
Multimodal Prehabilitation in Heart Transplant Recipients Improves Short-Term Post-Transplant Outcomes without Increasing Costs

 , , , , , , , , , and
on behalf of the Hospital Clínic de Barcelona Prehabilitation Group (Surgifit)
, , , , , , , , , and
on behalf of the Hospital Clínic de Barcelona Prehabilitation Group (Surgifit)
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
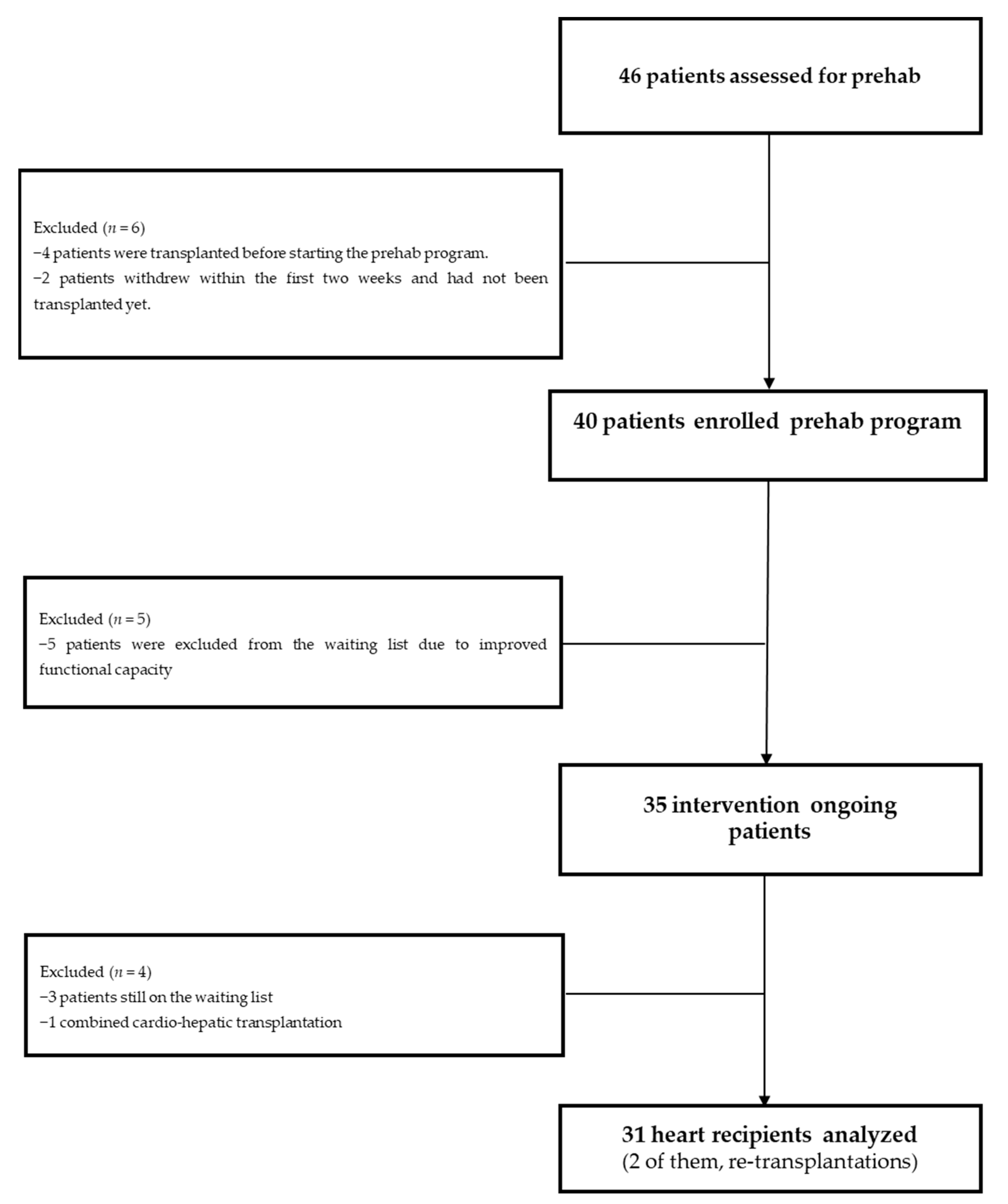
2.2. Participants
2.3. Intervention
2.4. Prehabilitation Program
2.5. Costs
2.6. Outcomes
2.7. Statistical Analysis and Sample Size Estimation
3. Results
3.1. Preoperative Effects of Prehabilitation
3.2. Impact of the Intervention on Postoperative Outcomes
3.3. Costs and Economic Impact
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Crespo-Leiro, M.G.; Metra, M.; Lund, L.H.; Milicic, D.; Costanzo, M.R.; Filippatos, G.; Gustafsson, F.; Tsui, S.; Barge-Caballero, E.; De Jonge, N.; et al. Advanced heart failure: A position statement of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 1505–1535. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of Ame. J. Am. Coll. Cardiol. 2017, 70, 776–803. [Google Scholar] [CrossRef] [PubMed]
- Kittleson, M.M.; Kobashigawa, J. Long-term care of the heart transplant recipient. Curr. Opin. Organ Transplant. 2014, 19, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Kittleson, M.M.; Kobashigawa, J.A. Cardiac Transplantation: Current Outcomes and Contemporary Controversies. JACC Heart Fail. 2017, 5, 857–868. [Google Scholar] [CrossRef] [PubMed]
- Bottiger, B.A.; Nicoara, A.; Snyder, L.D.; Wischmeyer, P.E.; Schroder, J.N.; Patel, C.B.; Daneshmand, M.A.; Sladen, R.N.; Ghadimi, K. Frailty in the End-Stage Lung Disease or Heart Failure Patient: Implications for the Perioperative Transplant Clinician. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1382–1392. [Google Scholar] [CrossRef] [PubMed]
- Leng, S.X.; Kittleson, M.M. Beyond the eyeball test: Impact and potential mechanisms of frailty in heart transplant candidates. J. Heart Lung Transplant. 2021, 40, 95–98. [Google Scholar] [CrossRef]
- Kobashigawa, J.; Shah, P.; Joseph, S.; Olymbios, M.; Bhat, G.; Dhital, K.; Eisen, H.; Kransdorf, E.; Patel, J.; Skorka, R.; et al. Frailty in heart transplantation: Report from the heart workgroup of a consensus conference on frailty. Am. J. Transplant. 2021, 21, 636–644. [Google Scholar] [CrossRef]
- Mauthner, O.; Claes, V.; Deschodt, M.; Jha, S.R.; Engberg, S.; Macdonald, P.S.; Newton, P.J.; De Geest, S. Handle with care: A systematic review on frailty in cardiac care and its usefulness in heart transplantation. Transplant. Rev. 2017, 31, 218–224. [Google Scholar] [CrossRef]
