10 (38) | 4 (44) | 0.756 | |
| Underlying cancer | Melanoma, n (%) | 19 (54) | 10 (38.5) | 9 (100) | 0.003 |
| Lymphoma, n (%) | 1 (3) | 1 (4) | 0 (0) | ||
| Non-small-cell lung cancer, n (%) | 10 (28) | 10 (38.5) | 0 (0) | ||
| Other, n (%) | 5 (14) | 5 (19) | 0 (0) | ||
| Previous chemotherapy, n (%) | 15 (43) | 13 (50) | 2 (22) | 0.153 | |
| Treatment line, n (IQR) | 1 (1–2) | 1 (1–2) | 1 (1–2) | 0.555 | |
| Number of ICI cycles, n (IQR) | 3 (1–4) | 2.5 (1–4.25) | 3 (2.5–4) | 0.476 | |
| Other IRAES, n (%) | 12 (34) | 8 (31) | 4 (44) | 0.463 | |
| AST, U/L (IQR) | 163 (75–483) | 156 (64–490) | 194 (96–428) | 0.942 | |
| ALT, U/L (IQR) | 300 (115–665) | 344 (115–665) | 285 (114–891) | 0.961 | |
| ALP, U/L (IQR) | 152 (108–223) | 172 (112–250) | 126 (71–166) | 0.104 | |
| Gamma-GT, U/L (IQR) | 147 (76–488) | 196 (94–526) | 115 (32–154) | 0.104 | |
| Total bilirubin, (umol/L) (IQR) | 8.2 (5.2–15.2) | 7.6 (5–19.2) | 9.8 (6.4–10.6) | 0.438 | |
| Prothrombin time, (PT) (%) | 100 (78–100) | 98 (72–100) | 100 (81–101) | 0.524 | |
| Platelets × 103/μL, (IQR) | 231 (199–255) | 231 (193–251) | 226 (193–281) | 0.925 | |
| R-factor (IQR) | 4.8 (2.4–9.1) | 4.35 (2.28–6.68) | 5.9 (2.5–21.5) | 0.184 | |
| RUCAM score (IQR) | 7 (6–9) | 8 (6.7–9) | 6 (6–8) | 0.130 | |
| Auto antibodies, n (%) | FAN > 1/80 ASMA > 1/80 | 19 (54) 2 (6) | 14 (54) 2 (8) | 5 (57) 0 (0) | 0.956 0.398 |
| Corticosteroid therapy, n(%) | 20 (57) | 13 (50) | 7 (78) | 0.153 | |
| Time until liver function tests normalization, days (IQR) | 60 (40–120) | 49 (37–67) | 120 (75–150) | 0.007 | |
| Histological pattern, n (%), available for 20 patients | Toxic | 6 (30) | 5 (36) | 1 (17) | 0.406 |
| Autoimmune | 1 (5) | 0 (0) | 1 (17) | 0.141 | |
| Granulomatous | 6 (30) | 3 (21) | 3 (50) | 0.253 | |
| Mixed (toxic + autoimmune) | 1 (5) | 1 (7) | 0 (0) | 0.497 | |
| None | 6 (30) | 5 (36) | 1 (17) | 0.355 | |
| Histological pattern, n (%) | Minimal necrosis | 10 (50) | 9 (45) | 1 (5) | 0.057 |
| Mild necrosis | 2 (10) | 0 (0) | 2 (10) | 0.026 | |
| Severe necrosis | 7 (35) | 3 (15) | 4 (20) | 0.058 | |
| ICI discontinuation, n (%) | 32 (91) | 23 (88) | 9 (100) | 0.294 | |
| ICI dose reduction, n (%) | 4 (11) | 1 (4) | 3 (33) | 0.021 | |
| ICI rechallenge, n (%) | Yes Same ICI Other ICI No | 4 (11) 4 (11) 27 (77) | 2 (8) 3 (11) 21 (80) | 2 (22) 1 (11) 6 (77) | 0.244 0.073 |
| Characteristics | With Corticosteroids (20) | Without Corticosteroids (15) | p-Value | |
|---|---|---|---|---|
| Patient profile: | ||||
| Type of immunotherapy, n (%) | Anti-PD-1 monotherapy | 13 (65) | 13 (87) | 0.153 |
| Anti-PD-1 + anti-CTLA-4 combination therapy | 7 (35) | 2 (13) | 0.153 | |
| Biochemical severity (ALT), n (%) | Grade 1 | 3 (15) | 2 (13) | 0.095 |
| Grade 2 | 2 (10) | 5 (33) | ||
| Grade 3 | 6 (30) | 6 (40) | ||
| Grade 4 | 9 (45) | 2 (13) | ||
| Histological severity (necrosis), n (%) | minimal | 5 (25) | 5 (33) | 0.057 |