- Macdonald, P. Frailty of the Heart Recipient. Transplantation 2021, 105, 2352–2361. [Google Scholar] [CrossRef]
- Jha, S.R.; Hannu, M.K.; Chang, S.; Montgomery, E.; Harkess, M.; Wilhelm, K.; Hayward, C.S.; Jabbour, A.; Spratt, P.M.; Newton, P.; et al. The Prevalence and Prognostic Significance of Frailty in Patients With Advanced Heart Failure Referred for Heart Transplantation. Transplantation 2016, 100, 429–436. [Google Scholar] [CrossRef]
- Khush, K.K.; Hsich, E.; Potena, L.; Cherikh, W.S.; Chambers, D.C.; Harhay, M.O.; Hayes, D.; Perch, M.; Sadavarte, A.; Toll, A.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-eighth adult heart transplantation report—2021; Focus on recipient characteristics. J. Heart Lung Transplant. 2021, 40, 1035–1049. [Google Scholar] [CrossRef] [PubMed]
- Lietz, K.; John, R.; Burke, E.A.; Ankersmit, J.H.; McCue, J.D.; Naka, Y.; Oz, M.C.; Mancini, D.M.; Edwards, N.M. Pretransplant Cachexia and Morbid Obesity Are Predictors of Increased Mortality after Heart Transplantation1. Transplantation 2001, 72, 277–283. [Google Scholar] [CrossRef]
- Gillis, C.; Carli, F. Promoting Perioperative Metabolic and Nutritional Care. Anesthesiology 2015, 123, 1455–1472. [Google Scholar] [CrossRef]
- Levett, D.Z.H.; Grimmett, C. Psychological factors, prehabilitation and surgical outcomes: Evidence and future directions. Anaesthesia 2019, 74, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Carli, F. Prehabilitation for the Anesthesiologist. Anesthesiology 2020, 133, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Barberan-Garcia, A.; Ubré, M.; Roca, J.; Lacy, A.M.; Burgos, F.; Risco, R.; Momblán, D.; Balust, J.; Blanco, I.; Martínez-Pallí, G. Personalised prehabilitation in high-risk patients undergoing elective major abdominal surgery: A randomized blinded controlled trial. Ann. Surg. 2018, 267, 50–56. [Google Scholar] [CrossRef]
- Drudi, L.M.; Tat, J.; Ades, M.; Mata, J.; Landry, T.; MacKenzie, K.S.; Steinmetz, O.K.; Gill, H.L. Preoperative Exercise Rehabilitation in Cardiac and Vascular Interventions. J. Surg. Res. 2019, 237, 3–11. [Google Scholar] [CrossRef]
- Scheede-Bergdahl, C.; Minnella, E.M.; Carli, F. Multi-modal prehabilitation: Addressing the why, when, what, how, who and where next? Anaesthesia 2019, 74 (Suppl. S1), 20–26. [Google Scholar] [CrossRef]
- Myers, J.; Niebauer, J.; Humphrey, R. Prehabilitation Coming of Age implications for cardiac and pulmonary rehabilitation. J. Cardiopulm. Rehabil. Prev. 2021, 41, 141–146. [Google Scholar] [CrossRef]
- McCann, M.; Stamp, N.; Ngui, A.; Litton, E. Cardiac Prehabilitation. J. Cardiothorac. Vasc. Anesth. 2019, 33, 2255–2265. [Google Scholar] [CrossRef]
- O’connor, C.M.; Whellan, D.J.; Lee, K.L.; Keteyian, S.J.; Cooper, L.S.; Ellis, S.J.; Leifer, E.S.; Kraus, W.E.; Kitzman, D.W.; Blumenthal, J.A.; et al. Efficacy and Safety of Exercise Training in Patients With Chronic Heart Failure: HF-ACTION randomized controlled trial. JAMA 2009, 301, 1439–1450. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Sagar, V.A.; Davies, E.J.; Briscoe, S.; Coats, A.J.; Dalal, H.; Lough, F.; Rees, K.; Singh, S.J.; Mordi, I.R. Exercise-based rehabilitation for heart failure. Cochrane Database Syst. Rev. 2014, 2014, CD003331. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Conraads, V.; Corrà, U.; Dickstein, K.; Francis, D.P.; Jaarsma, T.; McMurray, J.; Pieske, B.; Piotrowicz, E.; Schmid, J.-P.; et al. Exercise training in heart failure: From theory to practice. A consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur. J. Heart Fail. 2011, 13, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Gerhardt, A.; Weidner, G.; Grassmann, M.; Spaderna, H. Everyday Physical Activity in Ambulatory Heart Transplant Candidates: The Role of Expected Health Benefits, Social Support, and Potential Barriers. Int. J. Behav. Med. 2014, 21, 248–257. [Google Scholar] [CrossRef]
- Fleg, J.L.; Cooper, L.S.; Borlaug, B.A.; Haykowsky, M.J.; Kraus, W.E.; Levine, B.D.; Pfeffer, M.A.; Piña, I.L.; Poole, D.C.; Reeves, G.R.; et al. Exercise Training as Therapy for Heart Failure current status and future directions. Circ. Heart Fail. 2015, 8, 209–220. [Google Scholar] [CrossRef]
- Gimeno-Santos, E.; Coca-Martinez, M.; Arguis, M.J.; Navarro, R.; Lopez-Hernandez, A.; Castel, M.A.; Romano, B.; López-Baamonde, M.; Sandoval, E.; Farrero, M.; et al. Multimodal prehabilitation as a promising strategy for preventing physical deconditioning on the heart transplant waiting list. Eur. J. Prev. Cardiol. 2019, 27, 2367–2370. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef]
- Campbell, W.W.; Leidy, H.J. Dietary Protein and Resistance Training Effects on Muscle and Body Composition in Older Persons. J. Am. Coll. Nutr. 2007, 26, 696S–703S. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo Classification of Surgical Complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Slankamenac, K.; Graf, R.; Barkun, J.; Puhan, M.A.; Clavien, P.-A. The Comprehensive Complication Index: A novel continuous scale to measure surgical morbidity. Ann. Surg. 2013, 258, 1–7. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Dhand, N.K.; Khatkar, M.S.; Statulator: An Online Statistical Calculator. Sample Size Calculator for Comparing Two Independent Means. 2014. Available online: https://statulator.com/SampleSize/ss2M.html (accessed on 20 April 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 20 April 2023).