| mild | 2 (10) | 0 (0) | 0.342 | |
| severe | 7 (35) | 0 (0) | 0.036 | |
| Histology (yes), n (%) | 14 (70) | 6 (40) | 0.080 | |
| Histological pattern, n (%) | Toxic | 5 (25) | 1 (7) | 0.406 |
| Autoimmune | 1 (5) | 0 (0) | 0.497 | |
| Granulomatous | 4 (20) | 2 (13) | 0.913 | |
| Mixed Non | 1 (5) 3 (15) | 0 (0) 3 (20) | 0.497 0.253 | |
| Characteristics of care: | ||||
| ICI discontinuation, n (%) | 19 (95) | 13 (87) | 0.390 | |
| ICI rechallenge (same or other ICI), n (%) | 4 (25) 1 (5) | 3 (20) 0 (0) | 0.070 0.174 | |
| Time until improvement in liver function, n (%) | 90 (60–120) | 40 (30–57) | 0.015 |
| Characteristics | ICI Retreated Patients (8) | Non ICI-Retreated Patients (27) | p-Value |
|---|---|---|---|
| Biopsed, n (%) | 4 (50) | 16 (59) | 0.647 |
| Anti-PD-1 monotherapy, n (%) | 5 (63) | 21 (78) | 0.392 |
| Anti-PD-1/anti-CTLA-4 combination therapy, n (%) | 3 (38) | 6 (22) | 0.392 |
| Biochemical severity, grade 3–4 ALT at ICI-DILI, n (%) | 5 (63) | 18 (67) | 0.378 |
| Histological severity at ICI-DILI, n (%) | 3 (38) | 4 (15) | 0.068 |
| Corticosteroids, n (%) | 5 (63) | 15 (56) | 0.731 |
| 1-month oncological disease progression, n (%) | 4 (50) | 9 (33) | 0.598 |
| 3-month oncological disease progression, n (%) | 4 (50) | 8 (30) | 0.454 |
| 6-month oncological disease progression, n (%) | 2 (25) | 3 (11) | 0.433 |
| 12-month oncological disease progression, n (%) | 2 (25) | 4 (15) | 0.703 |
| Death | 4 (50) | 12 (44) | 0.923 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parlati, L.; Marcin, K.; Terris, B.; Vallet-Pichard, A.; Corouge, M.; Hollande, C.; Sogni, P.; Mallet, V.; Pol, S. Histological Characteristics and Management of Hepatitis on Immune Checkpoint Inhibitors: A Retrospective Descriptive Study. J. Clin. Med. 2023, 12, 3751. https://doi.org/10.3390/jcm12113751
Parlati L, Marcin K, Terris B, Vallet-Pichard A, Corouge M, Hollande C, Sogni P, Mallet V, Pol S. Histological Characteristics and Management of Hepatitis on Immune Checkpoint Inhibitors: A Retrospective Descriptive Study. Journal of Clinical Medicine. 2023; 12(11):3751. https://doi.org/10.3390/jcm12113751
Chicago/Turabian StyleParlati, Lucia, Kennie Marcin, Benoit Terris, Anaïs Vallet-Pichard, Marion Corouge, Clémence Hollande, Philippe Sogni, Vincent Mallet, and Stanislas Pol. 2023. "Histological Characteristics and Management of Hepatitis on Immune Checkpoint Inhibitors: A Retrospective Descriptive Study" Journal of Clinical Medicine 12, no. 11: 3751. https://doi.org/10.3390/jcm12113751
APA StyleParlati, L., Marcin, K., Terris, B., Vallet-Pichard, A., Corouge, M., Hollande, C., Sogni, P., Mallet, V., & Pol, S. (2023). Histological Characteristics and Management of Hepatitis on Immune Checkpoint Inhibitors: A Retrospective Descriptive Study. Journal of Clinical Medicine, 12(11), 3751. https://doi.org/10.3390/jcm12113751