- StataCorp. Stata Statistical Software: Release 17; StataCorp LLC: College Station, TX, USA, 2021. [Google Scholar]
- Gillis, C.; Fenton, T.R.; Sajobi, T.T.; Minnella, E.M.; Awasthi, R.; Loiselle, S.; Liberman, A.S.; Stein, B.; Charlebois, P.; Carli, F. Trimodal prehabilitation for colorectal surgery attenuates post-surgical losses in lean body mass: A pooled analysis of randomized controlled trials. Clin. Nutr. 2019, 38, 1053–1060. [Google Scholar] [CrossRef]
- Herdy, A.H.; Marcchi, P.L.B.; Vila, A.; Tavares, C.; Collaço, J.; Niebauer, J.; Ribeiro, J.P. Pre- and Postoperative Cardiopulmonary Rehabilitation in Hospitalized Patients Undergoing Coronary Artery Bypass Surgery a randomized controlled trial. Am. J. Phys. Med. Rehabil. 2008, 87, 714–719. [Google Scholar] [CrossRef]
- Mayo, N.E.; Feldman, L.; Scott, S.; Zavorsky, G.; Kim, D.J.; Charlebois, P.; Stein, B.; Carli, F. Impact of preoperative change in physical function on postoperative recovery: Argument supporting prehabilitation for colorectal surgery. Surgery 2011, 150, 505–514. [Google Scholar] [CrossRef]
- Molenaar, C.J.L.; Minnella, E.M.; Coca-Martinez, M.; Ten Cate, D.W.G.; Regis, M.; Awasthi, R.; Martínez-Palli, G.; López-Baamonde, M.; Sebio-Garcia, R.; Feo, C.V.; et al. Effect of Multimodal Prehabilitation on Reducing Postoperative Complications and Enhancing Functional Capacity Following Colorectal Cancer Surgery: The PREHAB Randomized Clinical Trial. JAMA Surg 2023. [Google Scholar] [CrossRef]
- Nagarajan, K.; Bennett, A.; Agostini, P.; Naidu, B. Is preoperative physiotherapy/pulmonary rehabilitation beneficial in lung resection patients? Interact. Cardiovasc. Thorac. Surg. 2011, 13, 300–302. [Google Scholar] [CrossRef]
- Myers, J.; Mcelrath, M.; Jaffe, A.; Smith, K.; Fonda, H.; Vu, A.; Hill, B.; Dalman, R. A Randomized Trial of Exercise Training in Abdominal Aortic Aneurysm Disease. Med. Sci. Sports Exerc. 2014, 46, 2–9. [Google Scholar] [CrossRef]
- Coca-Martinez, M.; Barberan-Garcia, A.; Risco, R.; Lopez-Baamonde, M.; Martinez-Palli, G. Fit for surgery? Evidence supporting prehabilitation programs. Br. J. Anaesth. 2018, 120, 1429. [Google Scholar] [CrossRef]
- Herrera-Santelices, A.; Argüello-Florencio, G.; Westphal, G.; Junior, N.N.; Zamunér, A.R. Effects of Supervised Physical Exercise as Prehabilitation on Body Composition, Functional Capacity and Quality of Life in Bariatric Surgery Candidates: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 5091. [Google Scholar] [CrossRef]
- Lotzke, H.; Brisby, H.; Gutke, A.; Hägg, O.; Jakobsson, M.; Smeets, R.; Lundberg, M. A Person-Centered Prehabilitation Program Based on Cognitive-Behavioral Physical Therapy for Patients Scheduled for Lumbar Fusion Surgery: A Randomized Controlled Trial. Phys. Ther. 2019, 99, 1069–1088. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Ying, H.; Rasmussen, S.V.P.; Schrack, J.; Haugen, C.E.; Chu, N.M.; Fernández, M.G.; Desai, N.; Walston, J.D.; Segev, D.L. Prehabilitation prior to kidney transplantation: Results from a pilot study. Clin. Transplant. 2019, 33, e13450. [Google Scholar] [CrossRef]
- Hoffman, M.; Chaves, G.; Ribeiro-Samora, G.A.; Britto, R.R.; Parreira, V.F. Effects of pulmonary rehabilitation in lung transplant candidates: A systematic review. BMJ Open 2017, 7, e013445. [Google Scholar] [CrossRef]
- Chen, Y.W.; Wang, C.Y.; Lai, Y.H.; Liao, Y.C.; Wen, Y.K.; Chang, S.T.; Huang, J.L.; Wu, T.J. Home-based cardiac rehabilitation improves quality of life, aerobic capacity, and readmission rates in patients with chronic heart failure. Medicine 2018, 97, e9629. [Google Scholar] [CrossRef]
- Sabbag, A.; Mazin, I.; Rott, D.; Hay, I.; Gang, N.; Tzur, B.; Goldkorn, R.; Goldenberg, I.; Klempfner, R.; Israel, A. The prognostic significance of improvement in exercise capacity in heart failure patients who participate in cardiac rehabilitation programme. Eur. J. Prev. Cardiol. 2018, 25, 354–361. [Google Scholar] [CrossRef]
- Jessup, M.; Banner, N.; Brozena, S.; Campana, C.; Costard-Jäckle, A.; Dengler, T.; Hunt, S.; Metra, M.; Rahmel, A.; Renlund, D. Optimal Pharmacologic and Non-pharmacologic Management of Cardiac Transplant Candidates: Approaches to Be Considered Prior to Transplant Evaluation: International Society for Heart and Lung Transplantation Guidelines for the Care of Cardiac Transplant Candidates. J. Heart Lung Transplant. 2006, 25, 1003–1023. [Google Scholar] [CrossRef]
- Mathur, S.; Janaudis-Ferreira, T.; Wickerson, L.; Singer, L.G.; Patcai, J.; Rozenberg, D.; Blydt-Hansen, T.; Hartmann, E.L.; Haykowsky, M.; Helm, D.; et al. Meeting Report: Consensus Recommendations for a Research Agenda in Exercise in Solid Organ Transplantation. Am. J. Transplant. 2014, 14, 2235–2245. [Google Scholar] [CrossRef]
- Sousa-Uva, M.; Head, S.J.; Milojevic, M.; Collet, J.-P.; Landoni, G.; Castella, M.; Dunning, J.; Gudbjartsson, T.; Linker, N.J.; Sandoval, E.; et al. 2017 EACTS Guidelines on perioperative medication in adult cardiac surgery. Eur. J. Cardio-Thoracic Surg. 2018, 53, 5–33. [Google Scholar] [CrossRef]
- Suarez-Pierre, A.; Lui, C.; Zhou, X.; Giuliano, K.; Etchill, E.; Almaraz-Espinoza, A.; Crawford, T.C.; Fraser, C.D.; Whitman, G.J.; Choi, C.W.; et al. Long-term Survival After Heart Transplantation: A Population-based Nested Case-Control Study. Ann. Thorac. Surg. 2021, 111, 889–898. [Google Scholar] [CrossRef]
- Khush, K.K.; Cherikh, W.S.; Chambers, D.C.; Goldfarb, S.; Hayes, D.; Kucheryavaya, A.Y.; Levvey, B.J.; Meiser, B.; Rossano, J.W.; Stehlik, J. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-fifth Adult Heart Transplantation Report—2018; Focus Theme: Multiorgan Transplantation. J. Heart Lung Transplant. 2018, 37, 1155–1168. [Google Scholar] [CrossRef]
- Hébert, M.; Cartier, R.; Dagenais, F.; Langlois, Y.; Coutu, M.; Noiseux, N.; El-Hamamsy, I.; Stevens, L.-M. Standardizing Postoperative Complications—Validating the Clavien-Dindo Complications Classification in Cardiac Surgery. Semin. Thorac. Cardiovasc. Surg. 2021, 33, 443–451. [Google Scholar] [CrossRef]
- Barberan-Garcia, A.; Ubre, M.; Pascual-Argente, N.; Risco, R.; Faner, J.; Balust, J.; Lacy, A.; Puig-Junoy, J.; Roca, J.; Martinez-Palli, G. Post-discharge impact and cost-consequence analysis of prehabilitation in high-risk patients undergoing major abdominal surgery: Secondary results from a randomised controlled trial. Br. J. Anaesth. 2019, 123, 450–456. [Google Scholar] [CrossRef]
- Ostrominski, J.W.; Hirji, S.; Bhatt, A.S.; Butler, J.; Fiuzat, M.; Fonarow, G.C.; Heidenreich, P.A.; Januzzi, J.L.; Lam, C.S.; Maddox, T.M.; et al. Cost and Value in Contemporary Heart Failure Clinical Guidance Documents. JACC Heart Fail. 2022, 10, 1–11. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Fonarow, G.C.; Opsha, Y.; Sandhu, A.T.; Sweitzer, N.K.; Warraich, H.J.; Butler, J.; Hsich, E.; Pressler, S.B.; Shah, K.; et al. Economic Issues in Heart Failure in the United States. J. Card. Fail. 2022, 28, 453–466. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (N = 51) | preHAB Group (N = 31) | p-Value | |
|---|---|---|---|
| Age (years) | 56 ± 12 | 54 ± 13 | 0.580 |
| Male n (%) | 30 (59) | 25 (81) | 0.072 |
| Smoker Status n (%) | 0.346 | ||
| Former Smoker | 27 (53) | 21 (68) | |
| End-Stage Heart Failure Etiology n (%) | 0.639 | ||
| Ischemic cardiomyopathy | 18 (35) | 13 (42) | |
| Dilated cardiomyopathy | 17 (33) | 8 (26) | |
| Hypertrophic cardiomyopathy | 6 (12) | 5 (16) | |
| Amyloid cardiomyopathy | 1 (2) | 2 (7) | |
| Toxic | 2 (4) | 0 (0) | |
| Others | 7 (14) | 3 (10) | |
| Charlson Comorbidity Index | 3.00 (2–5) | 4.00 (3–6) | 0.376 |
| Obesity (IMC >30) n (%) | 8 (16) | 7 (23) | 0.625 |
| Previous cardiac surgery n (%) | 13 (26) | 10 (32) | 0.683 |
| Levosimendan chronic treatment | 14 (28) | 13 (42) | 0.267 |
| Pulmonary hypertension | 0.911 | ||
| Moderate n (%) (PSAP 40–60 mmHg) | 13 (26) | 7 (23) | |
| Severe n (%) (PSAP > 60 mmHg) | 15 (29) | 10 (32) | |
| Specific pulmonary hypertension treatment n (%) | 16 (31) | 11 (36) | 0.887 |
| Bosentan | 8 (16) | 8 (26) | 0.404 |
| Sildenafil | 10 (20) | 6 (19) | 1.000 |
| Right heart catheterization | |||
| Cardiac index (L/min/m2) | 2.4 ± 1 | 2.2 ± 6 | 0.190 |
| Pulmonary vascular resistance (Wood units) | 1.9 ± 1 | 2.6 ± 2 | 0.014 |
| Left ventricle ejection fraction % | 25 (20–29) | 22 (20–35) | 0.693 |
| Arrhythmia history n (%) | |||
| No previous arrhythmia history | 10 (20) | 11 (36) | 0.181 |
| Atrial fibrillation | 31 (61) | 16 (52) | 0.559 |
| Cardiac resynchronization therapy | 9 (18) | 5 (16) | 1.000 |
| Implantable cardioverter- defibrillator | 41 (80) | 25 (81) | 1.000 |
| CFS-CSHA | Not available | 4 [4,5] | N/A |
| Frailty (CFS-CSHA ≥5) | Not available | 13 (42) | N/A |
| INTERMACS (Last month previous to HT) | 0.080 | ||
| 3 | 4 (8) | 1 (3) | |
| 4 | 17 (34) | 9 (29) | |
| 5 | 20 (40) | 14 (45) | |
| 6 | 9 (18) | 3 (10) | |
| 7 | 0 (0.0) | 4 (13) | |
| Time in waiting list (days) | 100 (28–277) | 186 (93–368) | 0.016 |
| Before Intervention | Post-Program | p-Value | |
|---|---|---|---|
| CPET parameters | |||
| Peak oxygen pulse (VO2/HR) (mL/beats) | 8 (5.92–10.05) | 10.4 (8.35–11.1) | 0.01 |
| Ventilatory efficiency (VE/VCO2) at anaerobic threshold | 39.06 ± 6.19 | 35.85 ± 6.11 | 0.077 |
| Oxygen uptake at anaerobic threshold (AT VO2) (mL/kg/min) | 7.91 ± 2.22 | 9.25 ± 1.94 | 0.033 |
| Peak oxygen uptake (VO2max) (mL/kg/min) | 10.1 (8–13) | 12.5 (10 -14.78) | 0.034 |
| Peak oxygen uptake (VO2max) % ref | 33 (25–45) | 42 (33–50) | 0.026 |
| Peak work-rate (watts) | 66.85 ± 27.56 | 85.67 ± 30.20 | 0.013 |
| Endurance time (seconds) | 281 (208–380) | 728 (397–900) | <0.001 |
| 6MWT (meters) | 411 (355.5–490.5) | 453 (424–514.3) | 0.081 |
| Sit-to-stand (repetitions) | 10 ± 4 | 14 ± 6 | 0.013 |
| YPAS total | 24 (15–37) | 49 (38–60) | <0.001 |
| Hand grip dominant hand (kg) | 33 ± 10 | 37 ± 10 | 0.248 |
| Hand grip non-dominant hand (kg) | 31 ± 10 | 33 ± 9 | 0.518 |
| HADS-anxiety | 5 (3–8) | 4 (2–7) | 0.34 |
| HADS-depression | 4 (2–7) | 4 (3–7) | 0.87 |
| MLHFQ | 58 ± 19 | 47 ± 19 | 0.046 |
| Control Group (N = 51) | preHAB Group (N = 31) | p-Value | |
|---|---|---|---|
| Total number of complications per patient | 5 (3–8) | 3 (2–3) | <0.001 |
| Minor complications (Clavien-Dindo 1 or 2) per patient | 4 (3–6) | 2 (1–3) | <0.001 |
| Major complications (Clavien-Dindo ≥3) per patient | 0 (0–2) | 0 (0–1) | 0.242 |
| Medical complications | 5 (3–7) | 2 (1–3) | <0.001 |
| Surgical complications | 0 (0–1) | 0 (0–1) | 0.167 |
| Comprehensive Complication Index (CCI) | 37 (30–72) | 31 (23–41) | 0.033 |
| Mechanical ventilation time (hours) | 37 (12–143) | 20 (12, 52) | 0.032 |
| ICU length of stay (days) | 7 (5–14) | 5 (3, 7) | 0.010 |
| Primary graft failure (%) | 5 (10) | 1 (3) | 0.502 |
| Surgical reinterventions during HT hospitalization | 7 (14) | 5 (16) | 1.000 |
| Hospitalization length of stay (days) | 23 (18–38) | 18 (16–22) | 0.008 |
| Discharge destination (%) | 0.009 | ||
| Home | 33 (65) | 29 (94) | |
| Nursing/rehabilitation facilities | 16 (31) | 1 (3) | |
| In-hospital mortality | 2 (4) | 1 (3) | 1.000 |
| 30-days after HT mortality | 1 (2) | 0 (0) | 1.000 |
| 3-months after HT mortality | 1 (2) | 2 (7) | 0.657 |
| 1-year after HT mortality | 3 (6) | 3 (10) | 0.839 |
| Control Group (N = 51) | preHAB Group (N = 31) | p-Value | |
|---|---|---|---|
| Arrhythmia requiring antiarrhythmic drugs | 15 (29) | 1 (3) | 0.009 |
| Arrhythmia requiring electrical cardioversion | 3 (6) | 0 (0) | 0.442 |
| Myocardial infarction | 1 (2) | 0 (0) | 1.000 |
| Cardiac arrest | 1 (2) | 1 (3) | 1.000 |
| Primary graft failure | 5 (10) | 1 (3) | 0.502 |
| ECMO/LVAD | 6 (12) | 1 (3) | 0.350 |
| Respiratory insufficiency requiring NIV/HFNC | 5 (10) | 0 (0) | 0.186 |
| Respiratory insufficiency requiring intubation | 2 (4) | 2 (7) | 1.000 |
| Difficult weaning/tracheostomy | 2 (4) | 2 (7) | 1.000 |
| Respiratory tract infection | 14 (28) | 3 (10) | 0.100 |
| Pleural effusion requiring chest-tube placement | 5 (10) | 1 (3) | 0.502 |
| Critical patient myopathy requiring intensified rehabilitation | 15 (29) | 2 (7) | 0.027 |
| Acute kidney injury requiring furosemide perfusion | 26 (51) | 10 (32) | 0.154 |
| Acute kidney injury requiring kidney replacement therapy | 9 (18) | 6 (19) | 1.000 |
| Nausea/vomiting | 20 (39) | 7 (23) | 0.190 |
| Paralytic ileus | 10 (20) | 0 (0) | 0.022 |
| Hyperglycemia requiring insulin infusion | 22 (43) | 8 (26) | 0.179 |
| Pressure ulcers | 3 (6) | 0 (0) | 0.442 |
| Digestive hemorrhage | 6 (12) | 0 (0) | 0.122 |
| Delirium | 16 (31) | 5 (16) | 0.203 |
| Deep venous thrombosis | 4 (8) | 3 (10) | 1.000 |
| Pulmonary thromboembolism | 0 (0) | 0 (0) | not applicable |
| Stroke | 1 (2) | 1 (3) | 1.000 |
| Urinary tract infection | 3 (6) | 0 (0) | 0.442 |
| Catheter-related bloodstream infection | 7 (14) | 2 (7) | 0.511 |
| Other infections | 14 (28) | 5 (16) | 0.364 |
| Reintervention | 7 (14) | 5 (16) | 1.000 |
| Post-surgical hemorrhage | 6 (12) | 2 (7) | 0.687 |
| Surgical site infection | 4 (8) | 1 (3) | 0.710 |
| Cardiac effusion/cardiac tamponade requiring drainage | 4 (8) | 5 (16) | 0.424 |
| Pneumothorax/hemothorax | 5 (10) | 2 (7) | 0.905 |
| Group | N | Median | 1st Quartile | 3rd Quartile | p-Value |
|---|---|---|---|---|---|
| Prehab | 31 | 49,771 € | 44,999 € | 54,432 € | 0.254 |
| Standard Care | 51 | 54,748 € | 45,765 € | 79,777 € |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Baamonde, M.; Arguis, M.J.; Navarro-Ripoll, R.; Gimeno-Santos, E.; Romano-Andrioni, B.; Sisó, M.; Terès-Bellès, S.; López-Hernández, A.; Burniol-García, A.; Farrero, M.; et al. Multimodal Prehabilitation in Heart Transplant Recipients Improves Short-Term Post-Transplant Outcomes without Increasing Costs. J. Clin. Med. 2023, 12, 3724. https://doi.org/10.3390/jcm12113724
López-Baamonde M, Arguis MJ, Navarro-Ripoll R, Gimeno-Santos E, Romano-Andrioni B, Sisó M, Terès-Bellès S, López-Hernández A, Burniol-García A, Farrero M, et al. Multimodal Prehabilitation in Heart Transplant Recipients Improves Short-Term Post-Transplant Outcomes without Increasing Costs. Journal of Clinical Medicine. 2023; 12(11):3724. https://doi.org/10.3390/jcm12113724
Chicago/Turabian StyleLópez-Baamonde, Manuel, María José Arguis, Ricard Navarro-Ripoll, Elena Gimeno-Santos, Bárbara Romano-Andrioni, Marina Sisó, Silvia Terès-Bellès, Antonio López-Hernández, Adrià Burniol-García, Marta Farrero, and et al. 2023. "Multimodal Prehabilitation in Heart Transplant Recipients Improves Short-Term Post-Transplant Outcomes without Increasing Costs" Journal of Clinical Medicine 12, no. 11: 3724. https://doi.org/10.3390/jcm12113724
APA StyleLópez-Baamonde, M., Arguis, M. J., Navarro-Ripoll, R., Gimeno-Santos, E., Romano-Andrioni, B., Sisó, M., Terès-Bellès, S., López-Hernández, A., Burniol-García, A., Farrero, M., Sebio-García, R., Sandoval, E., Sanz-de la Garza, M., Librero, J., García-Álvarez, A., Castel, M. Á., & Martínez-Pallí, G., on behalf of the Hospital Clínic de Barcelona Prehabilitation Group (Surgifit). (2023). Multimodal Prehabilitation in Heart Transplant Recipients Improves Short-Term Post-Transplant Outcomes without Increasing Costs. Journal of Clinical Medicine, 12(11), 3724. https://doi.org/10.3390/jcm12113724